
The Vitamin D, IL-6 and the eGFR Markers a Possible Way to Elucidate the Lung–Heart–Kidney Cross-Talk in COVID-19 Disease: A Foregone Conclusion

 ,
,  , ,
, ,  ,
,  ,
,  , , , , , ,
, , , , , ,  , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Specimen Collection and Laboratory Measurements
2.3. Statistical Methods
3. Results
3.1. Clinical Characteristics of the Research Subjects
3.2. Statistical Findings
3.3. Comparison of the Study Populations
- Hypotheses about the difference of vitamin D in three groups:
- 1.1.
- The hypothesis about the difference of vitamin D levels iin PP and NNp groups.
- 1.2.
- The hypothesis about the difference of vitamin D levels iin the PP and NNh groups.
- 1.3.
- The hypothesis about the difference of vitamin D levels in the NNp and NNh groups.
- Hypotheses about the difference of vitamin D in three groups:
- 2.1.
- The hypothesis about the difference of IL-6 levels iin the PP and NNp groups.
- 2.2.
- The hypothesis about the difference of IL-6 levels iin the PP and NNh groups.
- 2.3.
- The hypothesis about the difference of IL-6 levels iin the NNp and NNh groups.
- Hypotheses about the difference of vitamin D in three groups:
- 3.1.
- The hypothesis about the difference of eGFR levels in the PP and NNp groups.
- 3.2.
- The hypothesis about the difference of eGFR levels in the PP and NNh groups.
- 3.3.
- The hypothesis about the difference of eGFR levels in the NNp and NNh groups.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dattola, A.; Silvestri, M.; Bennardo, L.; Passante, M.; Scali, E.; Patruno, C.; Nisticò, S.P. Role of vitamins in skin health: A systematic review. Curr. Nutr. Rep. 2020, 9, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Aygun, H. Vitamin D can prevent COVID-19 infection-induced multiple organ damage. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2020, 393, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, Q.; Yang, J.; Ma, Y.; Ding, G. Angiotensin II induces cholesterol accumulation and injury in podocytes. Sci. Rep. 2017, 7, 10672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollert, K.C. The renin-angiotensin system and experimental heart failure. Cardiovasc. Res. 1999, 43, 838–849. [Google Scholar] [CrossRef] [Green Version]
