
The Impact of COVID-19 on Essential Medicines and Personal Protective Equipment Availability and Prices in Saudi Arabia

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- 1.
- Your age?
- 25–34 years
- 35–44 years
- 45–54 years
- 55–65 years
- >65 years
- 2.
- Gender:
- Male.
- Female.
- 3.
- What is your profession?
- Pharmacist.
- Physician.
- Nurse.
- Engineer.
- Other:________________
- 4.
- Your current position:________________________
- 5.
- How many years of experience do you have in the pharmaceutical supply chain/pharmaceutical purchasing or planning?
- None.
- 1–2 years.
- 2–4 years.
- 4–6 years.
- 6–8 years.
- >8 years.
- 6.
- Your hospital or healthcare institution is affiliated with which public or private entity:_______________________
- 7.
- The institution that you work in is located in which geographic region in the Kingdom?
- Riyadh.
- Makkah.
- AlMadinah.
- Asir.
- Albahah.
- Eastern province.
- Alqassim.
- Northern borders province.
- Jizan province.
- 8.
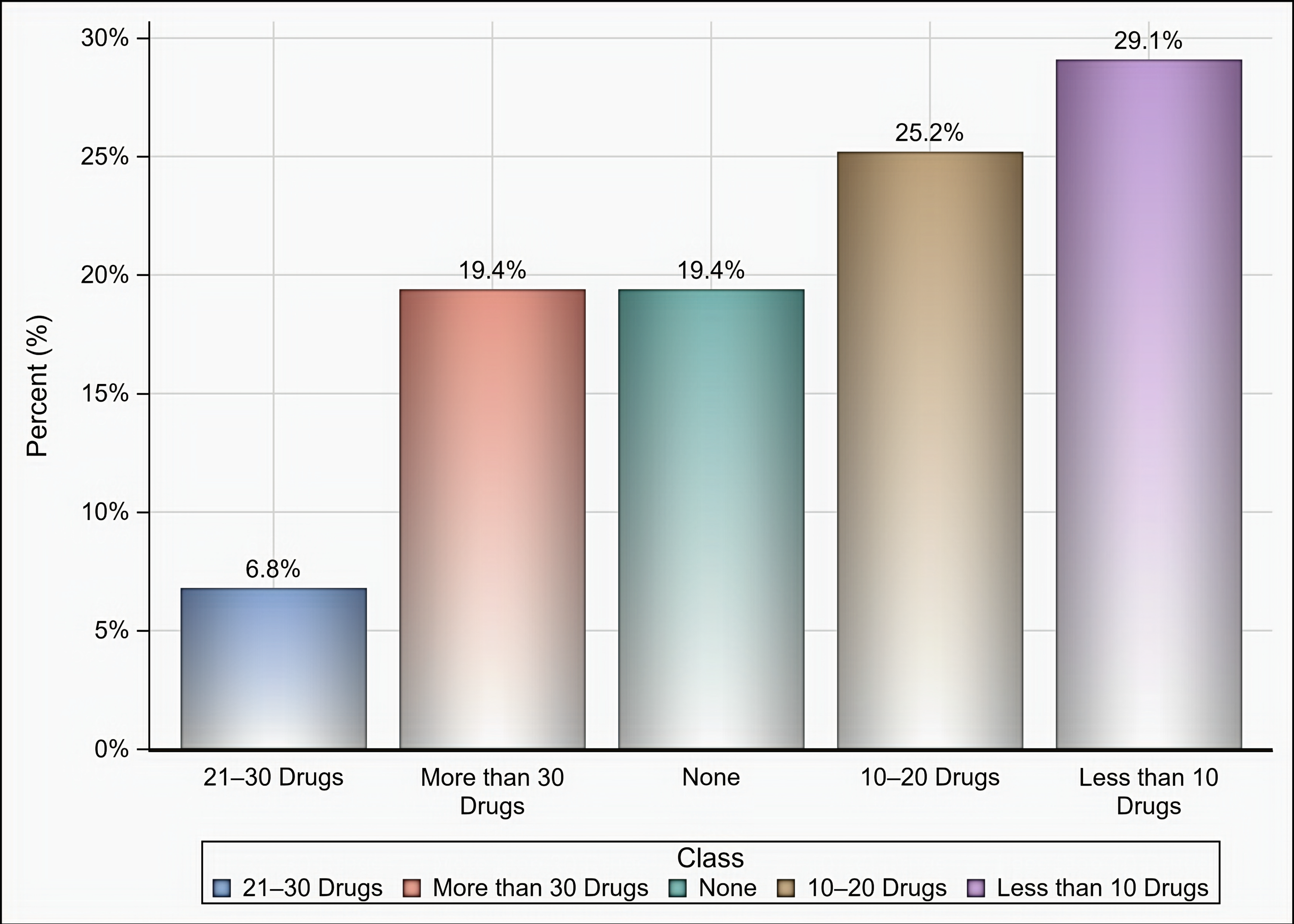
- What was the approximate number of medications that you faced shortages with during the COVID-19 pandemic?
