
The Potential of Cardiac Telerehabilitation as Delivery Rehabilitation Care Model in Heart Failure during COVID-19 and Transmissible Disease Outbreak: A Systematic Scoping Review of the Latest RCTs

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
- P (Population): Heart faillure patients;
- I (Intervention): Cardiac telerehabilitation;
- C (Comparison): Not applicable;
- O (Outcome): Delivery rehabilitation care model, safety, and efficacy;
- S (Studies): Randomized controlled trial studies.
2.4. Data Extraction
2.5. Quality Assessment
3. Results
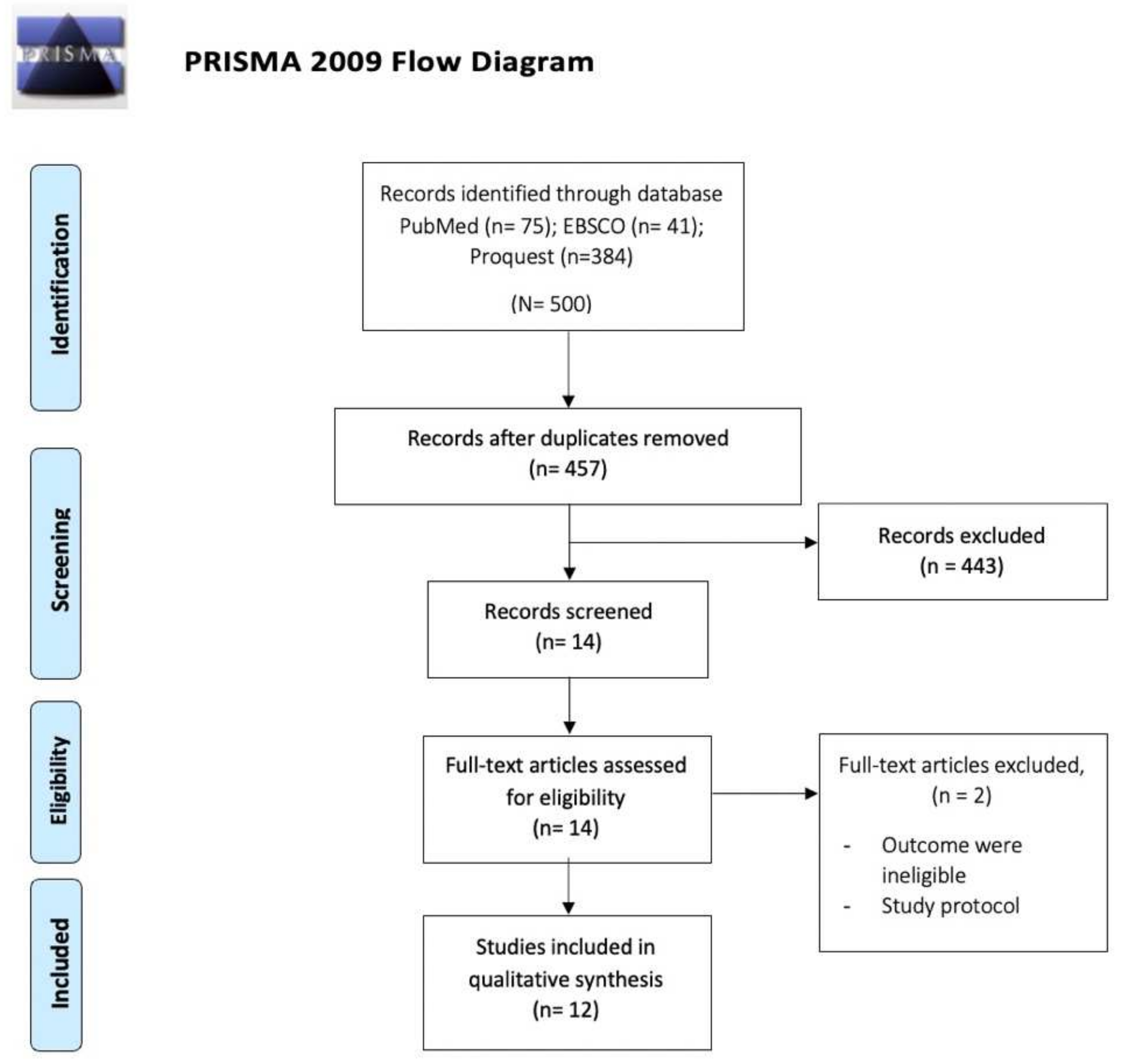
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Study Outcome
3.3.1. Cardiac Telerehabilitation Model
3.3.2. Delivery Rehabilitation Care Service
3.3.3. Feasibility, Safety, and Efficacy
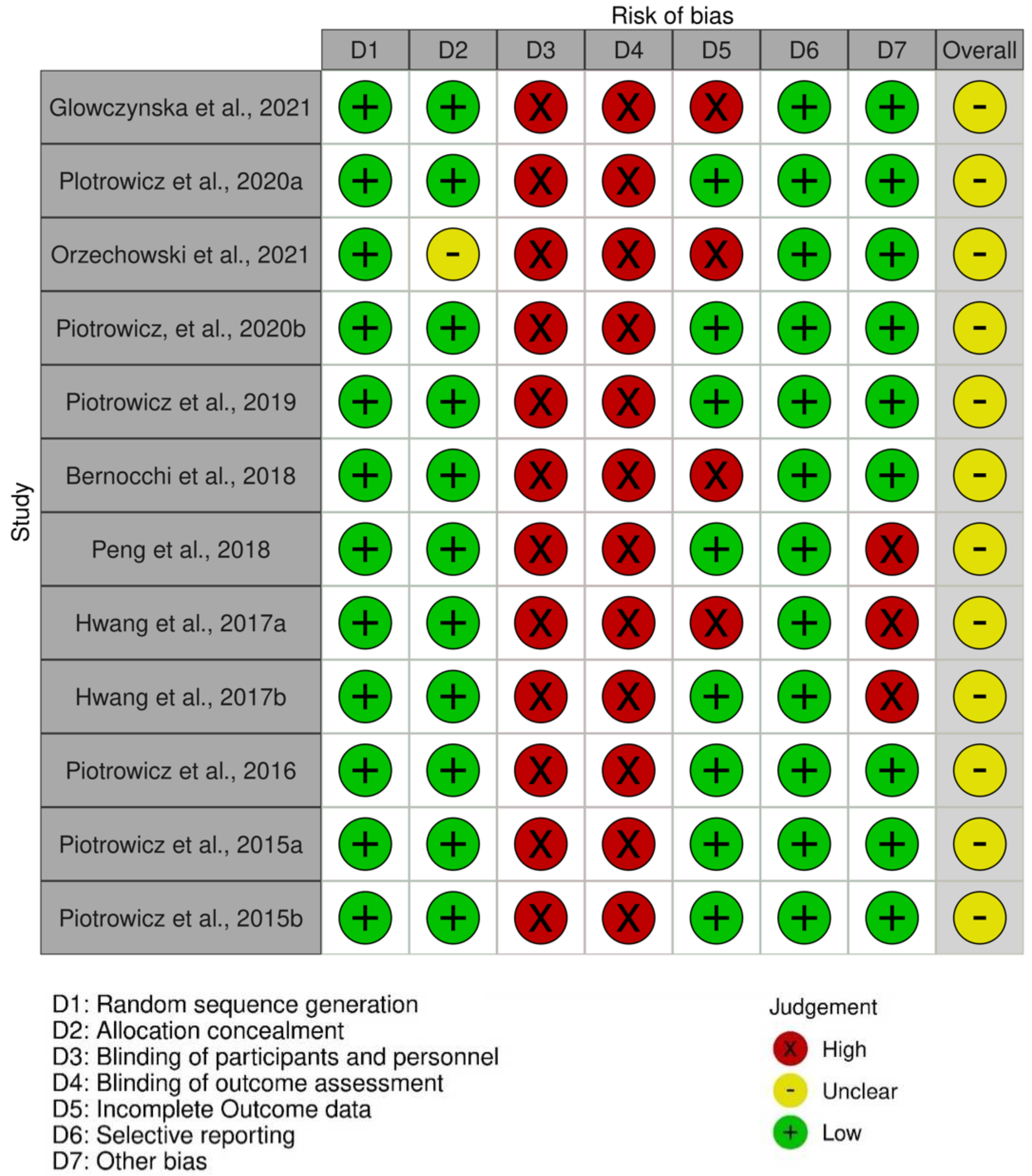
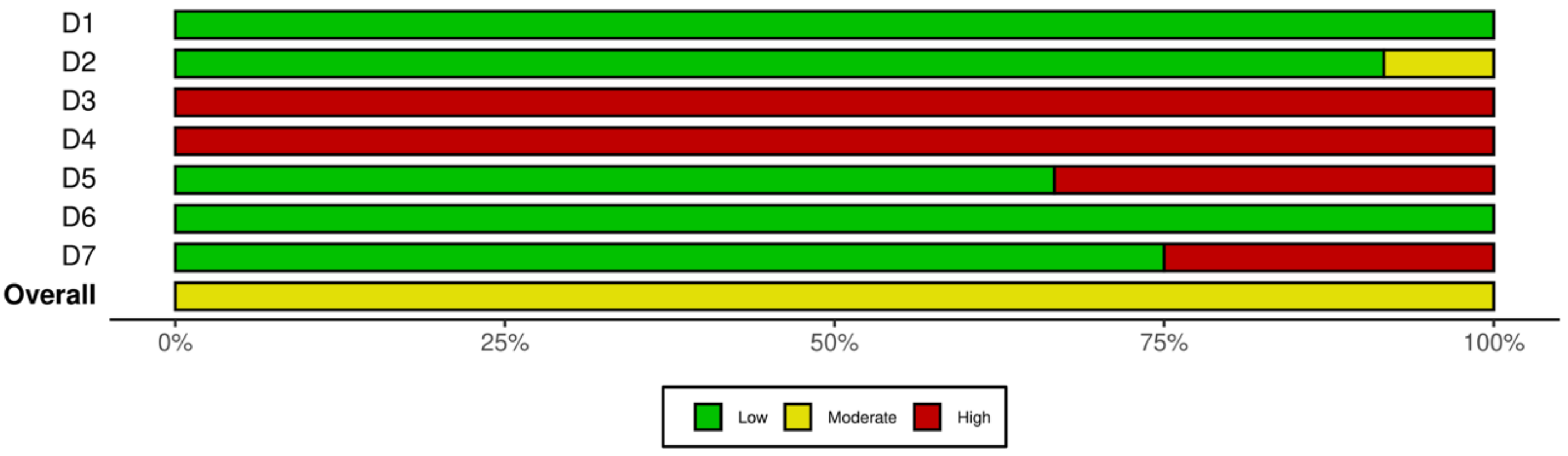
