
Multimodal Remote Home Monitoring of Lung Transplant Recipients during COVID-19 Vaccinations: Usability Pilot Study of the COVIDA Desk Incorporating Wearable Devices
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
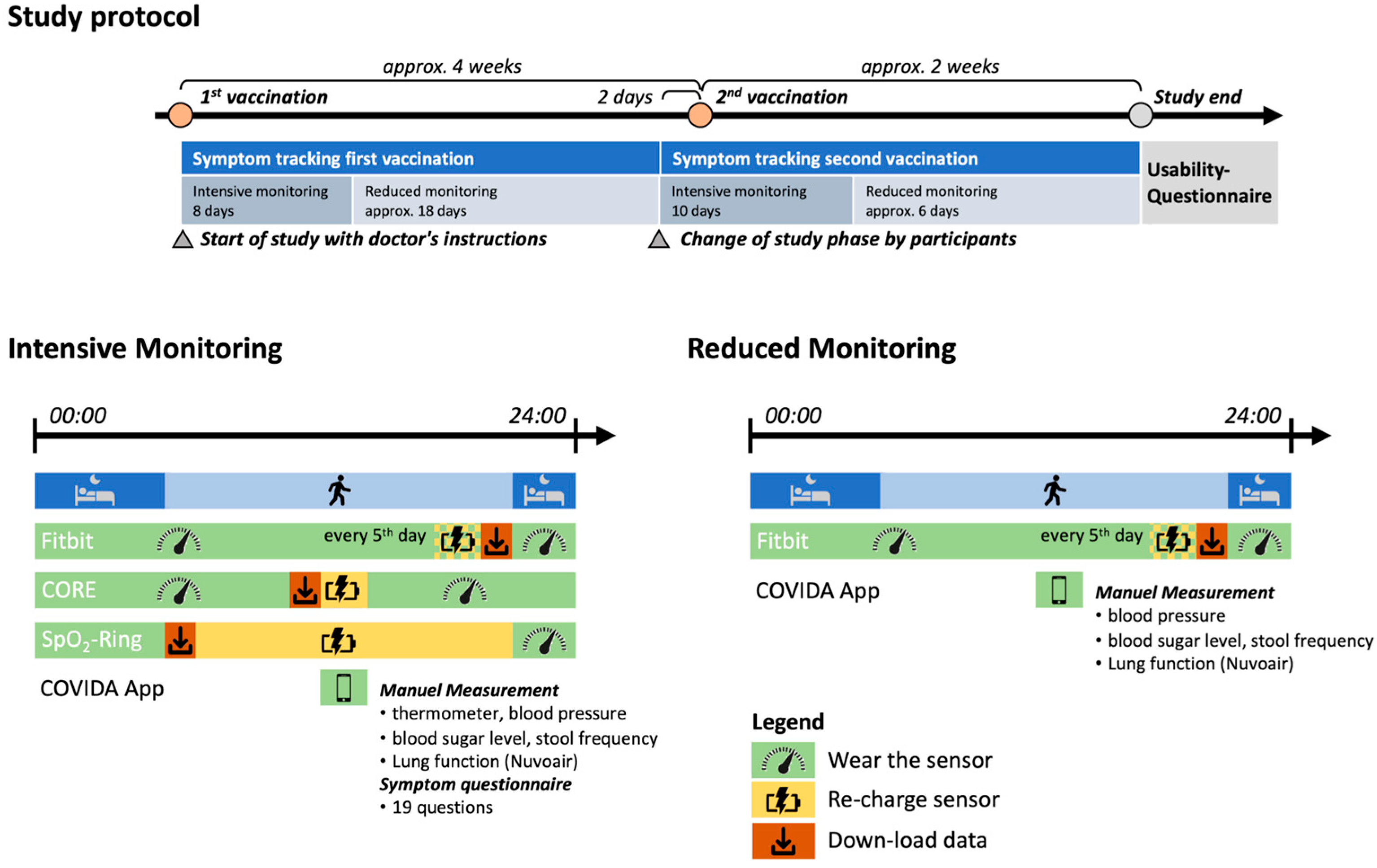
2.1. Study Design
2.2. Study Patients
2.3. Study Materials
2.4. Statistical Analysis
3. Results
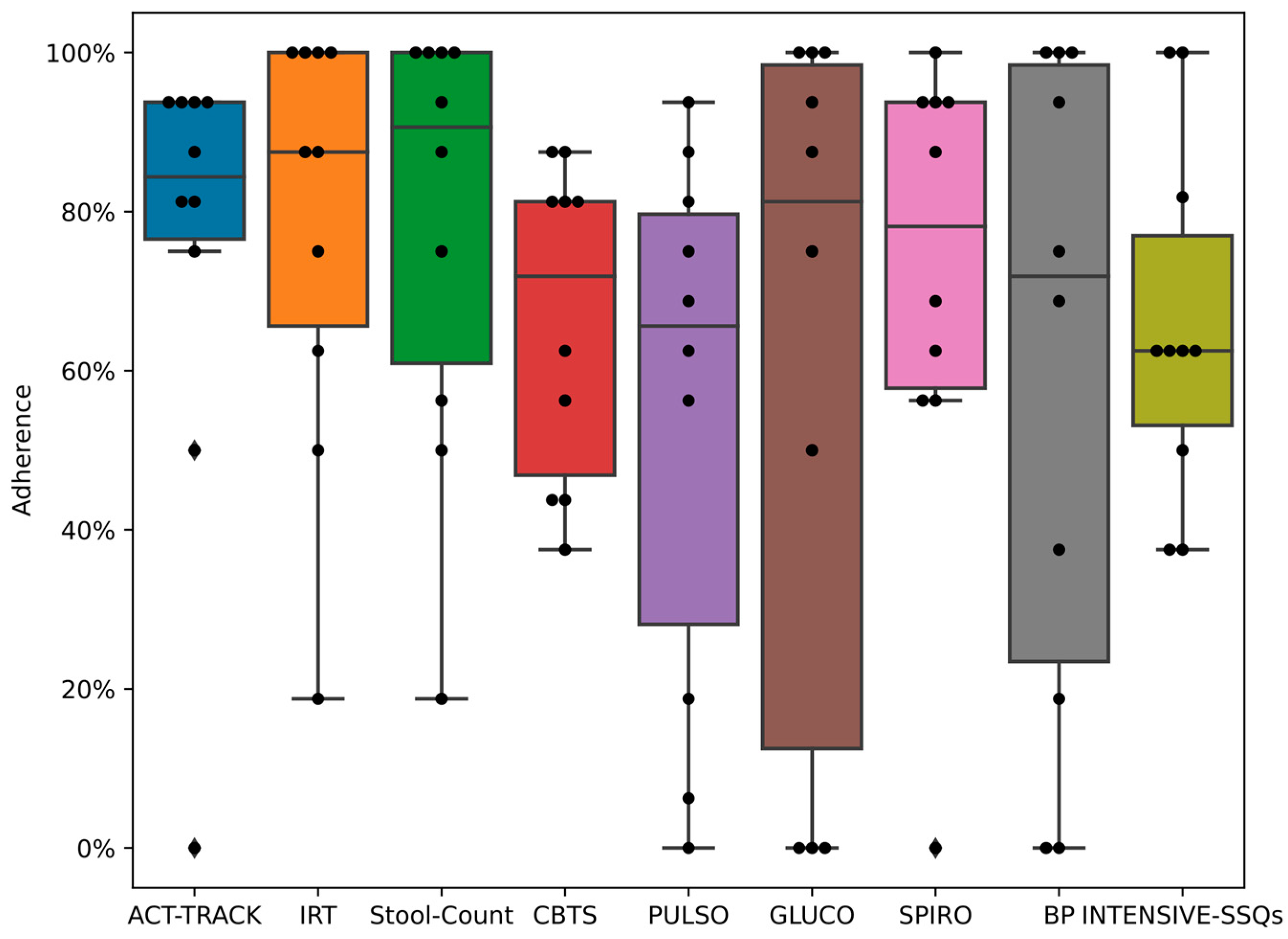
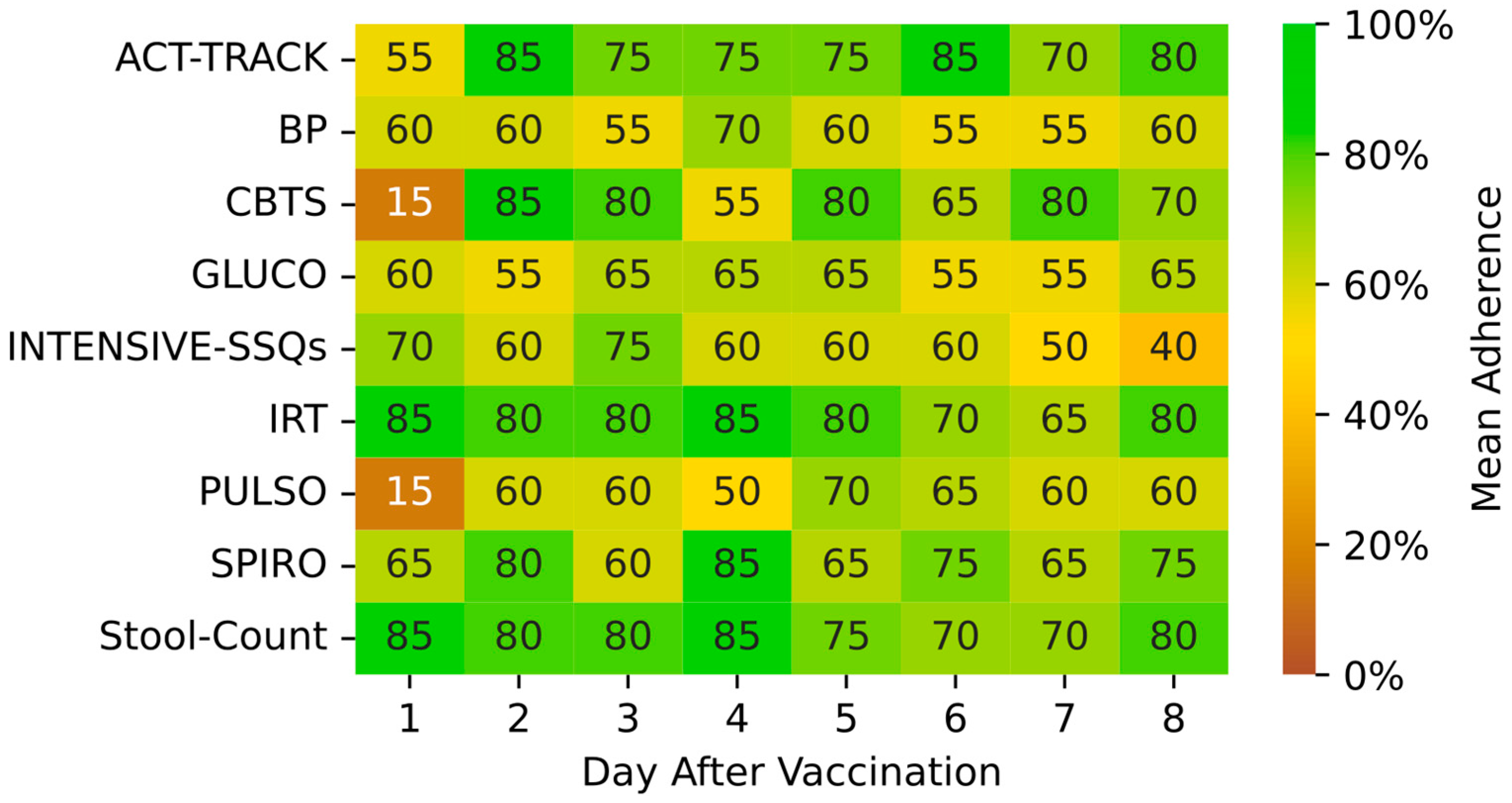
3.1. Patient Adherence and Technical Considerations
3.2. Patient Satisfaction and Acceptance for Continued Use
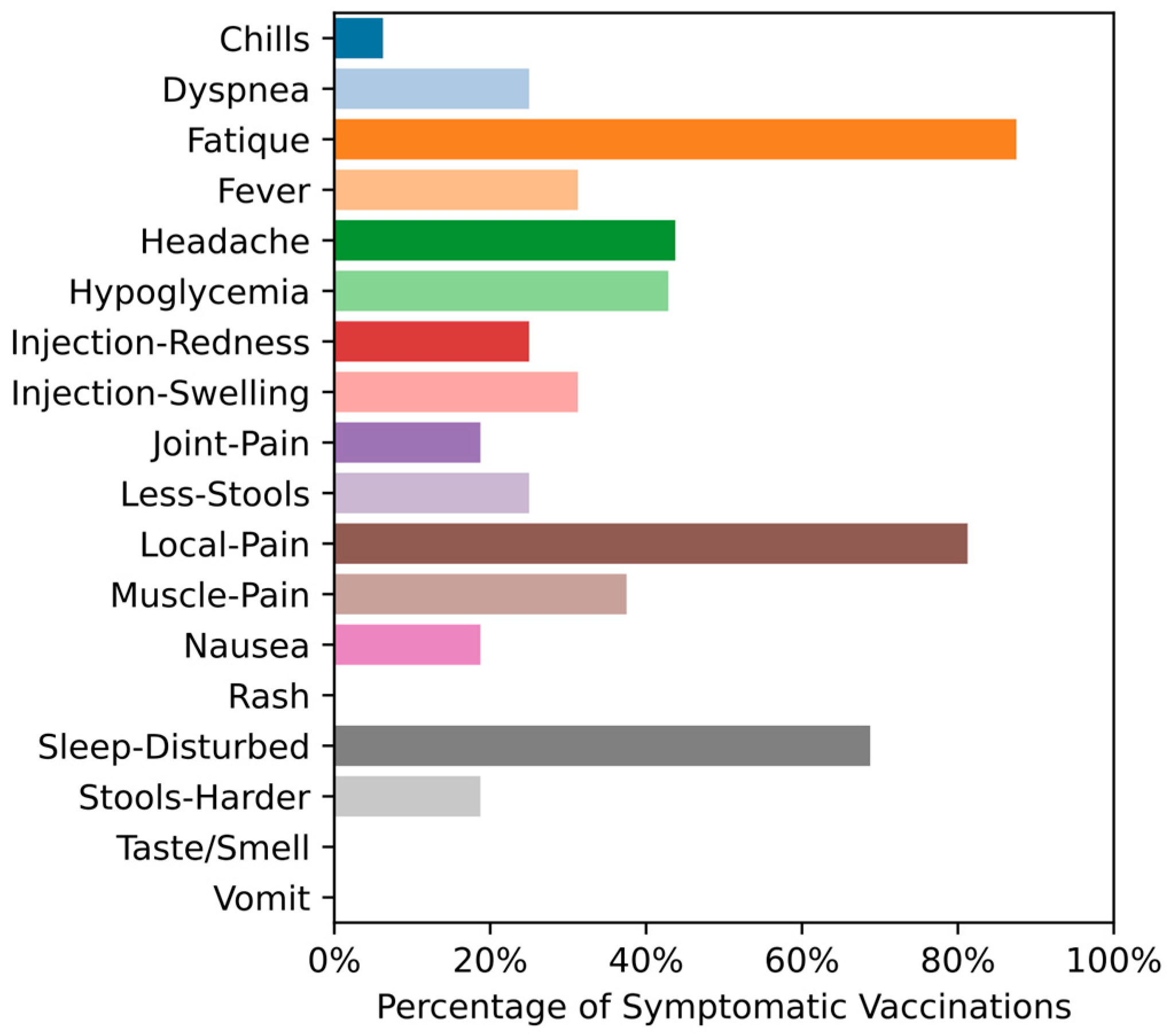
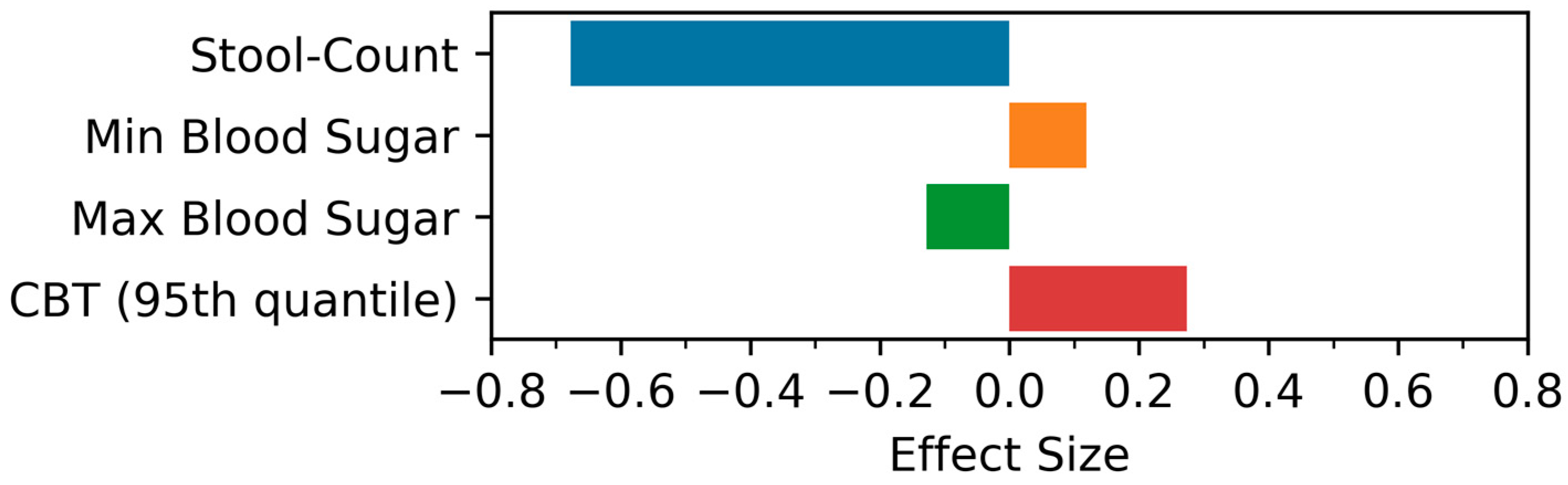
3.3. Physiological Data and Effect Size Estimation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LTR | Lung Transplant Recipients |
| FEV1 | Forced Expiratory Volume in 1 s |
| FVC | Forced Vital Capacity |
| GSM | Global System for Mobile Communications |
| HRA | Human Research Act |
| PROM | Patient-Reported Outcome |
| PULSO | PULSOoximeter |
| CBTS | Core Body Temperature Sensor |
| ACT-TRACK | ACTivity-TRACKer |
| IRT | InfRared Thermometer |
| INTENSIVE-SSQs | Intensive Symptom and Sign Questionnaires |
| REDUCED-SSQs | Reduced Symptom and Sign Questionnaires |
| SPIRO | SPIROmeter |
| BP | Blood Pressure |
| GLUC | GLUCOmeter |
| Systolic-BP | Systolic-Blood Pressure |
| Diastolic-BP | Diastolic-Blood Pressure |
| Max-BS | Max Blood Sugar |
| Min-BS | Min Blood Sugar |
| Stool-Count | Stool Count |
| Local Pain | Pain at the Injection Site |
| Local Erythema | Erythema at the injection site |
| Local Swelling | Swelling of the injection site |
| Rash | having Rash anywhere else (not at the injection site) |
| Headache | having Headache |
| Muscle-Pain | having Muscle Pain |
| Joint-Pain | having Joint Pain |
| Chills | having Chills |
| Smell | change in smelling or tasting capability |
| Fever | having Fever feelings or Fever |
| Fatigue | being tired |
| Dyspnea | shortness of breath |
| Hypoglycemia | having hypoglycemia |
