

Neuroimmunoendocrinology of SARS-CoV-2 Infection

 , ,
, , {kind=link}
Abstract
:1. Introduction
2. Methods
3. Involvement of Central Nervous System and Hypothalamic-Pituitary Axis in SARS-CoV-2 Infection
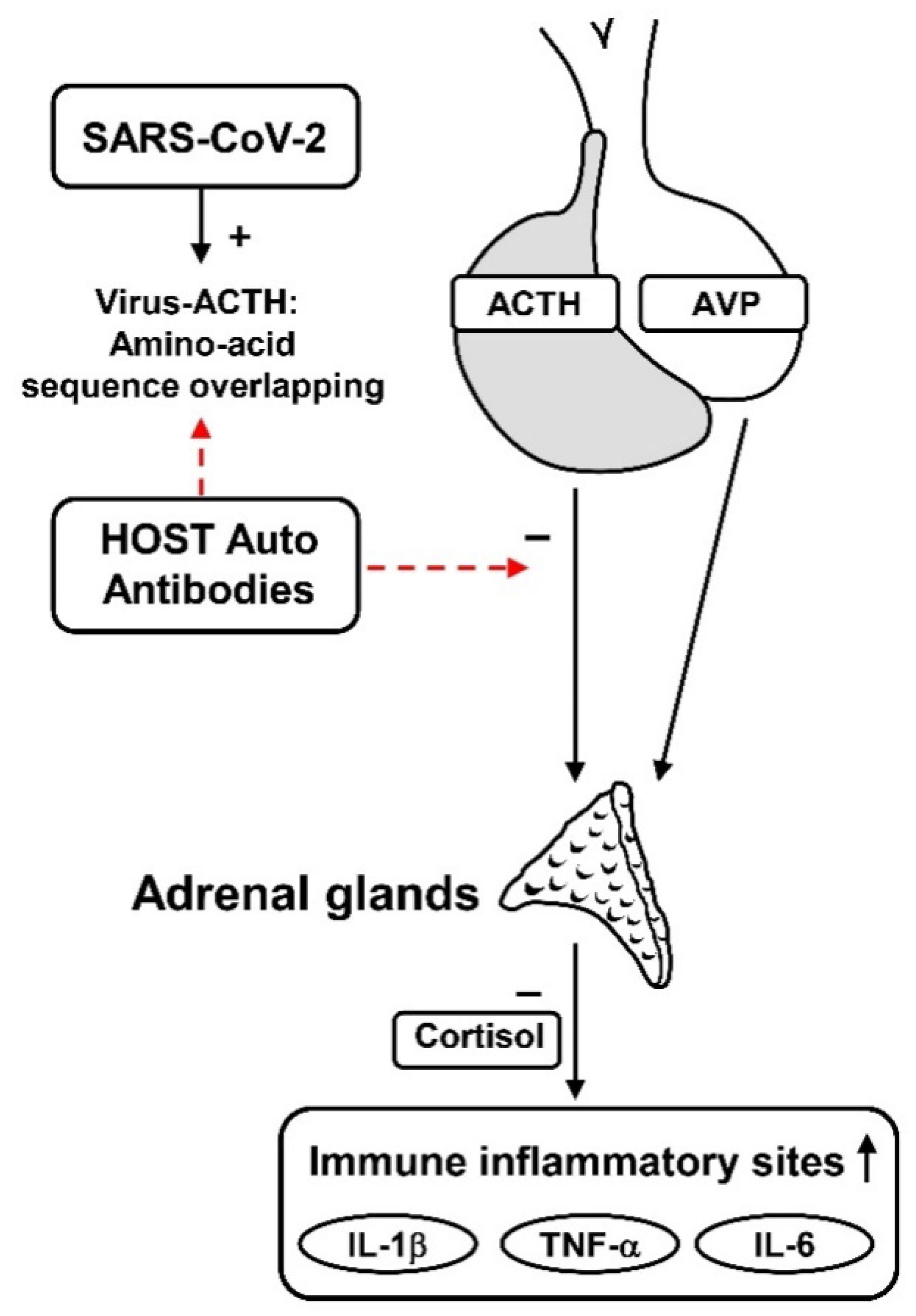
4. Hypothalamic-Pituitary Autoimmunity in SARS-CoV-2 Infection
5. Anti-Pituitary and Anti-Hypothalamus Antibodies Detection
6. May the Autoimmune/Inflammatory Syndrome Induced by Adjuvants (ASIA) of the SARS-CoV-2 Vaccine Evoke Neuro-Immune-Endocrine Disorders?