3.3.4. Quality of Included Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. List of Keywords Used during Literature Search Process
- Pubmed:
- ((“telehealth s”[All Fields] OR “telemedicine”[MeSH Terms] OR “telemedicine”[All Fields] OR “telehealth”[All Fields] OR “telenursing”[MeSH Terms] OR “telenursing”[All Fields]) AND (“cardiac rehabilitation”[MeSH Terms] OR (“cardiac”[All Fields] AND “rehabilitation”[All Fields]) OR “cardiac rehabilitation”[All Fields])) AND (“heart failure”[MeSH Terms] OR (“heart”[All Fields] AND “failure”[All Fields]) OR “heart failure”[All Fields] OR ((“congestive”[MeSH Subheading] OR “congestive”[All Field) AND (“heart failure”[MeSH Terms] OR (“heart”[All Fields] AND “failure”[All Fields]) OR “heart failure”[All Fields]))).
- ProQuest:
- (("telehealth s”[All Fields] OR “telemedicine”[MeSH Terms] OR “telemedicine”[All Fields] OR “telehealth”[All Fields] OR “telenursing”[MeSH Terms] OR “telenursing”[All Fields]) AND (“cardiac rehabilitation”[MeSH Terms] OR (“cardiac”[All Fields] AND “rehabilitation”[All Fields]) OR “cardiac rehabilitation”[All Fields])) AND (“heart failure”[MeSH Terms] OR (“heart”[All Fields] AND “failure”[All Fields]) OR “heart failure”[All Fields] OR ((“congestive”[MeSH Subheading] OR “congestivel”[All Fields]) AND (“heart failure”[MeSH Terms] OR (“heart”[All Fields] AND “failure”[All Fields]) OR “heart failure”[All Fields]))) with applied filters: scholarly journal, full text, peer review, and Publication date 2012–2020.
- EBSCO:
- (telehealth or telemedicine or telemonitoring or telepractice or telenursing or telecare) AND (cardiac rehabilitation or cardiovascular rehabilitation or cardiac rehab or cardiovascular rehab) AND (heart failure or cardiac failure or CHF or chronic heart failure or congestive heart failure).