- Ehrenreich, H.; Weissenborn, K.; Begemann, M.; Busch, M.; Vieta, E.; Miskowiak, K.W. Erythropoietin as candidate for supportive treatment of severe COVID-19. Mol. Med. 2020, 26, 1–9. [Google Scholar] [CrossRef]
- Balzanelli, M.G.; Distratis, P.; Aityan, S.K.; Amatulli, F.; Catucci, O.; Cefalo, A.; De Michele, A.; Dipalma, G.; Inchingolo, F.; Lazzaro, R.; et al. An alternative “Trojan Horse” hypothesis for COVID-19: Immune deficiency of IL-10 and SARS-CoV-2 biology. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 1. [Google Scholar] [CrossRef] [PubMed]
- Gnanaraj, J.; Radhakrishnan, J. Cardio-renal syndrome. F1000Research 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Charitos, I.; Ballini, A.; Bottalico, L.; Cantore, S.; Passarelli, P.C.; Inchingolo, F.; D’Addona, A.; Santacroce, L. Special features of SARS-CoV-2 in daily practice. World J. Clin. Cases 2020, 8, 3920–3933. [Google Scholar] [CrossRef]
- Pham, V.H.; Gargiulo Isacco, C.; Nguyen, K.C.D.; Le, S.H.; Tran, D.K.; Nguyen, Q.V.; Pham, H.T.; Aityan, S.; Pham, S.T.; Cantore, S.; et al. Rapid and sensitive diagnostic procedure for multiple detection of pandemic coronaviridae family members SARS-CoV-2, SARS-CoV, MERS-CoV and HCoV: A translational research and cooperation between the Phan Chau Trinh University in Vietnam and University of Bari “Aldo Moro” in Italy. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7173–7191. [Google Scholar] [CrossRef]
- Zhang, Y.; Leung, D.Y.; Richers, B.N.; Liu, Y.; Remigio, L.K.; Riches, D.W.; Goleva, E. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase-1. J. Immunol. 2012, 188, 2127–2135. [Google Scholar] [CrossRef] [Green Version]
- Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; Cefalo, A.; D’angela, G.; Catucci, O.; Palazzo, D.; Amatulli, F.; Tomassone, D.; Pham, V.H.; et al. Would the End of COVID-19 Infection as a Chronic Disease? J. Stem Cells Res. Dev. Ther. 2020, 6, 057. [Google Scholar] [CrossRef]
- Ronco, C.; Reis, T. Kidney involvement in COVID-19 and rationale for extracorporeal therapies. Nat. Rev. Nephrol. 2020, 16, 308–310. [Google Scholar] [CrossRef] [Green Version]
- Muvva, J.R.; Parasa, V.R.; Lerm, M.; Svensson, M.; Brighenti, S. Polarization of human monocyte-derived cells with vitamin D promotes control of mycobacterium tuberculosis infection. Front. Immunol. 2020, 10. [Google Scholar] [CrossRef]
- Kohlmeier, M. Avoidance of vitamin D deficiency to slow the COVID-19 pandemic. BMJ Nutr. Prev. Health 2020, 3, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Biesalski, H.K. Vitamin D deficiency and co-morbidities in COVID-19 patients—A fatal relationship? NFS J. 2020, 20, 10–21. [Google Scholar] [CrossRef]
- Holick, M.; Binkley, N.C.; Bischoff-Ferrari, H.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Rosen, C.J.; Abrams, S.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.; Jones, G.; Kovacs, C.; et al. IOM committee members respond to endocrine society vitamin D guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.; Bordea, I.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.; Isacco, C.; Marinelli, G.; et al. SARS-CoV-2 disease adjuvant therapies and supplements breakthrough for the infection prevention. Microorganisms 2021, 9, 525. [Google Scholar] [CrossRef]
- Zhou, Y.-F.; Luo, B.-A.; Qin, L.-L. The association between vitamin D deficiency and community-acquired pneumonia. Medicine 2019, 98, e17252. [Google Scholar] [CrossRef]
- Lau, F.H.; Majumder, R.; Torabi, R.; Saeg, F.; Hoffman, R.; Cirillo, J.D.; Greiffenstein, P. Vitamin D insufficiency is prevalent in severe COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef]
