
MiniQEEG and Neurofeedback in Diagnosis and Treatment of COVID-19-Related Panic Attacks: A Case Report

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Standard Recordings as Reference
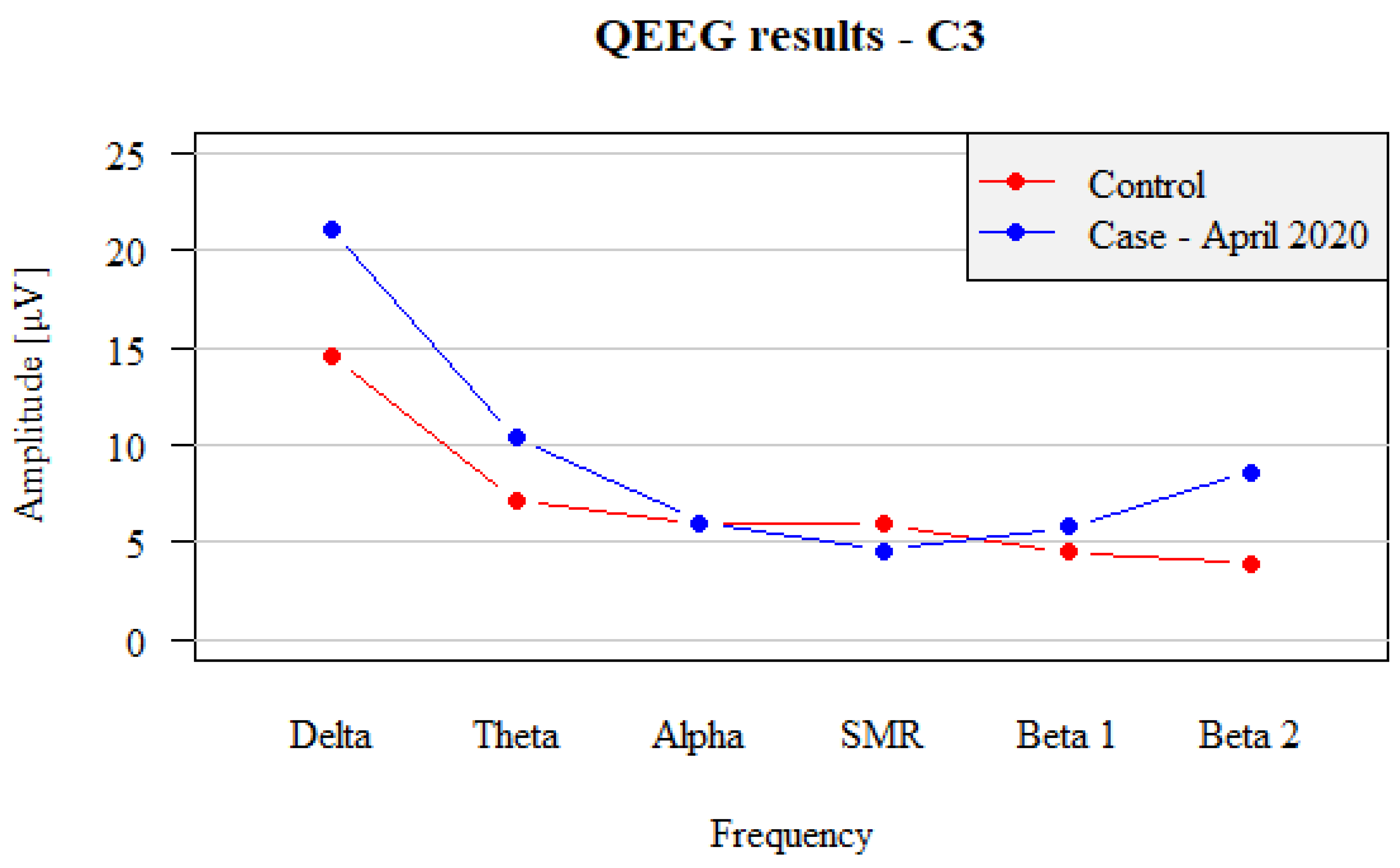
3.2. Analysis of the First Mini QEEG Recording (April 2020)
3.3. The Methods and Purpose of QEEG-Based Neurofeedback Training
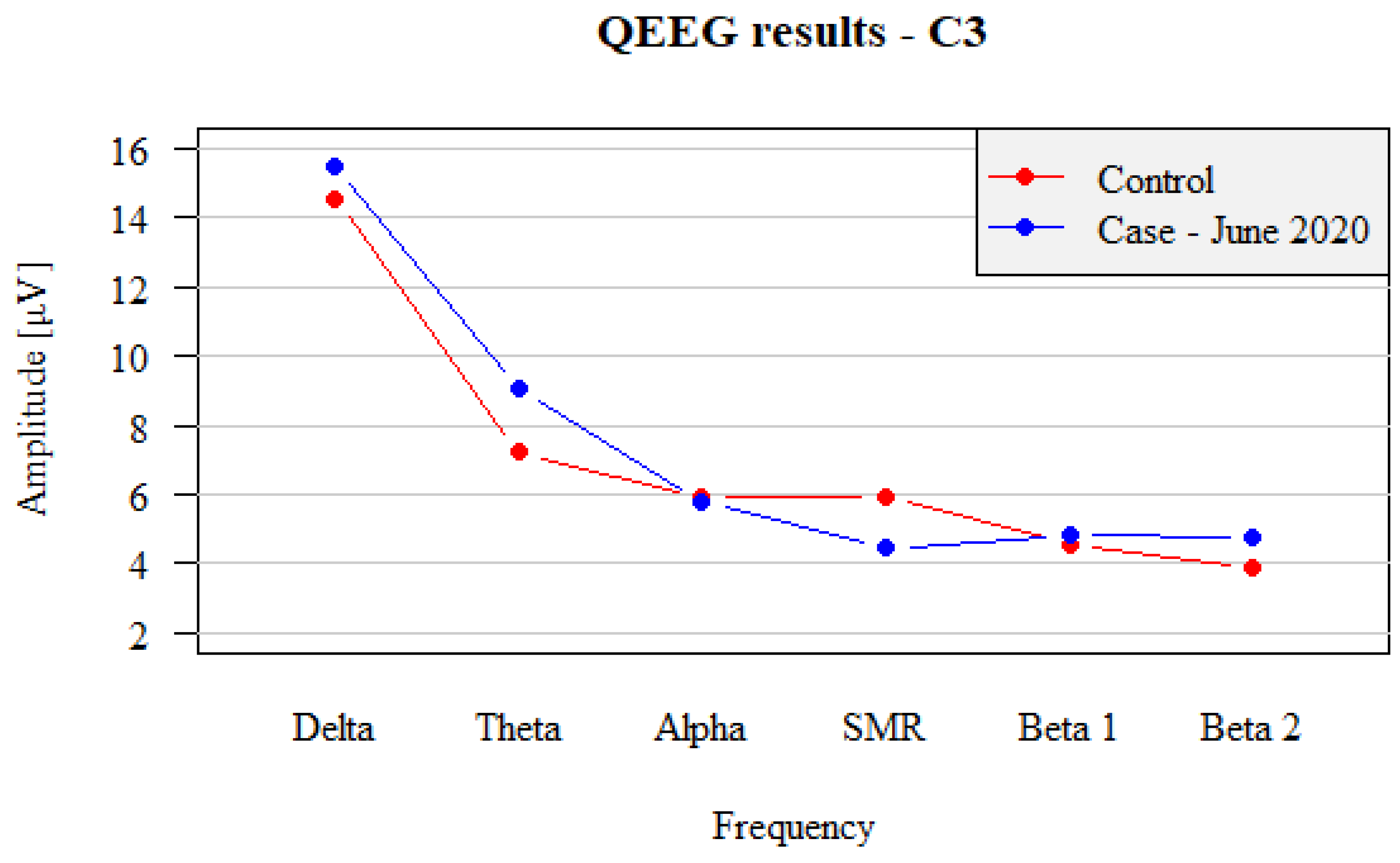
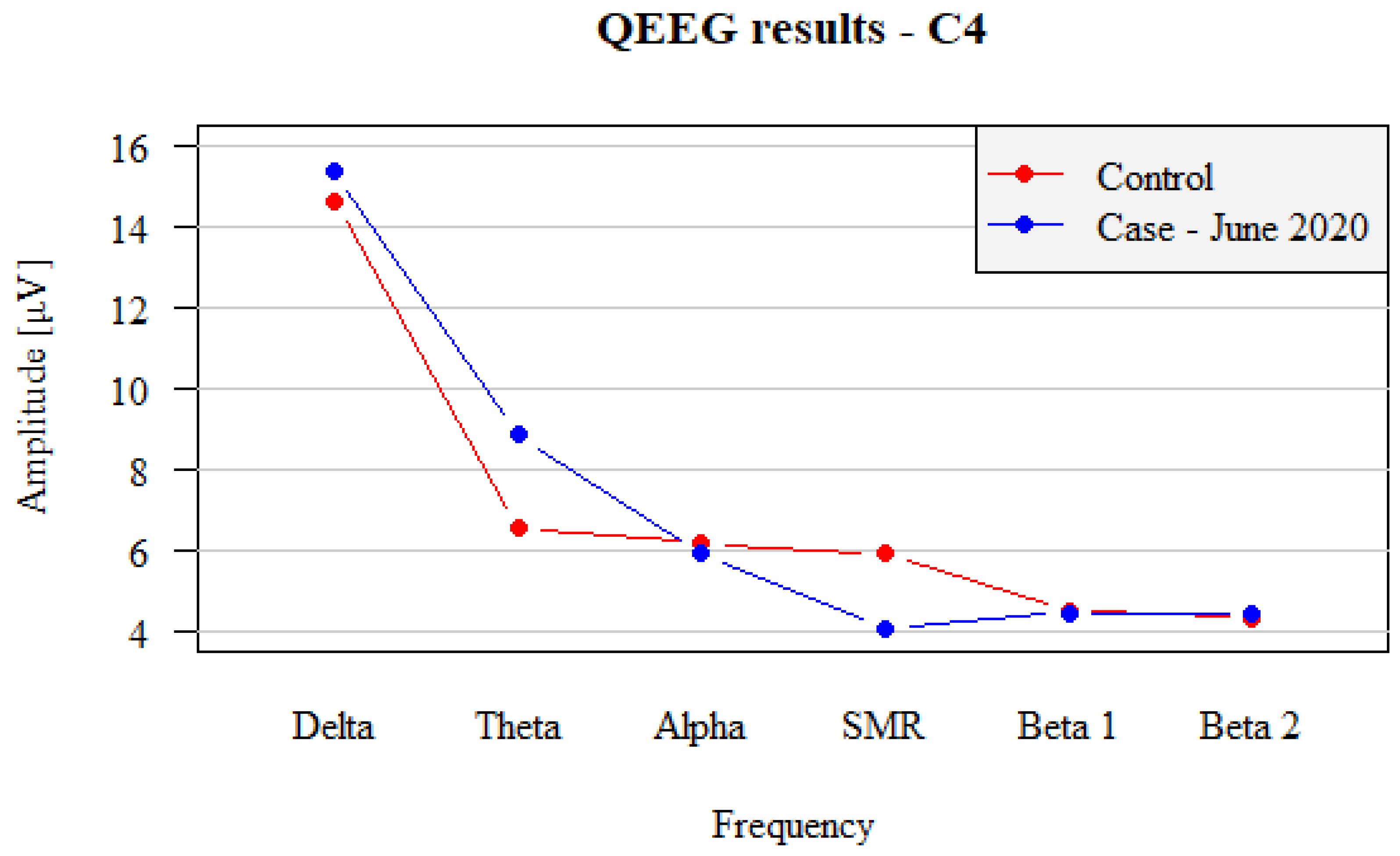
3.4. Results after Neurofeedback Trainings
3.5. Further Results—MiniQEEG Diagnosis and Subjective Effect of Treatment in April 2021 and in April 2022
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Craske, M.G.; Kircanski, K.; Epstein, A.; Wittchen, H.-U.; Pine, D.S.; Lewis-Fernández, R.; Hinton, D.; Anxiety, D.V.; Spectrum, O. Posttraumatic and Dissociative Disorder Work Group Panic disorder: A review of DSM-IV panic disorder and proposals for DSM-V. Depress. Anxiety 2010, 27, 93–112. [Google Scholar] [CrossRef] [PubMed]
- Meuret, A.E.; Kroll, J.; Ritz, T. Panic Disorder Comorbidity with Medical Conditions and Treatment Implications. Annu. Rev. Clin. Psychol. 2017, 13, 209–240. [Google Scholar] [CrossRef] [PubMed]
- Bighelli, I.; Castellazzi, M.; Cipriani, A.; Girlanda, F.; Guaiana, G.; Koesters, M.; Turrini, G.; Furukawa, T.A.; Barbui, C. Antidepressants versus placebo for panic disorder in adults. Cochrane Database Syst. Rev. 2018, 4, CD010676. