
A Calculator for COVID-19 Severity Prediction Based on Patient Risk Factors and Number of Vaccines Received

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Subjects and Study Design
2.2. Ethics Statement
2.3. SARS-CoV-2 Testing by Real-Time RT-PCR
2.4. Statistical Analyses
3. Results
3.1. Factors Associated with Hospitalization of SARS-CoV-2-Positive Individuals
3.2. Factors Associated with Mortality for SARS-CoV-2-Positive Individuals
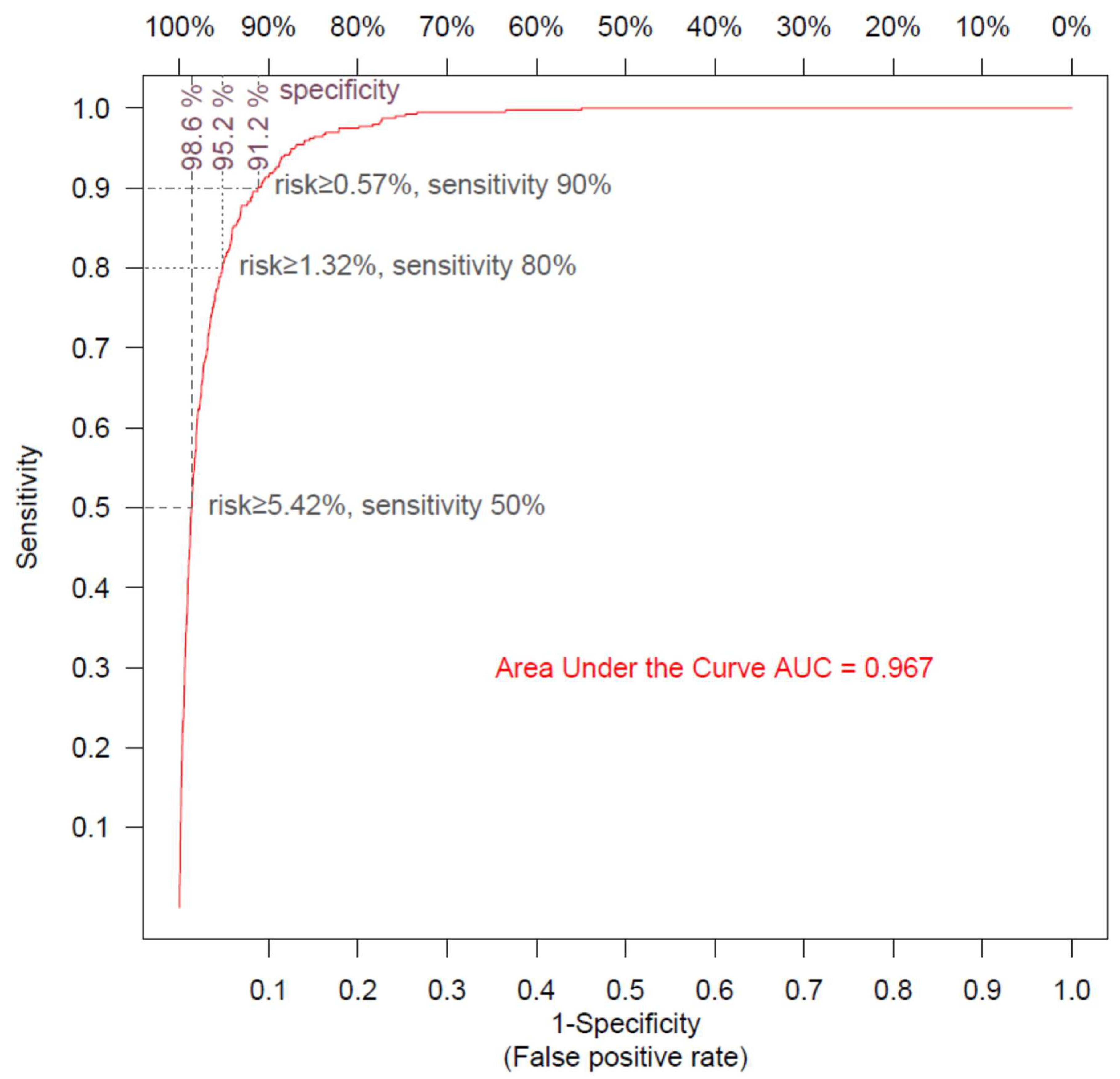
3.3. Risk Calculators
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUC | Area under the curve |
| BMI | Body mass index |
| COPD | Chronic obstructive pulmonary disease |
| COVID-19 | Coronavirus disease of 2019 |
| GFR | Glomerular filtration rate |
| LHS | Leumit Health Services |
| OR | Odds ratio |
| ROC | Receiver operating characteristic |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
References
- Fan, Y.; Chan, K.H.; Hung, I.F.N. Safety and efficacy of COVID-19 vaccines: A systematic review and meta-analysis of different vaccines at phase 3. Vaccines 2021, 9, 989. [Google Scholar] [CrossRef]
- Samaranayake, L.P.; Seneviratne, C.J.; Fakhruddin, K.S. Coronavirus disease 2019 (COVID-19) vaccines: A concise review. Oral Dis. 2021, in press. [Google Scholar] [CrossRef]
- Dyer, O. Covid-19: FDA expert panel recommends authorising molnupiravir but also voices concerns. BMJ 2021, 375, n2984. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Green, P.; Fan, V.S.; Dominitz, J.A.; O’Hare, A.M.; Backus, L.I.; Locke, E.; Eastment, M.C.; Osborne, F.T.; Ioannou, N.G.; et al. Development of COVIDVax Model to Estimate the Risk of SARS-CoV-2-Related Death among 7.6 Million US Veterans for Use in Vaccination Prioritization. JAMA Netw Open. 2021, 4, e214347. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.K. Booster Doses and Prioritizing Lives Saved. N. Engl. J. Med. 2021, 385, 2476–2477. [Google Scholar] [CrossRef]
- Persad, G.; Peek, M.E.; Shah, S.K. Fair Allocation of Scarce Therapies for COVID-19. Clin. Infect. Dis. 2021, 18, ciab1039. [Google Scholar] [CrossRef]
- Rosen, B.; Waitzberg, R.; Israeli, A. Israel’s rapid rollout of vaccinations for COVID-19. Isr. J. Health Policy Res. 2021, 10, 6. [Google Scholar] [CrossRef]
- Raz, A.; Keshet, Y.; Popper-Giveon, A.; Karkabi, M.S. One size does not fit all: Lessons from Israel’s Covid-19 vaccination drive and hesitancy. Vaccine 2021, 39, 4027–4028. [Google Scholar] [CrossRef]
- Experton, B.; Tetteh, H.A.; Lurie, N.; Walker, P.; Elena, A.; Hein, C.S.; Schwendiman, B.; Vincent, J.L.; Burrow, C.R. A predictive model for severe COVID-19 in the medicare population: A tool for prioritizing primary and booster COVID-19 vaccination. Biology 2021, 10, 1185. [Google Scholar] [CrossRef] [PubMed]
