
A Review of the Role of Imaging Modalities in the Evaluation of Viral Myocarditis with a Special Focus on COVID-19-Related Myocarditis


Abstract
:1. Introduction
2. Role of Imaging Modalities in Myocarditis
2.1. Echocardiography
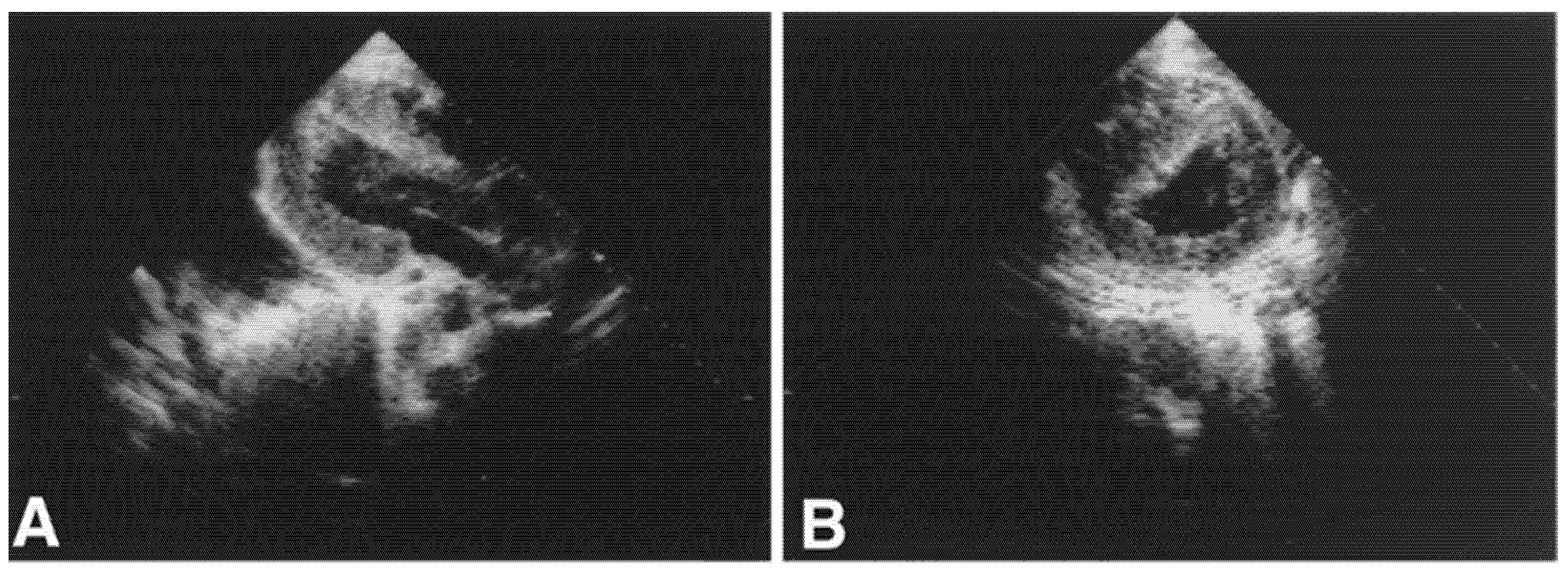
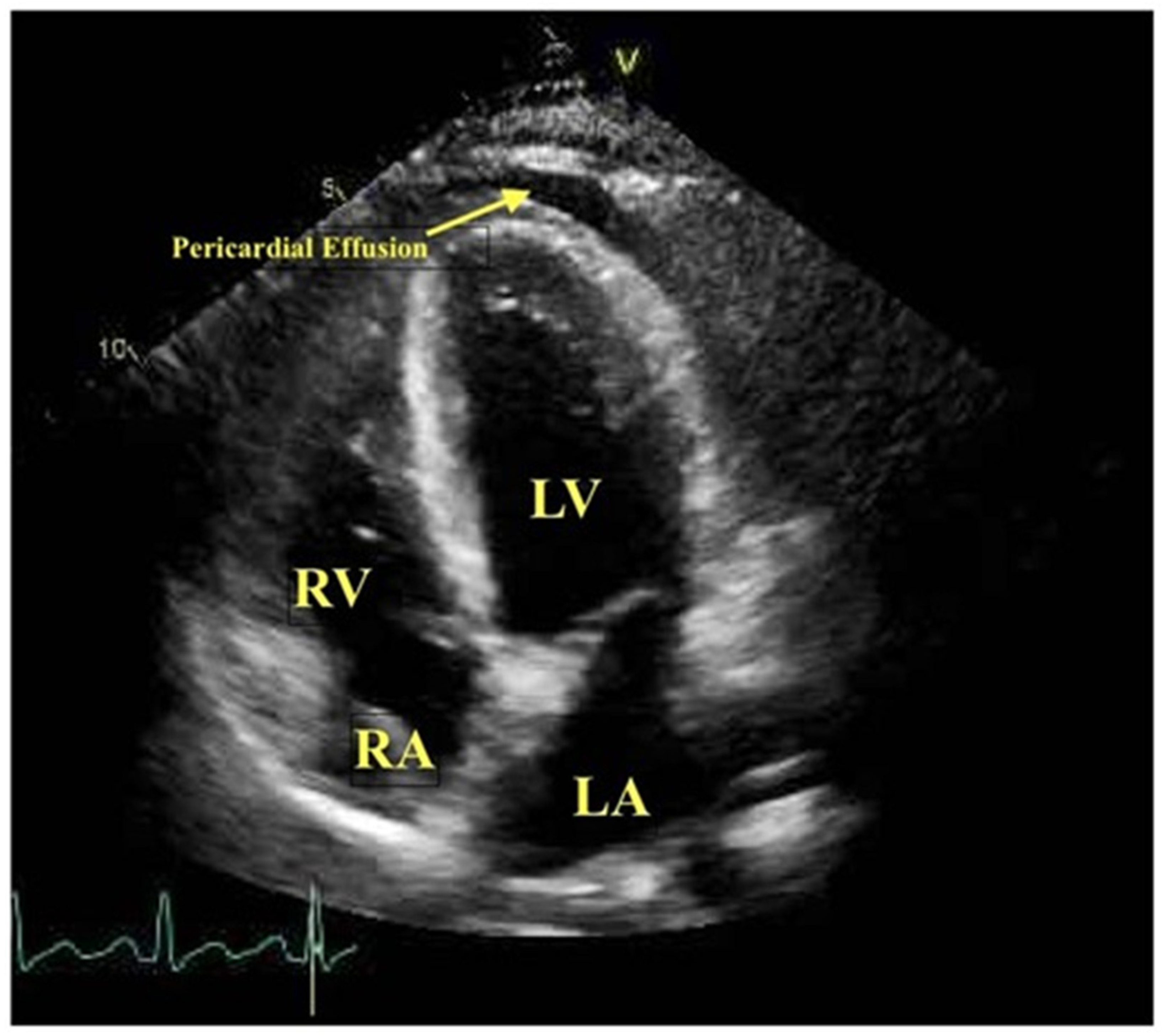
2.1.1. Two-Dimensional Transthoracic Echocardiography
2.1.2. Speckle Tracking Echocardiography
2.1.3. Tissue Doppler Imaging
2.1.4. Contrast Echocardiography
2.1.5. Three-Dimensional (3D) Transthoracic Echocardiography
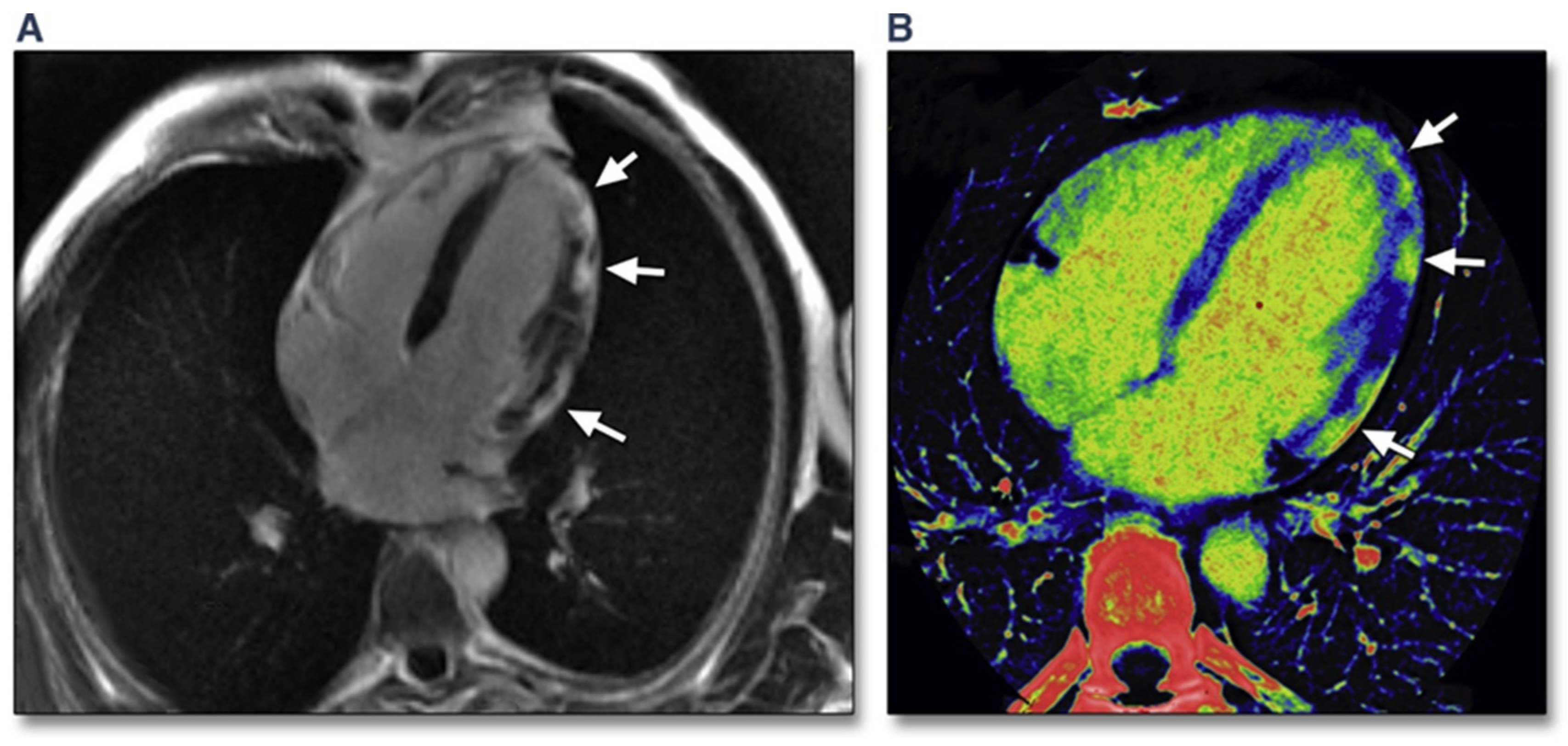
2.2. Cardiac Computed Tomography
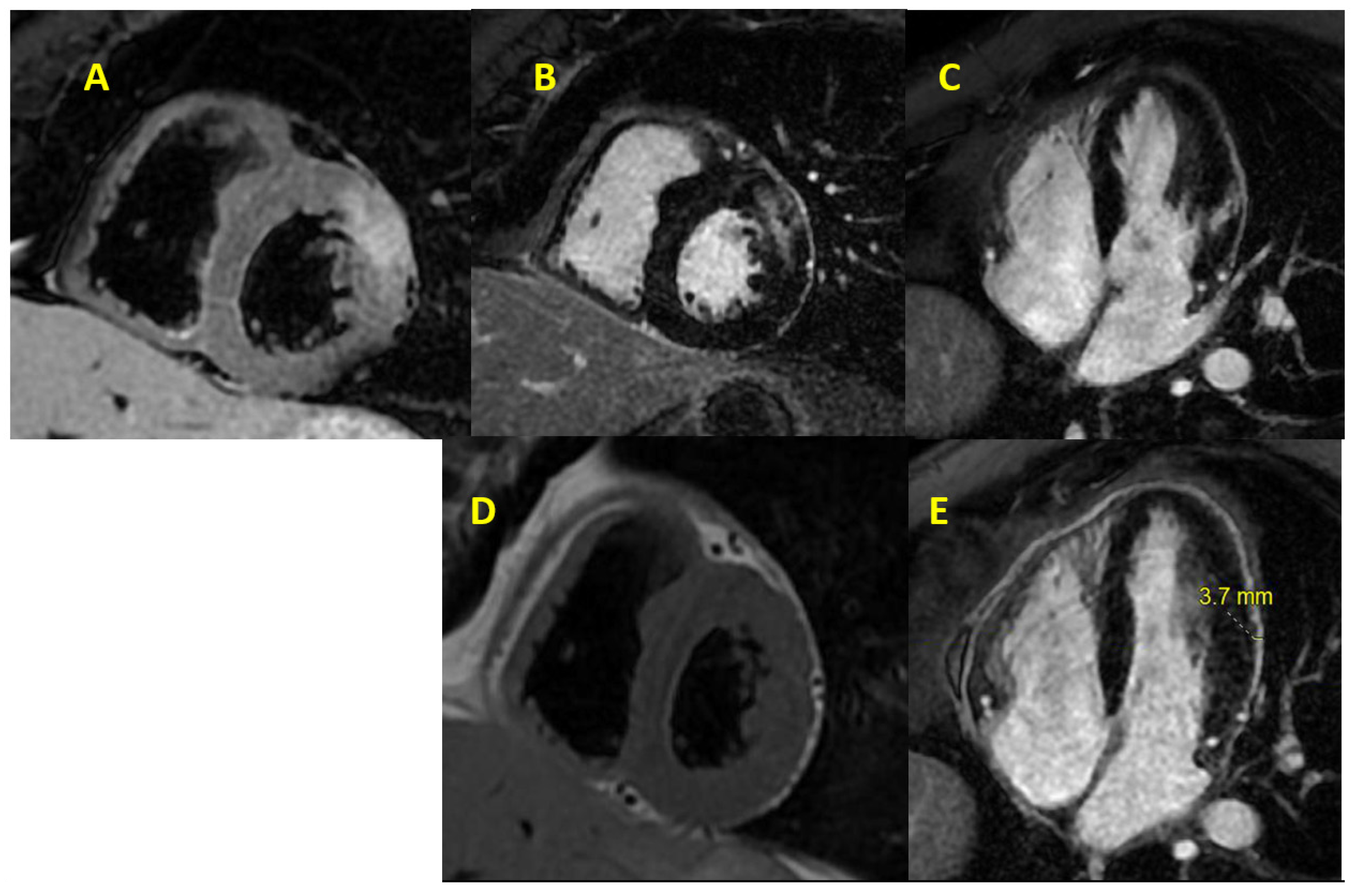
2.3. Cardiac Magnetic Resonance Imaging
2.4. Nuclear Scintigraphic Imaging
2.5. Combined Positron Emission Tomography and Computed Tomography (PET-CT)
3. The Role of Imaging in Determining Prognosis in Acute Myocarditis
4. COVID-19-Related Myocarditis
5. Imaging in COVID-19
5.1. Transthoracic Echocardiography in COVID-19
5.2. Cardiac Computerized Tomography in COVID-19
5.3. Cardiac Magnetic Resonance Imaging in COVID-19
5.4. Nuclear Imaging in COVID-19
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 18F-FDG | 18F-fluorodeoxyglucose |
| ACS | Acute coronary syndrome |
| ARDS | Acute respiratory distress syndrome |
| CCTA | Coronary computed tomography angiography |
| CMR | Cardiac magnetic resonance |
| COVID-19 | Coronavirus disease 2019 |
| CT | Computed tomography |
| ECG | Electrocardiogram |
| ECV | Extracellular volume |
| EGE | Early gadolinium enhancement |
| EMB | Endomyocardial biopsy |
| GBCA | Gadolinium-based contrast agent |
| LGE | Late gadolinium enhancement |
| LLC | Lake Louise criteria |
| LV | Left ventricle |
| LVEF | Left ventricular ejection fraction |
| PE | Pulmonary embolism |
| PET | Positron emission tomography |
| PPE | Personal protective equipment |
| RV | Right ventricle |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SPECT | Single-photon emission computed tomography |
| STE | Speckle tracking echocardiography |
| TDI | Tissue Doppler imaging |
| TTE | Transthoracic echocardiography |
References
- Blauwet, L.A.; Cooper, L.T. Myocarditis. Prog. Cardiovasc. Dis. 2010, 52, 274–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Calabrese, F.; Angelini, A.; Tona, F.; Vinci, A.; Bottaro, S.; Ramondo, A.; Carturan, E.; Iliceto, S.; Thiene, G.; et al. A prospective study of biopsy-proven myocarditis: Prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur. Heart J. 2007, 28, 1326–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef]
- Cooper, L.T., Jr. Myocarditis. N. Engl. J. Med. 2009, 360, 1526–1538. [Google Scholar] [CrossRef] [Green Version]
- Schultz, J.C.; Hilliard, A.A.; Cooper, L.T., Jr.; Rihal, C.S. Diagnosis and treatment of viral myocarditis. Mayo Clin. Proc. 2009, 84, 1001–1009. [Google Scholar] [CrossRef] [Green Version]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Oleszak, F.; Maryniak, A.; Botti, E.; Abrahim, C.; Salifu, M.O.; Youssef, M.; Henglein, V.L.; McFarlane, S.I. Myocarditis Associated With COVID-19. Am. J. Med. Case Rep. 2020, 8, 498–502. [Google Scholar] [CrossRef]
- Tahir, F.; Bin Arif, T.; Ahmed, J.; Malik, F.; Khalid, M. Cardiac Manifestations of Coronavirus Disease 2019 (COVID-19): A Comprehensive Review. Cureus 2020, 12, e8021. [Google Scholar] [CrossRef]
- Rose, N.R. Viral myocarditis. Curr. Opin. Rheumatol. 2016, 28, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kuhl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The role of endomyocardial biopsy in the management of cardiovascular disease: A scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007, 116, 2216–2233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammirati, E.; Veronese, G.; Cipriani, M.; Moroni, F.; Garascia, A.; Brambatti, M.; Adler, E.D.; Frigerio, M. Acute and Fulminant Myocarditis: A Pragmatic Clinical Approach to Diagnosis and Treatment. Curr. Cardiol. Rep. 2018, 20, 114. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Douglas, P.S.; Khandheria, B.; Stainback, R.F.; Weissman, N.J.; Brindis, R.G.; Patel, M.R.; Khandheria, B.; Alpert, J.S.; Fitzgerald, D.; Heidenreich, P.; et al. ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007 appropriateness criteria for transthoracic and transesophageal echocardiography: A report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American Society of Echocardiography, American College of Emergency Physicians, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and the Society for Cardiovascular Magnetic Resonance endorsed by the American College of Chest Physicians and the Society of Critical Care Medicine. J. Am. Coll. Cardiol. 2007, 50, 187–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, S.B.; Chen, N.; Parker, R.A., III; Hsu, J.Y. Transthoracic Echocardiography: Pitfalls and Limitations as Delineated at Cardiac CT and MR Imaging. RadioGraphics 2017, 37, 383–406. [Google Scholar] [CrossRef] [PubMed]