| Less Stools | Reduced stool count as compared to usual |
| Stool harder | change in stool consistency (harder) |
| Sleep-Disturbed | change in sleep quality (worse) |
| Nausea | Having Nausea |
| Vomit | Vomiting |
| Symptom | having any other Symptoms |
| Symptom-Intensity | Intensity of the other Symptom |
References
- Gholamzadeh, M.; Abtahi, H.; Safdari, R. Telemedicine in lung transplant to improve patient-centered care: A systematic review. Int. J. Med. Inform. 2022, 167, 104861. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Smith, P.J.; Sherwood, A.; Mabe, S.; Snyder, L.; Frankel, C.; McKee, D.C.; Hamilton, N.; Keefe, F.J.; Shearer, S.; et al. Remote Therapy to Improve Outcomes in Lung Transplant Recipients: Design of the INSPIRE-III Randomized Clinical Trial. Transplant. Direct 2020, 6, e535. [Google Scholar] [CrossRef]
- Schenkel, F.A.; Barr, M.L.; McCloskey, C.C.; Possemato, T.; O’Conner, J.; Sadeghi, R.; Bembi, M.; Duong, M.; Patel, J.; Hackmann, A.E.; et al. Use of a Bluetooth tablet-based technology to improve outcomes in lung transplantation: A pilot study. Am. J. Transplant. 2020, 20, 3649–3657. [Google Scholar] [CrossRef]
- Mofaz, M.; Yechezkel, M.; Guan, G.; Brandeau, M.L.; Patalon, T.; Gazit, S.; Yamin, D.; Shmueli, E. Self-Reported and Physiologic Reactions to Third BNT162b2 mRNA COVID-19 (Booster) Vaccine Dose. Emerg. Infect. Dis. 2022, 28, 1375–1383. [Google Scholar] [CrossRef]
- Koc, O.M.; Pierco, M.; Remans, K.; Van den Hende, T.; Verbeek, J.; Van Malenstein, H.; Van der Merwe, S.; Robaeys, G.; Monbaliu, D.; Pirenne, J.; et al. Telemedicine based remote monitoring after liver transplantation: Feasible in a select group and a more stringent control of immunosuppression. Clin. Transplant. 2022, 36, e14494. [Google Scholar] [CrossRef]
- Suhling, H.; Rademacher, J.; Zinowsky, I.; Fuge, J.; Greer, M.; Warnecke, G.; Smits, J.M.; Bertram, A.; Haverich, A.; Welte, T.; et al. Conventional vs. tablet computer-based patient education following lung transplantation—A randomized controlled trial. PLoS ONE 2014, 9, e90828. [Google Scholar] [CrossRef]