- Gimeno-Miguel, A.; Bliek-Bueno, K.; Poblador-Plou, B.; Carmona-Pírez, J.; Poncel-Falcó, A.; González-Rubio, F.; Ioakeim-Skoufa, I.; Pico-Soler, V.; Aza-Pascual-Salcedo, M.; Prados-Torres, A.; et al. Chronic diseases associated with increased likelihood of hospitalization and mortality in 68,913 COVID-19 confirmed cases in Spain: A population-based cohort study. PLoS ONE 2021, 16, e0259822. [Google Scholar] [CrossRef] [PubMed]
- Machado-Alba, J.E.; Valladales-Restrepo, L.F.; Machado-Duque, M.E.; Gaviria-Mendoza, A.; Sánchez-Ramírez, N.; Usma-Valencia, A.F.; Rodríguez-Martínez, E.; Rengifo-Franco, E.; Forero-Supelano, V.H.; Gómez-Ramirez, D.M.; et al. Factors associated with admission to the intensive care unit and mortality in patients with COVID-19, Colombia. PLoS ONE 2021, 16, e0260169. [Google Scholar] [CrossRef] [PubMed]
- Vahey, G.M.; McDonald, E.; Marshall, K.; Martin, S.W.; Chun, H.; Herlihy, R.; Tate, J.E.; Kawasaki, B.; Midgley, C.M.; Alden, N.; et al. Risk factors for hospitalization among persons with COVID-19-Colorado. PLoS ONE 2021, 16, e0256917. [Google Scholar] [CrossRef] [PubMed]
- Dennis, J.M.; Mateen, B.A.; Sonabend, R.; Thomas, N.J.; Patel, K.A.; Hattersley, A.T.; Denaxas, S.; McGovern, A.P.; Vollmer, S.J. Type 2 Diabetes and COVID-19-Related Mortality in the Critical Care Setting: A National Cohort Study in England, March–July 2020. Diabetes Care 2021, 44, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J. Diabetes, obesity, metabolism and SARS-CoV-2 infection: The end of the beginning. Cell Metab. 2021, 33, 479–498. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Gale, C.R.; Kivimäki, M.; Batty, G.D. Overweight, obesity, and risk of hospitalization for COVID-19: A community-based cohort study of adults in the United Kingdom. Proc. Natl. Acad. Sci. USA 2020, 117, 21011–21013. [Google Scholar] [CrossRef]
- Longmore, D.K.; Miller, J.E.; Bekkering, S.; Saner, C.; Mifsud, E.; Zhu, Y.; Saffery, R.; Nichol, A.; Colditz, G.; Short, K.R.; et al. Diabetes and overweight/obesity are independent, nonadditive risk factors for in-hospital severity of COVID-19: An international, multicenter retrospective meta-analysis. Diabetes Care 2021, 44, 1281–1290. [Google Scholar] [CrossRef]
- Zaki, N.; Alashwal, H.; Ibrahim, S. Association of hypertension, diabetes, stroke, cancer, kidney disease and high-cholesterol with COVID-19 disease severity and fatality: A systematic review. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1133–1142. [Google Scholar] [CrossRef]