- Bière, L.; Piriou, N.; Ernande, L.; Rouzet, F.; Lairez, O. Imaging of myocarditis and inflammatory cardiomyopathies. Arch. Cardiovasc. Dis. 2019, 112, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Jeserich, M.; Konstantinides, S.; Pavlik, G.; Bode, C.; Geibel, A. Non-invasive imaging in the diagnosis of acute viral myocarditis. Clin. Res. Cardiol. 2009, 98, 753–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escher, F.; Kasner, M.; Kühl, U.; Heymer, J.; Wilkenshoff, U.; Tschöpe, C.; Schultheiss, H.P. New echocardiographic findings correlate with intramyocardial inflammation in endomyocardial biopsies of patients with acute myocarditis and inflammatory cardiomyopathy. Mediat. Inflamm. 2013, 2013, 875420. [Google Scholar] [CrossRef] [Green Version]
- Pinamonti, B.; Alberti, E.; Cigalotto, A.; Dreas, L.; Salvi, A.; Silvestri, F.; Camerini, F. Echocardiographic findings in myocarditis. Am. J. Cardiol. 1988, 62, 285–291. [Google Scholar] [CrossRef]
- Felker, G.M.; Boehmer, J.P.; Hruban, R.H.; Hutchins, G.M.; Kasper, E.K.; Baughman, K.L.; Hare, J.M. Echocardiographic findings in fulminant and acute myocarditis. J. Am. Coll. Cardiol. 2000, 36, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, J.F.; Koshino, Y.; Bonnichsen, C.R.; Yu, Y.; Miller, F.A., Jr.; Pellikka, P.A.; Cooper, L.T., Jr.; Villarraga, H.R. Speckle tracking echocardiography in acute myocarditis. Int. J. Cardiovasc. Imaging 2013, 29, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Nesukay, E.; Kovalenko, V.; Cherniuk, S.; Danilenko, A. The diagnostic value of speckle-tracking echocardiography in myocarditis and dilated cardiomyopathy. Eur. Heart J. 2013, 34 (Suppl. 1), 3866. [Google Scholar] [CrossRef] [Green Version]
- Matshela, M.R. The role of echocardiography in acute viral myocarditis. Cardiovasc. J. Afr. 2019, 30, 239–244. [Google Scholar] [CrossRef]
- Løgstrup, B.B.; Nielsen, J.M.; Kim, W.Y.; Poulsen, S.H. Myocardial oedema in acute myocarditis detected by echocardiographic 2D myocardial deformation analysis. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1018–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturmberger, T.; Niel, J.; Aichinger, J.; Ebner, C. Acute myocarditis with normal wall motion detected with 2D speckle tracking echocardiography. Echo Res. Pract. 2016, 3, K15–K19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tünnemann-Tarr, A.; Stöbe, S.; Laufs, U.; Hagendorff, A.; Tayal, B. Speckle tracking echocardiography in a patient with viral myocarditis and acute myocardial infarction. J. Cardiol. Cases 2020, 22, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Escher, F.; Westermann, D.; Gaub, R.; Pronk, J.; Bock, T.; Al-Saadi, N.; Kühl, U.; Schultheiss, H.P.; Tschöpe, C. Development of diastolic heart failure in a 6-year follow-up study in patients after acute myocarditis. Heart 2011, 97, 709–714. [Google Scholar] [CrossRef] [Green Version]
- Urhausen, A.; Kindermann, M.; Bohm, M.; Kindermann, W. Images in cardiovascular medicine. Diagnosis of myocarditis by cardiac tissue velocity imaging in an olympic athlete. Circulation 2003, 108, e21–e22. [Google Scholar] [CrossRef] [Green Version]
- Olszewski, R.; Timperley, J.; Szmigielski, C.; Monaghan, M.; Nihoyannopoulos, P.; Senior, R.; Becher, H. The clinical applications of contrast echocardiography. Eur. J. Echocardiogr. 2007, 8, S13–S23. [Google Scholar] [CrossRef] [Green Version]
- Afonso, L.; Hari, P.; Pidlaoan, V.; Kondur, A.; Jacob, S.; Khetarpal, V. Acute myocarditis: Can novel echocardiographic techniques assist with diagnosis? Eur. J. Echocardiogr. 2010, 11, E5. [Google Scholar] [CrossRef] [Green Version]