- None.
- ≤10.
- 10–20.
- 21–30.
- ≥30.
- 9.
- Please mention the names of medications that your institution faced shortages with during the COVID-19 pandemic (A list of the World Health Organization (WHO) list of essential medicines is attached).
- 10.
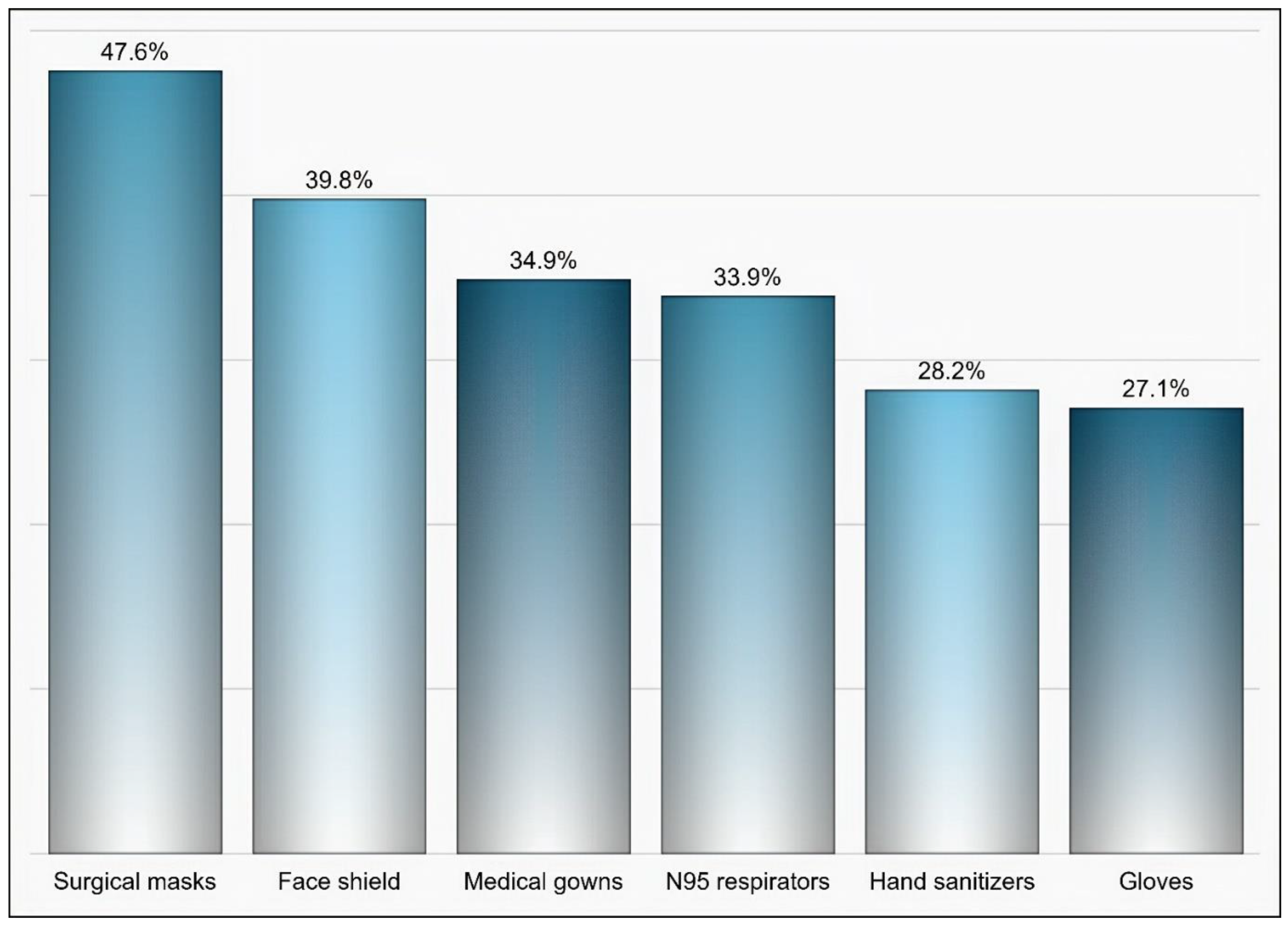
- Please mention the names of the Personal Protective Equipment (PPE) that your institution faced shortages with during COVID-19 pandemic.
- 11.
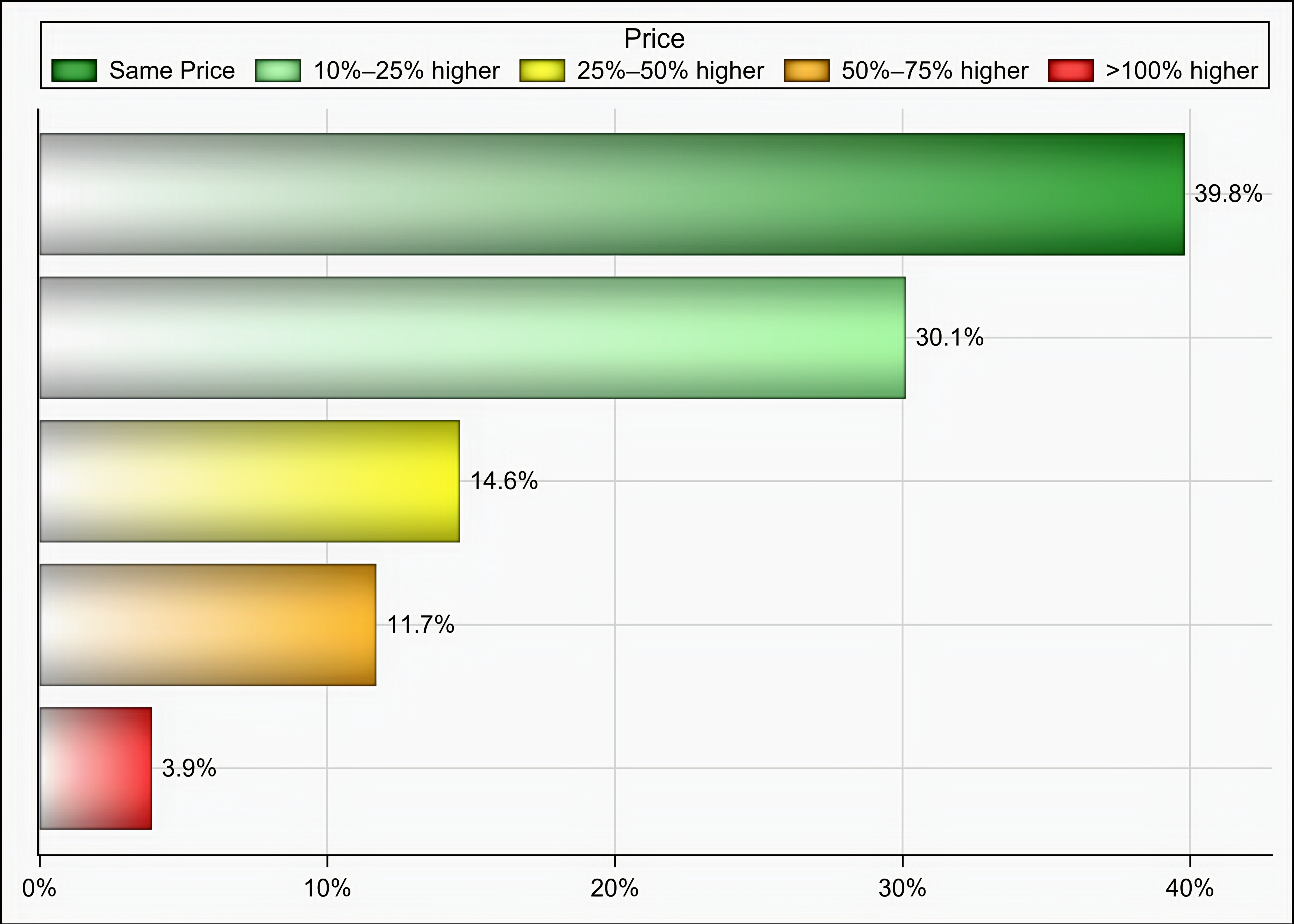
- Kindly, estimate the difference in the acquisition cost of the Essential Medicines as shown in the WHO list of essential drugs pre- and post the COVID-19 pandemic.
- Same price.
- 10–25%.
- 25–50%.
- 50–75%.
- 75–100%.
- >100%.
- Other:____________