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Health Emergency Dashboard. Available online: https://extranet.who.int/publicemergency (accessed on 19 May 2022).
- Medina-Enríquez, M.M.; Lopez-León, S.; Carlos-Escalante, J.A.; Aponte-Torres, Z.; Cuapio, A.; Wegman-Ostrosky, T. ACE2: The molecular doorway to SARS-CoV-2. Cell Biosci. 2020, 10, 148. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Longo, M.; Scappaticcio, L.; Petrizzo, M.; Castaldo, F.; Sarnataro, A.; Forestiere, D.; Caiazzo, F.; Bellastella, G.; Maiorino, M.I.; Capuano, A.; et al. Glucose control in home-isolated adults with type 1 diabetes affected by COVID-19 using continuous glucose monitoring. J. Endocrinol. Investig. 2022, 45, 445–452. [Google Scholar] [CrossRef]
- Bellastella, G.; Maiorino, M.I.; Esposito, K. Endocrine complications of COVID-19: What happens to the thyroid and adrenal glands? J. Endocrinol. Investig. 2020, 43, 1169–1170. [Google Scholar] [CrossRef]
- Chen, W.; Tian, Y.; Li, Z.; Zhu, J.; Wei, T.; Lei, J. Potential Interaction between SARS-CoV-2 and Thyroid: A Review. Endocrinology 2021, 162, bqab004. [Google Scholar] [CrossRef]
- Deng, S.Q.; Peng, H.J. Characteristics of and Public Health Responses to the Coronavirus Disease 2019 Outbreak in China. J. Clin. Med. 2020, 9, 575. [Google Scholar] [CrossRef] [Green Version]
- Kandasamy, M.; Radhakrishnan, R.K.; PoornimaiAbirami, G.P.; Roshan, S.A.; Yesudhas, A.; Balamuthu, K.; Prahalathan, C.; Shanmugaapriya, S.; Moorthy, A.; Essa, M.M.; et al. Possible Existence of the Hypothalamic-Pituitary-Hippocampal (HPH) Axis: A Reciprocal Relationship Between Hippocampal Specific Neuroestradiol Synthesis and Neuroblastosis in Ageing Brains with Special Reference to Menopause and Neurocognitive Disorders. Neurochem. Res. 2019, 44, 1781–1795. [Google Scholar] [CrossRef]
- Payus, A.O.; Liew Sat Lin, C.; Mohd Noh, M.; Jeffree, M.S.; Ali, R.A. SARS-CoV-2 infection of the nervous system: A review of the literature on neurological involvement in novel coronavirus disease-(COVID-19). Bosn. J. Basic Med. Sci. 2020, 20, 283–292. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain. Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host-Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef]
- Frara, S.; Allora, A.; Castellino, L.; di Filippo, L.; Loli, P.; Giustina, A. COVID-19 and the pituitary. Pituitary 2021, 24, 465–481. [Google Scholar] [CrossRef]
- Pal, R. COVID-19, hypothalamo-pituitary-adrenal axis and clinical implications. Endocrine 2020, 68, 251–252. [Google Scholar] [CrossRef]
- Chigr, F.; Merzouki, M.; Najimi, M. Autonomic Brain Centers and Pathophysiology of COVID-19. ACS Chem. Neurosci. 2020, 11, 1520–1522. [Google Scholar] [CrossRef]
- Puig-Domingo, M.; Marazuela, M.; Yildiz, B.O.; Giustina, A. COVID-19 and endocrine and metabolic diseases. An updated statement from the European Society of Endocrinology. Endocrine 2021, 72, 301–316. [Google Scholar] [CrossRef]
- Mongioì, L.M.; Barbagallo, F.; Condorelli, R.A.; Cannarella, R.; Aversa, A.; La Vignera, S.; Calogero, A.E. Possible long-term endocrine-metabolic complications in COVID-19: Lesson from the SARS model. Endocrine 2020, 68, 467–470. [Google Scholar] [CrossRef]