- Shiota, T. 3D echocardiography: The present and the future. J. Cardiol. 2008, 52, 169–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thuny, F.; Avierinos, J.F.; Jop, B.; Tafanelli, L.; Renard, S.; Riberi, A.; Métras, D.; Habib, G. Images in cardiovascular medicine. Massive biventricular thrombosis as a consequence of myocarditis: Findings from 2-dimensional and real-time 3-dimensional echocardiography. Circulation 2006, 113, e932–e933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuleri, K.H.; George, R.T.; Lardo, A.C. Applications of cardiac multidetector CT beyond coronary angiography. Nat. Rev. Cardiol. 2009, 6, 699–710. [Google Scholar] [CrossRef]
- Choi, S.I.; George, R.T.; Schuleri, K.H.; Chun, E.J.; Lima, J.A.; Lardo, A.C. Recent developments in wide-detector cardiac computed tomography. Int. J. Cardiovasc. Imaging 2009, 25 (Suppl. 1), 23–29. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Sechtem, U.; Schulz-Menger, J.; Holmvang, G.; Alakija, P.; Cooper, L.T.; White, J.A.; Abdel-Aty, H.; Gutberlet, M.; Prasad, S.; et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J. Am. Coll. Cardiol. 2009, 53, 1475–1487. [Google Scholar] [CrossRef] [Green Version]
- le Polain de Waroux, J.B.; Pouleur, A.C.; Goffinet, C.; Pasquet, A.; Vanoverschelde, J.L.; Gerber, B.L. Combined coronary and late-enhanced multidetector-computed tomography for delineation of the etiology of left ventricular dysfunction: Comparison with coronary angiography and contrast-enhanced cardiac magnetic resonance imaging. Eur. Heart J. 2008, 29, 2544–2551. [Google Scholar] [CrossRef] [Green Version]
- Bouleti, C.; Baudry, G.; Iung, B.; Arangalage, D.; Abtan, J.; Ducrocq, G.; Steg, P.-G.; Vahanian, A.; Henry-Feugeas, M.-C.; Pasi, N.; et al. Usefulness of Late Iodine Enhancement on Spectral CT in Acute Myocarditis. JACC Cardiovasc. Imaging 2017, 10, 826–827. [Google Scholar] [CrossRef]
- Liguori, C.; Farina, D.; Vaccher, F.; Ferrandino, G.; Bellini, D.; Carbone, I. Myocarditis: Imaging up to date. Radiol. Med. 2020, 125, 1124–1134. [Google Scholar] [CrossRef]
- Liu, P.P.; Mason, J.W. Advances in the understanding of myocarditis. Circulation 2001, 104, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Chetrit, M.; Friedrich, M.G. The unique role of cardiovascular magnetic resonance imaging in acute myocarditis. F1000Resarch 2018, 7, 1153. [Google Scholar] [CrossRef] [PubMed]
- Karamitsos, T.D.; Francis, J.M.; Neubauer, S. The current and emerging role of cardiovascular magnetic resonance in the diagnosis of nonischemic cardiomyopathies. Prog. Cardiovasc. Dis. 2011, 54, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Huttin, O.; Frikha, Z.; Brembilla-Perrot, B.; Sellal, J.M.; Mandry, D.; Aliot, E.; Juilliere, Y.; Sadoul, N.; Selton-Suty, C. Acute myocarditis presenting with ventricular arrhythmias: The role of CMR in the differential diagnosis of ARVD. Intern. Med. 2013, 52, 1915–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, R.; Trappe, H.J.; Klein, H.; Kemnitz, J. Chronic (or healed) myocarditis mimicking arrhythmogenic right ventricular dysplasia. Eur. Heart J. 1993, 14, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Monney, P.; Locca, D.; Muzzarelli, S.; Hullin, R.; Jeanrenaud, X.; Schwitter, J. IRM cardiaque: Imagerie de référence dans le diagnostic de la myocardite aiguë? (Cardiac magnetic resonance in acute myocarditis: A new non-invasive diagnostic gold standard?). Rev. Med. Suisse 2012, 8, 1177–1183. [Google Scholar]
- Lurz, P.; Eitel, I.; Adam, J.; Steiner, J.; Grothoff, M.; Desch, S.; Fuernau, G.; de Waha, S.; Sareban, M.; Luecke, C.; et al. Diagnostic performance of CMR imaging compared with EMB in patients with suspected myocarditis. JACC Cardiovasc. Imaging 2012, 5, 513–524. [Google Scholar] [CrossRef]
- Lewis, A.J.M.; Burrage, M.K.; Ferreira, V.M. Cardiovascular magnetic resonance imaging for inflammatory heart diseases. Cardiovasc. Diagn. Ther. 2020, 10, 598–609. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Mirakhur, A.; Anca, N.; Mikami, Y.; Merchant, N. T2-weighted imaging of the heart—A pictorial review. Eur. J. Radiol. 2013, 82, 1755–1762. [Google Scholar] [CrossRef]
- Guglin, M.; Nallamshetty, L. Myocarditis: Diagnosis and treatment. Curr. Treat. Options Cardiovasc. Med. 2012, 14, 637–651. [Google Scholar] [CrossRef]