References
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Gutierrez, E.J.; Yamin, M.; Siswanto, B.B.; Virani, S.S. Effect of Heart Failure on the Outcome of COVID-19—A Meta Analysis and Systematic Review. Am. J. Emerg. Med. 2021, 46, 204. [Google Scholar] [CrossRef] [PubMed]
- Pepera, G.; Tribali, M.S.; Batalik, L.; Petrov, I.; Papathanasiou, J. Epidemiology, Risk Factors and Prognosis of Cardiovascular Disease in the Coronavirus Disease 2019 (COVID-19) Pandemic Era: A Systematic Review. Rev. Cardiovasc. Med. 2022, 23, 28. [Google Scholar] [CrossRef] [PubMed]
- Tersalvi, G.; Winterton, D.; Cioffi, G.M.; Ghidini, S.; Roberto, M.; Biasco, L.; Pedrazzini, G.; Dauw, J.; Ameri, P.; Vicenzi, M. Telemedicine in Heart Failure During COVID-19: A Step into the Future. Front. Cardiovasc. Med. 2020, 7, 612818. [Google Scholar] [CrossRef] [PubMed]
- DeFilippis, E.M.; Reza, N.; Donald, E.; Givertz, M.M.; Lindenfeld, J.; Jessup, M. Considerations for Heart Failure Care During the COVID-19 Pandemic. JACC Heart Fail. 2020, 8, 681–691. [Google Scholar] [CrossRef]
- Reza, N.; DeFilippis, E.M.; Jessup, M. Secondary Impact of the COVID-19 Pandemic on Patients with Heart Failure. Circ. Heart Fail. 2020, 13, e007219. [Google Scholar] [CrossRef]
- Griffo, R.; Ambrosetti, M.; Furgi, G.; Carlon, R.; Chieffo, C.; Favretto, G.; Febo, O.; Corrà, U.; Fattirolli, F.; Giannuzzi, P.; et al. Standards and outcome measures in cardiovascular rehabilitation. Position paper GICR/IACPR. Monaldi Arch. Chest Dis. 2012, 78, 166–192. [Google Scholar] [CrossRef]
- Ting, P.; Saner, H.; Dafoe, W. The Lexicon of “Cardiac Rehabilitation”: Is It Time for an Evolutionary New Term? Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 251–253. [Google Scholar] [CrossRef]
- Kim, Y.H.; So, W.-Y. Gender Differences in Home-Based Cardiac Rehabilitation of Post-Percutaneous Coronary Intervention Patients. Aging Clin. Exp. Res. 2019, 31, 249–255. [Google Scholar] [CrossRef]
- Khoshrounejad, F.; Hamednia, M.; Mehrjerd, A.; Pichaghsaz, S.; Jamalirad, H.; Sargolzaei, M.; Hoseini, B.; Aalaei, S. Telehealth-Based Services During the COVID-19 Pandemic: A Systematic Review of Features and Challenges. Front. Public Health 2021, 9, 977. [Google Scholar] [CrossRef]
- Han, Y.; Zeng, H.; Jiang, H.; Yang, Y.; Yuan, Z.; Cheng, X.; Jing, Z.; Liu, B.; Chen, J.; Nie, S.; et al. CSC Expert Consensus on Principles of Clinical Management of Patients with Severe Emergent Cardiovascular Diseases During the COVID-19 Epidemic. Circulation 2020, 141, e810–e816. [Google Scholar] [CrossRef] [Green Version]
- Ajibade, A.; Younas, H.; Pullan, M.; Harky, A. Telemedicine in Cardiovascular Surgery during COVID-19 Pandemic: A Systematic Review and Our Experience. J. Card. Surg. 2020, 35, 2773–2784. [Google Scholar] [CrossRef] [PubMed]
- Galiero, R.; Pafundi, P.C.; Nevola, R.; Rinaldi, L.; Acierno, C.; Caturano, A.; Salvatore, T.; Adinolfi, L.E.; Costagliola, C.; Sasso, F.C. The Importance of Telemedicine during COVID-19 Pandemic: A Focus on Diabetic Retinopathy. J. Diabetes Res. 2020, 2020, 9036847. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.; Kenia, P.; Nagakumar, P.; Gupta, A. Paediatric and Adolescent Asthma: A Narrative Review of Telemedicine and Emerging Technologies for the Post-COVID-19 Era. Clin. Exp. Allergy 2021, 51, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Komariah, M.; Maulana, S.; Platini, H.; Pahria, T. A Scoping Review of Telenursing’s Potential as a Nursing Care Delivery Model in Lung Cancer During the COVID-19 Pandemic. J. Multidiscip. Healthc. 2021, 14, 3083–3092. [Google Scholar] [CrossRef]
- Indraratna, P.; Tardo, D.; Yu, J.; Delbaere, K.; Brodie, M.; Lovell, N.; Ooi, S.-Y. Mobile Phone Technologies in the Management of Ischemic Heart Disease, Heart Failure, and Hypertension: Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2020, 8, e16695. [Google Scholar] [CrossRef]