- Oetjens, M.T.; Luo, J.Z.; Chang, A.; Leader, J.B.; Hartzel, D.N.; Moore, B.S.; Strande, N.T.; Kirchner, H.L.; Ledbetter, D.H.; Justice, A.E.; et al. Electronic health record analysis identifies kidney disease as the leading risk factor for hospitalization in confirmed COVID-19 patients. PLoS ONE 2020, 15, e0242182. [Google Scholar] [CrossRef]
- Lian, Z.; Li, Y.; Wang, W.; Ding, W.; Niu, Z.; Yang, X.; Wu, C. The Prediction Model of Risk Factors for COVID-19 Developing into Severe Illness Based on 1046 Patients with COVID-19. Emerg. Med. Int. 2021, 2021, 7711056. [Google Scholar] [CrossRef]
- Gülsen, A.; König, I.R.; Jappe, U.; Drömann, D. Effect of comorbid pulmonary disease on the severity of COVID-19: A systematic review and meta-analysis. Respirology 2021, 26, 552–565. [Google Scholar] [CrossRef]
- Hosseinzadeh, R.; Goharrizi, M.A.S.B.; Bahardoust, M.; Alvanegh, A.G.; Ataee, M.R.; Bagheri, M.; Navidiyan, E.S.; Zijoud, S.R.H.; Heiat, M. Should all patients with hypertension be worried about developing severe coronavirus disease 2019 (COVID-19)? Clin. Hypertens. 2021, 27, 3. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.; Wee, J.H.; Kim, J.H.; Choi, H.G. The effects of previous asthma and COPD on the susceptibility to and severity of COVID-19: A nationwide cohort study in South Korea. J. Clin. Med. 2021, 10, 4626. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Zeng, M.; Wang, H.; Qin, C.; Hou, H.-Y.; Sun, Z.-Y.; Xu, S.-P.; Wang, G.-P.; Guo, C.-L.; Deng, Y.-K.; et al. Distinct effects of asthma and COPD comorbidity on disease expression and outcome in patients with COVID-19. Allergy Eur. J. Allergy Clin. Immunol. 2021, 76, 483–496. [Google Scholar] [CrossRef]
- Czernichow, S.; Beeker, N.; Rives-Lange, C.; Guerot, E.; Diehl, J.-L.; Katsahian, S.; Hulot, J.-S.; Poghosyan, T.; Carette, C.; Jannot, A.-S. Obesity Doubles Mortality in Patients Hospitalized for Severe Acute Respiratory Syndrome Coronavirus 2 in Paris Hospitals, France: A Cohort Study on 5795 Patients. Obesity 2020, 28, 2282–2289. [Google Scholar] [CrossRef]
- Recalde, M.; Roel, E.; Pistillo, A.; Sena, A.G.; Prats-Uribe, A.; Ahmed, W.-U.-R.; Alghoul, H.; Alshammari, T.M.; Alser, O.; Areia, C.; et al. Characteristics and outcomes of 627,044 COVID-19 patients living with and without obesity in the United States, Spain and the United Kingdom. Int. J. Obes. 2021, 45, 2347–2357. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M. The importance of hypertension as a risk factor for severe illness and mortality in COVID-19. Anaesthesia 2020, 75, 976–977. [Google Scholar] [CrossRef]