- 12.
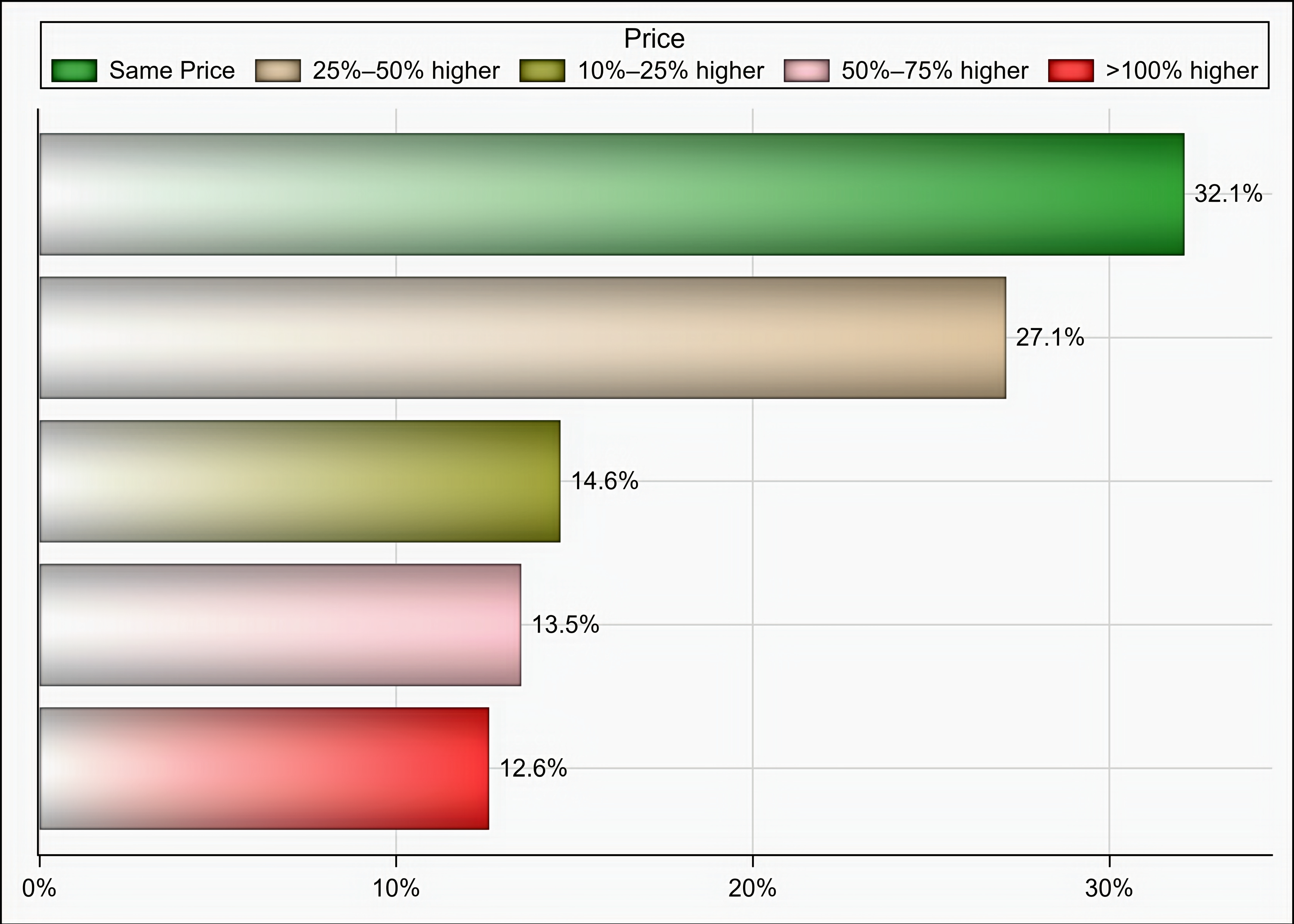
- Kindly, estimate the difference in the cost of PPE pre- and post the COVID-19 pandemic.
- Same price.
- 10–25%.
- 25–50%.
- 50–75%.
- 75–100%.
- >100%.
- Other:____________
- 13.
- Did your institution place any direct purchase order for a drug or PPE during the COVID-19 pandemic due to drug or PPE shortages?
- Yes.
- No.
References
- World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 11 December 2020).
- Ayati, N.; Saiyarsarai, P.; Nikfar, S. Short and long term impacts of COVID-19 on the pharmaceutical sector. DARU J. Pharm. Sci. 2020, 28, 799–805. [Google Scholar] [CrossRef]
