
Cutaneous Manifestations in SARS-CoV-2 Infection—A Series of Cases from the Largest Infectious Diseases Hospital in Western Romania


 and
and
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
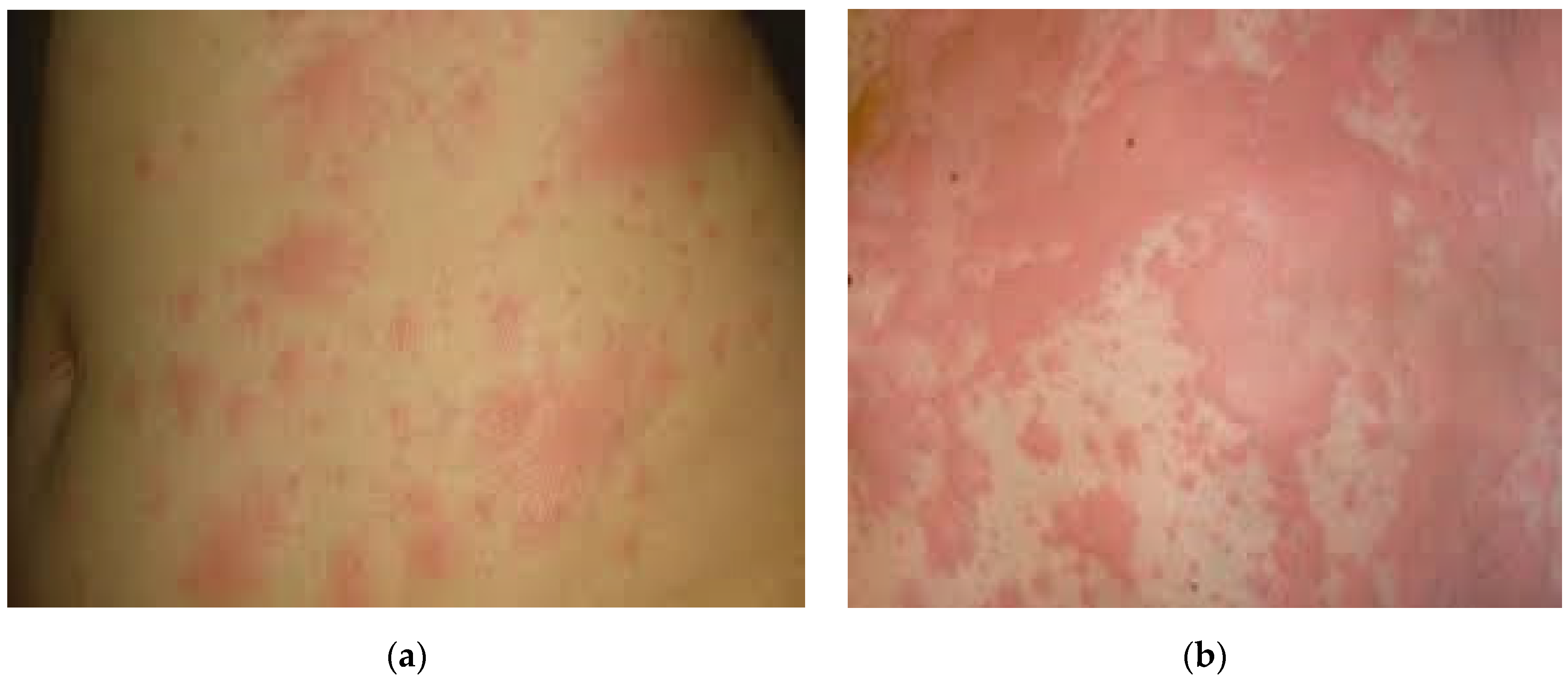
3.1. Case I
3.2. Case II
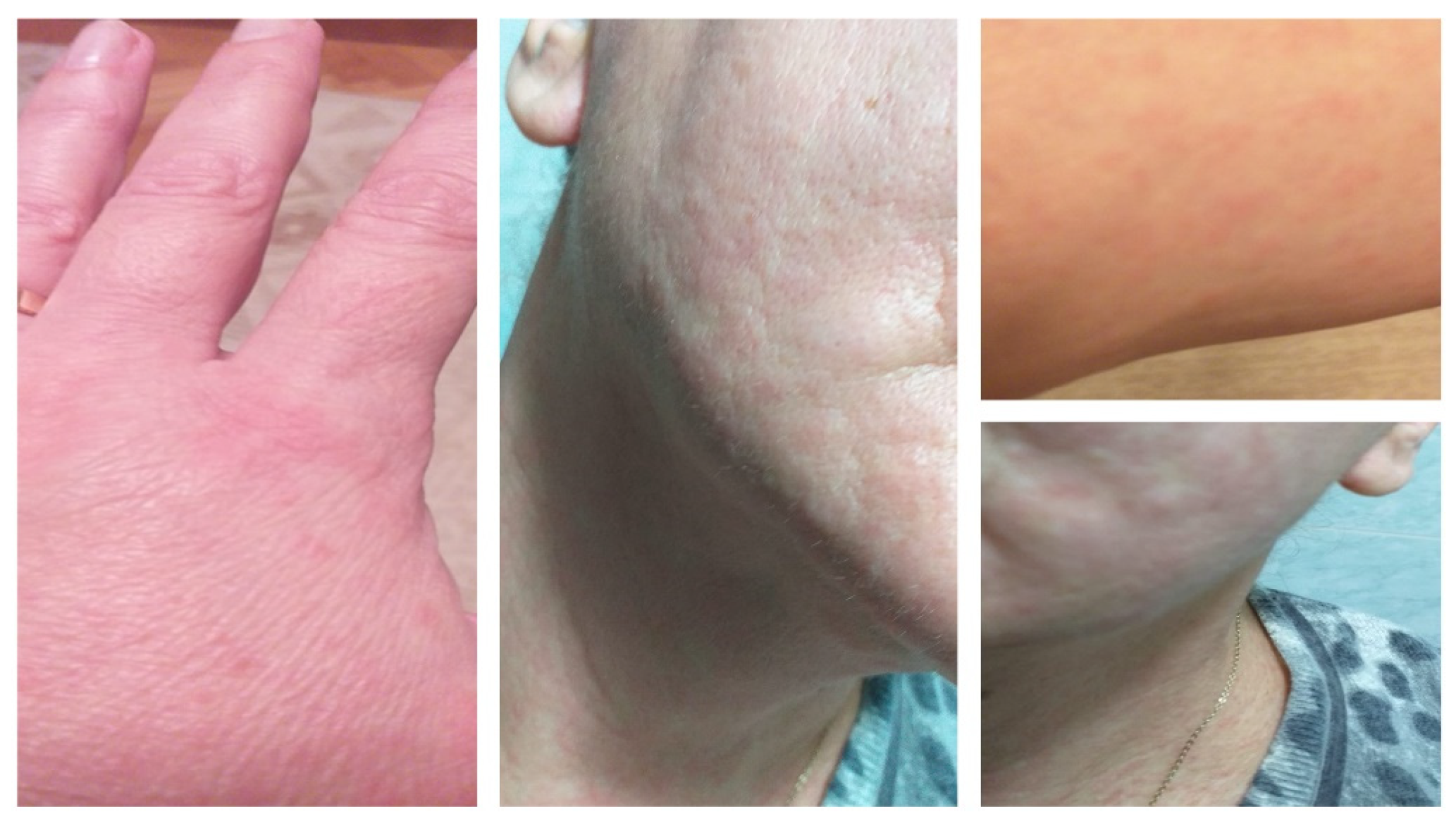
3.3. Case III
3.4. Case IV
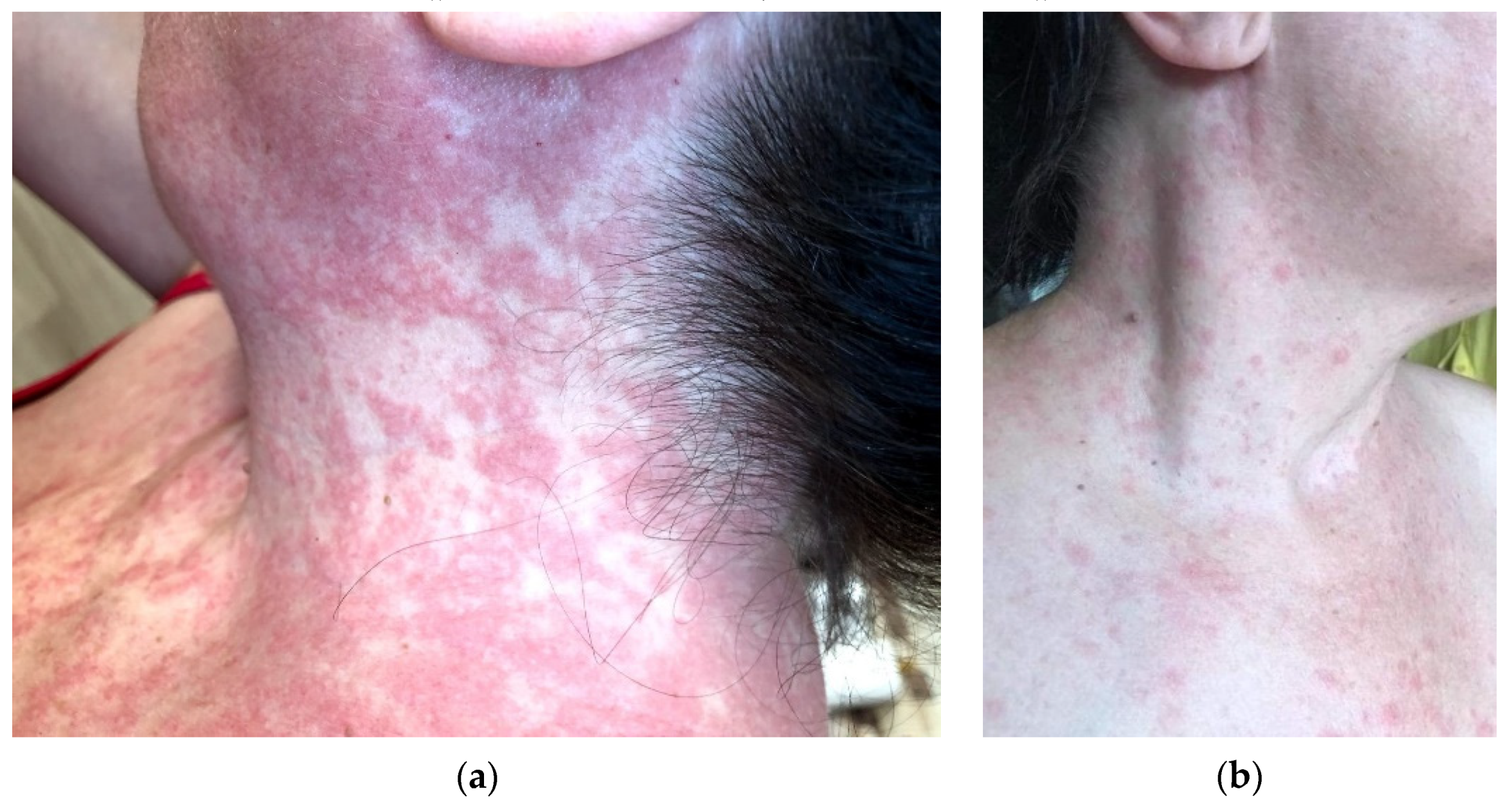
3.5. Case V
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leru, P.M.; Neguleţ, I.E.; Anton, V.F.; Baltă, M.D. Cutaneous Manifestations in COVID-19—Clinical Forms and Differential Diagnosis. Rom. J. Med. Pract. 2020, 15, 292–296. [Google Scholar] [CrossRef]
- Kahn, J.S.; McIntosh, K. History and Recent Advances in Coronavirus Discovery. Pediatr. Infect. Dis. J. 2005, 24, S223–S227. [Google Scholar] [CrossRef] [PubMed]
- Kasper, D.L.; Fauci, A.S. (Eds.) Harrison’s Infectious Diseases, 3rd ed.; McGraw-Hill Education Medical: New York, NY, USA, 2017; pp. 776–777. [Google Scholar]
- Cui, J.; Li, F.; Shi, Z.-L. Origin and Evolution of Pathogenic Coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, S.A.; Watson, A.K.; Swerdlow, D.L. Middle East Respiratory Syndrome (MERS). Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 16 June 2021).