- Fitzek, A.; Gerling, M.; Püschel, K.; Saeger, W. Post-mortem histopathology of pituitary and adrenals of COVID-19 patients. Leg. Med. 2022, 57, 102045. [Google Scholar] [CrossRef]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: Implications for pathogenesis and virus transmission pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- Frara, S.; Loli, P.; Allora, A.; Santini, C.; di Filippo, L.; Mortini, P.; Fleseriu, M.; Giustina, A. COVID-19 and hypopituitarism. Rev. Endocr. Metab. Disord. 2022, 23, 215–231. [Google Scholar] [CrossRef]
- Han, T.; Kang, J.; Li, G.; Ge, J.; Gu, J. Analysis of 2019-nCoV receptor ACE2 expression in different tissues and its significance study. Ann. Transl. Med. 2020, 8, 1077. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M. COVID-19 and the endocrine system: Exploring the unexplored. J. Endocrinol. Investig. 2020, 43, 1027–1031. [Google Scholar] [CrossRef]
- Ramos, A.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Joaquín, C.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Ros, M.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Martín, M.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Cachero, M.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Sospedra, M.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Martínez, E.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Sendrós, M.J.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Sánchez-Migallón, J.M.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain); Puig-Domingo, M.; (Endocrinology and Nutrition Service, Hospital Universitari Germans Trias i Pujol, Badalona, Spain). Nutritional Support in COVID-19 Patients 60th Congress of the Spanish Society of Endocrinology and Nutrition 2021. (Oral Communication).
- Vassiliadi, D.A.; Vassiliou, A.G.; Ilias, I.; Tsagarakis, S.; Kotanidou, A.; Dimopoulou, I. Pituitary-Adrenal Responses and Glucocorticoid Receptor Expression in Critically Ill Patients with COVID-19. Int. J. Mol. Sci. 2021, 22, 11473. [Google Scholar] [CrossRef] [PubMed]
- Berger, I.; Werdermann, M.; Bornstein, S.R.; Steenblock, C. The adrenal gland in stress-adaptation on a cellular level. J. Steroid Biochem. Mol. Biol. 2019, 190, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Wheatland, R. Molecular mimicry of ACTH in SARS—Implications for corticosteroid treatment and prophylaxis. Med. Hypotheses 2004, 63, 855–856. [Google Scholar] [CrossRef] [PubMed]
- Van den Berghe, G. Adrenal function/dysfunction in critically ill patients: A concise narrative review of recent novel insights. J. Anesth. 2021, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Marino, L.O.; Souza, H.P. Dysfunction of the hypothalamic-pituitary-adrenal axis in critical illness: A narrative review for emergency physicians. Eur. J. Emerg. Med. 2020, 27, 406–413. [Google Scholar] [CrossRef]
- Das, L.; Dutta, P.; Walia, R.; Mukherjee, S.; Suri, V.; Puri, G.D.; Mahajan, V.; Malhotra, P.; Chaudhary, S.; Gupta, R.; et al. Spectrum of Endocrine Dysfunction and Association with Disease Severity in Patients with COVID-19: Insights from a Cross-Sectional, Observational Study. Front. Endocrinol. 2021, 12, 645787. [Google Scholar] [CrossRef]
- Leow, M.K.; Kwek, D.S.; Ng, A.W.; Ong, K.C.; Kaw, G.J.; Lee, L.S. Hypocortisolism in survivors of severe acute respiratory syndrome (SARS). Clin. Endocrinol. 2005, 63, 197–202. [Google Scholar] [CrossRef]
- Gonen, M.S.; De Bellis, A.; Durcan, E.; Bellastella, G.; Cirillo, P.; Scappaticcio, L.; Longo, M.; Bircan, B.E.; Sahin, S.; Sulu, C.; et al. Assessment of Neuroendocrine Changes and Hypothalamo-Pituitary Autoimmunity in Patients with COVID-19. Horm. Metab. Res. 2022, 54, 153–161. [Google Scholar] [CrossRef]