- Du, Y.; Zhou, N.; Zha, W.; Lv, Y. Hypertension is a clinically important risk factor for critical illness and mortality in COVID-19: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 745–755. [Google Scholar] [CrossRef]
- Liang, X.; Shi, L.; Wang, Y.; Xiao, W.; Duan, G.; Yang, H.; Wang, Y. The association of hypertension with the severity and mortality of COVID-19 patients: Evidence based on adjusted effect estimates. J. Infect. 2020, 81, e44–e47. [Google Scholar] [CrossRef]
- Meng, Y.; Lu, W.; Guo, E.; Liu, J.; Yang, B.; Wu, P.; Lin, S.; Peng, T.; Fu, Y.; Li, F.; et al. Cancer history is an independent risk factor for mortality in hospitalized COVID-19 patients: A propensity score-matched analysis. J. Hematol. Oncol. 2020, 13, 75. [Google Scholar] [CrossRef]
- Israel, A.; Merzon, E.; Schäffer, A.A.; Golan-Cohen, A.; Ruppin, E.; Magen, E.; Vinker, S. Elapsed time since BNT162b2 vaccine and risk of SARS-CoV-2 infection: Test negative design study. BMJ 2021, 375, e067873. [Google Scholar] [CrossRef]
- Rennert, G.; Peterburg, Y. Prevalence of selected chronic diseases in Israel. Isr. Med. Assoc. J. 2001, 3, 404–408. [Google Scholar] [PubMed]
- Hamood, R.; Hamood, H.; Merhasin, I.; Keinan-Boker, L. A feasibility study to assess the validity of administrative data sources and self-reported information of breast cancer survivors. Isr. J. Health Policy Res. 2016, 5, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Lasko, T.A.; Bhagwat, J.G.; Zou, K.H.; Ohno-Machado, L. The use of receiver operating characteristic curves in biomedical informatics. J. Biomed. Inform. 2005, 38, 404–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamidi, T.K.K.; Tran-Nguyen, T.K.; Melvin, R.L.; Worthey, E.A. Development of An Individualized Risk Prediction Model for COVID-19 Using Electronic Health Record Data. Front. Big Data 2021, 4, 675882. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.A.; Mehta, N.; Diaz-Ordaz, K.; Lyons, R.A.; Sheikh, A.; Rahman, S.; Valabhji, J.; Sellen, P.; Haq, N.; et al. Risk prediction of COVID-19 related death and hospital admission in adults after COVID-19 vaccination: National prospective cohort study. BMJ 2021, 374, n2244. [Google Scholar] [CrossRef]
- Mauer, N.; Chiecca, G.; Carioli, G.; Gianfredi, V.; Iacoviello, L.; Bertagnolio, S.; Guerra, R.; Odone, A.; Signorelli, C. The First 110,593 COVID-19 Patients Hospitalised in Lombardy: A Regionwide Analysis of Case Characteristics, Risk Factors and Clinical Outcomes. Int. J. Public Health 2022, 67, 1604427. [Google Scholar] [CrossRef]