- Burry, L.D.; Barletta, J.F.; Williamson, D.; Kanji, S.; Maves, R.C.; Dichter, J.; Christian, M.D.; Geiling, J.; Erstad, B.L. It Takes a Village…: Contending with drug shortages during disasters. Chest 2020, 158, 2414–2424. [Google Scholar] [CrossRef]
- Huang, Y. The Coronavirus Outbreak Could Disrupt the U.S. Drug Supply. Council on Foreign Relations. Available online: https://www.cfr.org/in-brief/coronavirus-disrupt-us-drug-supply-shortages-fda (accessed on 23 November 2020).
- ASHP Drug Shortage. ASHP Drug Shortage List. Available online: https://www.ashp.org/Drug-Shortages/Current-Shortages/Drug-Shortages-List?page=CurrentShortages (accessed on 18 December 2020).
- U.S Food and Drug Administration. Current and Resolved Drug Shortages and Discontinuations Reported to FDA. Available online: https://www.accessdata.fda.gov/scripts/drugshortages/default.cfm (accessed on 10 November 2020).
- Sen-Crowe, B.; McKenney, M.; Elkbuli, A. Medication shortages during the COVID-19 pandemic: Saving more than COVID lives. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- World Health Organization. Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. Available online: https://www.who.int/news/item/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 18 November 2020).
- ASHP COVID-19 Resource Center. COVID-19 Periodic Pharmacy Resources Survey Results. Available online: https://www.ashp.org/COVID-19/Bi-weekly-PPE-Survey-Results-Covid-19?loginreturnUrl=SSOCheckOnly (accessed on 11 November 2020).