- Tanriverdi, F.; De Bellis, A.; Teksahin, H.; Alp, E.; Bizzarro, A.; Sinisi, A.A.; Bellastella, G.; Paglionico, V.A.; Bellastella, A.; Unluhizarci, K.; et al. Prospective investigation of pituitary functions in patients with acute infectious meningitis: Is acute meningitis induced pituitary dysfunction associated with autoimmunity? Pituitary 2012, 15, 579–588. [Google Scholar] [CrossRef]
- De Bellis, A.; Bellastella, G.; Pernice, V.; Cirillo, P.; Longo, M.; Maio, A.; Scappaticcio, L.; Maiorino, M.I.; Bellastella, A.; Esposito, K.; et al. Hypothalamic-Pituitary Autoimmunity and Related Impairment of Hormone Secretions in Chronic Fatigue Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, e5147–e5155. [Google Scholar]
- Zhang, Z.; Zoltewicz, J.S.; Mondello, S.; Newsom, K.J.; Yang, Z.; Yang, B.; Kobeissy, F.; Guingab, J.; Glushakova, O.; Robicsek, S.; et al. Human traumatic brain injury induces autoantibody response against glial fibrillary acidic protein and its breakdown products. PLoS ONE 2014, 9, e92698. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Yang, X.O. TH17 responses in cytokine storm of COVID-19: An emerging target of JAK2 inhibitor Fedratinib. J. Microbiol. Immunol. Infect. 2020, 53, 368–370. [Google Scholar] [CrossRef] [PubMed]
- Lania, A.; Sandri, M.T.; Cellini, M.; Mirani, M.; Lavezzi, E.; Mazziotti, G. Thyrotoxicosis in patients with COVID-19: The THYRCOV study. Eur. J. Endocrinol. 2020, 183, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Ye, Y.X.; Yao, H.; Sun, L.Q.; Wang, A.S.; Wang, Z.Y. Evaluation and observation of serum thd parathyroid hormone in patients with severe acute respiratory syndrome. Chin. J. Antituberculosis 2003, 25, 232–234. [Google Scholar]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. Bmj 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Zhou, W.; Xu, W. Thyroid Function Analysis in 50 Patients with COVID-19: A Retrospective Study. Thyroid Off. J. Am. Thyroid. Assoc. 2021, 31, 8–11. [Google Scholar] [CrossRef]
- Leszek, J.; Barreto, G.E.; Gąsiorowski, K.; Koutsouraki, E.; ÁvilaRodrigues, M.; Aliev, G. Inflammatory mechanisms and oxidative stress as key factors responsible for progression of neurodegeneration: Role of brain innate immune system. CNS Neurol. Disord. Drug Targets 2016, 15, 329–336. [Google Scholar] [CrossRef]
- Aitken, R.J.; Roman, S.D. Antioxidant systems and oxidative stress in the testes. Oxid. Med. Cell. Longev. 2008, 1, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Selvaraj, K.; Ravichandran, S.; Krishnan, S.; Radhakrishnan, R.K.; Manickam, N.; Kandasamy, M. Testicular Atrophy and Hypothalamic Pathology in COVID-19: Possibility of the Incidence of Male Infertility and HPG Axis Abnormalities. Reprod. Sci. 2021, 28, 2735–2742. [Google Scholar] [CrossRef]
- Sengupta, P.; Dutta, S. COVID-19 and hypogonadism: Secondary immune responses rule-over endocrine mechanisms. Hum. Fertil. 2021, 13, 1–6. [Google Scholar] [CrossRef]
- De Bellis, A.; Colao, A.; Di Salle, F.; Muccitelli, V.I.; Iorio, S.; Perrino, S.; Pivonello, R.; Coronella, C.; Bizzarro, A.; Lombardi, G.; et al. A longitudinal study of vasopressin cell antibodies, posterior pituitary function, and magnetic resonance imaging evaluations in subclinical autoimmune central diabetes insipidus. J. Clin. Endocrinol. Metab. 1999, 84, 3047–3051. [Google Scholar] [CrossRef] [PubMed]
