
The Changes in Trends of Lower Gastrointestinal Endoscopy Conducted in Children and Adolescents after the COVID-19 Outbreak in Korea
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Study Design
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. Baseline Characteristics of the Patients
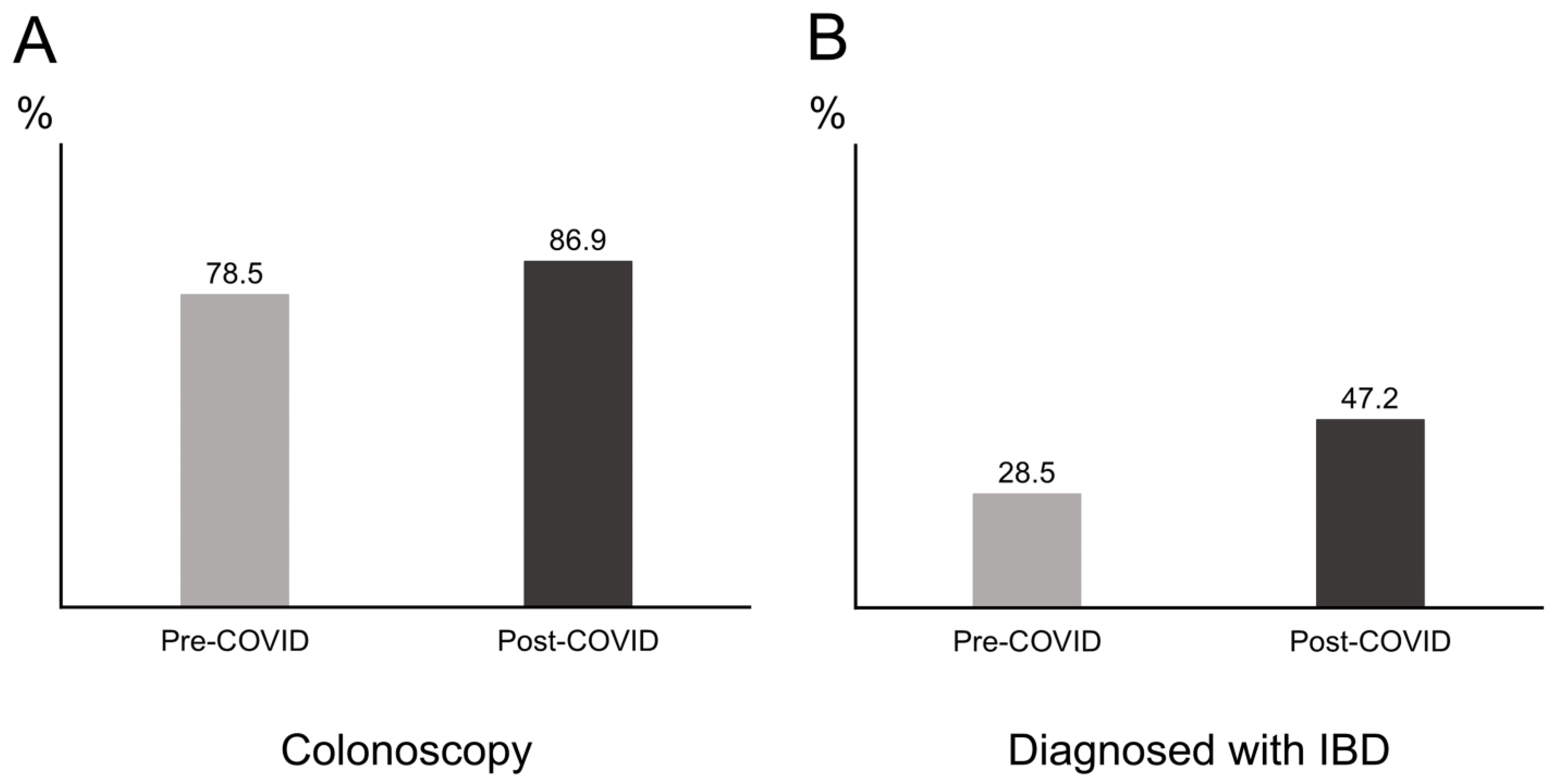
3.2. Comparison of Characteristics between the Pre- and PostCOVID-19 Era
3.3. Comparison of Characteristics between Patients Receiving Colonoscopies and Sigmoidoscopies
3.4. Factors Associated with Conducting a Colonoscopy over a Sigmoidoscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walsh, C.M.; Fishman, D.S.; Lerner, D.G. Pediatric Endoscopy in the Era of Coronavirus Disease 2019: A North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Position Paper. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Park, J.H. Changes in pediatric gastrointestinal endoscopy: Review of a recent hospital experience. Korean J. Pediatr. Gastroenterol. Nutr. 2007, 10, 20–27. [Google Scholar] [CrossRef]
- Lei, P.; Gu, F.; Hong, L.; Sun, Y.; Li, M.; Wang, H.; Zhong, B.; Chen, M.; Cui, Y.; Zhang, S. Pediatric colonoscopy in South China: A 12-year experience in a tertiary center. PLoS ONE 2014, 9, e95933. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H. Pediatric Colonoscopy: The Changing Patterns and Single Institutional Experience Over a Decade. Clin. Endosc. 2018, 51, 137–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.; Kim, E.Y. Sharing Our Experience of Operating an Endoscopy Unit in the Midst of a COVID-19 Outbreak. Clin. Endosc. 2020, 53, 243–245. [Google Scholar] [CrossRef]