- Alruthia, Y.S.; Alwhaibi, M.; Alotaibi, M.F.; Asiri, S.A.; Alghamdi, B.M.; Almuaythir, G.S.; Alsharif, W.R.; Alrasheed, H.H.; Alswayeh, Y.A.; Alotaibi, A.J.; et al. Drug shortages in Saudi Arabia: Root causes and recommendations. Saudi Pharm. J. 2018, 26, 947–951. [Google Scholar] [CrossRef]
- Alruthia, Y.S.; Alkofide, H.; Alajmi, R.; Balkhi, B.; Alghamdi, A.; Alnasser, A.; AlAyed, A.; Alshammari, M.; Alsuhaibani, D.; Alathbah, A. Drug shortages in large hospitals in Riyadh: A cross-sectional study. Ann. Saudi Med. 2017, 37, 375–385. [Google Scholar] [CrossRef] [Green Version]
- AlShehri, S.; AlShammari, A. Drug supply shortages in pharmacies: Causes and solutions; a case study in King Khaled Eye Special Hospital. Int. Bus. Manag. 2016, 10, 2453–2459. [Google Scholar]
- Alazmi, A.A.; Jastaniah, W.; Alhamdan, H.S.; Alyamani, A.O.; AlKhudhyr, W.I.; Abdullah, S.M.; Alzahrani, M.; Alsahafi, A.; Alohali, T.A.; Alkhelawi, T.; et al. Addressing Cancer Treatment Shortages in Saudi Arabia: Results of a National Survey and Expert Panel Recommendations. JCO Glob. Oncol. 2020, 6, 476–485. [Google Scholar] [CrossRef] [PubMed]
- U.S Food and Drug Administration. FDA Drug Shortages. Available online: https://www.accessdata.fda.gov/scripts/drugshortages/ (accessed on 11 November 2020).
- Khan, T.M.; Emeka, P.; Suleiman, A.K.; Alnutafy, F.S.; Aljadhey, H. Pharmaceutical pricing policies and procedures in Saudi Arabia: A Narrative Review. Ther. Innov. Regul. Sci. 2016, 50, 236–240. [Google Scholar] [CrossRef]
- Kanavos, P.; Tzouma, V.; Fontrier, A.M.; Kamphuis, B.; Parkin, G.C.; Saleh, S. Pharmaceutical Pricing and Reimbursement in the Middle East and North Africa Region. London School of Economics. Available online: http://www.lse.ac.uk/business-and-consultancy/consulting/consulting-reports/pharmaceutical-pricing-andreimbursement-in-the-middle-east-and-north-africa-region (accessed on 26 November 2020).
- Alruthia, Y.; Aljohani, B.; Alsharif, W.R.; Alrasheed, H.H.; Alghamdi, B.M.; Asiri, S.; Alarfaj, M.; Almuaythir, G.S.; Almazrou, S.; Almazroo, O.; et al. Prospects of Establishing a Saudi Version of the United States Food and Drug Administration Orange Book. Health Policy Technol. 2020. [Google Scholar] [CrossRef]
- World Health Organization. WHO Expert Committee on Specifications for Pharmaceutical Preparations; World Health Organ: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. WHO Model List of Essential Medicines: 17th List; World Health Organ: Geneva, Switzerland, 2011. [Google Scholar]
- Badreldin, H.A.; Atallah, B. Global drug shortages due to COVID-19: Impact on patient care and mitigation strategies. Res. Soc. Adm. Pharm. 2021, 17, 1946–1949. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, M.; Kotis, D.; Thomson, K.; Harrison, M.; Fennessy, G.; Postelnick, M.; Scheetz, M.H. Effects on Patient Care Caused by Drug Shortages: A Survey. J. Manag. Care Pharm. 2013, 19, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Goldsack, J.C.; Reilly, C.; Bush, C.; McElligott, S.; Bristol, M.N.; Motanya, U.N.; Field, R.; Vozniak, J.M.; Wong, Y.-N.; Schwartz, J.S.; et al. Impact of shortages of injectable oncology drugs on patient care. Am. J. Health Pharm. 2014, 71, 571–578. [Google Scholar] [CrossRef]