- Abdel-Aty, H.; Boyé, P.; Zagrosek, A.; Wassmuth, R.; Kumar, A.; Messroghli, D.; Bock, P.; Dietz, R.; Friedrich, M.G.; Schulz-Menger, J. Diagnostic performance of cardiovascular magnetic resonance in patients with suspected acute myocarditis: Comparison of different approaches. J. Am. Coll. Cardiol. 2005, 45, 1815–1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, V.M.; Piechnik, S.K.; Dall’Armellina, E.; Karamitsos, T.D.; Francis, J.M.; Ntusi, N.; Holloway, C.; Choudhury, R.P.; Kardos, A.; Robson, M.D.; et al. T(1) mapping for the diagnosis of acute myocarditis using CMR: Comparison to T2-weighted and late gadolinium enhanced imaging. JACC Cardiovasc. Imaging 2013, 6, 1048–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Aty, H.; Cocker, M.; Strohm, O.; Filipchuk, N.; Friedrich, M.G. Abnormalities in T2-weighted cardiovascular magnetic resonance images of hypertrophic cardiomyopathy: Regional distribution and relation to late gadolinium enhancement and severity of hypertrophy. J. Magn. Reson. Imaging 2008, 28, 242–245. [Google Scholar] [CrossRef]
- Mahrholdt, H.; Goedecke, C.; Wagner, A.; Meinhardt, G.; Athanasiadis, A.; Vogelsberg, H.; Fritz, P.; Klingel, K.; Kandolf, R.; Sechtem, U. Cardiovascular magnetic resonance assessment of human myocarditis: A comparison to histology and molecular pathology. Circulation 2004, 109, 1250–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, A.; Mahrholdt, H.; Holly, T.A.; Elliott, M.D.; Regenfus, M.; Parker, M.; Klocke, F.J.; Bonow, R.O.; Kim, R.J.; Judd, R.M. Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: An imaging study. Lancet 2003, 361, 374–379. [Google Scholar] [CrossRef]
- Verhaert, D.; Thavendiranathan, P.; Giri, S.; Mihai, G.; Rajagopalan, S.; Simonetti, O.P.; Raman, S.V. Direct T2 quantification of myocardial edema in acute ischemic injury. JACC Cardiovasc. Imaging 2011, 4, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Giri, S.; Chung, Y.C.; Merchant, A.; Mihai, G.; Rajagopalan, S.; Raman, S.V.; Simonetti, O.P. T2 quantification for improved detection of myocardial edema. J. Cardiovasc. Magn. Reson. 2009, 11, 56. [Google Scholar] [CrossRef] [Green Version]
- Messroghli, D.R.; Greiser, A.; Fröhlich, M.; Dietz, R.; Schulz-Menger, J. Optimization and validation of a fully-integrated pulse sequence for modified look-locker inversion-recovery (MOLLI) T1 mapping of the heart. J. Magn. Reson. Imaging 2007, 26, 1081–1086. [Google Scholar] [CrossRef]
- Piechnik, S.K.; Ferreira, V.M.; Dall’Armellina, E.; Cochlin, L.E.; Greiser, A.; Neubauer, S.; Robson, M.D. Shortened Modified Look-Locker Inversion recovery (ShMOLLI) for clinical myocardial T1-mapping at 1.5 and 3 T within a 9 heartbeat breathhold. J. Cardiovasc. Magn. Reson. 2010, 12, 69. [Google Scholar] [CrossRef] [Green Version]
- Chow, K.; Flewitt, J.A.; Green, J.D.; Pagano, J.J.; Friedrich, M.G.; Thompson, R.B. Saturation recovery single-shot acquisition (SASHA) for myocardial T(1) mapping. Magn. Reson. Med. 2014, 71, 2082–2095. [Google Scholar] [CrossRef]
- Roujol, S.; Weingärtner, S.; Foppa, M.; Chow, K.; Kawaji, K.; Ngo, L.H.; Kellman, P.; Manning, W.J.; Thompson, R.B.; Nezafat, R. Accuracy, precision, and reproducibility of four T1 mapping sequences: A head-to-head comparison of MOLLI, ShMOLLI, SASHA, and SAPPHIRE. Radiology 2014, 272, 683–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baeßler, B.; Schaarschmidt, F.; Stehning, C.; Schnackenburg, B.; Maintz, D.; Bunck, A.C. A systematic evaluation of three different cardiac T2-mapping sequences at 1.5 and 3T in healthy volunteers. Eur. J. Radiol. 2015, 84, 2161–2170. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Bassareo, P.; Saba, L. Cardiac Involvement in COVID-19-Assessment with Echocardiography and Cardiac Magnetic Resonance Imaging. SN Compr. Clin. Med. 2020, 2, 845–851. [Google Scholar] [CrossRef]
- Mavrogeni, S.; Apostolou, D.; Argyriou, P.; Velitsista, S.; Papa, L.; Efentakis, S.; Vernardos, E.; Kanoupaki, M.; Kanoupakis, G.; Manginas, A. T1 and T2 Mapping in Cardiology: “Mapping the Obscure Object of Desire”. Cardiology 2017, 138, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Huber, A.T.; Bravetti, M.; Lamy, J.; Bacoyannis, T.; Roux, C.; De Cesare, A.; Rigolet, A.; Benveniste, O.; Allenbach, Y.; Kerneis, M.; et al. Non-invasive differentiation of idiopathic inflammatory myopathy with cardiac involvement from acute viral myocarditis using cardiovascular magnetic resonance imaging T1 and T2 mapping. J. Cardiovasc. Magn. Reson. 2018, 20, 11. [Google Scholar] [CrossRef]
- Kim, R.J.; Albert, T.S.; Wible, J.H.; Elliott, M.D.; Allen, J.C.; Lee, J.C.; Parker, M.; Napoli, A.; Judd, R.M. Performance of delayed-enhancement magnetic resonance imaging with gadoversetamide contrast for the detection and assessment of myocardial infarction: An international, multicenter, double-blinded, randomized trial. Circulation 2008, 117, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef] [Green Version]
