Predictors of Acute Encephalopathy in Patients with COVID-19

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Dropout Criteria
3. Results
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALT | Alanine transaminase |
| aPTT | Activated partial thromboplastin time |
| ARDS | Acute respiratory distress syndrome |
| AST | Aspartate transaminase |
| CPK | Creatine phosphokinase |
| CRP | C-reactive protein |
| CT | Computed tomography |
| DIC | Disseminated intravascular coagulation |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| LDH | Lactate dehydrogenase |
| MERS-CoV | Middle East respiratory syndrome-related coronavirus |
| PCR | Polymerase chain reaction |
| PT | Prothrombin time |
| RNA | Ribonucleic acid |
| ROC | Receiver operating characteristic |
| SARS-CoV | Severe acute respiratory syndrome-related coronavirus |
| WHO | World Health Organization |
| WBCs | White blood cells |
References
- Ellul, M.A.; Benjamin, L.; Singh, B.; Lant, S.; Michael, B.D.; Easton, A.; Kneen, R.; Defres, S.; Sejvar, J.; Solomon, T. Neurological associations of COVID-19. Lancet Neurol. 2020, 19, 767–783. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beach, S.R.; Praschan, N.C.; Hogan, C.; Dotson, S.; Merideth, F.; Kontos, N.; Fricchione, G.L.; Smith, F.A. Delirium in COVID-19: A case series and exploration of potential mechanisms for central nervous system involvement. Gen. Hosp. Psychiatry 2020, 65, 47–53. [Google Scholar] [CrossRef]
- Khan, B.A.; Perkins, A.J.; Prasad, N.K.; Shekhar, A.; Campbell, N.L.; Gao, S.; Wang, S.; Khan, S.H.; Marcantonio, E.R.; Twigg, H.L.; et al. Biomarkers of Delirium Duration and Delirium Severity in the ICU. Crit. Care Med. 2020, 48, 353–361. [Google Scholar] [CrossRef]
- Estabrooks, C.A.; Straus, S.E.; Flood, C.M.; Keefe, J.; Armstrong, P.; Donner, G.J.; Boscart, V.; Ducharme, F.; Silvius, J.L.; Wolfson, M.C. Restoring trust: COVID-19 and the future of long-term care in Canada. Facets 2020, 5, 651–691. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Martinotti, G.; Barlati, S.; Prestia, D.; Palumbo, C.; Giordani, M.; Cuomo, A.; Miuli, A.; Paladini, C.; Amore, M.; Bondi, E.; et al. Psychomotor agitation and hyperactive delirium in COVID-19 patients treated with aripiprazole 9.75 mg/1.3 mL immediate release. Psychopharmacology 2020, 237, 3497–3501. [Google Scholar] [CrossRef] [PubMed]