- Chebotareva, N.; Berns, S.; Androsova, T.; Moiseev, S. Risk factors for invasive and non-invasive ventilatory support and mortality in hospitalized patients with COVID-19. Med. Intensiva 2022, 46, 355. [Google Scholar] [CrossRef]
- Lim, W.S.; Van Der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377. [Google Scholar] [CrossRef] [Green Version]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2021, 28, 202–221. [Google Scholar] [CrossRef]
- Callaway, E.; Ledford, H. How bad is Omicron? What scientists know so far. Nature 2021, 600, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| (A) | |||||
| Not Hospitalized | Hospitalized (Not Deceased) | Deceased | |||
| N (%) | 98,894 (97.9%) | 1752 (1.7%) | 393 (0.4%) | ||
| Vaccines doses | 0 | 82,261 (83.2%) | 1405 (80.2%) | 295 (75.1%) | |
| 1 | 4732 (4.8%) | 138 (7.9%) | 32 (8.1%) | ||
| 2 | 10,436 (10.6%) | 176 (10.0%) | 61 (15.5%) | ||
| 3 | 1465 (1.5%) | 33 (1.9%) | 5 (1.3%) | ||
| Sex | Female | 48,565 (49.1%) | 798 (45.5%) | 169 (43.0%) | |
| Age | Mean (SD) | 29.44 (19.17) | 58.44 (19.03) | 75.27 (13.06) | |
| Age category | 5–11 | 19,603 (19.8%) | 19 (1.1%) | 0 (0.0%) | |
| 12–17 | 15,999 (16.2%) | 30 (1.7%) | 0 (0.0%) | ||
| 18–39 | 34,374 (34.8%) | 245 (14.0%) | 6 (1.5%) | ||
| 40–59 | 20,361 (20.6%) | 561 (32.0%) | 44 (11.2%) | ||
| ≥60 | 8557 (8.7%) | 897 (51.2%) | 343 (87.3%) | ||
| Comorbidities | Hypertension | 9321 (9.4%) | 880 (50.2%) | 301 (76.6%) | |
| Pulmonary disease | 1592 (1.6%) | 167 (9.5%) | 74 (18.8%) | ||
| Malignancy | 2258 (2.3%) | 202 (11.5%) | 83 (21.1%) | ||
| BMI category | Underweight | <18.5 | 22,506 (22.8%) | 44 (2.5%) | 10 (2.5%) |
| Normal | 18.5–25 | 32,373 (32.7%) | 283 (16.2%) | 83 (21.1%) | |
| Overweight | 25–30 | 21,396 (21.6%) | 566 (32.3%) | 126 (32.1%) | |
| Obese I | 30–35 | 10,763 (10.9%) | 444 (25.3%) | 85 (21.6%) | |
| Obese II+ | ≥35 | 5493 (5.6%) | 372 (21.2%) | 72 (18.3%) | |
| *missing* | 6363 (6.4%) | 43 (2.5%) | 17 (4.3%) | ||
| Kidney function GFR category | G1 (normal) | ≥90 | 64,097 (64.8%) | 850 (48.5%) | 95 (24.2%) |
| G2 | 60–89 | 12,622 (12.8%) | 596 (34.0%) | 142 (36.1%) | |
| G3a | 45–59 | 840 (0.8%) | 140 (8.0%) | 68 (17.3%) | |
| G3b | 30–44 | 263 (0.3%) | 74 (4.2%) | 46 (11.7%) | |
| G4/G5 | <30 | 151 (0.2%) | 45 (2.6%) | 37 (9.4%) | |
| *missing* | 20,921 (21.2%) | 47 (2.7%) | 5 (1.3%) | ||
| Hemoglobin A1C range | <6.5 | 38,743 (92.2%) | 1106 (72.2%) | 268 (70.7%) | |
| [6.5, 8.0] | 2129 (5.1%) | 253 (16.5%) | 70 (18.5%) | ||
| [8.0, 10.0] | 815 (1.9%) | 115 (7.5%) | 31 (8.2%) | ||
| ≥10.0 | 328 (0.8%) | 58 (3.8%) | 10 (2.6%) | ||
| *missing* | 56,879 (57.5%) | 220 (12.6%) | 14 (3.6%) | ||
| (B) | |||||