- Kirkbride, R.R.; Rawal, B.; Mirsadraee, S.; Galperin-Aizenberg, M.; Wechalekar, K.; Ridge, C.A.; Litmanovich, D.E. Imaging of Cardiac Infections: A Comprehensive Review and Investigation Flowchart for Diagnostic Workup. J. Thorac. Imaging 2020, 36, W70–W88. [Google Scholar] [CrossRef]
- Baeßler, B.; Treutlein, M.; Schaarschmidt, F.; Stehning, C.; Schnackenburg, B.; Michels, G.; Maintz, D.; Bunck, A.C. A novel multiparametric imaging approach to acute myocarditis using T2-mapping and CMR feature tracking. J. Cardiovasc. Magn. Reson. 2017, 19, 71. [Google Scholar] [CrossRef] [Green Version]
- Luetkens, J.A.; Faron, A.; Isaak, A.; Dabir, D.; Kuetting, D.; Feisst, A.; Schmeel, F.C.; Sprinkart, A.M.; Thomas, D. Comparison of Original and 2018 Lake Louise Criteria for Diagnosis of Acute Myocarditis: Results of a Validation Cohort. Radiol. Cardiothorac. Imaging 2019, 1, 3. [Google Scholar] [CrossRef]
- Alexander, C.; Oberhausen, E. Myocardial scintigraphy. Semin. Nucl. Med. 1995, 25, 195–201. [Google Scholar] [CrossRef]
- Moralidis, E.; Mantziari, L.; Gerasimou, G.; Styliadis, I.H.; Gotzamani-Psarrakou, A. Somatostatin analogue scintigraphy in a patient with viral myocarditis. Hell. J. Nucl. Med. 2012, 15, 144–146. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Henkin, R.E.; Robinson, J.A.; Subramanian, R.; Scanlon, P.J.; Gunnar, R.M. Gallium-67 imaging in patients with dilated cardiomyopathy and biopsy-proven myocarditis. Circulation 1984, 70, 58–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strain, J.E.; Fine, E.; Grose, R.M.; Kramer, D.C.; Cho, S.; Factor, S.M. Comparison of myocardial biopsy and gallium-67 imaging for diagnosing myocarditis. Circulation 1983, 68 (Suppl. 111), 208. [Google Scholar]
- Hung, M.Y.; Hung, M.J.; Cheng, C.W. Use of gallium 67 scintigraphy to differentiate acute myocarditis from acute myocardial infarction. Tex. Heart Inst. J. 2007, 34, 305–309. [Google Scholar]
- Narula, J.; Khaw, B.A.; Dec, G.W.; Palacios, I.F.; Newell, J.B.; Southern, J.F.; Fallon, J.T.; Strauss, H.W.; Haber, E.; Yasuda, T. Diagnostic accuracy of antimyosin scintigraphy in suspected myocarditis. J. Nucl. Cardiol. 1996, 3, 371–381. [Google Scholar] [CrossRef]
- Yasuda, T.; Palacios, I.F.; Dec, G.W.; Fallon, J.T.; Gold, H.K.; Leinbach, R.C.; Strauss, H.W.; Khaw, B.A.; Haber, E. Indium 111-monoclonal antimyosin antibody imaging in the diagnosis of acute myocarditis. Circulation 1987, 76, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Le Guludec, D.; Sarda, L.; Rouzet, F.; Merlet, P.; Slama, M.S.; Lebtahi, R. Imaging inflammatory cardiomyopathies. J. Nucl. Cardiol. 2005, 12, 731–739. [Google Scholar] [CrossRef]
- Martin, M.E.; Moya-Mur, J.L.; Casanova, M.; Crespo-Diez, A.; Asin-Cardiel, E.; Castro-Beiras, J.M.; Diez-Jimenez, L.; Ballester, M.; Carrio, I.; Narula, J. Role of noninvasive antimyosin imaging in infants and children with clinically suspected myocarditis. J. Nucl. Med. 2004, 45, 429–437. [Google Scholar]
- Kühl, U.; Lauer, B.; Souvatzoglu, M.; Vosberg, H.; Schultheiss, H.P. Antimyosin scintigraphy and immunohistologic analysis of endomyocardial biopsy in patients with clinically suspected myocarditis--evidence of myocardial cell damage and inflammation in the absence of histologic signs of myocarditis. J. Am. Coll. Cardiol. 1998, 32, 1371–1376. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Ma, P.; Bax, J.J.; Blom, N.; Yu, Y.; Wang, Y.; Han, X.; Wang, Y.; Van Der Wall, E.E. 99mTc-MIBI myocardial perfusion imaging in myocarditis. Nucl. Med. Commun. 2003, 24, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Javadi, H.; Jallalat, S.; Pourbehi, G.; Semnani, S.; Mogharrabi, M.; Nabipour, I.; Ravanbod, M.; Amini, A.; Assadi, M. The role of gated myocardial perfusion scintigraphy (GMPS) in myocarditis: A case report and review of the literature. Nucl. Med. Rev. Cent. East. Eur. 2011, 14, 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiratli, P.O.; Tuncel, M.; Ozkutlu, S.; Caglar, M. Gated myocardial perfusion scintigraphy in children with myocarditis: Can it be considered as an indicator of clinical outcome? Nucl. Med. Commun. 2008, 29, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Skouri, H.N.; Dec, G.W.; Friedrich, M.G.; Cooper, L.T. Noninvasive imaging in myocarditis. J. Am. Coll. Cardiol. 2006, 48, 2085–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoey, E.T.; Gulati, G.S.; Ganeshan, A.; Watkin, R.W.; Simpson, H.; Sharma, S. Cardiovascular MRI for assessment of infectious and inflammatory conditions of the heart. AJR Am. J. Roentgenol. 2011, 197, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Boccara, F.; Blanchard-Lemoine, B.; Sarda, L.; Bardet, J.; Le Guludec, D.; Cohen, A. Conduite diagnostique dans les myocardites aiguës (Diagnostic strategy in acute myocarditis). Arch. Mal. CoEur. Vaiss. 1998, 91, 1151–1158. [Google Scholar] [PubMed]