- Cavalheiro, A.H.; Silva Cardoso, J.; Rocha, A.; Moreira, E.; Azevedo, L.F. Effectiveness of Tele-Rehabilitation Programs in Heart Failure: A Systematic Review and Meta-Analysis. Health Serv. Insights 2021, 14, 11786329211021668. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; Strickland, W.; Neelagaru, S.; Raval, N.; Krueger, S.; et al. Wireless Pulmonary Artery Haemodynamic Monitoring in Chronic Heart Failure: A Randomised Controlled Trial. Lancet 2011, 377, 658–666. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Okeke, O.C.; Boateng, J.S. Composite HPMC and Sodium Alginate Based Buccal Formulations for Nicotine Replacement Therapy. Int. J. Biol. Macromol. 2016, 91, 31–44. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, 898. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Bernocchi, P.; Vitacca, M.; La Rovere, M.T.; Volterrani, M.; Galli, T.; Baratti, D.; Paneroni, M.; Campolongo, G.; Sposato, B.; Scalvini, S. Home-Based Telerehabilitation in Older Patients with Chronic Obstructive Pulmonary Disease and Heart Failure: A Randomised Controlled Trial. Age Ageing 2018, 47, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Su, Y.; Hu, Z.; Sun, X.; Li, X.; Dolansky, M.A.; Qu, M.; Hu, X. Home-Based Telehealth Exercise Training Program in Chinese Patients with Heart Failure A Randomized Controlled Trial. Medicine 2018, 97, e12069. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Mierzyńska, A.; Banach, M.; Jaworska, I.; Pencina, M.; Kowalik, I.; Pluta, S.; Szalewska, D.; Opolski, G.; Zaręba, W.; et al. Quality of Life in Heart Failure Patients Undergoing Hybrid Comprehensive Telerehabilitation versus Usual Care—Results of the Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. Arch. Med. Sci. 2021, 17, 1599–1612. [Google Scholar] [CrossRef]
- Główczyńska, R.; Piotrowicz, E.; Szalewska, D.; Piotrowicz, R.; Kowalik, I.; Pencina, M.J.; Zaręba, W.; Banach, M.; Orzechowski, P.; Pluta, S.; et al. Effects of Hybrid Comprehensive Telerehabilitation on Cardiopulmonary Capacity in Heart Failure Patients Depending on Diabetes Mellitus: Subanalysis of the TELEREH-HF Randomized Clinical Trial. Cardiovasc. Diabetol. 2021, 20, 106. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Pencina, M.J.; Opolski, G.; Zarȩba, W.; Banach, M.; Kowalik, I.; Orzechowski, P.; Szalewska, D.; Pluta, S.; Główczyńska, R.; et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-Term Outcomes in Patients with Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 300–308. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Stepnowska, M.; Leszczyńska-Iwanicka, K.; Piotrowska, D.; Kowalska, M.; Tylka, J.; Piotrowski, W.; Piotrowicz, R. Quality of Life in Heart Failure Patients Undergoing Home-Based Telerehabilitation versus Outpatient Rehabilitation—A Randomized Controlled Study. Eur. J. Cardiovasc. Nurs. 2015, 14, 256–263. [Google Scholar] [CrossRef]
- Orzechowski, P.; Piotrowicz, R.; Zaręba, W.; Główczyńska, R.; Szalewska, D.; Pluta, S.; Irzmański, R.; Kalarus, Z.; Banach, M.; Opolski, G.; et al. Assessment of ECG during Hybrid Comprehensive Telerehabilitation in Heart Failure Patients—Subanalysis of the Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. Ann. Noninvasive Electrocardiol. 2021, 26, e12887. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Piotrowicz, R.; Opolski, G.; Pencina, M.; Banach, M.; Zaręba, W. Hybrid Comprehensive Telerehabilitation in Heart Failure Patients (TELEREH-HF): A Randomized, Multicenter, Prospective, Open-Label, Parallel Group Controlled Trial—Study Design and Description of the Intervention. Am. Heart J. 2019, 217, 148–158. [Google Scholar] [CrossRef]
- Hwang, R.; Bruning, J.; Morris, N.R.; Mandrusiak, A.; Russell, T. Home-Based Telerehabilitation Is Not Inferior to a Centre-Based Program in Patients with Chronic Heart Failure: A Randomised Trial. J. Physiother. 2017, 63, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Piotrowicz, E.; Piotrowski, W.; Piotrowicz, R. Positive Effects of the Reversion of Depression on the Sympathovagal Balance after Telerehabilitation in Heart Failure Patients. Ann. Noninvasive Electrocardiol. 2016, 21, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Zieliński, T.; Bodalski, R.; Rywik, T.; Dobraszkiewicz-Wasilewska, B.; Sobieszczańska-Małek, M.; Stepnowska, M.; Przybylski, A.; Browarek, A.; Szumowski, Ł.; et al. Home-Based Telemonitored Nordic Walking Training Is Well Accepted, Safe, Effective and Has High Adherence among Heart Failure Patients, Including Those with Cardiovascular Implantable Electronic Devices: A Randomised Controlled Study. Eur. J. Prev. Cardiol. 2015, 22, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Hwang, R.; Mandrusiak, A.; Morris, N.R.; Peters, R.; Korczyk, D.; Bruning, J.; Russell, T. Exploring Patient Experiences and Perspectives of a Heart Failure Telerehabilitation Program: A Mixed Methods Approach. Heart Lung J. Acute Crit. Care 2017, 46, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Baranowski, R.; Bilinska, M.; Stepnowska, M.; Piotrowska, M.; Wójcik, A.; Korewicki, J.; Chojnowska, L.; Malek, L.A.; Klopotowski, M.; et al. A New Model of Home-Based Telemonitored Cardiac Rehabilitation in Patients with Heart Failure: Effectiveness, Quality of Life, and Adherence. Eur. J. Heart Fail. 2010, 12, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Opasich, C.; Pinna, G.D.; Bobbio, M.; Sisti, M.; Demichelis, B.; Febo, O.; Forni, G.; Riccardi, R.; Riccardi, P.G.; Capomolla, S.; et al. Peak Exercise Oxygen Consumption in Chronic Heart Failure: Toward Efficient Use in the Individual Patient. J. Am. Coll. Cardiol. 1998, 31, 766–775. [Google Scholar] [CrossRef]