- Kim, H.; Baek, S.; Hong, S.-M.; Lee, J.; Jung, S.M.; Lee, J.; Cho, M.-L.; Kwok, S.-K.; Park, S.-H. 1,25-dihydroxy vitamin D3 and interleukin-6 blockade synergistically regulate rheumatoid arthritis by suppressing interleukin-17 production and osteoclastogenesis. J. Korean Med. Sci. 2020, 35, e40. [Google Scholar] [CrossRef]
- White, J.H. Vitamin D metabolism and signaling in the immune system. Rev. Endocr. Metab. Disord. 2011, 13, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.; Barrat, F.J.; Crain, C.; Heath, V.L.; Savelkoul, H.F.J.; O’Garra, A. 1α,25-dihydroxyvitamin d3 has a direct effect on naive CD4+ T cells to enhance the development of Th2 cells. J. Immunol. 2001, 167, 4974–4980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Michelle, S.; Maguire, J.L.; Russell, M.L.; Smieja, M.; Walter, S.D.; Loeb, M. Low serum 25-hydroxyvitamin D level and risk of upper respiratory tract infection in children and adolescents. Clin. Infect. Dis. 2013, 57, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Gunasekar, P.; Swier, V.J.; Fleegel, J.P.; Boosani, C.; Radwan, M.M.; Agrawal, D.K. Vitamin D and macrophage polarization in epicardial adipose tissue of atherosclerotic swine. PLoS ONE 2018, 13, e0199411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz, S.; Dobnig, H.; Nijpels, G.; Heine, R.J.; Stehouwer, C.D.A.; Snijder, M.B.; Van Dam, R.M.; Dekker, J.M. Vitamin D and mortality in older men and women. Clin. Endocrinol. 2009, 71, 666–672. [Google Scholar] [CrossRef]
- Kempker, J.A.; Han, J.E.; Tangpricha, V.; Ziegler, T.R.; Martin, G.S. Vitamin D and sepsis. Derm. Endocrinol. 2012, 4, 101–108. [Google Scholar] [CrossRef]
- Silberstein, M. Correlation between premorbid IL-6 levels and COVID-19 mortality: Potential role for Vitamin D. Int. Immunopharmacol. 2020, 88, 106995. [Google Scholar] [CrossRef]