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.G. Generalized anxiety disorder. In Effective Brief Therapies: A Clinician’s Guide; Hersen, M., Biaggio, M., Eds.; Academic Press: San Diego, CA, USA, 2000; pp. 158–178. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Impact of the DSM-IV to DSM-5 Changes on the National Survey on Drug Use and Health [Internet]; Substance Abuse and Mental Health Services Administration (US): Rockville, MD, USA, 2016. [Google Scholar]
- Roest, A.M.; de Vries, Y.A.; Lim, C.C.W.; Wittchen, H.U.; Stein, D.J.; Adamowski, T.; Hamzawi, A.A.; Bromet, E.J.; Viana, M.C.; de Girolamo, G.; et al. A comparison of DSM-5 and DSM-IV agoraphobia in the World Mental Health Surveys. Depress. Anxiety 2019, 36, 499–510. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Chiu, W.T.; Jin, R.; Ruscio, A.M.; Shear, K.; Walters, E.E. The Epidemiology of Panic Attacks, Panic Disorder, and Agoraphobia in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2006, 63, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.Y.; Hedrick, R.M.; Ishak, W.W. Panic Attacks in hyperaldosteronism. Innov. Clin. Neurosci. 2019, 16, 19–21. [Google Scholar]
- Bystritsky, A.; Kerwin, L.; Niv, N.; Natoli, J.L.; Abrahami, N.; Klap, R.; Wells, K.; Young, A.S. Clinical and subthreshold panic disorder. Depress. Anxiety 2009, 27, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Freire, R.C.; Ferreira-Garcia, R.; Cabo, M.C.; Martins, R.M.; Nardi, A.E. Panic attack provocation in panic disorder patients with a computer simulation. J. Affect. Disord. 2019, 264, 498–505. [Google Scholar] [CrossRef]
