Mass testing and containment of Covid-19
*Corresponding Author(s):
Momiao XiongDepartment Of Biostatistics And Data Science, School Of Public Health, The University Of Texas Health Science Center At Houston, Houston, TX 77030, United States
Tel:713-500-9894,
Fax:713-500-0900
Email:Momiao.Xiong@uth.tmc.edu
Abstract
Urgent public health interventions to mitigate the spread of Covid-19 curtailed most social activities and work. Meanwhile, maintaining social distancing and lockdown will cause substantial economic loss and social damage. Now the critical question is how to reopen the economy while containing the COVID-19 pandemic without social distancing restrictions?
The solution is mass testing. Alternative public health intervention strategies such as shelter-in-place and social distancing policies that may halt economic activities may be curtailed if virus testing which is an effective way to contain Covid-19 is expanded. Although the U.S. still has a longer path ahead, we have estimated that if the number of daily tests is 581,000 per day, i.e., the current number of daily tests would need to be doubled in order for Covid-19 to be contained and social distancing measures to be lifted.
Keywords
Coronavirus Test; COVID-19; Interventions; Reopen Economy; Social Distancing
INTRODUCTION
As of May 17, 2020, the confirmed number cases of Covid-19 in the US have exceeded over 1.4 million cases of coronavirus (COVID-19), which promoted urgent public health interventions to mitigate the spread of Covid-19 by curtailing most social activities and work. Meanwhile, maintaining social distancing and lockdown will cause substantial economic losses and social damage. Now the critical question is how to reopen the economy, while containing the COVID-19 pandemic without social distancing restrictions? The solution is mass testing.
While vaccine and proven effective treatments are currently not available, nonpharmaceutical interventions such as social distancing, school and manufacturing plant closures, cancellations of group events and gatherings, and travel (air, sea and highway) restrictions had not only substantially slowed down the spread of Covid-19, but also effectively “shut down” society and damaged economic activity. An alternative strategy for curbing the spread of Covid-19 is coronavirus testing [1]. Massive testing and symptom screening are implemented to allow early detection of new cases. Early detected individuals must be immediately isolated, and their contacts must also be quickly identified and quarantined.
METHODS
Massive testing provides an alternative intervention for effectively stopping transmission. We can use massive testing to reduce the need for nonpharmaceutical interventions. The question is what rate of the testing should be increased to contain the Covid-19 while relaxing social distancing and reopening economic activities. To quantitatively answer this question, we evaluated the effects of the test rate and social distancing measures, including the percent change in public interventions such as visiting retail stores and recreational facilities, grocery stores and pharmacies, parks, transit stations, workplaces, and residential areas. A tool for evaluation of the effects of the test ratio and social distancing indexes on stopping the spread of Cencovid-19 is stacked autoencoders.
Stacked autoencoders
Single layer autoencoder (AE) is a three-layer feedforward neural network [2]. The first layer is the input layer, the third layer is the reconstruction layer, and the second layer is the hidden layer. The input vector is denoted by Xt , [Υt, Υt-1,...Υt-k-1,At]T , here Υt is the number of cases at the time t and 0 ≤ At≤1 is the public health intervention measure variable. Similar to the reproduction number in the epidemiological models, all interventions can be comprehensively viewed as a control variable taking values in the interval (0, 1). A value of 1 for intervention indicates that intervention is the strongest with a reproduction number R close to zero. A value of zero for intervention variables indicates that no restrictions on social-economic activities are imposed. The intervention measure comprehensively represents the parameters of interventions in the epidemiological models that describe the transmission dynamics of Covid-19. Increasing intervention measures will reduce the number of new cases.
AE attempts to generate an output that reconstructs its input by mapping the hidden vector to the reconstruction layer. The single layer AE attempts to minimize the error between the input vector and the reconstruction vector. We develop stacked autoencoders with 4 layers that consist of two single-layer AEs stacked layer by layer [2]. The dimensions of the input layer, the first hidden layer and the second hidden layer are 8, 32 and 4, respectively. After the first single-layer AE is trained, we remove the reconstruction layer of the first single layer AE and keep the hidden layer of the first single AE as the input layer of the second single-layer AE. Repeat the training process for the second single-layer AE. The output of the final node that fully connects to the hidden layer of the second single-layer AE is the predicted number of cases Υt+1 and intervention measure At+1. The algorithm for generating the intervention measure is summarized as follows.