- Kim, J.Y.; Choe, P.G.; Oh, Y.; Oh, K.J.; Kim, J.; Park, S.J.; Park, J.H.; Na, H.K.; Oh, M.D. The First Case of 2019 Novel Coronavirus Pneumonia Imported into Korea from Wuhan, China: Implication for Infection Prevention and Control Measures. J. Korean Med. Sci. 2020, 35, e61. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, K.; Holub, J.L.; Gilger, M.A.; Shub, M.D.; McOmber, M.; Tsou, M.; Fishman, D.S. Quality indicators for pediatric colonoscopy: Results from a multicenter consortium. Gastrointest. Endosc. 2016, 83, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Nambu, R.; Hagiwara, S.I.; Kakuta, F.; Hara, T.; Shimizu, H.; Abukawa, D.; Iwama, I.; Kagimoto, S.; Arai, K. Current role of colonoscopy in infants and young children: A multicenter study. BMC Gastroenterol. 2019, 19, 149. [Google Scholar] [CrossRef] [PubMed]
- Gilger, M.A.; Gold, B.D. Pediatric endoscopy: New information from the PEDS-CORI project. Curr. Gastroenterol. Rep. 2005, 7, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.J.; Cho, I.H.; Yoo, H.J.; Choi, H.; Lee, B.I.; Kim, S.Y.; Jeong, D.C.; Chung, S.Y.; Kang, J.H. Diagnostic yield of pediatric colonoscopies based on presenting symptoms in a secondary hospital. Korean J. Pediatr. Gastroenterol. Nutr. 2011, 14, 368–375. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.W.; Chung, W.C.; Sung, H.J.; Kang, Y.G.; Hong, S.L.; Cho, K.W.; Kang, D.; Lee, I.H.; Jeon, E.J. Current status and clinical impact of pediatric endoscopy in Korea. Korean J. Gastroenterol. 2014, 64, 333–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakkar, K.; El-Serag, H.B.; Mattek, N.; Gilger, M. Complications of pediatric colonoscopy: A five-year multicenter experience. Clin. Gastroenterol. Hepatol. 2008, 6, 515–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, Y.H.; Lee, K.H.; Chan, K.W.; Sihoe, J.D.; Cheung, S.T.; Mou, J.W. Colonoscopy in Hong Kong Chinese children. World J. Gastroenterol. 2010, 16, 1119–1122. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.J.; Cho, S.M.; Choe, B.H.; Jang, H.J.; Choi, K.H.; Kang, B.; Kim, J.E.; Hwang, J.H. Characteristics and Incidence Trends for Pediatric Inflammatory Bowel Disease in Daegu-Kyungpook Province in Korea: A Multi-Center Study. J. Korean Med. Sci. 2018, 33, e132. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, D.E.; Olson, A.D. Colonoscopy or sigmoidoscopy as the initial evaluation of pediatric patients with colitis: A survey of physician behavior and a cost analysis. J. Pediatr. Gastroenterol. Nutr. 1997, 25, 26–31. [Google Scholar] [CrossRef]
- Parra-Blanco, A.; Ruiz, A.; Alvarez-Lobos, M.; Amorós, A.; Gana, J.C.; Ibáñez, P.; Ono, A.; Fujii, T. Achieving the best bowel preparation for colonoscopy. World J. Gastroenterol. 2014, 20, 17709–17726. [Google Scholar] [CrossRef]
- Choe, J.Y.; Choi, S.; Song, K.H.; Jang, H.J.; Choi, K.H.; Yi, D.Y.; Hong, S.J.; Hwang, J.H.; Cho, S.M.; Kim, Y.J.; et al. Incidence and Prevalence Trends of Pediatric Inflammatory Bowel Disease in the Daegu-Kyungpook Province From 2017 to 2020. Front. Pediatr. 2022, 9, 810173. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) (n = 1307) | |
|---|---|
| Male | 805 (61.6) |
| Age at LGI endoscopy (years) | 15.0 (11.0–17.0) |
| Height (cm) | 160.4 (142.5–170.0) |
| Weight (kg) | 50.8 (34.7–60.2) |
| BMI (kg/m2) | 19.0 (16.6–21.8) |
| Year of first LGI endoscopy | |
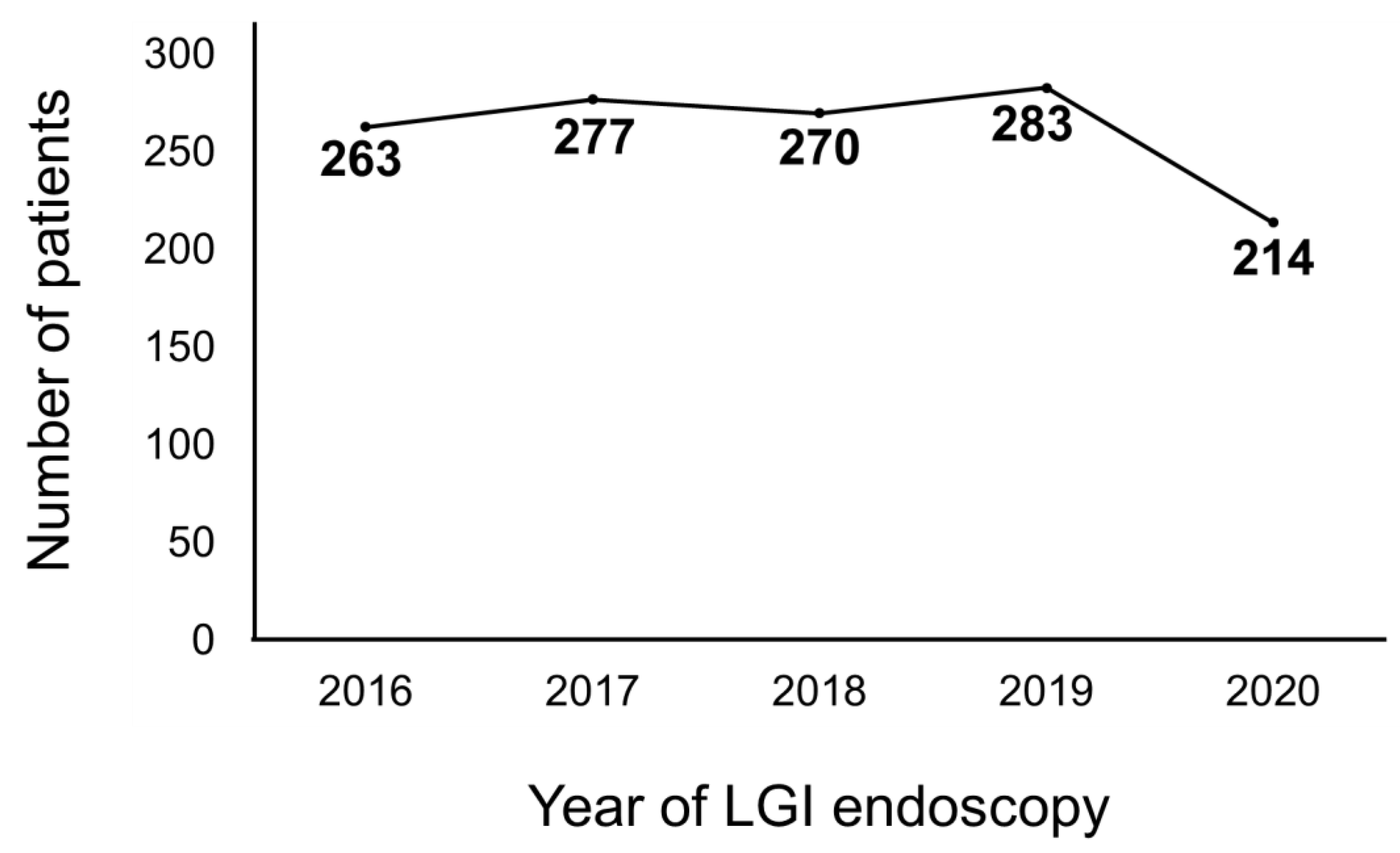
| 2016 | 263 (20.1) |
| 2017 | 277 (21.2) |
| 2018 | 270 (20.7) |
| 2019 | 283 (21.7) |
| 2020 | 213 (16.3) |
| LGI endoscopy type | |
| Colonoscopy | 1041 (79.6) |
| Sigmoidoscopy | 266 (20.4) |
| Sedation/Anesthesia type | |
| Intravenous sedation | 1235 (94.5) |
| General anesthesia | 8 (0.6) |
| None | 64 (4.9) |
| n (%) (n = 1307) | |
|---|---|
| Gastrointestinal bleeding | 494 (37.8) |
| Chronic diarrhea | 463 (35.4) |
| Abdominal pain | 262 (20.0) |
| Weight loss | 22 (1.7) |
| Perianal discharge | 19 (1.5) |
| Growth retardation | 18 (1.4) |
| Anemia | 13 (1.0) |
| Foreign body removal | 7 (0.5) |
| Vomiting | 4 (0.3) |
| Lip pigmentation | 2 (0.2) |
| Hypoalbuminemia | 1 (0.1) |