- Locke, A.B.; Kirst, N.; Shultz, C.G. Diagnosis and management of generalized anxiety disorder and panic disorder in adults. Am. Fam. Physician 2015, 91, 617–624. [Google Scholar]
- Kesebir, S.; Yosmaoglu, A. QEEG in affective disorder: About to be a biomarker, endophenotype and predictor of treatment response. Heliyon 2018, 4, e00741. [Google Scholar] [CrossRef] [Green Version]
- Bonnstetter, R.; Collura, T.; Cantor, D. Application of qEEG in forensic psychiatry. Int. J. Psychophysiol. 2018, 131, S3–S4. [Google Scholar] [CrossRef]
- Thatcher, R.W.; Lubar, J.F. History of the scientific standards of QEEG normative databases. In Introduction to QEEG and Neurofeedback: Advanced Theory and Applications; Budzinsky, T., Budzinski, H., Evans, J., Abarbanel, A., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 29–59. [Google Scholar]
- Nuwer, M.R. Quantitative EEG: I. Techniques and problems of frequency analysis and topographic mapping. J. Clin. Neurophysiol. 1988, 5, 1–43. [Google Scholar] [CrossRef] [PubMed]
- Borkowski, P. Biofeedback Innowacje; Akademia, im. Jana Długosza: Częstochowa, Poland, 2015. [Google Scholar]
- Wiśniewska, M.; Gmitrowicz, A.; Pawełczyk, N. Zastosowanie QEEG w psychiatrii z uwzględnieniem populacji rozwojowej. Psychiatr. Psychol. Klin. 2016, 16, 188–193. (In Polish) [Google Scholar] [CrossRef]