- Sengpiel, J.; Fuehner, T.; Kugler, C.; Avsar, M.; Bodmann, I.; Boemke, A.; Simon, A.; Welte, T.; Gottlieb, J. Use of telehealth technology for home spirometry after lung transplantation: A randomized controlled trial. Prog. Transplant. 2010, 20, 310–317. [Google Scholar] [CrossRef]
- Rosenberger, E.M.; DeVito Dabbs, A.J.; DiMartini, A.F.; Landsittel, D.P.; Pilewski, J.M.; Dew, M.A. Long-Term Follow-up of a Randomized Controlled Trial Evaluating a Mobile Health Intervention for Self-Management in Lung Transplant Recipients. Am. J. Transplant. 2017, 17, 1286–1293. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, S.M.; Lindgren, B.R.; Robiner, W.; Lindquist, R.; Hertz, M.; Carlin, B.P.; VanWormer, A. A randomized controlled trial comparing health and quality of life of lung transplant recipients following nurse and computer-based triage utilizing home spirometry monitoring. Telemed. E-Health 2013, 19, 897–903. [Google Scholar] [CrossRef] [Green Version]
- Keating, B.J.; Mukhtar, E.H.; Elftmann, E.D.; Eweje, F.R.; Gao, H.; Ibrahim, L.I.; Kathawate, R.G.; Lee, A.C.; Li, E.H.; Moore, K.A.; et al. Early detection of SARS-CoV-2 and other infections in solid organ transplant recipients and household members using wearable devices. Transpl. Int. 2021, 34, 1019–1031. [Google Scholar] [CrossRef]
- Brakenhoff, T.B.; Franks, B.; Goodale, B.M.; van de Wijgert, J.; Montes, S.; Veen, D.; Fredslund, E.K.; Rispens, T.; Risch, L.; Dowling, A.V.; et al. A prospective, randomized, single-blinded, crossover trial to investigate the effect of a wearable device in addition to a daily symptom diary for the Remote Early Detection of SARS-CoV-2 infections (COVID-RED): A structured summary of a study protocol for a randomized controlled trial. Trials 2021, 22, 694. [Google Scholar] [CrossRef]
