Psychosocial Distress in Adult Patients Awaiting Cancer Surgery during the COVID-19 Pandemic

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population
2.3. Questionnaires
2.4. Semi-Structured Interviews
2.5. Qualitative Analysis
2.6. Quantitative Analysis
2.7. Statistical Methods
2.8. Integration
3. Results
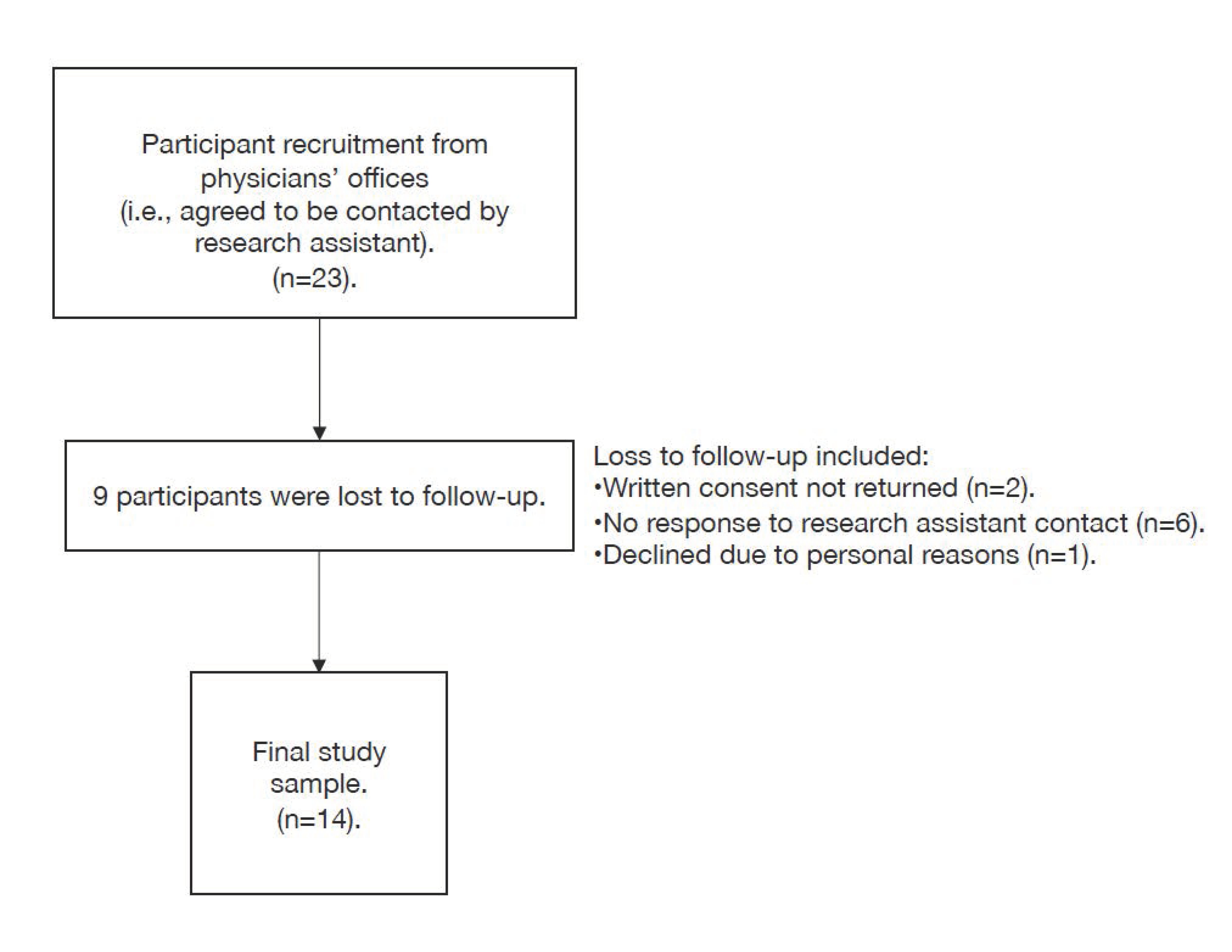
3.1. Participants
3.2. Qualitative Analysis
3.2.1. Uncertainty
“…was an emotional rollercoaster basically. It’s something I never want to experience again because I’m not a doctor, all I knew that I have a tumor that had to be removed, and waiting. … I had to wait six months for my surgery because of COVID. And so me not knowing, that’s a lot to worry because I don’t know if it’s growing or spreading. … On a daily basis, that was very stressful. And it was really hard to concentrate because it couldn’t leave your mind, really.”[Participant #9]
“The prospect of this expanding into colon cancer was not a nice thought. So I had extreme concerns about that. As you know, I mean, one of the other issues about this, of course, is being prostate cancer, is incontinence, erectile dysfunction, sexual function. These are all very emotional and difficult life changing possibilities. And of course, with the delay, you know, how much worse could these things go? Would this guarantee that I would be incontinent, that I would have to wear diapers? You know, these are highly amplified by the delay.”[Participant #13]
“Whether or not the COVID-19 is here, whether the COVID-19 is going to strike me, get rid of this cancer. Get it out. And this is why I think… Like yes, I understand everything about the COVID-19. But when there’s a major surgery that has to be done, those hospitals should automatically put us through. … I could have died waiting for that surgery. Not from the COVID-19 but what was in my body…”[Participant #11]
3.2.2. Life Changes
“I’m an obsessive gardener and reader and knitter. And so there hasn’t been that much difference in that respect. … it was very annoying because I like to walk, and I couldn’t go to the beaches and so on and so forth. But I managed. I can be pretty creative when necessary. So compared to many people, I’m all right.”[Participant #19]
3.2.3. Coping with Stress
“I guess when I get stressed, I probably kind of close down or try not to think about it. I’ve been trying to keep busy doing other things so I don’t think about it. But then it gets to a point that, you know, you just… It’s hard.”[Participant #7]
“I mean we have a lot of support. We have a lot of family and friends and church people that they all know. Like, I let everybody know that this is what I have to have done, and the date of my surgery. And everybody is very supportive and have sent a lot of encouraging messages and things to me.”[Participant #5]
“Well, the stress and the strain that I was under … Like my [family member] had a stroke two years ago, and I like to keep things away from him that’s going to get him stressed out and that. So, I’m doing everything I can not to like talk about it.”[Participant #11]