| Not Hospitalized | Hospitalized (Not Deceased) | Deceased | |||
| BMI category | Underweight | <18.5 | 25,090 (25.4%) | 47 (2.7%) | 10 (2.5%) |
| Normal | 18.5–25 | 34,615 (35.0%) | 294 (16.8%) | 85 (21.6%) | |
| Overweight | 25–30 | 22,687 (22.9%) | 593 (33.8%) | 139 (35.4%) | |
| Obese I | 30–35 | 11,006 (11.1%) | 446 (25.5%) | 87 (22.1%) | |
| Obese II+ | ≥35 | 5496 (5.6%) | 372 (21.2%) | 72 (18.3%) | |
| Kidney function GFR category | G1 (normal) | ≥90 | 84,503 (85.4%) | 887 (50.6%) | 90 (22.9%) |
| G2 | 60–89 | 13,124 (13.3%) | 590 (33.7%) | 144 (36.6%) | |
| G3a | 45–59 | 860 (0.9%) | 141 (8.0%) | 71 (18.1%) | |
| G3b | 30–44 | 256 (0.3%) | 87 (5.0%) | 47 (12.0%) | |
| G4/G5 | <30 | 151 (0.2%) | 47 (2.7%) | 41 (10.4%) | |
| Hemoglobin A1C range | <6.5 | 95,481 (96.5%) | 1322 (75.5%) | 282 (71.8%) | |
| [6.5, 8.0] | 2266 (2.3%) | 257 (14.7%) | 70 (17.8%) | ||
| [8.0, 10.0] | 819 (0.8%) | 115 (6.6%) | 31 (7.9%) | ||
| ≥10.0 | 328 (0.3%) | 58 (3.3%) | 10 (2.5%) | ||
| Odds Ratio * | 95% Confidence Interval | p | βi (Coefficient) | |||
|---|---|---|---|---|---|---|
| β0 | (Intercept) | 0.001 | 0.0000 | −6.754369 | ||
| Age | Continuous in years | 1.061 | [1.057–1.064] | 0.0000 | 0.058834 | |
| Sex | Male | 1.000 | reference | 0 | ||
| Female | 0.657 | [0.598–0.722] | 0.0000 | −0.420262 | ||
| Vaccine doses | 0 | 1.000 | reference | 0 | ||
| 1 | 0.823 | [0.694–0.976] | 0.0248 | −0.195301 | ||
| 2 | 0.602 | [0.521–0.697] | 0.0000 | −0.506982 | ||
| 3 | 0.339 | [0.241–0.476] | 0.0000 | −1.082553 | ||
| BMI category | Underweight | <18.5 | 0.937 | [0.697–1.260] | 0.6674 | −0.064998 |
| Normal | 18.5–25 | 1.000 | reference | 0 | ||
| Overweight | 25–30 | 1.324 | [1.158–1.513] | 0.0000 | 0.280302 | |
| Obese I | 30–35 | 1.664 | [1.441–1.922] | 0.0000 | 0.509396 | |
| Obese II+ | ≥35 | 2.932 | [2.514–3.419] | 0.0000 | 1.075528 | |
| Kidney function GFR category | G1 (Normal) | ≥90 | 1.000 | reference | 0 | |
| G2 | 60–89 | 1.058 | [0.947–1.183] | 0.3197 | 0.056446 | |
| G3a | 45–59 | 1.568 | [1.296–1.898] | 0.0000 | 0.450065 | |
| G3b | 30–44 | 2.774 | [2.164–3.555] | 0.0000 | 1.020266 | |
| G4/G5 | <30 | 4.000 | [2.952–5.420] | 0.0000 | 1.386290 | |
| Hemoglobin A1C % | <6.5 | 1.000 | reference | 0 | ||
| [6.5, 8.0] | 1.454 | [1.263–1.673] | 0.0000 | 0.374131 | ||
| [8.0, 10.0] | 1.908 | [1.559–2.334] | 0.0000 | 0.645939 | ||
| ≥10.0 | 3.048 | [2.284–4.068] | 0.0000 | 1.114620 | ||
| Comorbidities | Hypertension | 1.270 | [1.130–1.428] | 0.0001 | 0.239212 | |
| Pulmonary disease | 1.331 | [1.134–1.563] | 0.0005 | 0.286110 | ||
| Malignancy | 1.197 | [1.030–1.390] | 0.0188 | 0.179418 | ||