- Mat, L.N.I.; Sulaiman, W.A.W.; Kee, H.F.; Baharin, M.A.S.; Ghenesan, S.; Ishak, S.N.; Abidin, W.F.Z.; Daud, N.L.F.; Yun, T.H. Clinical manifestations of delirium in elderly. MNJ (Malang Neurol. J.) 2018, 4, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Mizuguchi, M. Influenza encephalopathy and related neuropsychiatric syndromes. Influ. Other Respir. Viruses 2013, 7, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Kotfis, K.; Roberson, S.W.; Wilson, J.; Pun, B.; Ely, E.W.; Jeżowska, I.; Jezierska, M.; Dabrowski, W. COVID-19: What do we need to know about ICU delirium during the SARS-CoV-2 pandemic? Anaesthesiol. Intensive Ther. 2020, 52, 132–138. [Google Scholar] [CrossRef]
- Yadav, H.; Kor, D.J. Platelets in the pathogenesis of acute respiratory distress syndrome. Am. J. Physiol. Cell. Mol. Physiol. 2015, 309, L915–L923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prokop, M.; van Everdingen, W.; van Rees Vellinga, T.; van Ufford, J.Q.; Stöger, L.; Beenen, L.; Geurts, B.; Gietema, H.; Krdzalic, J.; Schaefer-Prokop, C.; et al. CO-RADS–A categorical CT assessment scheme for patients with suspected COVID-19: Definition and evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef] [PubMed]
- Slooter, A.J.; Otte, W.M.; Devlin, J.W.; Arora, R.C.; Bleck, T.P.; Claassen, J.; Duprey, M.S.; Ely, E.W.; Kaplan, P.W.; Latronico, N.; et al. Updated nomencla-ture of delirium and acute encephalopathy: Statement of ten Societies. Intensive Care Med. 2020, 46, 1020–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. Criteria for Releasing COVID-19 Patients from Isolation: Scientific Brief, 17 June 2020 (No. WHO/2019-nCoV/Sci_Brief/Discharge_From_Isolation/2020.1); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Hani, C.; Trieu, N.; Saab, I.; Dangeard, S.; Bennani, S.; Chassagnon, G.; Revel, M.-P. COVID-19 pneumonia: A review of typical CT findings and differential diagnosis. Diagn. Interv. Imaging 2020, 101, 263–268. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Yum, S.K.; Moon, C.-J.; Youn, Y.-A.; Sung, I.K. Changes in lactate dehydrogenase are associated with central gray matter lesions in newborns with hypoxic-ischemic encephalopathy. J. Matern. Neonatal Med. 2017, 30, 1177–1181. [Google Scholar] [CrossRef] [PubMed]
- Sweetman, D.; Kelly, L.A.; Zareen, Z.; Nolan, B.; Murphy, J.; Boylan, G.; Donoghue, V.; Molloy, E.J. Coagulation Profiles Are Associated With Early Clinical Outcomes in Neonatal Encephalopathy. Front. Pediatr. 2019, 7, 399. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.-Y.; Huang, C.-C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month Follow-up Study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef] [PubMed]