- Ribas, V.R.; Ribas, R.G.; Nóbrega, J.D.A.; Da Nóbrega, M.V.; Espécie, J.A.D.A.; Calafange, M.T.; Calafange, C.D.O.M.; Martins, H.A.D.L. Pattern of anxiety, insecurity, fear, panic and/or phobia observed by quantitative electroencephalography (QEEG). Dement. Neuropsychol. 2018, 12, 264–271. [Google Scholar] [CrossRef] [Green Version]
- Finnigan, S.; van Putten, M.J. EEG in ischaemic stroke: Quantitative EEG can uniquely inform (sub-)acute prognoses and clinical management. Clin. Neurophysiol. 2013, 124, 10–19. [Google Scholar] [CrossRef]
- Sainio, K.; Stenberg, D.; Keskimäki, I.; Muuronen, A.; Kaste, M. Visual and spectral EEG analysis in the evaluation of the outcome in patients with ischemic brain infarction. Electroencephalogr. Clin. Neurophysiol. 1983, 56, 117–124. [Google Scholar] [CrossRef]
- Radziszewska, M.; Kaźmierski, J.; Sobów, T. Predyktory odpowiedzi na leczenie przeciwdepresyjne w zapisie EEG i QEEG. Psychiatr. Psychol. Klin. 2015, 15, 19–25. (In Polish) [Google Scholar] [CrossRef]
- Janssen, T.; Geladé, K.; Bink, M.; van Mourik, R.; Twisk, J.; Maras, A.; Oosterlaan, J. Long-term effects of theta/beta neurofeedback on EEG power spectra in children with attention deficit hyperactivity disorder. Clin. Neurophysiol. 2020, 131, 1332–1341. [Google Scholar] [CrossRef]