- Gepner, Y.; Mofaz, M.; Oved, S.; Yechezkel, M.; Constantini, K.; Goldstein, N.; Eisenkraft, A.; Shmueli, E.; Yamin, D. Utilizing wearable sensors for continuous and highly-sensitive monitoring of reactions to the BNT162b2 mRNA COVID-19 vaccine. Commun. Med. 2022, 2, 27. [Google Scholar] [CrossRef]
- Schuurmans, M.M.; Tini, G.M.; Zuercher, A.; Hofer, M.; Benden, C.; Boehler, A. Practical approach to emergencies in lung transplant recipients: How we do it. Respiration 2012, 84, 163–175. [Google Scholar] [CrossRef] [Green Version]
- Jacobsen, M.; Rottmann, P.; Dembek, T.A.; Gerke, A.L.; Gholamipoor, R.; Blum, C.; Hartmann, N.U.; Verket, M.; Kaivers, J.; Jager, P.; et al. Feasibility of Wearable-Based Remote Monitoring in Patients During Intensive Treatment for Aggressive Hematologic Malignancies. JCO Clin. Cancer Inform. 2022, 6, e2100126. [Google Scholar] [CrossRef]
- Kohlbrenner, D.; Clarenbach, C.F.; Ivankay, A.; Zimmerli, L.; Gross, C.S.; Kuhn, M.; Brunschwiler, T. Multisensory Home-Monitoring in Individuals with Stable Chronic Obstructive Pulmonary Disease and Asthma: Usability Study of the CAir-Desk. JMIR Hum. Factors 2022, 9, e31448. [Google Scholar] [CrossRef]
- Laugwitz, B.H.T.; Schrepp, M. Construction and Evaluation of a User Experience Questionnaire. In Lecture Notes in Computer Science; Holzinger, A., Ed.; Springer: Berlin/Heidelberg, Germany, 2008; Volume 5298, pp. 63–76. [Google Scholar]
- Schrepp, M.H.A.; Thomaschewski, J. Applying the User Experience Questionnaire (UEQ) in Different Evaluation Scenarios. In Design, User Experience, and Usability. Theories, Methods, and Tools for Designing the User Experience; Marcus, A., Ed.; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2014; Volume 8517, pp. 383–392. [Google Scholar]
- Villavicencio, A.; Ebisu, Y.; Raja, M.; Sanchez-Covarrubias, A.P.; Reynolds, J.M.; Natori, Y. Adverse events after SARS-CoV-2 vaccination in solid organ transplant recipients: A systematic review. Transpl. Infect. Dis. 2022, 24, e13936. [Google Scholar] [CrossRef]