- Vargas, M.; Servillo, G. Serum lactate dehydrogenase as an early marker of posterior reversible encephalopathy syndrome: Keep your eyes open on the score of severity brain oedema. Anaesth. Intensive Care 2013, 41, 436–437. [Google Scholar]
- Lv, C.; Gao, B. Serum lactate dehydrogenase as a predictor of outcome in posterior reversible encephalopathy syndrome: Imperative to unify. Am. J. Neuroradiol. 2015, 36, E29–E30. [Google Scholar] [CrossRef] [Green Version]
- Scullen, T.; Keen, J.; Mathkour, M.; Dumont, A.S.; Kahn, L. COVID-19 associated encephalopathies and cerebrovascular disease: The New Orleans experience. World Neurosurg. 2020, 141, e437–e446. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Control Group (n = 20) | Main Group (n = 10) | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 47.9 ± 7.3 | 51.0 ± 10.5 | 0.417 |
| Sex, women (n, %) | 11 (55%) | 3 (30%) | 0.260 |
| Arterial hypertension (AH) (n, %) | 8 (40%) | 7 (70%) | 0.245 |
| Type 2 diabetes mellitus (DM) (n, %) | 3 (15%) | 2 (20%) | 0.999 |
| Obesity (body mass index > 30 kg/m2) (n, %) | 12 (60%) | 4 (40%) | 0.442 |
| Chronic renal failure (n, %) | 0 (0%) | 0 (0%) | - |
| Peripheral artery disease (n, %) | 0 (0%) | 0 (0%) | - |
| Lung disease (n, %) | 0 (0%) | 1 (10%) | 0.333 |
| Parameters | Group without Encephalopathy (n = 20) | Group with Encephalopathy (n = 10) | p-Value |
|---|---|---|---|
| Degree of severity of coronavirus pneumonia (n, %) | <0.001 | ||
| Grade 0–1 | 0 | 0 | |
| Grade 2 | 7 (35%) | 0 | |
| Grade 3 | 11 (55%) | 2 (20%) | |
| Grade 4 | 2 (10%) | 8 (80%) | |
| Severity of the right lung damage, % (Me (Q25%; Q75%)) | 50 (40; 75) | 75 (75; 80) | 0.003 |
| Severity of the left lung damage, % (Me (Q25%; Q75%)) | 50 (50; 75) | 75 (75; 80) | <0.001 |
| Smell disturbances (n, %) | 7 (35%) | 3 (30%) | 0.036 |
| Taste disturbances (n, %) | 4 (20%) | 2 (20%) | 0.302 |
| Parameters | Patients without Encephalopathy (n = 19) | Patients with Encephalopathy (n = 2) | p-Value |
|---|---|---|---|
| Mean awake SpO2 | 93.1 (92.6; 94.2) | 93.9 (91.4; 96.3) | 0.853 |
| Minimal awake SpO2 | 78.5 (73; 84) | 76.0 (72; 80) | 0.589 |
| Mean asleep SpO2 | 91.8 (86.6; 93.7) | 93.2 (90.5; 95.9) | 0.589 |
| Minimal asleep SpO2 | 76.5 (71; 82) | 84 (79; 89) | 0.263 |
| Oxygen desaturation index | 23.4 (9.3; 27.1) | 4.65 (1.5; 7.8) | 0.095 |
| Parameters | Index of Slow-Wave Activity | Mean N20 Peak Latency, Right | Mean N20 Peak Latency, Left | Mean Peak-to-Peak Amplitude of P14/N20, Right | Mean Peak-to-Peak Amplitude of P14/N20, Left |
|---|---|---|---|---|---|
| Mean awake SpO2 | −0.079 | −0.201 | −0.225 | 0.015 | 0.132 |
| Minimal awake SpO2 | 0.175 | 0.091 | 0.094 | 0.182 | 0.007 |