- Cut, T.G.; Tudoran, C.; Lazureanu, V.E.; Marinescu, A.R.; Dumache, R.; Tudoran, M. Spontaneous Pneumomediastinum, Pneumothorax, Pneumopericardium and Subcutaneous Emphysema—Not So Uncommon Complications in Patients with COVID-19 Pulmonary Infection—A Series of Cases. J. Clin. Med. 2021, 10, 1346. [Google Scholar] [CrossRef] [PubMed]
- Shen, K.; Yang, Y.; Wang, T.; Zhao, D.; Jiang, Y.; Jin, R.; Zheng, Y.; Xu, B.; Xie, Z.; Lin, L.; et al. Diagnosis, Treatment, and Prevention of 2019 Novel Coronavirus Infection in Children: Experts’ Consensus Statement. World J. Pediatr. 2020, 16, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Wollina, U.; Karadağ, A.S.; Rowland-Payne, C.; Chiriac, A.; Lotti, T. Cutaneous Signs in COVID-19 Patients: A Review. Dermatol. Ther. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Genovese, G.; Moltrasio, C.; Gaspari, V.; Vezzoli, P.; Maione, V.; Misciali, C.; Sena, P.; Patrizi, A.; Offidani, A.; et al. The Clinical Spectrum of COVID-19–Associated Cutaneous Manifestations: An Italian Multicenter Study of 200 Adult Patients. J. Am. Acad. Dermatol. 2021, 84, 1356–1363. [Google Scholar] [CrossRef]
- Xue, X.; Mi, Z.; Wang, Z.; Pang, Z.; Liu, H.; Zhang, F. High Expression of ACE2 on Keratinocytes Reveals Skin as a Potential Target for SARS-CoV-2. J. Investig. Dermatol. 2021, 141, 206–209.e1. [Google Scholar] [CrossRef]
- Sachdeva, M.; Gianotti, R.; Shah, M.; Bradanini, L.; Tosi, D.; Veraldi, S.; Ziv, M.; Leshem, E.; Dodiuk-Gad, R.P. Cutaneous Manifestations of COVID-19: Report of Three Cases and a Review of Literature. J. Dermatol. Sci. 2020, 98, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the Cutaneous Manifestations of COVID -19: A Rapid Prospective Nationwide Consensus Study in Spain with 375 Cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef]
- Rodriguez-Cerdeira, C.; Uribe-Camacho, B.I.; Silverio-Carrasco, L.; Méndez, W.; Mahesh, A.R.; Tejada, A.; Beirana, A.; Martinez-Herrera, E.; Alba, A.; Arenas, R.; et al. Cutaneous Manifestations in COVID-19: Report on 31 Cases from Five Countries. Biology 2021, 10, 54. [Google Scholar] [CrossRef]
- Singh, H.; Kaur, H.; Singh, K.; Sen, C.K. Cutaneous Manifestations of COVID-19: A Systematic Review. Adv. Wound Care 2021, 10, 51–80. [Google Scholar] [CrossRef]
- Torrelo, A.; Andina, D.; Santonja, C.; Noguera-Morel, L.; Bascuas-Arribas, M.; Gaitero-Tristán, J.; Alonso-Cadenas, J.A.; Escalada-Pellitero, S.; Hernández-Martín, Á.; Torre-Espi, M.; et al. Erythema Multiforme-like Lesions in Children and COVID-19. Pediatr. Dermatol. 2020, 37, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.W.; Tam, Y.C.; Oh, C.C. Skin Manifestations of COVID-19: A Worldwide Review. JAAD Int. 2021, 2, 119–133. [Google Scholar] [CrossRef]