3.2.4. Communication
“I’d say that the impact and the anxiety was all before I had enough information. Once I had enough information… And you know, hats off and great thank you to both of those specialists that I mentioned at how communicative they were and how not one phone call that I had with them felt like I was taking up their time or that there was a time limit on the call. So what got me through and eased the anxiety and everything was good information in the meantime”[Participant #14]
“And of course, every time I called, I would just get a recording that said, ‘Everything’s shut down; everything’s shut down’. … It was stressful…very stressful.”[Participant #15]
“I just wish sometimes that I could have…if there was a number that you could have called to just say, ‘Hey, what’s going on or do you think surgeries would be opening up soon?’”.[Participant #18]
“Like I was frustrated because I mean I would call Dr. [X’s] office and not really get any kind of response, you know? Like you’d get a message about COVID and appointments are…there’s no appointments happening, you know, because of COVID, and we’ll contact you. And you’d leave messages and… You know, I left a couple of messages and never got any response, you know?”[Participant #7]
3.2.5. Experiences
“My concern was, and maybe I was selfish in thinking this, oh, my gosh, if I get to the hospital…if they do my surgery during, you know, when COVID first started, if I did go in for my surgery, how will I know…what if other nurses and doctors who were working with people all the time, what if they’re around somebody that has COVID and didn’t know it, and then they get it, and they’re asymptomatic so they won’t know? And what if I pick it up, and I’m so not strong, gosh, would I be able to fight COVID along with everything else?”[Participant #18]
“…The people at the hospital, the staff, everybody that was there—everybody—made you realize, like, you know, you’re so lucky that… You know, I had to wait but I was so lucky to be in good hands afterwards. Like they were amazing. Like I don’t know how they do these jobs, but they were all amazing, which made me feel so much better.”[Participant #18]
3.2.6. Health Services
“…one wonders … what’s the best evil here? Clearly, the public good is more important. But at what point is what potentially is I guess it’s determined to be not life threatening, but at what point is prostate cancer less and less important than other life-threatening situations?”[Participant #13]
3.3. Quantitative Analysis
3.4. Integration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy. 2008, 13, 92–98. [Google Scholar] [CrossRef]
- Nova Scotia Health Authority Perioperative Services. NSHA Perioperative and Interventional Radiology Services during COVID-19 Pandemic. Available online: https://www.cdha.nshealth.ca/system/files/sites/documents/perioperative-and-ir-services-during-covid3204pm.pdf (accessed on 30 January 2021).