- McBride, A.; Holle, L.M.; Westendorf, C.; Sidebottom, M.; Griffith, N.; Muller, R.J.; Hoffman, J.M. National survey on the effect of oncology drug shortages on cancer care. Am. J. Health Pharm. 2013, 70, 609–617. [Google Scholar] [CrossRef]
- Krivak, T.; Smith, A.; Zorn, K.; Sukumvanich, P.; Olawaiye, A.B.; Kelley, J.; Krivak, T.C. Outcomes analysis of an alternative formulation of PEGylated liposomal doxorubicin in recurrent epithelial ovarian carcinoma during the drug shortage era. Onco Targets Ther. 2014, 7, 1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vail, E.; Gershengorn, H.B.; Hua, M.; Walkey, A.J.; Rubenfeld, G.; Wunsch, H. Association Between US Norepinephrine Shortage and Mortality Among Patients with Septic Shock. JAMA 2017, 317, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, M.M.; Skoglund, E.; Pentoney, Z.; Scheetz, M.H. Developing a Method for Reporting Patient Harm Due to Antimicrobial Shortages. Infect. Dis. Ther. 2014, 3, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, E.; Ferri, D. The Role of the Joint Procurement Agreement during the COVID-19 Pandemic: Assessing Its Usefulness and Discussing Its Potential to Support a European Health Union. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Tirupathi, R.; Bharathidasan, K.; Palabindala, V.; Salim, S.A.; A Al-Tawfiq, J. Comprehensive review of mask utility and challenges during the COVID-19 pandemic. Infez. Med. 2020, 28, 57–63. [Google Scholar] [PubMed]
- Kursumovic, E.; Lennane, S.; Cook, T. Deaths in healthcare workers due to COVID-19: The need for robust data and analysis. Anaesthesia 2020, 75, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hegde, S.; LaFiura, C.; Raghavan, M.; Sun, N.; Cheng, S.; Rebholz, C.M.; Seidelmann, S.B. Access to personal protective equipment in exposed healthcare workers and COVID-19 illness, severity, symptoms and duration: A population-based case-control study in six countries. BMJ Glob. Health 2021, 6, e004611. [Google Scholar] [CrossRef] [PubMed]
- WHO Solidarity Trial Consortium. Repurposed antiviral drugs for COVID-19—interim WHO SOLIDARITY trial results. N. Engl. J. Med. 2020, 384, 497–511. [Google Scholar]
- Saudi Arabia Commissions COVID-19 Testing Kits. Available online: https://news.yahoo.com/saudi-arabia-commissions-covid-19-203900867.html (accessed on 18 December 2020).
- World Takes Stock of Covid-19 Drug after US Snaps Up Supplies. Available online: https://www.irishtimes.com/news/world/us/world-takes-stock-of-covid-19-drug-after-us-snaps-up-supplies-1.4293396 (accessed on 18 December 2020).
- Trump Administration Secures New Supplies of Remdesivir for the United States|HHS.gov. Available online: https://www.hhs.gov/about/news/2020/06/29/trump-administration-secures-new-supplies-remdesivir-united-states.html (accessed on 18 December 2020).
- Procurement Strategies for Navigating the COVID-19 Crisis from around the World—Open Contracting Partnership. Available online: https://www.open-contracting.org/2020/04/08/5-procurement-strategies-for-navigating-the-covid-19-crisis-from-around-the-world/ (accessed on 18 December 2020).