- Dec, G.W.; Palacios, I.; Yasuda, T.; Fallon, J.T.; Khaw, B.A.; Strauss, H.W.; Haber, E. Antimyosin antibody cardiac imaging: Its role in the diagnosis of myocarditis. J. Am. Coll. Cardiol. 1990, 16, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, A.; Klingel, K.; Kandolf, R.; Sechtem, U. Imaging in inflammatory heart disease: From the past to current clinical practice. Hell. J. Cardiol. 2009, 50, 449–460. [Google Scholar]
- Lawal, I.; Sathekge, M. F-18 FDG PET/CT imaging of cardiac and vascular inflammation and infection. Br. Med. Bull. 2016, 120, 55–74. [Google Scholar] [CrossRef]
- Chen, W.; Jeudy, J. Assessment of Myocarditis: Cardiac MR, PET/CT, or PET/MR? Curr. Cardiol. Rep. 2019, 21, 76. [Google Scholar] [CrossRef]
- Schneider, S.; Batrice, A.; Rischpler, C.; Eiber, M.; Ibrahim, T.; Nekolla, S.G. Utility of multimodal cardiac imaging with PET/MRI in cardiac sarcoidosis: Implications for diagnosis, monitoring and treatment. Eur. Heart J. 2014, 35, 312. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, D.; Bauckneht, M.; Altini, C.; Popescu, C.E.; Ferro, P.; Monaco, L.; Borra, A.; Ferrari, C.; Caobelli, F. The role of positron emission tomography in the assessment of cardiac sarcoidosis. Br. J. Radiol. 2019, 92, 20190247. [Google Scholar] [CrossRef] [PubMed]
- von Olshausen, G.; Hyafil, F.; Langwieser, N.; Laugwitz, K.L.; Schwaiger, M.; Ibrahim, T. Detection of acute inflammatory myocarditis in Epstein Barr virus infection using hybrid 18F-fluoro-deoxyglucose-positron emission tomography/magnetic resonance imaging. Circulation 2014, 130, 925–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nensa, F.; Poeppel, T.D.; Krings, P.; Schlosser, T. Multiparametric assessment of myocarditis using simultaneous positron emission tomography/magnetic resonance imaging. Eur. Heart J. 2014, 35, 2173. [Google Scholar] [CrossRef] [Green Version]
- Prato, F.S.; Butler, J.; Sykes, J.; Keenliside, L.; Blackwood, K.J.; Thompson, R.T.; White, J.A.; Mikami, Y.; Thiessen, J.D.; Wisenberg, G. Can the inflammatory response be evaluated using 18F-FDG within zones of microvascular obstruction after myocardial infarction? J. Nucl. Med. 2015, 56, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Lamacie, M.M.; Almufleh, A.; Nair, V.; Stadnick, E.; Birnie, D.; Beanlands, R.; Chih, S. Serial 18F-Fluorodeoxyglucose Positron Emission Tomography Imaging in a Patient With Giant Cell Myocarditis. Circ. Cardiovasc. Imaging 2020, 13, e009940. [Google Scholar] [CrossRef]
- Nensa, F.; Kloth, J.; Tezgah, E.; Poeppel, T.D.; Heusch, P.; Goebel, J.; Nassenstein, K.; Schlosser, T. Feasibility of FDG-PET in myocarditis: Comparison to CMR using integrated PET/MRI. J. Nucl. Cardiol. 2018, 25, 785–794. [Google Scholar] [CrossRef]
- FDG-PET/CT Images Comparing to MRI and Endomyocardial Biopsy in Myocarditis (STREAM). ClinicalTrials.gov Identifier: NCT04085718. Available online: https://clinicaltrials.gov/ct2/show/NCT04085718 (accessed on 29 December 2021).
- Chopra, H.; Arangalage, D.; Bouleti, C.; Zarka, S.; Fayard, F.; Chillon, S.; Laissy, J.P.; Henry-Feugeas, M.C.; Steg, P.G.; Vahanian, A.; et al. Prognostic value of the infarct- and no n-infarct like patterns and cardiovascular magnetic resonance parameters on long-term outcome of patients after acute myocarditis. Int. J. Cardiol. 2016, 212, 63–69. [Google Scholar] [CrossRef]
- Mewton, N.; Dernis, A.; Bresson, D.; Zouaghi, O.; Croisille, P.; Flocard, E.; Douek, P.; Bonnefoy-Cudraz, E. Myocardial biomarkers and delayed enhanced cardiac magnetic resonance relationship in clinically suspected myocarditis and insight on clinical outcome. J. Cardiovasc. Med. 2015, 16, 696–703. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; et al. Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis With Preserved Systolic Function: ITAMY Study. J. Am. Coll. Cardiol. 2017, 70, 1977–1987. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 9 December 2021).