- Freeman, E.E.; McMahon, D.E.; Lipoff, J.B.; Rosenbach, M.; Kovarik, C.; Desai, S.R.; Harp, J.; Takeshita, J.; French, L.E.; Lim, H.W.; et al. The Spectrum of COVID-19–Associated Dermatologic Manifestations: An International Registry of 716 Patients from 31 Countries. J. Am. Acad. Dermatol. 2020, 83, 1118–1129. [Google Scholar] [CrossRef]
- Barnes, B.J.; Adrover, J.M.; Baxter-Stoltzfus, A.; Borczuk, A.; Cools-Lartigue, J.; Crawford, J.M.; Daßler-Plenker, J.; Guerci, P.; Huynh, C.; Knight, J.S.; et al. Targeting Potential Drivers of COVID-19: Neutrophil Extracellular Traps. J. Exp. Med. 2020, 217, e20200652. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Cassano, N.; Genovese, G.; Moltrasio, C.; Vena, G.A. Cutaneous Manifestations in Patients with COVID-19: A Preliminary Review of an Emerging Issue. Br. J. Dermatol. 2020, 183, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Lai, W. Dermatology Staff Participate in Fight against Covid-19 in China. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [Green Version]
- Recalcati, S. Cutaneous Manifestations in COVID-19: A First Perspective. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e212–e213. [Google Scholar] [CrossRef] [PubMed]
- Öksüm Solak, E.; Baran Ketencioğlu, B.; Çinar, S.L.; Kartal, D.; Borlu, M. Coronavirus Disease 2019 (COVID-19) Accompanied by Maculopapular Rash: A Case Study. Cureus 2020, 12, e10414. [Google Scholar] [CrossRef] [PubMed]
- Larenas-Linnemann, D.; Luna-Pech, J.; Navarrete-Rodríguez, E.M.; Rodríguez-Pérez, N.; Arias-Cruz, A.; Blandón-Vijil, M.V.; Del Rio-Navarro, B.E.; Estrada-Cardona, A.; Onuma-Takane, E.; Pozo-Beltrán, C.F.; et al. Cutaneous Manifestations Related to COVID-19 Immune Dysregulation in the Pediatric Age Group. Curr. Allergy Asthma Rep. 2021, 21, 13. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Dianzani, C.; Agozzino, M.; Giuffrida, R.; Marangi, G.F.; di Meo, N.; Morariu, S.-H.; Persichetti, P.; Segreto, F.; Zalaudek, I.; et al. Cutaneous Manifestations in Confirmed COVID-19 Patients: A Systematic Review. Biology 2020, 9, 449. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laboratory Data | Normal Range | Case I Admission | Case I Follow-Up | Case II Admission | Case II Follow-Up |
|---|---|---|---|---|---|
| RBC | 4,000,000–5,500,000/mmc | 4,120,000 | 4,470,000 | 5,090,000 | 4,290,000 |
| Hemoglobin | 11.5–16 g/dL | 10.6 ↓ | 11.5 | 14 | 11.9 |