- Flisiak-Antonijczuk, H.; Adamowska, S.; Chładzińska-Kiejna, S.; Kalinowski, R.; Adamowski, T. Metoda EEG-biofeedback w terapii pacjentów z rozpoznaniem ADHD–przegląd badań. Pediatr. Med. Rodz. 2014, 10, 91–96. (In Polish) [Google Scholar] [CrossRef]
- Kopańska, M.; Ochojska, D.; Muchacka, R.; Dejnowicz-Velitchkov, A.; Banaś-Ząbczyk, A.; Szczygielski, J. Comparison of QEEG Findings before and after Onset of Post-COVID-19 Brain Fog Symptoms. Sensors 2022, 22, 6606. [Google Scholar] [CrossRef]
- Hammond, D.C. What is Neurofeedback? J. Neurother. 2006, 10, 24–36. [Google Scholar] [CrossRef] [Green Version]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Stijelja, S.; Mishara, B.L. COVID-19 and Psychological Distress—Changes in Internet Searches for Mental Health Issues in New York During the Pandemic. JAMA Intern. Med. 2020, 180, 1703–1706. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Thakura, V.; Jain, A. COVID 2019-suicides: A global psychological pandemic. Brain Behav. Immun. 2020, 88, 952–953. [Google Scholar] [CrossRef]
- De Carvalho, M.R.; Velasques, B.B.; Freire, R.C.; Cagy, M.; Marques, J.B.; Teixeira, S.; Thomaz, R.; Range, B.P.; Piedade, R.; Akiskal, H.S.; et al. Frontal cortex absolute beta power measurement in Panic Disorder with Agoraphobia patients. J. Affect. 2015, 184, 176–181. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Outbreak Situation. Retrieved 27 March 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 18 October 2020).