- Panitchote, A.; Mehkri, O.; Hastings, A.; Hanane, T.; Demirjian, S.; Torbic, H.; Mireles-Cabodevila, E.; Krishnan, S.; Duggal, A. Factors associated with acute kidney injury in acute respiratory distress syndrome. Ann. Intensiv. Care 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Balzanelli, G.M.; Distratis, P.; Amatulli, F.; Catucci, O.; Cefalo, A.; Lazzaro, R.; Palazzo, D.; Aityan, K.S.; Dipalma, G.; Inchingolo, F. Clinical features in predicting COVID-19. Biomed. J. Sci. Tech. Res. 2020, 29, 22921–22926. [Google Scholar]
- Balzanelli, G.M.; Distratis, P.; Aityan, S.K.; Amatulli, F.; Catucci, O.; Cefalo, A.; DiPalma, G.; Inchingolo, F.; Lazzaro, R.; Nguyen, K.C.D.; et al. COVID-19 and COVID-like patients: A brief analysis and findings of two deceased cases. Open Access Maced. J. Med. Sci. 2020, 8, 490–495. [Google Scholar] [CrossRef]
- Charitos, I.A.; Del Prete, R.; Inchingolo, F.; Mosca, A.; Carretta, D.; Ballini, A.; Santacroce, L. What we have learned for the future about COVID-19 and healthcare management of it? Acta Biomed. 2020, 91, e2020126. [Google Scholar] [CrossRef]
- Grant, W.; Lahore, H.; McDonnell, S.; Baggerly, C.; French, C.; Aliano, J.; Bhattoa, H. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Wielen, R.; de Groot, L.; van Staveren, W.; Löwik, M.; Berg, H.V.D.; Haller, J.; Moreiras, O. Serum vitamin D concentrations among elderly people in Europe. Lancet 1995, 346, 207–210. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, L.E.; Burke, F.; Mura, M.; Zheng, Y.; Qureshi, O.S.; Hewison, M.; Walker, L.S.K.; Lammas, D.A.; Raza, K.; Sansom, D.M. 1,25-dihydroxyvitamin D3 and il-2 combine to inhibit T cell production of inflammatory cytokines and promote development of regulatory T cells expressing CTLA-4 and FoxP3. J. Immunol. 2009, 183, 5458–5467. [Google Scholar] [CrossRef] [Green Version]
- Hunter, C.; Jones, S.A. IL-6 as a keystone cytokine in health and disease. Nat. Immunol. 2015, 16, 448–457. [Google Scholar] [CrossRef]
- Jones, S.A.; Jenkins, B.J. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nat. Rev. Immunol. 2018, 18, 773–789. [Google Scholar] [CrossRef]
- Karahan, S.; Katkat, F. Impact of serum 25(OH) vitamin D level on mortality in patients with COVID-19 in Turkey. J. Nutr. Health Aging 2020, 25, 189–196. [Google Scholar] [CrossRef]