- Tongco, M.D.C. Purposive sampling as a tool for informant selection. Ethnobot. Res. Appl. 2007, 5, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Cliff, A.M.; MacDonagh, R.P. Psychosocial morbidity in prostate cancer: II. A comparison of patients and partners. BJU Int. 2000, 86, 834–839. [Google Scholar] [CrossRef] [Green Version]
- Ng, C.G.; Mohamed, S.; Kaur, K.; Sulaiman, A.H.; Zainal, N.Z.; Taib, N.A.; MyBCC Study Group. Perceived distress and its association with depression and anxiety in breast cancer patients. PLoS ONE 2017, 12, e0172975. [Google Scholar] [CrossRef] [PubMed]
- Sawka, A.M.; Ghai, S.; Tomlinson, G.; Rotstein, L.; Gilbert, R.; Gullane, P.; Pasternak, J.; Brown, D.; de Almeida, J.; Irish, J.; et al. A protocol for a Canadian prospective observational study of decision-making on active surveillance or surgery for low-risk papillary thyroid cancer. BMJ Open 2018, 8, e020298. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, H.; Schofield, P.; Cockburn, J.; Butow, P.; Tattersall, M.; Turner, J.; Girgis, A.; Bandaranayake, D.; Bowman, D. How to recognize and manage psychological distress in cancer patients. Eur. J. Cancer Care (Engl.) 2005, 14, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived stress scale. In Measuring Stress: A Guide for Health and Social Scientists; Cohen, S., Kessler, R.C., Gordon, L.U., Eds.; Oxford University Press: New York, NY, USA, 1994; p. 10. [Google Scholar]
- Cohen, S. Perceived stress in a probability sample of the United States. In The Claremont Symposium on Applied Social Psychology. The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage Publications, Inc.: New York, NY, USA, 1988; pp. 31–67. [Google Scholar]
- Daubenmier, J.J.; Weidner, G.; Marlin, R.; Crutchfield, L.; Dunn-Emke, S.; Chi, C.; Gao, B.; Carroll, P.; Ornish, D. Lifestyle and health-related quality of life of men with prostate cancer managed with active surveillance. Urology 2006, 67, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Eskander, A.; Devins, G.M.; Freeman, J.; Wei, A.C.; Rotstein, L.; Chauhan, N.; Sawka, A.M.; Brown, D.; Irish, J.; Gilbert, R.; et al. Waiting for thyroid surgery: A study of psychological morbidity and determinants of health associated with long wait times for thyroid surgery. Laryngoscope 2013, 123, 541–547. [Google Scholar] [CrossRef]
- Golden-Kreutz, D.M.; Browne, M.W.; Frierson, G.M.; Andersen, B.L. Assessing stress in cancer patients: A second-order factor analysis model for the Perceived Stress Scale. Assessment 2004, 11, 216–223. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. APA Handbook of Research Methods in Psychology; Cooper, H., Camic, P., Sher, K., Panter, A.T., Long, D., Rindskopf, D., Eds.; APA Handbooks in Psychology Series and APA Reference Books Collection; American Psychological Association: Washington, MA, USA, 2012; Volume 2, pp. 51–57. [Google Scholar]