- Mancini, D.M.; Eisen, H.; Kussmaul, W.; Mull, R.; Edmunds, L.H., Jr.; Wilson, J.R. Value of Peak Exercise Oxygen Consumption for Optimal Timing of Cardiac Transplantation in Ambulatory Patients with Heart Failure. Circulation 1991, 83, 778–786. [Google Scholar] [CrossRef]
- Correction Piepoli, M.F.; Davos, C.; Francis, D.P.; Coats, A.J.S.; Belardinelli, R.; Purcaro, A.; Dubach, P.; Myers, J.; Giannuzzi, P.; Temporelli, P.L.; et al. Exercise Training Meta-Analysis of Trials in Patients with Chronic Heart Failure (ExTraMATCH). Br. Med. J. 2004, 328, 189–192. [Google Scholar] [CrossRef]
- Batalik, L.; Dosbaba, F.; Hartman, M.; Konecny, V.; Batalikova, K.; Spinar, J. Long-Term Exercise Effects after Cardiac Telerehabilitation in Patients with Coronary Artery Disease: 1-Year Follow-up Results of the Randomized Study. Eur. J. Phys. Rehabil. Med. 2021, 57, 807–814. [Google Scholar] [CrossRef]
- Batalik, L.; Pepera, G.; Papathanasiou, J.; Rutkowski, S.; Líška, D.; Batalikova, K.; Hartman, M.; Felšőci, M.; Dosbaba, F. Is the Training Intensity in Phase Two Cardiovascular Rehabilitation Different in Telehealth versus Outpatient Rehabilitation? J. Clin. Med. 2021, 10, 4069. [Google Scholar] [CrossRef]
- Stefanakis, M.; Batalik, L.; Antoniou, V.; Pepera, G. Safety of Home-Based Cardiac Rehabilitation: A Systematic Review. Heart Lung 2022, 55, 117–126. [Google Scholar] [CrossRef]
- Stefanakis, M.; Batalik, L.; Papathanasiou, J.; Dipla, L.; Antoniou, V.; Pepera, G. Exercise-Based Cardiac Rehabilitation Programs in the Era of COVID-19: A Critical Review. Rev. Cardiovasc. Med. 2021, 22, 1143–1155. [Google Scholar] [CrossRef] [PubMed]
- De Cristo, D.; Pinto Do Nascimento, N.; Dias, A.S.; Sachetti, A. Telerehabilitation for Cardiac Patients: Systematic Review. Int. J. Cardiovasc. Sci. 2018, 31, 443–450. [Google Scholar] [CrossRef]
- Babu, A.S.; Arena, R.; Ozemek, C.; Lavie, C.J. COVID-19: A Time for Alternate Models in Cardiac Rehabilitation to Take Centre Stage. Can. J. Cardiol. 2020, 36, 792. [Google Scholar] [CrossRef] [PubMed]
- Leochico, C.F.D.; Espiritu, A.I.; Ignacio, S.D.; Mojica, J.A.P. Challenges to the Emergence of Telerehabilitation in a Developing Country: A Systematic Review. Front. Neurol. 2020, 11, 1007. [Google Scholar] [CrossRef]
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine Practice: Review of the Current Ethical and Legal Challenges. Telemed. e-Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef]
- Battineni, G.; Nittari, G.; Sirignano, A.; Amenta, F. Are Telemedicine Systems Effective Healthcare Solutions during the COVID-19 Pandemic? J. Taibah Univ. Med. Sci. 2021, 16, 305–306. [Google Scholar] [CrossRef]
- Su, J.; Zhang, Y.; Ke, Q.Q.; Su, J.K.; Yang, Q.H. Mobilizing Artificial Intelligence to Cardiac Telerehabilitation. Rev. Cardiovasc. Med. 2022, 23, 45. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Location | Sample | |||
|---|---|---|---|---|---|---|
| Patients’ Diagnoses | Size | Gender (Male%) | Age (Year) | |||
| Główczyńska et al. (2021) [25] | RCT | Poland | stable HF with LVEF < 40% | 782 | n = 698 | IG: HTCR 65 ± 8.1 UC 63.4 ± 7.9 CG: HTCR 60.6 ± 11.7 UC 61.1 ± 11.2 |
| Piotrowicz et al. (2020) [24] | RCT | Poland | stable HF NYHA class I, II, or III and left LVEF ≤ 40% | 859 | 89.0 | IG: 62.2 ±10.9 CG; 62.1 ±10.2 |
| Orzechowski et al. (2021) [28] | RCT | Poland | stable HF NYHA class I, II, or III and left LVEF of 40% | 386 | 89.6 | 62 ± 11 |
| Piotrowicz et al. (2020) [26] | RCT | Poland | stable HF NYHA class I, II, or III and left LVEF ≤ 40% | 425 | 88.7 | 62.6 ± 10.8 |
| Piotrowicz et al. (2019) [29] | RCT | Poland | stable HF NYHA class I, II, or III and left LVEF ≤ 40% | 850 | N/I | N/I |
| Bernocchi et al. (2018) [22] | RCT | Italy | COPD and HF | 112 | 82.1 | 70 ± 9 |
| Peng et al. (2018) [23] | RCT | China | a primary diagnosis of chronic HF NYHA class I to III | 98 | 59.2 | 66.3 ± 10.5 |
| Hwang et al. (2017)-a [30] | RCT | Australia | chronic heart failure with a reduced or preserved ejection fraction | 53 | 75.0 | 67 ± 12 |