- Gross, C.; Kohlbrenner, D.; Clarenbach, C.F.; Ivankay, A.; Brunschwiler, T.; Nordmann, Y.; Wangenheim, F.V. A Telemonitoring and Hybrid Virtual Coaching Solution “CAir” for Patients with Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e20412. [Google Scholar] [CrossRef]
- Murray, K.R.; Foroutan, F.; Amadio, J.M.; Posada, J.D.; Kozuszko, S.; Duhamel, J.; Tsang, K.; Farkouh, M.E.; McDonald, M.; Billia, F.; et al. Remote Mobile Outpatient Monitoring in Transplant (Reboot) 2.0: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2021, 10, e26816. [Google Scholar] [CrossRef]
- Sidhu, A.; Chaparro, C.; Chow, C.W.; Davies, M.; Singer, L.G. Outcomes of telehealth care for lung transplant recipients. Clin. Transplant. 2019, 33, e13580. [Google Scholar] [CrossRef]
- Finkelstein, S.M.; MacMahon, K.; Lindgren, B.R.; Robiner, W.N.; Lindquist, R.; VanWormer, A.; Hertz, M.I. Development of a remote monitoring satisfaction survey and its use in a clinical trial with lung transplant recipients. J. Telemed. Telecare 2012, 18, 42–46. [Google Scholar] [CrossRef] [Green Version]
- Hajesmaeel-Gohari, S.; Bahaadinbeigy, K. The most used questionnaires for evaluating telemedicine services. BMC Med. Inform. Decis. Mak. 2021, 21, 36. [Google Scholar] [CrossRef]
- Schrepp, M.; Hinderks, A.; Thomaschewski, J. Construction of a Benchmark for the User Experience Questionnaire (UEQ). Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Hallett, A.M.; Greenberg, R.S.; Boyarsky, B.J.; Shah, P.D.; Ou, M.T.; Teles, A.T.; Krach, M.R.; Lopez, J.I.; Werbel, W.A.; Avery, R.K.; et al. SARS-CoV-2 messenger RNA vaccine antibody response and reactogenicity in heart and lung transplant recipients. J. Heart Lung Transplant. 2021, 40, 1579–1588. [Google Scholar] [CrossRef]
- Ou, M.T.; Boyarsky, B.J.; Motter, J.D.; Greenberg, R.S.; Teles, A.T.; Ruddy, J.A.; Krach, M.R.; Jain, V.S.; Werbel, W.A.; Avery, R.K.; et al. Safety and Reactogenicity of 2 Doses of SARS-CoV-2 Vaccination in Solid Organ Transplant Recipients. Transplantation 2021, 105, 2170–2174. [Google Scholar] [CrossRef]