- Moran-Ellis, J.; Alexander, V.D.; Cronin, A.; Dickinson, M.; Fielding, J.; Sleney, J.; Thomas, H. Triangulation and integration: Processes, claims and implications. Qual. Res. 2006, 6, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Bultz, B.D.; Groff, S.L.; Fitch, M.; Blais, M.C.; Howes, J.; Levy, K.; Mayer, C. Implementing screening for distress, the 6th vital sign: A Canadian strategy for changing practice. Psychooncology 2011, 20, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Holland, J.C.; Bultz, B.D. The NCCN guideline for distress management: A case for making distress the sixth vital sign. J. Natl. Compr. Canc. Netw. 2007, 5, 3–7. [Google Scholar] [CrossRef]
- Linardos, M.; Carnevale, S.; Agostini, L.; Belella, D. Multidisciplinary interview to assess distress in patients waiting for breast cancer treatments. Trans. Cancer Res. 2018, 7, S266–S271. [Google Scholar] [CrossRef]
- Visser, M.R.M.; van Lanschot, J.J.B.; van der Velden, J.; Kloek, J.J.; Gouma, D.J.; Sprangers, M.A.G. Quality of life in newly diagnosed cancer patients waiting for surgery is seriously impaired. J. Surg. Oncol. 2006, 93, 571–577. [Google Scholar] [CrossRef]
- Gagliardi, A.R.; Yip, C.Y.Y.; Irish, J.; Wright, F.C.; Rubin, B.; Ross, H.; Green, R.; Abbey, S.; McAndrews, M.P.; Stewart, D.E. The psychological burden of waiting for procedures and patient-centred strategies that could support the mental health of wait-listed patients and caregivers during the COVID-19 pandemic: A scoping review. Health Expect. 2021, 1–13. [Google Scholar] [CrossRef]
- Leung, M.S.T.; Lin, S.G.; Chow, J.; Harky, A. COVID-19 and Oncology: Service transformation during pandemic. Cancer Med. 2020, 9, 7161–7171. [Google Scholar] [CrossRef] [PubMed]
- Dale, W.; Bilir, P.; Han, M.; Meltzer, D. The role of anxiety in prostate carcinoma: A structured review of the literature. Cancer 2005, 104, 467–478. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Miyauchi, A.; Ito, Y.; Ito, M.; Kudo, T.; Tanaka, M.; Kohsaka, K.; Kasahara, T.; Nishihara, E.; Fukata, S.; et al. Quality of Life in Patients with Low-Risk Papillary Thyroid Microcarcinoma: Active Surveillance Versus Immediate Surgery. Endocr. Pract. 2020, 26, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, K.J.; Meyer, M.E.; Giobbie-Hurder, A.; Emmons, K.M.; Weeks, J.C.; Winer, E.P.; Partridge, A.H. Long-term risk perceptions of women with ductal carcinoma in situ. Oncologist 2013, 18, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | n | % |
|---|---|---|
| Total participants | 14 | 100 |
| Demographics | ||
| Sex | ||
| Female | 10 | 71.4 |
| Education (highest level of completion) | ||
| Less than high school | 2 | 14.3 |
| High school | 2 | 14.3 |
| College or undergraduate university | 6 | 42.8 |
| Postgraduate university or professional program | 4 | 28.6 |
| Living situation | ||
| Children in home | 2 | 14.3 |
| Partner in home | 11 | 78.6 |
| Others in home (roommates, other family members) | 1 | 7.1 |
| Other (people other than those above) | 2 | 14.3 |
| Marital status | ||
| Married | 8 | 57.2 |
| Single/never married | 2 | 14.3 |
| Divorced/separated | 1 | 7.1 |
| Common-law | 2 | 14.3 |
| Widowed | 1 | 7.1 |
| Clinical Characteristics | ||
| Number of medical history diagnoses | ||
| 0 | 0 | 0.0 |
| 1 | 3 | 21.4 |
| 2 | 1 | 7.1 |
| 3+ | 10 | 71.5 |
| Prior surgical history/experiences | ||