- Silva, C.A.; Vicente, M.C.; Tenorio-Lopes, L.; Soliz, J.; Gargaglioni, L.H. Erythropoietin in the Locus coeruleus attenuates the ventilatory response to CO2 in rats. Respir. Physiol. Neurobiol. 2017, 236, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordea, I.; Xhajanka, E.; Candrea, S.; Bran, S.; Onișor, F.; Inchingolo, A.; Malcangi, G.; Pham, V.; Inchingolo, A.; Scarano, A.; et al. Coronavirus (SARS-CoV-2) pandemic: Future challenges for dental practitioners. Microorganisms 2020, 8, 1704. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-B.; Lin, A.M.-Y.; Chiu, T. Systemic vitamin D3 attenuated oxidative injuries in the locus coeruleus of rat brain. Ann. N. Y. Acad. Sci. 2003, 993, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Lisse, T.S. Vitamin D regulation of a SOD1-to-SOD2 antioxidative switch to prevent bone cancer. Appl. Sci. 2020, 10, 2554. [Google Scholar] [CrossRef] [Green Version]
- Ivanova, D.; Zhelev, Z.; Getsov, P.; Nikolova, B.; Aoki, I.; Higashi, T.; Bakalova, R. Vitamin K: Redox-modulation, prevention of mitochondrial dysfunction and anticancer effect. Redox Biol. 2018, 16, 352–358. [Google Scholar] [CrossRef]
- Shioi, A.; Morioka, T.; Shoji, T.; Emoto, M. The inhibitory roles of vitamin K in progression of vascular calcification. Nutrients 2020, 12, 583. [Google Scholar] [CrossRef] [Green Version]
- Balzanelli, M.; Distratis, P.; Catucci, O.; Amatulli, F.; Cefalo, A.; Lazzaro, R.; Aityan, K.S.; Dalagni, G.; Nico, A.; De Michele, A.; et al. Clinical and diagnostic findings in COVID-19 patients: An original research from SG Moscati Hospital in Taranto Italy. J. Biol. Regul. Homeost. Agents. 2021, 35. [Google Scholar]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental disinfection of a dental clinic during the COVID-19 pandemic: A narrative insight. BioMed Res. Int. 2020, 2020, 1–15. [Google Scholar] [CrossRef]