- Gluck, M.; Scherbaum, W.A. Substrate specificity for the detection of autoantibodies to anterior pituitary cells in human sera. Horm. Metab. Res. 1990, 22, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Maghnie, M.; Lorini, R.; Severi, F. Antipituitary antibodies in patients with pituitary abnormalities and hormonal deficiency. Clin. Endocrinol. 1994, 40, 809–810. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, P.; Newschaffer, C.; Olivi, A.; Pomper, M.G.; Burger, P.C.; Rose, N.R. Autoimmune hypophysitis. Endocr. Rev. 2005, 26, 599–614. [Google Scholar] [CrossRef] [Green Version]
- Caturegli, P.; Lupi, I.; Landek-Salgado, M.; Kimura, H.; Rose, N.R. Pituitary autoimmunity: 30 years later. Autoimmun. Rev. 2008, 7, 631–637. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.J.; Bensing, S.; Burns, C.; Robinson, P.J.; Kasperlik-Zaluska, A.A.; Scott, R.J.; Kämpe, O.; Crock, P.A. Identification of TPIT and other novel autoantigens in lymphocytic hypophysitis: Immunoscreening of a pituitary cDNA library and development of immunoprecipitation assays. Eur. J. Endocrinol. 2012, 166, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Tatsumi, K.I.; Kimuri, M.; Takano, T.; Murakani, Y.; Takao, T.; Hashimoto, K.; Kato, Y.; Amino, N. Detection of autoantibodies against the pituitary-specific protein in patients with lymphocytic hypophysitis. Eur. J. Endocrinol. 2002, 147, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Crock, P. Cytosolic autoantigens in lymphocytic hypophysitis. J. Clin. Endocrinol. Metab. 1998, 83, 609–618. [Google Scholar] [CrossRef]
- Tanaka, S.; Tatsumi, K.I.; Takano, T.; Murakami, Y.; Takao, T.; Yamakita, N.; Tahara, S.; Teramoto, A.; Hashimoto, K.; Kato, Y.; et al. Anti-alpha-enolase antibodies in pituitary disease. Endocr. J. 2003, 50, 697–702. [Google Scholar] [CrossRef] [Green Version]
- Bensing, S.; Fetissov, S.O.; Mulder, J.; Perheentupa, J.; Gustafsson, J.; Husebye, E.S.; Oscarson, M.; Ekwall, O.; Crock, P.A.; Hokfelt, T.; et al. Pituitary autoantibodies in autoimmune polyendocrine syndrome type 1. Proc. Natl. Acad. Sci. USA 2007, 104, 949–954. [Google Scholar] [CrossRef] [Green Version]
- Lupi, I.; Broman, K.W.; Tzou, S.C.; Gutenberg, A.; Martino, E.; Caturegli, P. Novel autoantigens in autoimmune hypophysitis. Clin. Endocrinol. 2008, 69, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Bottazzo, G.F.; Pouplard, A.; Florin-Christensen, A.; Doniach, D. Autoantibodies to prolactin-secreting cells of human pituitary. Lancet 1975, 2, 97–101. [Google Scholar] [CrossRef]
- Bottazzo, G.F.; McIntosh, C.; Stanford, W.; Preece, M. Growth hormone cell antibodies and partial growth hormone deficiency in a girl with Turner’s syndrome. Clin. Endocrinol. 1980, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pouplard, A. Pituitary autoimmunity. Horm. Res. 1982, 16, 289–297. [Google Scholar] [CrossRef]
- Mayfield, R.K.; Levine, J.H.; Gordon, L.; Powers, J.; Galbraith, R.M.; Rawe, S.E. Lymphoid adenohypophysitis presenting as a pituitary tumor. Am. J. Med. 1980, 69, 619–623. [Google Scholar]
- Wild, R.A.; Kepley, M. Lymphocytic hypophysitis in a patient with amenorrhea and hyperprolactinemia. A case report. J. Reprod. Med. 1986, 31, 211–216. [Google Scholar]
- Komatsu, M.; Kondo, T.; Yamauchi, K.; Yokokawa, N.; Ichikawa, K.; Ishihara, M.; Aizawa, T.; Yamada, T.; Imai, Y.; Tanaka, K. Antipituitary antibodies in patients with the primary empty sella syndrome. J. Clin. Endocrinol. Metab. 1988, 67, 633–638. [Google Scholar] [CrossRef]