Algorithm

Two Stage Regressions
DATA SOURCES
The analysis was conducted for virus testing and Google Community Mobility data from March 17, 2020 to May 4, 2020 which were downloaded from https://covidtracking.com/ and https://www.google.com/covid19/mobility/. The data on the number of confirmed, new and death cases of Covid-19 from January 22, 2020 to May 4, 2020, were obtained from the Johns Hopkins Coronavirus Resource Center (https://coronavirus.jhu.edu/MAP.HTM)
RESULTS
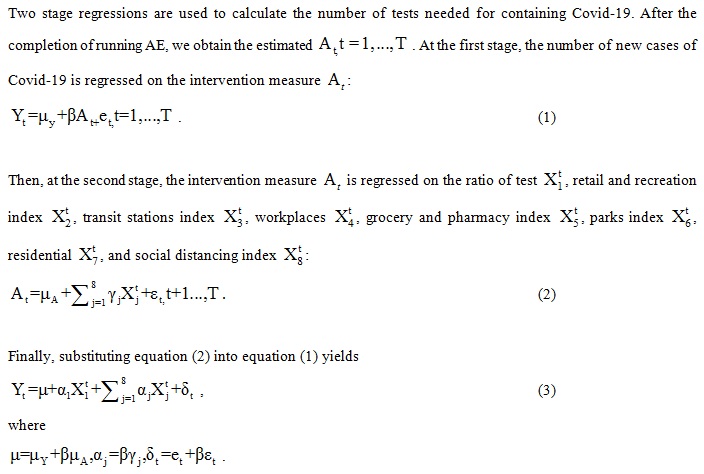
Standardized simple and multiple regressions were used to evaluate the effects of the rate of virus testing, Google Community Mobility Indices and social distancing index on curbing the spread of Covid-19. The number of new cases were converted into the ratio of new cases by dividing by the US population size and subsequently multiplying by 1000. The rate of the virus testing was defined as the ratio of the total number of tests over the US population size and multiplying by 1000. The mobility indexes were recorded as the percentage changes from the baseline before the outbreak of Covid-19. When the rate of the virus testing increased and the mobility indexes decreased, the intervention measure increased, which in turn, reduced the number (ratio) of new cases. The regression of the number of new cases on the intervention measure is
Yt = 0.256-0.264At
Then, we regress the intervention measure on the rate of virus test, Google Mobility Indices and social distancing index using equation (2). By combining two stage regressions, we finally obtained the resulting regressions that regressed the number (ratio) of new cases on the testing rate, Google Mobility Indices and social distancing index. The coefficients of the resulting simple and multiple regressions were summarized in Table 1. Table 1 showed that the virus testing played a similar role in the mitigation of Covid-19 as the social distancing measures had played. We also observed that the effect of the rate of the test was larger than that of the Google Community Mobility Indices. Next, we calculated how many virus tests would be needed to contain Covid-19 if social distancing interventions were lifted, i.e., assuming that the percentage changes from the baseline of all Indices were zero. Using multiple regression in Table 1, we calculated that an increase of 140,048 tests was needed to reduce 10,000 new cases. The 95% interval for the required number of tests to reduce 10,000 new cases was (107,983, 195,756). The number of new cases on May 8, 2020 was 26,956. The complete containment of Covid-19 in the US required an additional 377,513 daily tests. Its 95% interval was (291,079, 527,680).
|
Regress and Simple Regression |
Regressor |
Intercept |
Coefficient |
|
|
|
|
|
|
Number of New Cases |
Retail and Recreation |
0.15 |
0.0528 |
|
|
Grocery and Pharmacy |
0.141 |
0.079 |
|
|
Parks |
0.14 |
0.0528 |
|
|
Transit Stations |
0.25 |
0.238 |
|
|
Workplaces |
0.173 |
0.106 |
|
|
Residential |
0.158 |
0.158 |
|
|
Rate of Test |
0.163 |
-0.098 |
|
Multiple Regression |
|
|
|
|
|
0.118 |
||
|
|
Rate of Test |
-0.085 |
|
|
|
Retail and Recreation |
-0.002 |
|
|
|
Transit Stations |
0.001 |
|
|
|
Workplaces |
0.000162 |
|
|
|
Grocery and Pharmacy |
0.000776 |
|
|
|
Parks |
0.000103 |
|
|
|
Residential |
|
0.00146 |
Table 1: Coefficients of the number of new cases regressing on the rate of virus test and Google mobility indexes.