- Wu, M.; Li, S.X.; Xue, P.; Zhou, J.; Tang, X. COVID-19 Vaccine Could Trigger the Relapse of Secondary Hypersomnia. Nat. Sci. Sleep 2021, 13, 2267–2271. [Google Scholar] [CrossRef]
- Gautschi, F.; Hage, R.; Steinack, C.; Schuurmans, M.M. Evaluation of possible adverse events in relationship to the SARS-CoV-2 vaccination in cystic fibrosis patients with or without lung transplantation: A retrospective single-centre case series. J. Cyst. Fibros. 2022, 21, S55. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Relevant Modalities a | Threshold | Adherence Day Threshold |
|---|---|---|
| Physical activity, wrist-worn a | Step count; (threshold) use >20 h/day | Steps ≥ 100 |
| Core Body Temperature a | Continuous Temperature measurements; use >20 h/day | Recording ≥ 1 h |
| Symptoms, Signs and Measurements a | COVIDA symptom and measurement log questionnaire; at least one answer provided | Completed questionnaire |
| Spirometry a | Forced expiratory volume in 1 s, forced vital capacity; both values provided | ≥3 valid exhalations |
| Forehead Infrared Temperature skin sensor a | Forehead Temperature: value provided | Recording ≥ 1 h |
| Nocturnal Pulmometry SpO2-Ring b | Oxygen saturation; use >5 h/day | Recording ≥ 1 audio file |
| Blood pressure and blood glucose monitoring b | diastolic/systolic value provided, blood glucose result provided | Recording ≥ 1 result |
| Characteristics | Lung Transplant Recipients (n = 10) |
|---|---|
| Age (years), median (range) | 47.5 (19–62) |
| Sex (female/male), n (%) | 4/6 (40%/60%) |
| Underlying diagnosis, no | 2 Pulmonary fibrosis 3 COPD 5 Cystic fibrosis |
| Time since transplant, median (range), days | 1579.5 (40–6842) |
| Forced expiratory volume in 1 s (FEV1) (% predicted), median (range) | 77.5 (40–130) |
| Forced vital capacity (FVC) (% predicted), median (range) | 76.5 (36–120) |
| Smoking status (yes/no), n (%) | No 0/10 (0%/100%) |
| Comment No | Text Information Provided by Patient | Comment by Research Team |
|---|---|---|