| Hwang et al. (2017)-b [33] | RCT | Australia | HF unspesificy | 17 | 88.0 | 69 ± 12 |
| Piotrowicz et al. (2016) [31] | RCT | Poland | HF unspesificy | 69 | n = 61 | IG 54.3 ± 10.38 CG 60.4 ± 11.9 |
| Piotrowicz et al. (2015)-a [32] | RCT | Poland | stable HFNYHA class II/III with LVEF < 40% | 131 | 85.0 | 56.4 ± 10.9 |
| Piotrowicz et al. (2015)-b [27] | RCT | Poland | stable HFNYHA class II/III with LVEF < 40% | 108 | n = 95 | IG: 54.4 ± 10.9 CG:62.1 ± 12.5 |
| Type of Telehealth | Model | Input | Process | Output |
|---|---|---|---|---|
| Hybrid cardiac telerehabilitation (HCT) [24,25,26,27,28,29,31,32,34] | Using a mobile phone for voice communication and TR set. A TR set (Pro Plus Company, Poland) consists of EHO mini device, blood pressure monitoring, and weighing equipment. | First, patients use their phones to answer questions on their current health, including fatigue, dyspnea, symptoms, body mass, and medications taken before starting an exercise session. Second, the EHO mini will record ECG data from three precordial leads and send it to the monitoring center through a mobile phone network. Each patient’s EHO mini device features preprogrammed training sessions (defined exercise duration, breaks, timing of ECG recording). The automated ECG registration is timed to the exercise training. The device indicates what needs to be done via sound and light signals. There are bleeps and light signals from color-emitting LEDs. Bleeps and green diode blinking means that the patient needs to move. “Stop exercise” is indicated by other bleeps and blinking of a red diode. The ECG recording starts automatically coinciding with peak exercise. | Prior to allowing the beginning of the training session, health workers will evaluate data from CIED remote monitoring. Patients are permitted to begin the training session if no contraindications are detected. | Exercise: The monitoring center evaluated the safety, efficacy, and accuracy of the program. By using HR data during exercise and patients’ subjective assessments of the Borg scale, experts could change the training workload or even stop the session if necessary. Psychological support: Telephone interaction was also employed for mental health. Education: All exercise training modalities (the Borg scale and how to run a TR set) were taught. Nutritional counseling, lipid management, smoking cessation, and psychosocial assistance were also included. All outcomes were assessed at baseline and after completing the 9-week program. Patients will be followed-up for a maximum of 24 months. |
| Home-based telerehabilitation program [22] | Telerehabilitation home-based program (Telerehab-HBP) using smartphone, oximeter, and portable one-lead ECG (Card Guard Scientific Survival Ltd., Rehovot, Israel). | With the cardiologist and pulmonologist directing the program, the nurses made a weekly structured phone call to each patient to collect information about disease status and symptoms, nutrition, lifestyle, and medications. Patients were given a pulse oximeter and a portable one-lead ECG to monitor vital signs in real time. The rehabilitation consisted of light and hard traning. Light training included 15–25 min on a mini-ergometer with no load, 30 min of callisthenic exercises three times a week, and two days of free walking. ‘Hard level’ included 30–45 min of mini-ergometer with total load (0–60 W), 30–40 min of muscle-strengthening exercises with 0.5 kg weights, and pedometer-based walking. Patients might call for any emergency conditions 24 h a day. | Patients were required to report every program’s daily performance and issues during the telephone appointment. The physiotherapist would provide changes in the number and intensity of training sessions every 4 months or when issues arose by assessing the Borg scale at the end of any training session. | General clinical condition: asthenia, muscle pain, and joint pain. Physical activity: duration of exercises and number of steps. Clinical parameters before and after training (blood pressure, heart rate, oxygen saturation, and Borg scale). Education: lifestyle changes and the importance of performing exercise. First follow-up was done 4 months after hospital discharge; 2nd follow-up was done 2 months later. Patients’ satisfaction was measured during the first follow-up. Other outcomes were assessed at both first and second follow-up. |