| Hematocrit | 35.5–47% | 31.5 ↓ | 34.2 ↓ | 42.1 | 36.1 |
| Platelets | 150,000–400,000/mmc | 338,000 | 406,000 | 323,000 | 214,000 |
| WBC | 4000–10,000/mmc | 7280 | 8760 | 9300 | 5920 |
| NE | 1500–7500 (30–65%) | 3790 (52.1%) | 2700 (30.8%) | 5760 (61.9%) | 3530 (59.6%) |
| LY | 3000–9500 (30–55%) | 3170 (43.5%) | 5060 (57.8%) | 2600 (28%) | 1580 (26.7%) |
| Fibrinogen | 1.8–3.5 g/L | 3.18 | 2.66 | 4.62 ↑ | 4.44 ↑ |
| D-Dimers | <0.5 μg/mL | 1.41 ↑ | 0.97 ↑ | 0.97 ↑ | 0.81 ↑ |
| PT | 9.8–12.1 s | 12.8 ↑ | 11.7 | 10 | 10.1 |
| PT | 70–120% | 89.6 | 107.3 | >130 ↑ | >130 ↑ |
| INR | <1.1 | 1.05 | 0.96 | 0.80 | 0.80 |
| APTT | 22.1–28.1 s | 23.6 | 20.4 ↓ | 18.1 ↓ | 19.8 ↓ |
| Lactate | 4.5–19.8 mg/dL | 16.39 | 11.74 | 14.86 | 12.8 |
| AST | 0–32 U/L | 48.1 ↑ | 26.2 | 21.5 | 17.2 |
| ALT | 0–33 U/L | 13.4 | 8.3 | 27.8 | 35.5 ↑ |
| Serum urea | 0–50 mg/dL | 31.7 | 24.1 | 36.3 | 18.5 |
| Creatinine | 0.50–0.90 mg/dL | 0.32 | 0.22 | 0.64 | 0.53 |
| Glucose | 74–106 mg/dL | 129 ↑ | 74 | 95 | 91 |
| Ferritin | 15–150 μg/L | 42.97 | 19.13 | 118.98 | 235.31 ↑ |
| CRP | 0–5 mg/L | 12.5 ↑ | 1.92 | 9.33 ↑ | 26.75 ↑ |
| IL-6 | 0–7 pg/mL | - | <1.50 | - | - |
| Laboratory Data | Normal Range | Case III Admission | Case III First Follow-Up | Case III Second Follow-Up | Case IV Admission | Case IV First Follow-Up | Case IV Second Follow-Up |
|---|---|---|---|---|---|---|---|
| RBC | 4,000,000–5,500,000/mmc | 4,690,000 | 4,700,000 | 5,020,000 | 4,580,000 | 4,900,000 | 4,470,000 |
| Hemoglobin | 11.5–16 g/dL | 14.3 | 14.3 | 15.1 | 14.4 | 15.1 | 13.9 |
| Hematocrit | 35.5–47% | 41.7 | 41.3 | 42.7 | 41.1 | 43.1 | 38.7 |
| Platelets | 150,000–400,000/mmc | 159,000 | 175,000 | 252,000 | 201,000 | 358,000 | 241,000 |
| WBC | 4000–10,000/mmc | 2260 ↓ | 7130 | 6840 | 4700 | 17,760 ↑ | 13,870 ↑ |
| NE | 1500–7500 (30–65%) | 900 (39.9%) ↓ | 6000 (84.2%) | 5660 (82.7%) | 2850 (60.6%) | 15,340 (6.4%) ↑ | 8680 (31.4%) |
| LY | 3000–9500 (30–55%) | 1150 (50.9%) ↓ | 830 (11.6%) ↓ | 880 (12.9%) ↓ | 1540 (32.8%) ↓ | 1900 (10.7%) ↓ | 4360 (31.4%) |
| Fibrinogen | 1.8–3.5 g/L | 3.03 | 3.19 | - | 3.58 ↑ | 4.85 ↑ | 3.39 |
| D-Dimers | <0.5 μg/mL | 0.31 | 0.36 | 0.4 | 0.41 | 0.41 | 0.34 |
| PT | 9.8%–12.1 s | 10.9 | 10.1 | - | 11.7 | 10.5 | - |
| PT | 70–120% | >130 ↑ | >130 ↑ | - | 112.8 | >130 ↑ | - |
| INR | <1.1 | 0.87 | 0.80 | - | 0.94 | 0.84 | - |
| APTT | 22.1–28.1 s | 27.6 | 24.1 | - | 25.1 | 21.3 ↓ | - |
| Lactate | 4.5–19.8 mg/dL | 9.88 | 41.18 ↑ | 35.85 ↑ | 9.87 | 23.33 ↑ | - |
| AST | 0–32 U/L | 20.2 | 60.1 ↑ | 14.1 | 27.6 | 11.9 | 10.1 |