- De Lorenzo, A.; Kasal, D.A.; Tura, B.R.; Lamas, C.C.; Rey, H.C. Acute cardiac injury in patients with COVID-19. Am. J. Cardiovasc. Dis. 2020, 10, 28–33. [Google Scholar] [PubMed]
- Atri, D.; Siddiqi, H.K.; Lang, J.P.; Nauffal, V.; Morrow, D.A.; Bohula, E.A. COVID-19 for the Cardiologist: Basic Virology, Epidemiology, Cardiac Manifestations, and Potential Therapeutic Strategies. JACC Basic Transl. Sci. 2020, 5, 518–536. [Google Scholar] [CrossRef] [PubMed]
- Purdy, A.; Ido, F.; Sterner, S.; Tesoriero, E.; Matthews, T.; Singh, A. Myocarditis in COVID-19 presenting with cardiogenic shock: A case series. Eur. Heart J. Case Rep. 2021, 5, ytab028. [Google Scholar] [CrossRef]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and Cardiovascular Disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirzada, A.; Mokhtar, A.T.; Moeller, A.D. COVID-19 and Myocarditis: What Do We Know So Far? CJC Open 2020, 2, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Agricola, E.; Beneduce, A.; Esposito, A.; Ingallina, G.; Palumbo, D.; Palmisano, A.; Ancona, F.; Baldetti, L.; Pagnesi, M.; Melisurgo, G.; et al. Heart and Lung Multimodality Imaging in COVID-19. JACC Cardiovasc. Imaging 2020, 13, 1792–1808. [Google Scholar] [CrossRef]
- Cameli, M.; Pastore, M.C.; Henein, M.; Aboumarie, H.S.; Mandoli, G.E.; D’Ascenzi, F.; Cameli, P.; Franchi, F.; Mondillo, S.; Valente, S. Safe performance of echocardiography during the COVID-19 pandemic: A practical guide. Rev. Cardiovasc. Med. 2020, 21, 217–223. [Google Scholar] [CrossRef]
- Citro, R.; Pontone, G.; Bellino, M.; Silverio, A.; Iuliano, G.; Baggiano, A.; Manka, R.; Iesu, S.; Vecchione, C.; Asch, F.M.; et al. Role of multimodality imaging in evaluation of cardiovascular involvement in COVID-19. Trends Cardiovasc. Med. 2021, 31, 8–16. [Google Scholar] [CrossRef]
- The European Society for Cardiology. ESC Guidance for the Diagnosis and Management of CV Disease during the COVID-19 Pandemic-Updated. Available online: https://www.escardio.org/Education/COVID-19-and-Cardiology (accessed on 9 December 2021).
- Zhang, L.; Wang, B.; Zhou, J.; Kirkpatrick, J.; Xie, M.; Johri, A.M. Bedside Focused Cardiac Ultrasound in COVID-19 from the Wuhan Epicenter: The Role of Cardiac Point-of-Care Ultrasound, Limited Transthoracic Echocardiography, and Critical Care Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 676–682. [Google Scholar] [CrossRef]
- Huang, G.; Vengerovsky, A.; Morris, A.; Town, J.; Carlbom, D.; Kwon, Y. Development of a COVID-19 Point-of-Care Ultrasound Protocol. J. Am. Soc. Echocardiogr. 2020, 33, 903–905. [Google Scholar] [CrossRef] [PubMed]
- Picard, M.H.; Weiner, R.B. Echocardiography in the Time of COVID-19. J. Am. Soc. Echocardiogr. 2020, 33, 674–675. [Google Scholar] [CrossRef] [PubMed]
- Drake, D.H.; De Bonis, M.; Covella, M.; Agricola, E.; Zangrillo, A.; Zimmerman, K.G.; Cobey, F.C. Echocardiography in Pandemic: Front-Line Perspective, Expanding Role of Ultrasound, and Ethics of Resource Allocation. J. Am. Soc. Echocardiogr. 2020, 33, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, P.; Croft, L.B.; Ro, R.; Anastasius, M.; Zhao, W.; Giustino, G.; Argulian, E.; Goldman, M.E.; Sharma, S.K.; Kini, A.; et al. Biventricular strain by speckle tracking echocardiography in COVID-19: Findings and possible prognostic implications. Future Cardiol. 2021, 17, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.S.; Rojas, G.A.; Sondhi, M.; Pothuru, S.; Pydi, R.; Kancherla, N.; Singh, R.; Ahmed, N.K.; Shah, J.; Tousif, S.; et al. Myocarditis associated with Covid-19 disease: A systematic review of published case reports and case series. J. Clin. Pract. 2021, 75, e14470. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Wang, H.; Ma, F.; Cui, G.L.; Peng, L.Y.; Li, C.Z.; Zeng, H.S.; Marian, A.J.; Wang, D.W. Widespread myocardial dysfunction in COVID-19 patients detected by myocardial strain imaging using 2-D speckle-tracking echocardiography. Acta Pharmacol. Sin. 2021, 42, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Croft, L.B.; Krishnamoorthy, P.; Ro, R.; Anastasius, M.; Zhao, W.; Buckley, S.; Goldman, M.; Argulian, E.; Sharma, S.K.; Kini, A.; et al. Abnormal left ventricular global longitudinal strain by speckle tracking echocardiography in COVID-19 patients. Future Cardiol. 2021, 17, 655–661. [Google Scholar] [CrossRef]
- Trogen, B.; Gonzalez, F.J.; Shust, G.F. COVID-19-Associated Myocarditis in an Adolescent. Pediatric Infect. Dis. J. 2020, 39, e204–e205. [Google Scholar] [CrossRef]
- Goerlich, E.; Minhas, A.S.; Mukherjee, M.; Sheikh, F.H.; Gilotra, N.A.; Sharma, G.; Michos, E.D.; Hays, A.G. Multimodality Imaging for Cardiac Evaluation in Patients with COVID-19. Curr. Cardiol. Rep. 2021, 23, 44. [Google Scholar] [CrossRef]
- Kirkpatrick, J.N.; Mitchell, C.; Taub, C.; Kort, S.; Hung, J.; Swaminathan, M. ASE Statement on Protection of Patients and Echocardiography Service Providers During the 2019 Novel Coronavirus Outbreak: Endorsed by the American College of Cardiology. J. Am. Coll. Cardiol. 2020, 75, 3078–3084. [Google Scholar] [CrossRef]
- Gerber, B.L.; Belge, B.; Legros, G.J.; Lim, P.; Poncelet, A.; Pasquet, A.; Gisellu, G.; Coche, E.; Vanoverschelde, J.L. Characterization of acute and chronic myocardial infarcts by multidetector computed tomography: Comparison with contrast-enhanced magnetic resonance. Circulation 2006, 113, 823–833. [Google Scholar] [CrossRef] [Green Version]
- Pontone, G.; Baggiano, A.; Conte, E.; Teruzzi, G.; Cosentino, N.; Campodonico, J.; Rabbat, M.G.; Assanelli, E.; Palmisano, A.; Esposito, A.; et al. “Quadruple Rule-Out” With Computed Tomography in a COVID-19 Patient With Equivocal Acute Coronary Syndrome Presentation. JACC Cardiovasc. Imaging 2020, 13, 1854–1856. [Google Scholar] [CrossRef] [PubMed]
- Beitzke, D.; Salgado, R.; Francone, M.; Kreitner, K.F.; Natale, L.; Bremerich, J.; Gutberlet, M.; Mousseaux, E.; Nikolaou, K.; Peebles, C.; et al. Cardiac imaging procedures and the COVID-19 pandemic: Recommendations of the European Society of Cardiovascular Radiology (ESCR). Int. J. Cardiovasc. Imaging 2020, 36, 1801–1810. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.M.; Hwang, S.H.; Lee, H.J. Role of Cardiac Computed Tomography in the Diagnosis of Left Ventricular Myocardial Diseases. J. Cardiovasc. Imaging. 2019, 27, 73–92. [Google Scholar] [CrossRef] [Green Version]