| 1 | It is very exciting for me to see how my vital parameters are and additionally also my daily step count | Positive feedback |
| 2 | Monitoring OK for vaccination period, but not for every day all week. Measurements 3× per week would be better/ideal. Especially when used over long periods of time. | Positive feedback |
| 3 | The apparatus did not function well, therefore it was not appropriate for me. The controlling/surveillance is too extreme. | Negative feedback |
| 4 | The COVIDA app should have a correction button or at least give one the option to go back one step. Otherwise, clear and good. | Suggestion improvement software |
| 5 | The app (COVIDA app) unfortunately gets stuck so that one quite often spends more time entering the vital parameters | Technical issue |
| 6 | COVIDA app: the symptom log should be better editable | Suggestion improvement software |
| 7 | COVIDA app: the entry of data should be possible until 23.59 (not only until 23:00) | Suggestion improvement software |
| 8 | The Core thermometer sometimes falls off | Usability issue |
| 9 | One has to be careful not to lose the CORE thermometer depending on the trousers one wears. | Usability issue |
| 10 | The Core thermometer is interesting. When one is feeling well I would not continue using it 24/7 since one measures the temperature with the forehead infrared thermometer | Addressing double measurements by two methods |
| 11 | Suggest a Core thermometer with integrated chest belt analogue to “Polar T31 chest belt”. | Suggested improvement hardware |
| 12 | The wrist accelerometer was for me a bit uncomfortable | Adverse device event |
| 13 | The accelerometer can lead to wrong statements, for example in court | Not totally clear what the patient means by this. |
| 14 | The Ring-Pulse oximeter disturbs when used for longer durations, especially when one is still awake | Usability issue |
| 15 | The Ring-Pulse oximeter is not a good idea for sleeping it always falls off. | Usability issue |