| Odds Ratio * | 95% Confidence Interval | p | βi (Coefficient) | |||
|---|---|---|---|---|---|---|
| β0 | (Intercept) | 0.000 | 0.0000 | –11.227376 | ||
| Age | Continuous in years | 1.105 | [1.095–1.115] | 0.0000 | 0.099573 | |
| Sex | Male | 1.000 | reference | 0 | ||
| Female | 0.500 | [0.401–0.625] | 0.0000 | –0.692446 | ||
| Vaccine doses | 0 | 1.000 | reference | 0 | ||
| 1 | 0.921 | [0.627–1.354] | 0.6771 | –0.081842 | ||
| 2 | 0.936 | [0.698–1.254] | 0.6561 | –0.066541 | ||
| 3 | 0.223 | [0.091–0.551] | 0.0011 | –1.498783 | ||
| BMI category | Underweight | <18.5 | 2.179 | [1.056–4.496] | 0.0350 | 0.778997 |
| Normal | 18.5–25 | 1.000 | reference | 0 | ||
| Overweight | 25–30 | 0.979 | [0.733–1.307] | 0.8866 | −0.021027 | |
| Obese I | 30–35 | 1.085 | [0.785–1.500] | 0.6196 | 0.081961 | |
| Obese II+ | ≥35 | 1.963 | [1.383–2.786] | 0.0002 | 0.674479 | |
| Kidney function GFR category | G1 (Normal) | ≥90 | 1.000 | reference | 0 | |
| G2 | 60–89 | 1.283 | [0.965–1.705] | 0.0861 | 0.249162 | |
| G3a | 45–59 | 2.000 | [1.390–2.878] | 0.0002 | 0.693180 | |
| G3b | 30–44 | 3.097 | [2.035–4.715] | 0.0000 | 1.130578 | |
| G4/G5 | <30 | 6.888 | [4.389–10.810] | 0.0000 | 1.929831 | |
| Hemoglobin A1C % | <6.5 | 1.000 | reference | 0 | ||
| [6.5, 8.0] | 1.137 | [0.851–1.518] | 0.3842 | 0.128408 | ||
| [8.0, 10.0] | 1.479 | [0.983–2.226] | 0.0602 | 0.391618 | ||
| ≥10.0 | 1.782 | [0.905–3.510] | 0.0948 | 0.577767 | ||
| Comorbidities | Hypertension | 1.348 | [1.011–1.797] | 0.0421 | 0.298497 | |
| Pulmonary disease | 1.475 | [1.113–1.956] | 0.0069 | 0.388824 | ||
| Malignancy | 1.138 | [0.868–1.491] | 0.3489 | 0.129199 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Israel, A.; Schäffer, A.A.; Merzon, E.; Green, I.; Magen, E.; Golan-Cohen, A.; Vinker, S.; Ruppin, E. A Calculator for COVID-19 Severity Prediction Based on Patient Risk Factors and Number of Vaccines Received. Microorganisms 2022, 10, 1238. https://doi.org/10.3390/microorganisms10061238
Israel A, Schäffer AA, Merzon E, Green I, Magen E, Golan-Cohen A, Vinker S, Ruppin E. A Calculator for COVID-19 Severity Prediction Based on Patient Risk Factors and Number of Vaccines Received. Microorganisms. 2022; 10(6):1238. https://doi.org/10.3390/microorganisms10061238
Chicago/Turabian StyleIsrael, Ariel, Alejandro A. Schäffer, Eugene Merzon, Ilan Green, Eli Magen, Avivit Golan-Cohen, Shlomo Vinker, and Eytan Ruppin. 2022. "A Calculator for COVID-19 Severity Prediction Based on Patient Risk Factors and Number of Vaccines Received" Microorganisms 10, no. 6: 1238. https://doi.org/10.3390/microorganisms10061238