| Mean asleep SpO2 | 0.088 | −0.146 | −0.155 | −0.509 | −0.161 |
| Minimal asleep SpO2 | 0.170 | −0.332 | −0.371 | −0.027 | 0.101 |
| Oxygen desaturation index | −0.256 | −0.230 | −0.122 | 0.347 | 0.267 |
| Parameters | Group without Encephalopathy (n = 20) | Group with Encephalopathy (n = 10) | p-Value |
|---|---|---|---|
| White blood cells, WBCs (×109/L) | 6 (4; 6) | 7 (5; 10) | 0.120 |
| Lymphocytes (×109/L) | 1.07 (0.82; 1.44) | 0.69 (0.44; 1.20) | 0.044 |
| Platelets (×109/L) | 195 (158; 250) | 229 (187; 271) | 0.142 |
| Alanine transaminase, ALT, U/L | 38 (24; 57) | 27 (20; 40) | 0.267 |
| Aspartate transaminase, AST, U/L | 38 (31; 50) | 48 (30; 53) | 0.475 |
| Lactate dehydrogenase, LDH, U/L | 310 (237; 445) | 521 (347; 751) | 0.022 |
| Creatinine, μmol/L | 98 (81; 105) | 76 (71; 89) | 0.149 |
| C-reactive protein, CRP, μg/L | 81 (39; 113) | 171 (60; 277) | 0.155 |
| Ferritin, μg/L | 589 (181; 669) | 605 (357; 668) | 0.681 |
| D-dimer, μg/mL | 0.55 (0.38; 0.65) | 1.16 (0.70; 2.53) | 0.019 |
| Prothrombin time, PT, s | 14 (13; 14) | 15 (14; 15) | 0.031 |
| Activated partial thromboplastin time, aPTT, s | 34 (32; 38) | 37 (31; 44) | 0.530 |
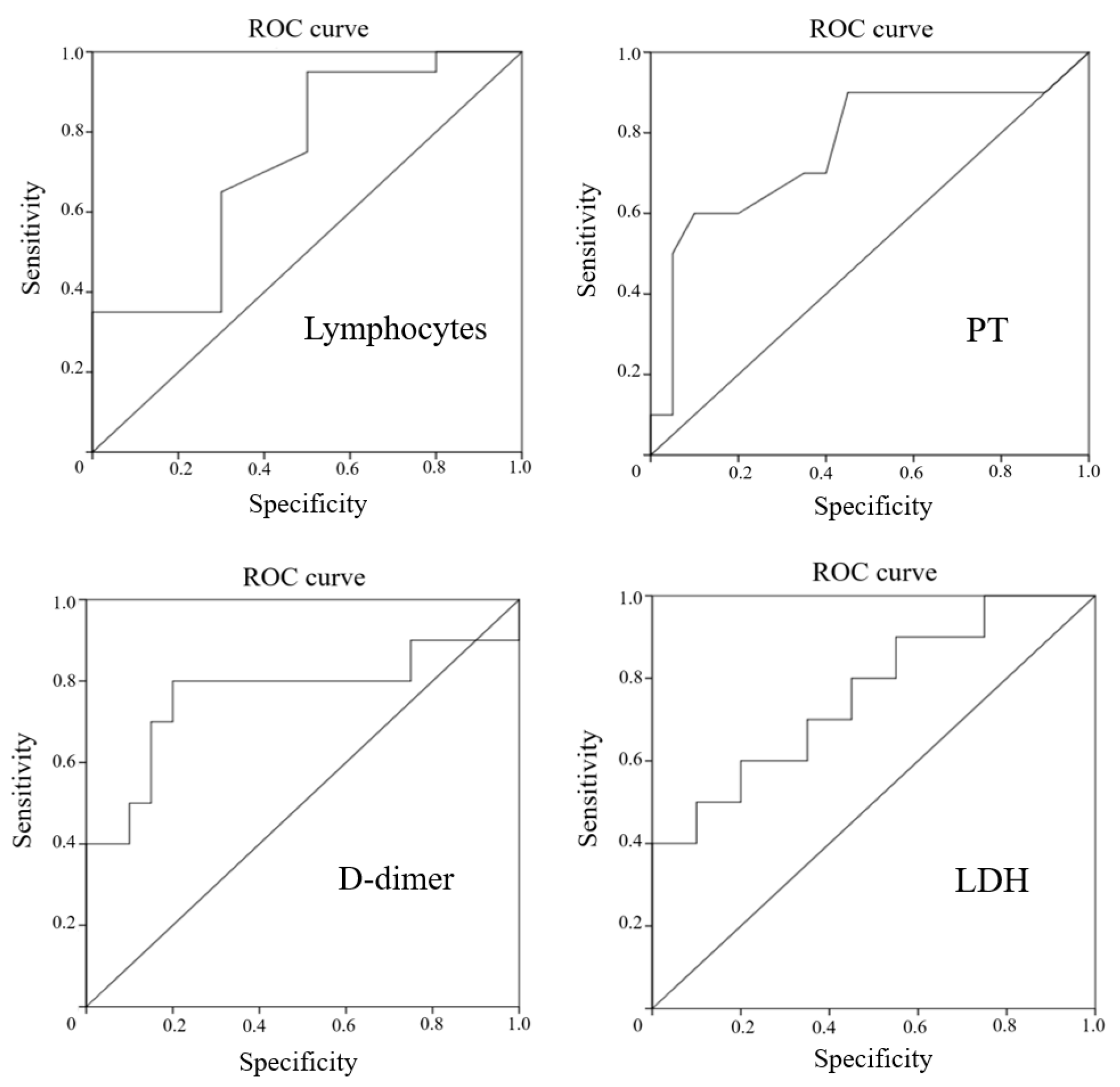
| Predictors | AUC | 95% CI, Boundary | Cutoff Values | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Lactate dehydrogenase, LDH | 0.760 | 0.573 | 0.947 | 476.5 | 60% | 80% |
| D-dimer | 0.765 | 0.547 | 0.983 | 0.68 | 80% | 80% |
| Prothrombin time, PT | 0.765 | 0.565 | 0.965 | 14.45 | 60% | 90% |
| Lymphocytes | 0.730 | 0.531 | 0.929 | 0.56 | 95% | 50% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinogradov, O.I.; Ogarkova, T.K.; Shamtieva, K.V.; Alexandrov, P.V.; Mushba, A.V.; Kanshina, D.S.; Yakovleva, D.V.; Surma, M.A.; Nikolaev, I.S.; Gorst, N.K. Predictors of Acute Encephalopathy in Patients with COVID-19. J. Clin. Med. 2021, 10, 4821. https://doi.org/10.3390/jcm10214821
Vinogradov OI, Ogarkova TK, Shamtieva KV, Alexandrov PV, Mushba AV, Kanshina DS, Yakovleva DV, Surma MA, Nikolaev IS, Gorst NK. Predictors of Acute Encephalopathy in Patients with COVID-19. Journal of Clinical Medicine. 2021; 10(21):4821. https://doi.org/10.3390/jcm10214821
Chicago/Turabian StyleVinogradov, Oleg I., Tatyana K. Ogarkova, Kamila V. Shamtieva, Pavel V. Alexandrov, Astanda V. Mushba, Daria S. Kanshina, Daria V. Yakovleva, Maria A. Surma, Ilia S. Nikolaev, and Nadezhda Kh. Gorst. 2021. "Predictors of Acute Encephalopathy in Patients with COVID-19" Journal of Clinical Medicine 10, no. 21: 4821. https://doi.org/10.3390/jcm10214821