- Mau, M.; Phillips, T.M.; Ratner, R.E. Presence of anti-pituitary hormone antibodies in patients with empty sella syndrome and pituitary tumours. Clin. Endocrinol. 1993, 8, 495–500. [Google Scholar] [CrossRef]
- Crock, P.; Salvi, M.; Miller, A.; Wall, J.; Guyda, H. Detection of anti-pituitary autoantibodies by immunoblotting. J. Immunol. Methods. 1993, 162, 31–40. [Google Scholar] [CrossRef]
- O’Dwyer, D.T.; Clifton, V.; Hall, A.; Smith, R.; Robinson, P.J.; CrocK, P.A. Pituitary autoantibodies in lymphocytic hypophysitis target both gamma- and alpha-Enolase—A link with pregnancy? Arch. Physiol. Biochem. 2002, 110, 94–98. [Google Scholar] [CrossRef]
- De Bellis, A.; Sinisi, A.A.; Pane, E.; Dello Iacovo, A.; Bellastella, G.; Di Scala, G.; Falorni, A.; Giavoli, C.; Gasco, V.; Giordano, R.; et al. Pituitary 123 Author’s personal copy. Involvement of hypothalamus autoimmunity in patients with autoimmune hypopituitarism: Role of antibodies to hypothalamic cells. Italian Autoimmune Hypophysitis Network Group. J. Clin. Endocrinol. Metab. 2012, 97, 3684–3690. [Google Scholar] [CrossRef] [PubMed]
- Vera-Lastra, O.; Navarro, A.O.; Cruz Dominguez, M.P.; Medina, G.; Sanchez-Valadez, T.I.; Jara, L.J. Two cases os Graves’ disease following SARS-Cov2 vaccination: An autoimmune/Inflammatory autoimmunity/ induced by adjuvants. Thyroid 2021, 31, 1436–1439. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.W.; Lee, K.K.; Lee, C.H.; Lee, A.C.H.; Hung, I.F.N.; Tan, K.C.B. Development of Graves’ disease after SARS-Cov2 mRNA vaccination: A case report and literature review. Front. Public Health 2021, 9, 778964. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Howland, T. Graves’ diseases following COVID-19 vaccination. Cureus 2022, 14, e2441-48. [Google Scholar] [CrossRef] [PubMed]
- Pujol, A.; Gomez, L.A.; Gallegos, C.; Nicolau, J.; Sanchís, P.; González-Freire, M.; López-González, Á.A.; Dotres, K.; Masmiquel, L. Thyroid as target of adjuvant autoimmunity/inflammatory syndrome due to mRNA-based SARS-CoV2 vaccination from Graves’disease to silent thyroiditis. J. Endocrinol. Investig. 2022, 45, 875–882. [Google Scholar] [CrossRef]
- Patrizio, A.; Ferrari, S.M.; Antonelli, A.; Fallale, P. A case of Graves’ disease and type 1 diabetes mellitus following SARS-CoV2 vaccination. J. Autoimmun. 2021, 125, 102738. [Google Scholar] [CrossRef]
- Morita, S.; Tsuji, T.; Kishimoto, S.; Uraki, S.; Takeshima, K.; Iwakura, H.; Furuta, H.; Nishi, M.; Inaba, H.; Matsuoka, T.A. Isolated ACTH deficiency following immunization with BNT162b2: iSARS-CoV-2 vaccine: A case report. BMC Musculoskelet. Disord. 2022, 22, 185. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellastella, G.; Cirillo, P.; Carbone, C.; Scappaticcio, L.; Maio, A.; Botta, G.; Tomasuolo, M.; Longo, M.; Pontillo, A.; Bellastella, A.; et al. Neuroimmunoendocrinology of SARS-CoV-2 Infection. Biomedicines 2022, 10, 2855. https://doi.org/10.3390/biomedicines10112855
Bellastella G, Cirillo P, Carbone C, Scappaticcio L, Maio A, Botta G, Tomasuolo M, Longo M, Pontillo A, Bellastella A, et al. Neuroimmunoendocrinology of SARS-CoV-2 Infection. Biomedicines. 2022; 10(11):2855. https://doi.org/10.3390/biomedicines10112855
Chicago/Turabian StyleBellastella, Giuseppe, Paolo Cirillo, Carla Carbone, Lorenzo Scappaticcio, Antonietta Maio, Graziella Botta, Maria Tomasuolo, Miriam Longo, Alessandro Pontillo, Antonio Bellastella, and et al. 2022. "Neuroimmunoendocrinology of SARS-CoV-2 Infection" Biomedicines 10, no. 11: 2855. https://doi.org/10.3390/biomedicines10112855