| ALT | 0–33 U/L | 18.1 | 62.7 ↑ | 33.4 ↑ | 27.5 | 21.3 | 21.5 |
| Serum urea | 0–50 mg/dL | 23.5 | 33.1 | 41.5 | 19.1 | 33.4 | 34.8 |
| Creatinine | 0.50–0.90 mg/dL | 0.78 | 0.72 | 0.67 | 0.83 | 0.61 | 0.54 |
| Glucose | 74–106 mg/dL | 90 | 131 | 139 | 96 | 76 | 247 ↑↑ |
| Ferritin | 15–150 μg/L | 385.99 ↑ | 514.8 ↑ | 2524.4 ↑↑↑ | 28.14 | 71.98 | 145.39 |
| CRP | 0–5 mg/L | 2.47 | 1.13 | 0.58 | 1.37 | 6.51 ↑ | 2.67 |
| IL-6 | 0–7 pg/mL | 12.42 ↑ | 7.59 ↑ | - | 11.96 ↑ | <1.50 | 4.47 |
| Laboratory Data | Normal Range | Case V Admission | Case V Follow-Up |
|---|---|---|---|
| RBC | 4,000,000–5,500,000/mmc | 4,600,000 | 4,350,000 |
| Hemoglobin | 11.5–16 g/dL | 12.7 | 12.2 |
| Hematocrit | 35.5–47% | 38 | 36 |
| Platelets | 150,000–400,000/mmc | 279,000 | 198,000 |
| WBC | 4000–10,000/mmc | 8210 | 11,750 ↑ |
| NE | 1500–7500 (30–65%) | 7350 (89.5%) | 9770 (83.2%) ↑ |
| LY | 3000–9500 (30–55%) | 770 (9.4%) ↓ | 920 (7.8%) ↓ |
| Fibrinogen | 1.8–3.5 g/L | 2.70 | 1.70 |
| D-Dimers | <0.5 μg/mL | 0.59 | 0.37 |
| PT | 9.8–12.1 s | 11.1 | 10.7 |
| PT | 70–120% | 115 | 125.1 |
| INR | <1.1 | 0.93 | 0.90 |
| APTT | 22.1–28.1 s | 23 | 20.3 |
| Lactate | 4.5–19.8 mg/dL | 16.95 | 20.21 ↑ |
| AST | 0–32 U/L | 15.1 | 51.6 ↑ |
| ALT | 0–33 U/L | 14.6 | 70.9 ↑ |
| Serum urea | 0–50 mg/dL | 16.3 | 53.2 ↑ |
| Creatinine | 0.50–0.90 mg/dL | 0.61 | 0.68 |
| Glucose | 74–106 mg/dL | 141 ↑ | 115 ↑ |
| Ferritin | 15–150 μg/L | 37.16 | 239.81 ↑ |
| CRP | 0–5 mg/L | 1.24 | 0.31 |
| IL-6 | 0–7 pg/mL | <1.5 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laza, R.; Musta, V.F.; Nicolescu, N.D.; Marinescu, A.R.; Mocanu, A.; Vilceanu, L.; Paczeyka, R.; Cut, T.G.; Lazureanu, V.E. Cutaneous Manifestations in SARS-CoV-2 Infection—A Series of Cases from the Largest Infectious Diseases Hospital in Western Romania. Healthcare 2021, 9, 800. https://doi.org/10.3390/healthcare9070800
Laza R, Musta VF, Nicolescu ND, Marinescu AR, Mocanu A, Vilceanu L, Paczeyka R, Cut TG, Lazureanu VE. Cutaneous Manifestations in SARS-CoV-2 Infection—A Series of Cases from the Largest Infectious Diseases Hospital in Western Romania. Healthcare. 2021; 9(7):800. https://doi.org/10.3390/healthcare9070800
Chicago/Turabian StyleLaza, Ruxandra, Virgil Filaret Musta, Narcisa Daniela Nicolescu, Adelina Raluca Marinescu, Alexandra Mocanu, Laura Vilceanu, Roxana Paczeyka, Talida Georgiana Cut, and Voichita Elena Lazureanu. 2021. "Cutaneous Manifestations in SARS-CoV-2 Infection—A Series of Cases from the Largest Infectious Diseases Hospital in Western Romania" Healthcare 9, no. 7: 800. https://doi.org/10.3390/healthcare9070800