DISCUSSION
Alternative public health intervention strategies such as shelter-in-place and social distancing policies that may halt economic activities may be curtailed if virus testing which is an effective way to contain Covid-19 is expanded. Now the question is how many tests per day are needed to control the spread of Covid-19. The testing level in the U.S. this week was 264,000 persons per day. Some investigators suggested that the number of daily tests must be doubled or tripled, or even should be expanded to more than a 75-fold increase to control the spread of Covid-19 [3,4]. Although the U.S. still has a long path ahead, we estimated that if the number of daily tests is 581,000 (533,492, 967,136) per day, i.e., the current number of daily tests would have to be doubled or increased to four times (upper bound) in order for Covid-19 to be contained and social distancing measures to be lifted.
The true number of Covid-19 cases may never be known. To incorporate the uncertainty into the model, in addition to the mean number of virus tests, we estimated the confidence interval of the required number of tests.
When the number of tests is increased, a natural question is what mass testing strategy is. Clinical doctors and public health agencies have different testing goals. Doctors test patients to make an individual diagnosis; public health agencies need to estimate the population prevalence and how Covid-19 is spread in communities. Several test strategies can be considered. The community-based symptom screening and testing, which are supported by contact tracing, quarantine, and isolation, can be made widely available to allow early identification of new cases. This would ideally be supported by point of care tests that are accurate and reliable. Some vulnerable communities, such as nursing homes must be tested. In addition to making an individual diagnosis test, we also need to test a randomly selected small number of people stratified by age, gender, health status, race, economic status in order to learn what proportion of the people in the group who have been infected, or are currently infected, and among them, how many have symptoms, or not. We need to allocate adequate portion of tests for studies of the general population. We do not need to test everyone, but solely the minimal number to estimate the distribution of asymptomatic carriers to assist with developing future test plans.
Case and contact tracing are essential disease control measure to stop the further spread of Covid-19. CDC had made revisions for contact tracing on June 12, 2020 [5]. To expand the testing, the following strategies for expanding the capacity for contact tracing and self-isolation should be taken. First, we should expand staffing resources to hire qualified and well-trained case investigators and contact tracers. Second, we should adequately train staff with excellent and tactful interpersonal communication skills and professional behaviors. Third, we must adopt and use digital tools for case management or contact tracing. Fourth, we can use the CDC programmatic guidance, technical assistance, and resources which are provided by CDC to hire qualified staffs and efficiently train new and existing staff. When more and more people are tested and infected individuals are identified and isolated, the proportions of the infected individuals in the population and the number of people that need to be traced will all be reduced. The capacity problem for contact tracing will be alleviated.
CONFLICT OF INTEREST
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
REFERENCES
- Peto J, Alwan NA, Godfrey KM, Burgess RA, Hunter DJ (2020) Universal weekly testing as the UK COVID-19 lockdown exit strategy. Lancet 395: 1420-1421.
- Bao W, Yue J, Rao Y (2017) A deep learning framework for financial time series using stacked autoencoders and long-short term memory. PLoS One 12: e0180944
- Meyer R (2020) There’s one big reason the U.S. economy can’t reopen. The Atlantic, USA.
- Stein R, Wroth C, Hurt A (2020) U.S. coronavirus testing still falls short. How's your state doing? Shots - Health News, USA.
- https://www.cdc.gov/coronavirus/2019-ncov/downloads/php/contact-tracing-CDC-role-and-approach.pdf.
Citation: Fang S, Hu Z, Xu T, Zhang K, Li S, et al. (2020) Mass testing and containment of Covid-19. J Emerg Med Trauma Surg Care S1: 001
Copyright: © 2020 Shenying Fang, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.