| 16 | Spirometer: I would prefer an oval mouthpiece | Suggested improvement hardware |
| Pat No | COVIDA-Desk (Y or N) | Ring-Pulsoxy | CORE Temp | Accelero-Meter | Infrared Thermometer | COVIDA App | Spirometer |
|---|---|---|---|---|---|---|---|
| 1 | Y | Neutral | (Y) | Neutral | Y | Y | Y |
| 2 | Y | (N) | (Y) | (Y) | Y | (Y) | Y |
| 3 | Y | Neutral | Neutral | Y | Neutral | (Y) | (Y) |
| 4 | N | Neutral | (N) | Y | Y | Y | Y |
| 5 | Y | Neutral | (Y) | Y | (Y) | (Y) | (Y) |
| 6 | N | N | (N) | Y | Y | Y | (Y) |
| 7 | N | (N) | (N) | Neutral | (Y) | (N) | (Y) |
| 8 | Y | (Y) | Y | Y | (Y) | Y | Y |
| 9 | Y | (N) | (N) | Y | Neutral | (Y) | Y |
| 10 | N | (N) | N | N | (Y) | (N) | (Y) |
| Y or (Y) | 6 | 1 | 4 | 7 | 8 | 8 | 10 |
| Neutral | 3 | 1 | 2 | 2 | 0 | 0 | |
| N or (N) | 4 | 5 | 5 | 1 | 0 | 2 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuurmans, M.M.; Muszynski, M.; Li, X.; Marcinkevičs, R.; Zimmerli, L.; Monserrat Lopez, D.; Michel, B.; Weiss, J.; Hage, R.; Roeder, M.; et al. Multimodal Remote Home Monitoring of Lung Transplant Recipients during COVID-19 Vaccinations: Usability Pilot Study of the COVIDA Desk Incorporating Wearable Devices. Medicina 2023, 59, 617. https://doi.org/10.3390/medicina59030617
Schuurmans MM, Muszynski M, Li X, Marcinkevičs R, Zimmerli L, Monserrat Lopez D, Michel B, Weiss J, Hage R, Roeder M, et al. Multimodal Remote Home Monitoring of Lung Transplant Recipients during COVID-19 Vaccinations: Usability Pilot Study of the COVIDA Desk Incorporating Wearable Devices. Medicina. 2023; 59(3):617. https://doi.org/10.3390/medicina59030617
Chicago/Turabian StyleSchuurmans, Macé M., Michal Muszynski, Xiang Li, Ričards Marcinkevičs, Lukas Zimmerli, Diego Monserrat Lopez, Bruno Michel, Jonas Weiss, René Hage, Maurice Roeder, and et al. 2023. "Multimodal Remote Home Monitoring of Lung Transplant Recipients during COVID-19 Vaccinations: Usability Pilot Study of the COVIDA Desk Incorporating Wearable Devices" Medicina 59, no. 3: 617. https://doi.org/10.3390/medicina59030617