- Basu, R.K.; Wheeler, D.S. Kidney-lung cross-talk and acute kidney injury. Pediatr. Nephrol. 2013, 28, 2239–2248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oishi, Y.; Manabe, I. Organ system crosstalk in cardiometabolic disease in the age of multimorbidity. Front. Cardiovasc. Med. 2020, 7. [Google Scholar] [CrossRef]
- Cozzolino, M.; Ketteler, M.; Zehnder, D. The vitamin D system: A crosstalk between the heart and kidney. Eur. J. Hear. Fail. 2010, 12, 1031–1041. [Google Scholar] [CrossRef] [Green Version]
- Bellocchio, L.; Bordea, I.; Ballini, A.; Lorusso, F.; Hazballa, D.; Isacco, C.; Malcangi, G.; Inchingolo, A.; Dipalma, G.; Inchingolo, F.; et al. Environmental issues and neurological manifestations associated with COVID-19 pandemic: New aspects of the disease? Int. J. Environ. Res. Public Health 2020, 17, 8049. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M. Taste Dysfunction and Long COVID-19. Front. Cell. Infect. Microbiol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Mean | ±δ | Confidence Interval | ||
|---|---|---|---|---|---|
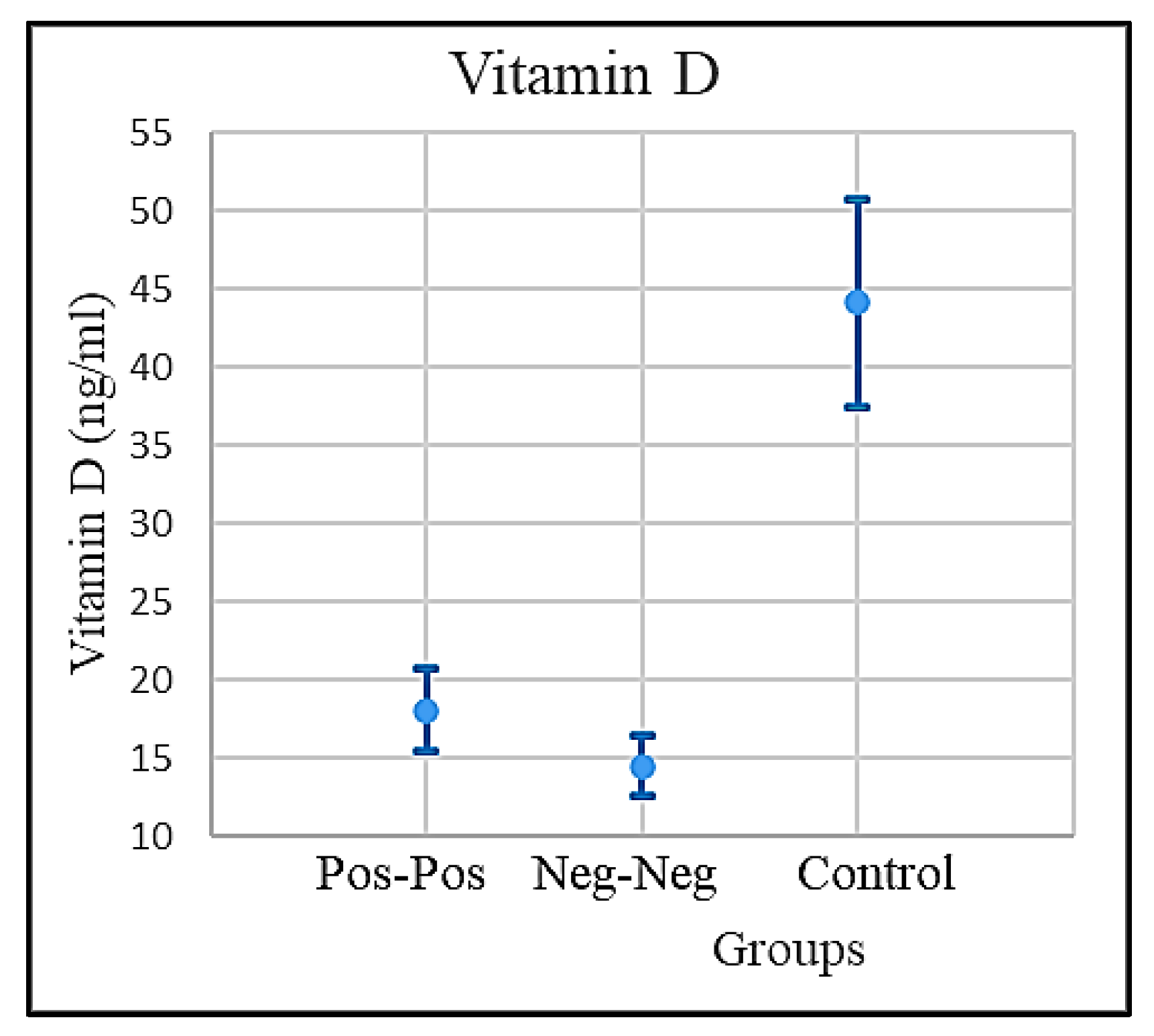
| Vitamin D (ng/mL) | PP Patients | 18.0475 | 2.639475 | 15.40802 | 20.68698 |
| NNp | 14.49355 | 1.871572 | 12.62198 | 16.36512 | |
| NNh (Healthy) | 44.0986 | 6.599012 | 37.49959 | 50.69762 | |
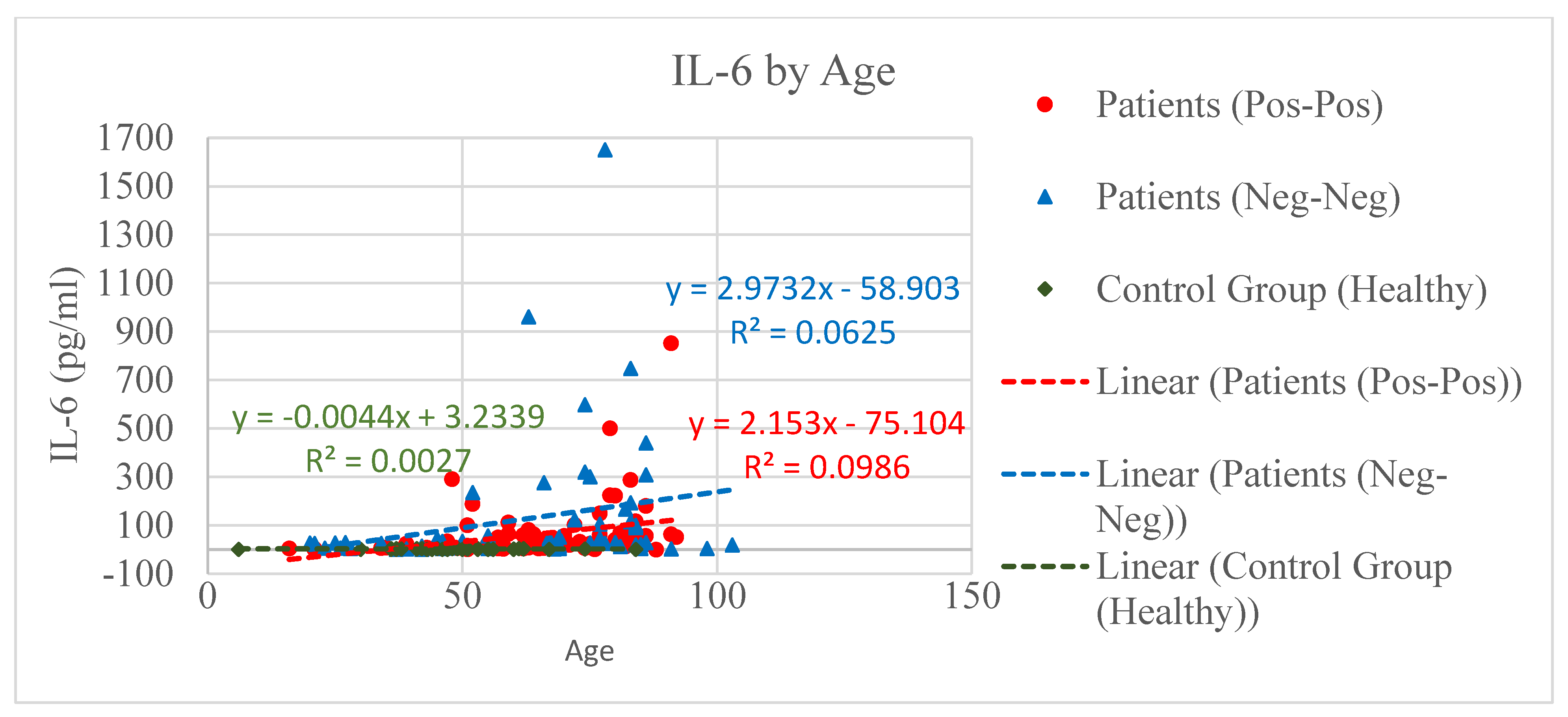
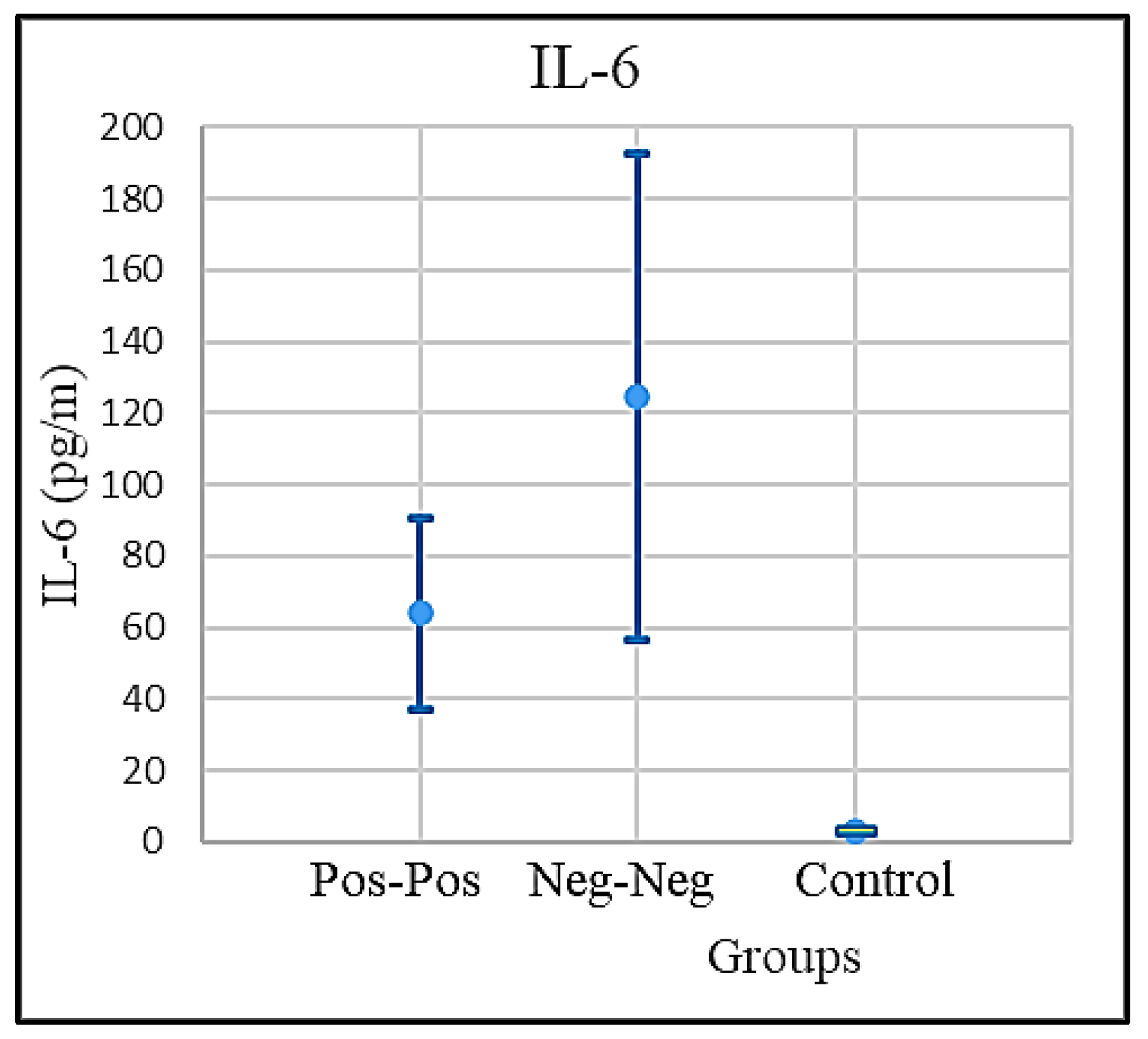
| IL-6 (pg/m) | PP Patients | 64.10633 | 26.77383 | 37.3325 | 90.88016 |
| NNp | 124.5258 | 68.18824 | 56.33757 | 192.714 | |
| NNh (Healthy) | 3.023256 | 0.337694 | 2.685562 | 3.36095 | |
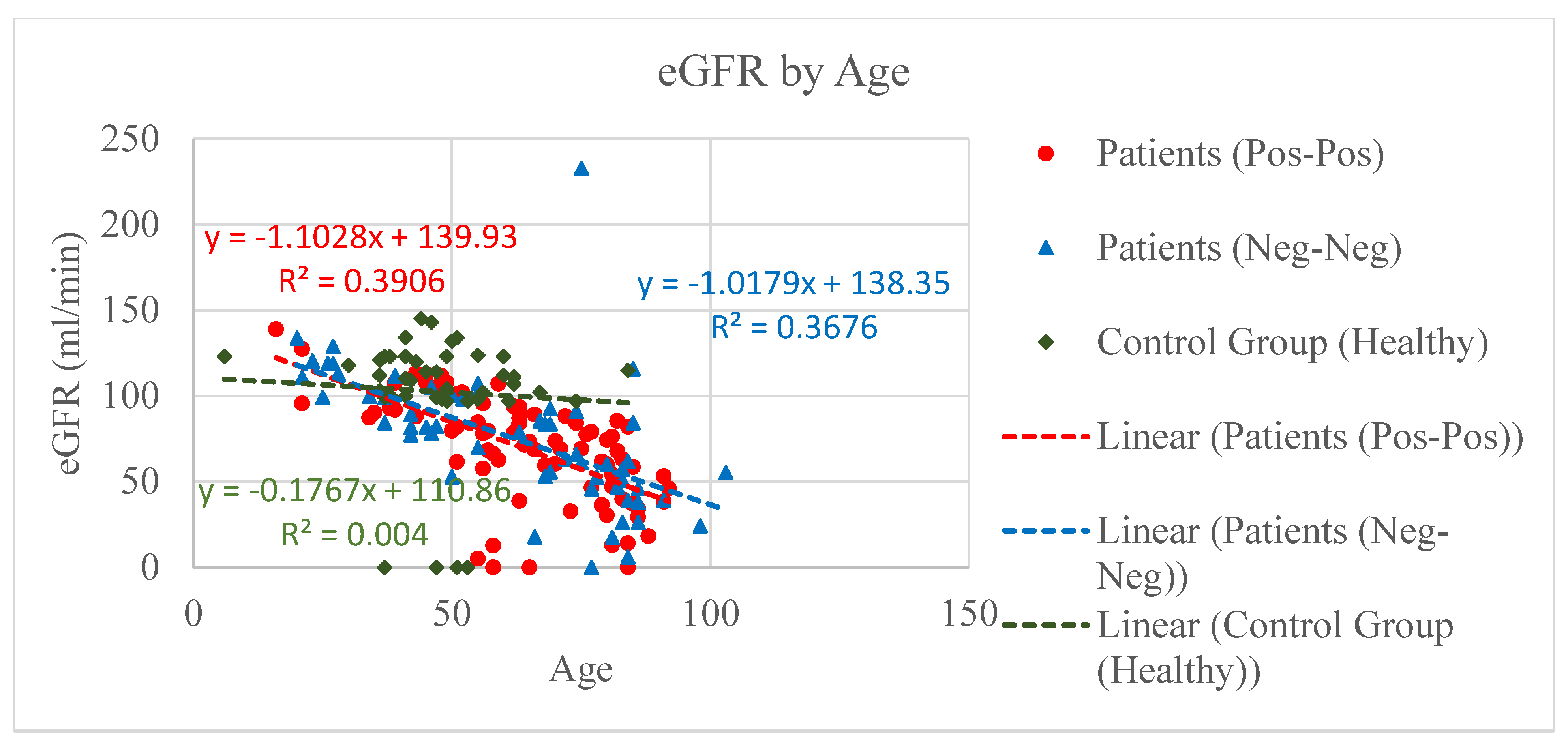
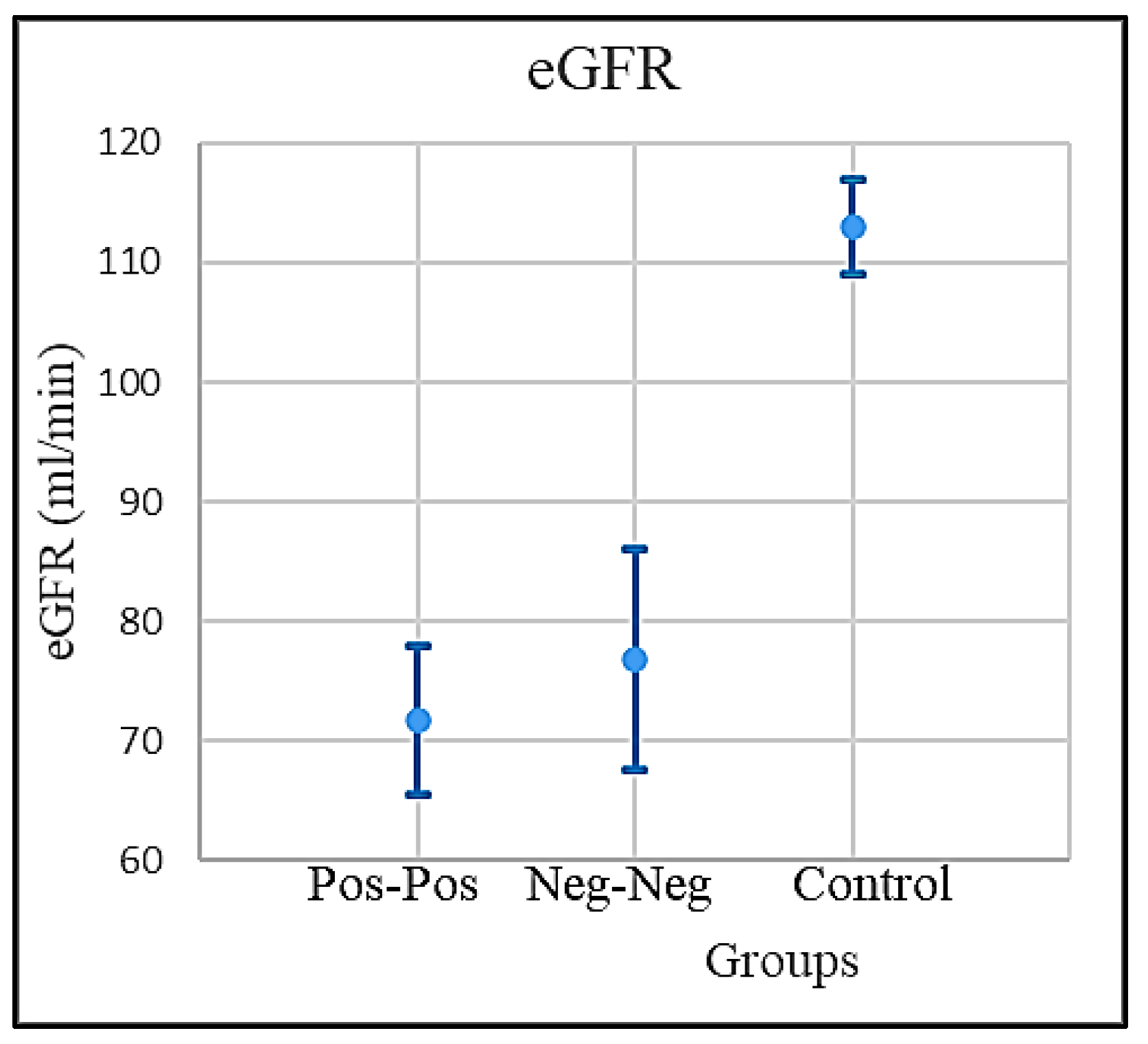
| eGFR (mL/min) | PP Patients | 71.71623 | 6.263475 | 65.45276 | 77.97971 |
| NNp | 76.79361 | 68.18824 | 8.605366 | 144.9818 | |
| NNh (Healthy) | 112.9769 | 4.122511 | 108.8544 | 117.0994 | |
| Vitamin D (ng/mL) | |||
|---|---|---|---|
| PP | NNp | NNh | |
| Diff of means = | 3.55 | 26.05 | 29.61 |
| Sp = | 10.20 | 15.90 | 14.92 |
| 1/sqrt(np) = | 0.17 | 0.19 | 0.20 |