- De Carvalho, M.R.; Velasques, R.F.; Cagy, M.; Marques, J.B.; Teixeira, S.; Range, B.P.; Piedade, R.; Riberio, P.; Nardi, A.E. Alpha absolute power measurement in panic disorder with agoraphobia patients. J. Affect. Disord. 2013, 151, 259–264. [Google Scholar] [CrossRef]
- Wise, V.; McFarlane, A.C.; Clark, C.R.; Battersby, M. An integrative assessment of brain and body function ‘atrest’ in panicdisorder: A combinedquantitative EEG/autonomicfunctionstudy. Int. J. Psychophysiol. 2011, 79, 155–165. [Google Scholar] [CrossRef]
- Hanaoka, A.; Kikuchi, M.; Komuro, R.; Oka, H.; Kidani, T.; Ichikawa, S. EEG coherenceanalysis in nevermedicatedpatients with panicdisorder. Clin. EEG Neurosci. 2005, 36, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Knott, V.J.; Bakish, D.; Lusk, S.; Barkely, J.; Perugini, M. Quantitative EEG correlates of panic disorder. Psychiatry Res. 1996, 68, 31–39. [Google Scholar] [CrossRef]
- Dantendorfer, K.; Prayer, D.; Kramer, J.; Amering, M.; Baischer, W.; Berger, P.; Schoder, M.; Steinberger, K.; Windhaber, J.; Imhof, H.; et al. High frequency of EEG and MRI brain abnormalities in panic disorder. Psychiatry Res. 1996, 68, 41–53. [Google Scholar] [CrossRef]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed]
- Uvais, N.A. COVID-19-Associated Panic Disorder. Prim. Care Companion CNS Disord. 2021, 23, 20l02826. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Cohen, C. Post-COVID-19 Panic Disorder in Older Adults: Two Case Reports. Am. J. Geriatr. Psychiatry 2021, 29, S58–S59. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Channel | Delta 0.5–3.0 Hz | Theta 4.0–8.0 Hz | Alpha 8.0–12.0 Hz | SMR 12.0–15.0 Hz | Beta 1 15.0–20.0 Hz | Beta 2 20.0–34.0 Hz | |
|---|---|---|---|---|---|---|---|
| C3 | Amplitude (µV) | ±20 (~20% < C4) | ±15 (~20% < C4) | ±10 (~20% < C4) | 4–10 (~20% < C4) | 4–10 (~20% > C4) | 4–10 (~20% > C4) |
| C4 | Amplitude (µV) | ±20 (~20% > C3) | ±20 (~20% > C3) | ±20 (~20% > C3) | 4–10 (~20% > C3) | 4–10 (~20% < C3) | 4–10 (~20% < C3) |
| Channel | Delta 0.5–3.0 Hz | Theta 4.0–8.0 Hz | Alpha 8.0–12.0 Hz | SMR 12.0–15.0 Hz | Beta 1 15.0–20.0 Hz | Beta 2 20.0–34.0 Hz | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | |
| C3 | Amplitude (µV) | 21.06 | 14.46 | 10.44 | 7.29 | 6.04 | 5.26 | 4.59 | 4.16 | 5.81 | 4.68 | 8.62 | 4.34 |
| C4 | Amplitude (µV) | 21.44 | 14.53 | 10.02 | 7.98 | 5.19 | 6.34 | 3.82 | 4.25 | 5.09 | 4.17 | 8.79 | 4.83 |
| Channel | Delta 0.5–3.0 Hz | Theta 4.0–8.0 Hz | Alpha 8.0–12.0 Hz | SMR 12.0–15.0 Hz | Beta 1 15.0–20.0 Hz | Beta 2 20.0–34.0 Hz | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | 2020 | 2022 | |
| C3 | Amplitude (µV) | 21.06 | 15.5 | 10.44 | 9.05 | 6.04 | 5.8 | 4.59 | 4.45 | 5.81 | 4.86 | 8.62 | 4.78 |
| C4 | Amplitude (µV) | 21.44 | 15.31 | 10.02 | 8.85 | 5.19 | 5.9 | 3.82 | 4.05 | 5.09 | 4.46 | 8.79 | 4.41 |
| State-Trait Anxiety Inventory (STAI) the X-1 Scale | |
|---|---|
| First interview | 71 scores/10 sten |
| After 8 weeks/16 EEG Biofeedback trainings | 44 scores/6 sten |
| After 1 year (2021) | 41scores/6 sten |
| After 2 years (2022) | 42 scores/6 sten |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopańska, M.; Dejnowicz-Velitchkov, A.; Bartman, P.; Szczygielski, J. MiniQEEG and Neurofeedback in Diagnosis and Treatment of COVID-19-Related Panic Attacks: A Case Report. Brain Sci. 2022, 12, 1541. https://doi.org/10.3390/brainsci12111541
Kopańska M, Dejnowicz-Velitchkov A, Bartman P, Szczygielski J. MiniQEEG and Neurofeedback in Diagnosis and Treatment of COVID-19-Related Panic Attacks: A Case Report. Brain Sciences. 2022; 12(11):1541. https://doi.org/10.3390/brainsci12111541
Chicago/Turabian StyleKopańska, Marta, Agnieszka Dejnowicz-Velitchkov, Paulina Bartman, and Jacek Szczygielski. 2022. "MiniQEEG and Neurofeedback in Diagnosis and Treatment of COVID-19-Related Panic Attacks: A Case Report" Brain Sciences 12, no. 11: 1541. https://doi.org/10.3390/brainsci12111541