- Rider, A.E.; Templet, D.J.; Daley, M.J.; Shuman, C.; Smith, L.V. Clinical dilemmas and a review of strategies to manage drug shortages. J. Pharm. Pract. 2013, 26, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Bogaert, P.; Bochenek, T.; Prokop, A.; Pilc, A. A Qualitative Approach to a Better Understanding of the Problems Underlying Drug Shortages, as Viewed from Belgian, French and the European Union’s Perspectives. PLoS ONE 2015, 10, e0125691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, A.; Alkharfy, K.M.; Alrabiah, Z.; Alhossan, A. Saudi Arabia, pharmacists and COVID-19 pandemic. J. Pharm. Policy Pract. 2020, 13, 1–3. [Google Scholar] [CrossRef]
- Cohen, J.; Rodgers, Y.V.D.M. Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Prev. Med. 2020, 141, 106263. [Google Scholar] [CrossRef]
- Wouters, O.J.; Sandberg, D.M.; Pillay, A.; Kanavos, P.G. The impact of pharmaceutical tendering on prices and market concentration in South Africa over a 14-year period. Soc. Sci. Med. 2019, 220, 362–370. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Age (yrs.) | |
| 25–34 yrs. | 43 (41.7) |
| 35–44 yrs. | 40 (38.8) |
| 45–54 yrs. | 16 (15.5) |
| 55–65 yrs. | 4 (3.9) |
| Gender | |
| Male | 67 (65) |
| Female | 36 (35) |
| Profession | |
| Pharmacist | 95 (92.2) |
| Physician | 1 (0.97) |
| Engineer | 1 (0.97) |
| Supply chain specialist | 6 (5.83) |
| Place of work | |
| Ministry of defense- and aviation-affiliated healthcare institutions | 25 (24.27) |
| Ministry of health-affiliated healthcare institutions | 43 (41.75) |
| Ministry of interior-affiliated healthcare institutions | 17 (16.50) |
| Ministry of national guard-affiliated healthcare institutions | 5 (4.85) |
| University-affiliated hospitals | 8 (7.77) |
| Private hospitals | 5 (4.85) |
| Geographic region | |
| Riyadh | 61 (59.22) |
| Makkah | 13 (12.62) |
| AlMadinah | 2 (1.94) |
| Asir | 2 (1.94) |
| Albahah | 2 (1.94) |
| Eastern province | 19 (18.45) |
| Alqassim | 1 (0.97) |
| Northern borders province | 2 (1.94) |
| Jizan province | 1 (0.97) |
| Years of experience in supply chain | |
| <1 year | 13 (12.62) |
| 1–2 years | 10 (9.71) |
| 2–4 yyears | 6 (5.83) |
| 4–6 years | 11 (10.68) |
| 6–8 years | 17 (16.50) |
| >8 years | 46 (44.66) |
| Name | N (%) |
|---|---|
| Tocilizumab | 53 (51.45) |
| Hydroxychloroquine | 44 (43.68) |
| Lopinavir/Ritonavir | 35 (33.98) |
| Ribavirin | 27 (26.21) |
| Enoxaparin | 18 (17.47) |
| Interferon beta-1b | 17 (16.50) |
| Dexamethasone | 17 (16.50) |
| Cisatracurium besilate | 14 (13.59) |
| Furosemide | 11 (10.67) |
| Prednisolone | 11 (10.67) |
| Methimazole | 9 (8.73) |
| Hydrocortisone | 9 (8.73) |
| Methylprednisolone | 8 (7.76) |
| Levetiracetam | 7 (6.79) |
| Piperacillin/Tazobactam | 7 (6.79) |
| Vancomycin | 4 (3.88) |
| Warfarin | 3 (2.91) |
| Metformin | 3 (2.91) |
| Ropivacaine | 3 (2.91) |
| Pertuzumab | 2 (1.94) |
| Trastuzumab | 2 (1.94) |
| Bevacizumab | 2 (1.94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljadeed, R.; AlRuthia, Y.; Balkhi, B.; Sales, I.; Alwhaibi, M.; Almohammed, O.; Alotaibi, A.J.; Alrumaih, A.M.; Asiri, Y. The Impact of COVID-19 on Essential Medicines and Personal Protective Equipment Availability and Prices in Saudi Arabia. Healthcare 2021, 9, 290. https://doi.org/10.3390/healthcare9030290
Aljadeed R, AlRuthia Y, Balkhi B, Sales I, Alwhaibi M, Almohammed O, Alotaibi AJ, Alrumaih AM, Asiri Y. The Impact of COVID-19 on Essential Medicines and Personal Protective Equipment Availability and Prices in Saudi Arabia. Healthcare. 2021; 9(3):290. https://doi.org/10.3390/healthcare9030290
Chicago/Turabian StyleAljadeed, Rana, Yazed AlRuthia, Bander Balkhi, Ibrahim Sales, Monira Alwhaibi, Omar Almohammed, Abdulaziz J. Alotaibi, Ali M. Alrumaih, and Yousif Asiri. 2021. "The Impact of COVID-19 on Essential Medicines and Personal Protective Equipment Availability and Prices in Saudi Arabia" Healthcare 9, no. 3: 290. https://doi.org/10.3390/healthcare9030290