| Fever of unknown origin | 1 (0.1) |
| Oral ulcer | 1 (0.1) |
| Colonoscopy (n = 1044) | Sigmoidoscopy (n = 263) | Total (n = 1307) | |
|---|---|---|---|
| Normal | 402 (38.5) | 85 (32.3) | 487 (37.3) |
| Crohn’s disease | 273 (26.1) | 9 (3.4) | 282 (21.6) |
| Non-specific colitis | 134 (12.8) | 74 (28.1) | 208 (15.9) |
| Ulcerative colitis | 98 (9.4) | 29 (11.0) | 127 (9.7) |
| Colorectal polyps | 60 (5.7) | 18 (6.8) | 78 (6.0) |
| EGID | 26 (2.5) | 6 (2.3) | 32 (2.4) |
| Pseudomembranous colitis | 4 (0.4) | 16 (6.1) | 20 (1.5) |
| Hemorrhoids | 15 (1.4) | 2 (0.8) | 17 (1.3) |
| Allergic colitis | 0 (0.0) | 12 (4.6) | 12 (0.9) |
| Foreign body | 4 (0.4) | 3 (1.1) | 7 (0.5) |
| Proctitis | 6 (0.6) | 1 (0.4) | 7 (0.5) |
| GVHD | 1 (0.1) | 4 (1.5) | 5 (0.4) |
| Diverticulum/Diverticulitis | 4 (0.4) | 0 (0.0) | 4 (0.3) |
| Solitary rectal ulcer | 3 (0.3) | 1 (0.4) | 4 (0.3) |
| Angiodysplasia | 3 (0.3) | 0 (0.0) | 3 (0.2) |
| Behcet’s disease | 3 (0.3) | 0 (0.0) | 3 (0.2) |
| Sigmoid volvulus | 1 (0.1) | 2 (0.8) | 3 (0.2) |
| Terminal ileitis | 3 (0.3) | 0 (0.0) | 3 (0.2) |
| TB enterocolitis | 2 (0.2) | 0 (0.0) | 2 (0.2) |
| Collagenous colitis | 1 (0.1) | 0 (0.0) | 1 (0.1) |
| Ischemic colitis | 0 (0.0) | 1 (0.4) | 1 (0.1) |
| Microvillous inclusion disease | 1 (0.1) | 0 (0.0) | 1 (0.1) |
| PreCOVID-19 Era (n = 1093) | PostCOVID-19 Era (n = 214) | p-Value | |
|---|---|---|---|
| Indication in accordance to LGI guidelines | 0.261 | ||
| Yes | 864 (79.0) | 177 (82.7) | |
| No | 229 (21.0) | 37 (17.3) |
| Colonoscopy (n = 1041) | Sigmoidoscopy (n = 266) | p-Value | |
|---|---|---|---|
| Male | 649 (62.3) | 156 (58.6) | 0.300 |
| Age at diagnosis (years) | 15.2 (12.9–17.1) | 7.5 (2.5–15.6) | <0.001 |
| Sedation/Anesthesia type | <0.001 | ||
| Intravenous sedation | 1035 (99.4) | 200 (75.2) | |
| General anesthesia | 5 (0.5) | 3 (1.1) | |
| None | 1 (0.1) | 63 (23.7) | |