| Yes | 12 | 85.7 |
| Disease site | ||
| Breast | 3 | 21.4 |
| Prostate | 3 | 21.4 |
| Thyroid | 3 | 21.4 |
| Kidney | 2 | 14.4 |
| Gynecological | 3 | 21.4 |
| Diagnoses | ||
| WDTC | 3 | 21.4 |
| ADH | 3 | 21.4 |
| RCC | 3 | 21.4 |
| Prostate Cancer | 3 | 21.4 |
| Uterine Cancer | 1 | 7.1 |
| Endometrial Adenocarcinoma | 1 | 7.1 |
| Completed surgery prior to interview | ||
| Yes | 9 | 64.3 |
| Questionnaire | Score Range | N | % | Median | IQR |
|---|---|---|---|---|---|
| HADS | |||||
| Total Score | 0–42 | 14 | 100 | 12.5 | 14.3 |
| Anxiety score | 0–21 | 14 | 100 | 8.5 | 6.5 |
| Normal | 0–7 | 5 | 35.7 | ||
| Borderline abnormal | 8–10 | 4 | 28.6 | ||
| Abnormal | 11–21 | 5 | 35.7 | ||
| Depression score | 0–21 | 14 | 100 | 5.0 | 7.8 |
| Normal | 0–7 | 8 | 57.1 | ||
| Borderline abnormal | 8–10 | 4 | 28.6 | ||
| Abnormal | 11–21 | 2 | 14.3 | ||
| PSS | |||||
| Total score | 0–40 | 14 | 100 | 19.0 | 11.5 |
| Low stress | 0–13 | 5 | 35.7 | ||
| Moderate stress | 14–26 | 7 | 50.0 | ||
| High perceived stress | 27–40 | 2 | 14.3 | ||
| Questionnaire | Score (Median, IQR) | High Endorsement of Symptoms Score | Supporting Quote | Low Endorsement of Symptoms Score | Supporting Quote |
|---|---|---|---|---|---|
| HADS | 12.5 (14.3) | 26 | Oh, I could not sleep. I did not sleep, no. It was to the point where I had to concentrate and start trying a routine to figure out how to sleep because I was just too worried. | 4 | You know, I’ve wondered, you know, is that going to continue to spread or how fast might that spread or will they find more when they do surgery? So I have had that thought. But I certainly realize there’s nothing I can do about it. What is, is. What’s there is there. But no, I’m not, you know, depressed or anything like that. |
| PSS | 19.0 (11.5) | 32 | Well, it was extremely stressful being told that everything was cancelled. That was very frightening to me. It’s like what do you mean cancelled? | 5 | I mean no one’s looking forward to surgery in the first place. But because they never gave me a sense of urgency in the first place, that I felt, you know, okay, about it. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forner, D.; Murnaghan, S.; Porter, G.; Mason, R.J.; Hong, P.; Taylor, S.M.; Bentley, J.; Hirsch, G.; Noel, C.W.; Rigby, M.H.; et al. Psychosocial Distress in Adult Patients Awaiting Cancer Surgery during the COVID-19 Pandemic. Curr. Oncol. 2021, 28, 1867-1878. https://doi.org/10.3390/curroncol28030173
Forner D, Murnaghan S, Porter G, Mason RJ, Hong P, Taylor SM, Bentley J, Hirsch G, Noel CW, Rigby MH, et al. Psychosocial Distress in Adult Patients Awaiting Cancer Surgery during the COVID-19 Pandemic. Current Oncology. 2021; 28(3):1867-1878. https://doi.org/10.3390/curroncol28030173
Chicago/Turabian StyleForner, David, Sarah Murnaghan, Geoffrey Porter, Ross J. Mason, Paul Hong, S. Mark Taylor, James Bentley, Gregory Hirsch, Christopher W. Noel, Matthew H. Rigby, and et al. 2021. "Psychosocial Distress in Adult Patients Awaiting Cancer Surgery during the COVID-19 Pandemic" Current Oncology 28, no. 3: 1867-1878. https://doi.org/10.3390/curroncol28030173