| df = | 140 | 121 | 103 |
| t-cr = | 1.98 | 1.98 | 1.98 |
| t-score = | 2.06 | 8.67 | 10.00 |
| Test is | Significant | Significant | Significant |
| IL-6 (pg/m) | |||
|---|---|---|---|
| PP | NNp | NNh | |
| Diff of means = | 60.42 | 61.08 | 121.50 |
| Sp = | 198.93 | 97.24 | 206.60 |
| 1/sqrt(np) = | 0.17 | 0.19 | 0.20 |
| df = | 140 | 121 | 103 |
| t-cr = | 1.98 | 1.98 | 1.98 |
| t-score = | 1.80 | 3.32 | 2.96 |
| Test is | Insignificant | Significant | Significant |
| eGFR (mL/min) | |||
|---|---|---|---|
| PP | NNp | NNh | |
| Diff of means = | 5.08 | 41.26 | 36.18 |
| Sp = | 32.27 | 24.09 | 29.69 |
| 1/sqrt(np) = | 0.17 | 0.19 | 0.20 |
| df = | 140 | 121 | 103 |
| t-cr = | 1.98 | 1.98 | 1.98 |
| t-score = | 0.93 | 9.06 | 6.14 |
| Test is | Insignificant | Significant | Significant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; Cefalo, A.; Catucci, O.; Aityan, S.K.; Dipalma, G.; Vimercati, L.; Inchingolo, A.D.; Maggiore, M.E.; et al. The Vitamin D, IL-6 and the eGFR Markers a Possible Way to Elucidate the Lung–Heart–Kidney Cross-Talk in COVID-19 Disease: A Foregone Conclusion. Microorganisms 2021, 9, 1903. https://doi.org/10.3390/microorganisms9091903
Balzanelli MG, Distratis P, Lazzaro R, Cefalo A, Catucci O, Aityan SK, Dipalma G, Vimercati L, Inchingolo AD, Maggiore ME, et al. The Vitamin D, IL-6 and the eGFR Markers a Possible Way to Elucidate the Lung–Heart–Kidney Cross-Talk in COVID-19 Disease: A Foregone Conclusion. Microorganisms. 2021; 9(9):1903. https://doi.org/10.3390/microorganisms9091903
Chicago/Turabian StyleBalzanelli, Mario Giosuè, Pietro Distratis, Rita Lazzaro, Angelo Cefalo, Orazio Catucci, Sergey Khachatur Aityan, Gianna Dipalma, Luigi Vimercati, Alessio Danilo Inchingolo, Maria Elena Maggiore, and et al. 2021. "The Vitamin D, IL-6 and the eGFR Markers a Possible Way to Elucidate the Lung–Heart–Kidney Cross-Talk in COVID-19 Disease: A Foregone Conclusion" Microorganisms 9, no. 9: 1903. https://doi.org/10.3390/microorganisms9091903