- Poon, M.; Leipsic, J.; Kim, M.; Welt, F.; Rose, G. Impact of Cardiovascular Care of COVID-19: Lessons Learned, Current Challenges, and Future Opportunities. Radiol. Cardiothorac. Imaging 2020, 2, e200251. [Google Scholar] [CrossRef] [PubMed]
- Dambrin, G.; Laissy, J.P.; Serfaty, J.M.; Caussin, C.; Lancelin, B.; Paul, J.F. Diagnostic value of ECG-gated multidetector computed tomography in the early phase of suspected acute myocarditis. A preliminary comparative study with cardiac MRI. Eur. Radiol. 2007, 17, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.; Palmisano, A.; Barbera, M.; Vignale, D.; Benedetti, G.; Spoladore, R.; Ancona, M.B.; Giannini, F.; Oppizzi, M.; Del Maschio, A.; et al. Cardiac Computed Tomography in Troponin-Positive Chest Pain: Sometimes the Answer Lies in the Late Iodine Enhancement or Extracellular Volume Fraction Map. JACC Cardiovasc. Imaging 2019, 12, 745–748. [Google Scholar] [CrossRef]
- Rodriguez-Granillo, G.A.; Carrascosa, P.; Cipriano, S.; de Zan, M.; Deviggiano, A.; Capunay, C.; Cury, R.C. Myocardial signal density levels and beam-hardening artifact attenuation using dual-energy computed tomography. Clin. Imaging 2015, 39, 809–814. [Google Scholar] [CrossRef]
- Skulstad, H.; Cosyns, B.; Popescu, B.A.; Galderisi, M.; di Salvo, G.; Donal, E.; Petersen, S.; Gimelli, A.; Haugaa, K.H.; Muraru, D.; et al. COVID-19 pandemic and cardiac imaging: EACVI recommendations on precautions, indications, prioritization, and protection for patients and healthcare personnel. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 592–598. [Google Scholar] [CrossRef]
- Choi, A.D.; Abbara, S.; Branch, K.R.; Feuchtner, G.M.; Ghoshhajra, B.; Nieman, K.; Pontone, G.; Villines, T.C.; Williams, M.C.; Blankstein, R. Society of Cardiovascular Computed Tomography guidance for use of cardiac computed tomography amidst the COVID-19 pandemic Endorsed by the American College of Cardiology. J. Cardiovasc. Comput. Tomogr. 2020, 14, 101–104. [Google Scholar] [CrossRef]
- Sanghvi, S.K.; Schwarzman, L.S.; Nazir, N.T. Cardiac MRI and Myocardial Injury in COVID-19: Diagnosis, Risk Stratification and Prognosis. Diagnostics 2021, 11, 130. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.; Kyvernitakis, A.; Mikolich, J.R.; Biederman, R.W.W. Contemporary use of cardiac imaging for COVID-19 patients: A three center experience defining a potential role for cardiac MRI. Int. J. Cardiovasc. Imaging 2021, 37, 1721–1733. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, S.; Tong, M.S.; Borchers, J.; Zareba, K.M.; Obarski, T.P.; Simonetti, O.P.; Daniels, C.J. Cardiovascular Magnetic Resonance Findings in Competitive Athletes Recovering From COVID-19 Infection. JAMA Cardiol. 2021, 6, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Daniels, C.J.; Rajpal, S.; Greenshields, J.T.; Rosenthal, G.L.; Chung, E.H.; Terrin, M.; Jeudy, J.; Mattson, S.E.; Law, I.H.; Borchers, J.; et al. Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes With Recent SARS-CoV-2 Infection: Results From the Big Ten COVID-19 Cardiac Registry. JAMA Cardiol. 2021, 6, 1078–1087. [Google Scholar] [CrossRef]
- Wang, H.; Li, R.; Zhou, Z.; Jiang, H.; Yan, Z.; Tao, X.; Li, H.; Xu, L. Cardiac involvement in COVID-19 patients: Mid-term follow up by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 14. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.; Van, T.A.; Krug, R.; Hetts, S.W.; Wilson, M.W. Cardiac MR imaging: Current status and future direction. Cardiovasc. Diagn. Ther. 2015, 5, 290–310. [Google Scholar] [CrossRef]
- Kelle, S.; Bucciarelli-Ducci, C.; Judd, R.M.; Kwong, R.Y.; Simonetti, O.; Plein, S.; Raimondi, F.; Weinsaft, J.W.; Wong, T.C.; Carr, J. Society for Cardiovascular Magnetic Resonance (SCMR) recommended CMR protocols for scanning patients with active or convalescent phase COVID-19 infection. J. Cardiovasc. Magn. Reson. 2020, 22, 61. [Google Scholar] [CrossRef]
- Skali, H.; Murthy, V.L.; Al-Mallah, M.H.; Bateman, T.M.; Beanlands, R.; Better, N.; Calnon, D.A.; Dilsizian, V.; Gimelli, A.; Pagnanelli, R.; et al. Guidance and Best Practices for Nuclear Cardiology Laboratories During the COVID-19 Pandemic: An Information Statement From ASNC and SNMMI. Circ. Cardiovasc. Imaging 2020, 13, e011761. [Google Scholar] [CrossRef]
- Minamimoto, R.; Hotta, M.; Ishikane, M.; Inagaki, T. FDG-PET/CT images of COVID-19: A comprehensive review. Glob. Health Med. 2020, 2, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.K.K.; Demirjian, N.L.; Dadgar, H.; Gholamrezanezhad, A. Imaging of COVID-19: CT, MRI, and PET. Semin. Nucl. Med. 2020, 51, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.R.; Shah, A.S.V.; Ombati, K.O.; Nganga, E.; Gitau, S.; Makhdomi, K.; Chung, M.H.; Vinayak, S. CardiOvaScular Mechanisms In Covid-19: Methodology of a prospective observational multimodality imaging study (COSMIC-19 study). BMC Cardiovasc. Disord. 2021, 21, 234. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conventional Echocardiography Findings in Viral Myocarditis: |
|---|
|
| Technique | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|
| Standard CMR Techniques | Increased T2 signal | 68 | 91 |
| Increased EGE | 70 | 74 | |
| Increased LGE | 68 | 96 | |
| Novel CMR Techniques | T1 mapping | 89 | 90 |
| T2 mapping | 78 | 84 | |
| ECV mapping | 75 | 76 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adeboye, A.; Alkhatib, D.; Butt, A.; Yedlapati, N.; Garg, N. A Review of the Role of Imaging Modalities in the Evaluation of Viral Myocarditis with a Special Focus on COVID-19-Related Myocarditis. Diagnostics 2022, 12, 549. https://doi.org/10.3390/diagnostics12020549
Adeboye A, Alkhatib D, Butt A, Yedlapati N, Garg N. A Review of the Role of Imaging Modalities in the Evaluation of Viral Myocarditis with a Special Focus on COVID-19-Related Myocarditis. Diagnostics. 2022; 12(2):549. https://doi.org/10.3390/diagnostics12020549
Chicago/Turabian StyleAdeboye, Adedayo, Deya Alkhatib, Asra Butt, Neeraja Yedlapati, and Nadish Garg. 2022. "A Review of the Role of Imaging Modalities in the Evaluation of Viral Myocarditis with a Special Focus on COVID-19-Related Myocarditis" Diagnostics 12, no. 2: 549. https://doi.org/10.3390/diagnostics12020549