| Indication: LGI bleeding | 326 (31.3) | 168 (63.2) | <0.001 |
| Indication: chronic diarrhea | 417 (40.1) | 46 (17.3) | <0.001 |
| Diagnosis: IBD | 374 (35.9) | 38 (14.3) | <0.001 |
| Follow-up LGI endoscopy | 207 (19.9) | 34 (12.8) | 0.010 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Sex (male vs. female) | 1.17 (0.89–1.53) | 0.269 | ||
| Age at LGI endoscopy (years) | 1.23 (1.20–1.26) | <0.001 | 1.19 (1.12–1.27) | <0.001 |
| Weight at LGI endoscopy (kg) | 1.06 (1.05–1.07) | <0.001 | 1.00 (0.99–1.02) | 0.773 |
| LGI endoscopy performance year (post- vs. pre-COVID-19) | 1.77 (1.18–2.73) | 0.008 | 1.60 (1.00–2.63) | 0.058 |
| Indication: LGI bleeding (yes vs. no) | 0.27 (0.20–0.35) | <0.001 | 0.56 (0.37–0.83) | 0.005 |
| Indication: chronic diarrhea (yes vs. no) | 3.20 (2.29–4.54) | <0.001 | 1.35 (0.84–2.15) | 0.213 |
| Diagnosis: IBD (yes vs. no) | 3.36 (2.36–4.92) | <0.001 | 1.80 (1.20–2.77) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.W.; Kang, B.; Choi, S.; Choe, B.-H.; Kim, Y.B.; Lee, K.J.; Kim, H.J.; Jang, H.-J.; Choi, S.Y.; Yi, D.Y.; et al. The Changes in Trends of Lower Gastrointestinal Endoscopy Conducted in Children and Adolescents after the COVID-19 Outbreak in Korea. Medicina 2022, 58, 1378. https://doi.org/10.3390/medicina58101378
Lee SW, Kang B, Choi S, Choe B-H, Kim YB, Lee KJ, Kim HJ, Jang H-J, Choi SY, Yi DY, et al. The Changes in Trends of Lower Gastrointestinal Endoscopy Conducted in Children and Adolescents after the COVID-19 Outbreak in Korea. Medicina. 2022; 58(10):1378. https://doi.org/10.3390/medicina58101378
Chicago/Turabian StyleLee, Sang Woo, Ben Kang, Sujin Choi, Byung-Ho Choe, Yu Bin Kim, Kyung Jae Lee, Hyun Jin Kim, Hyo-Jeong Jang, So Yoon Choi, Dae Yong Yi, and et al. 2022. "The Changes in Trends of Lower Gastrointestinal Endoscopy Conducted in Children and Adolescents after the COVID-19 Outbreak in Korea" Medicina 58, no. 10: 1378. https://doi.org/10.3390/medicina58101378