| Home-based telehealth exercise training progam [23] | An instant messaging service allows users to communicate online using text, audio, or video. The exercise training program used QQ and Wechat software to communicate and supervise. | Prior to the intervention, an instant messenger (QQ and Wechat) group was created for patients and researchers to communicate. Stage 1 (1–4 weeks) concentrated on endurance workouts, with three 20-min sessions each week. Walking was the most prevalent modality used in the first stage. Patients had 12 20-min exercise sessions three times per week. The second stage (5–8 weeks) included 5 30-min resistance and muscular strengthening sessions. The patients did endurance workouts before moving on to resistance. Walking, jogging, and calisthenics were used to train the muscles. The second stage included 20 30-min workout sessions five days a week. The participants could also contact cardiac nurses through phone or Wechat at any moment. Referral services were also provided if necessary. | During the activity training program, cardiac nurses called or texted to check on patients every week. Questions and responses were followed up with talks regarding the current situation and challenges. Physiotherapists were in charge of monitoring, assessing, and changing the training intensity as needed. The workout prescription prioritized exercise intensity. This intervention measured exercise intensity by target HR, which was determined using the HR reserve method. | Patients’ exercise intensity, evaluated by target HR. Target training HR equals 40–70% of HR reserve + resting HF. Participants were required to complete 3 surveys at discharge (as baseline), 2 months following discharge (post-test 1), and 6 months following discharge (post-test 2). |
| Home-based telerehabilitation [30,33] | Online video conferencing software | Exercise prescription was adjusted to each participant’s goals and reviewed continually by the treating physiotherapist. Participants could borrow a laptop computer, a mobile broadband device with 3G wireless internet, an automatic sphygmomanometer, a finger pulse oximeter, free weights, and resistance bands. In case of any questions or technical issues, participants could call for technical help by phone. Each participant was instructed to self-monitor and vocally report their blood pressure, heart rate, and oxygen saturation levels. Weight, blood sugar, peripheral edema, and general wellness were also measured if applicable. | The telerehabilitation program was provided to groups of up to four participants in their homes via a synchronous videoconferencing platform. | This 12-week heart failure rehabilitation program included 60 min of exercise at the treating hospital, twice a week. Session length was 40 min, including a 10-min warm-up, followed by a 10-min cool-down. The exercise intensity started at 9 (very mild) and progressively increased to 13 (slightly strenuous). The exercise prescription was adjusted to the participant’s goals and continually reviewed by the treating physiotherapist. Self-management, nutritional and physical activity counseling, psychological therapies, pharmaceuticals, and risk factor management were all covered by multidisciplinary healthcare. Participants were also given home workouts three times per week at the same intensity as the supervised sessions. Assessment were done at baseline, week 12 (1st follow-up), and week 24 (2nd follow up). |
| Study | Outcome | Intervention | Results | ||
|---|---|---|---|---|---|
| Feasibility | Efficacy | Safety | |||
| Główczyńska et al. (2021) [25] | Cardiopulmonary exercise capacity (using CPET) | Hybrid cardiac telerehabilitation | N/I | Patients in HCTR group were associated with longer exercise time. The differences in exercise time between HCTR and UC were 12.0 s (95% CI: 15.1–39.1; p = 0.666) in DM and 43.1 s (95% CI: 24.0–63.0 s; p < 0.001) in non-DM. HCTR group was also associated with lower ventilation at rest compared to UC. The differences were −0.34 L/min (95% CI: 1.60,−0.91 L/min; p = 0.892) in DM and 0.83 L/min (95% CI 0.06, 1.73 L/min; p = 0.082) in non-DM. In VE/VCO2 slope, a non-significant difference was found: 1.52 (95% CI; 1.55–4.59; p = 0.579) for DM vs. − 1.44 (95% CI −3.64–0.77; p = 0.336) for non-DM. | Both HCTR and UC are safe in DM and non-DM patients, as evidenced by lack of significant adverse effects experienced by patients. |
| Piotrowicz et al. (2020) [24] | QoL (SF-36) | Hybrid cardiac telerehabilitation | No patients were exluded or lost to follow-up during 9-week study period. | HCTR significantly improved overall QoL (p = 0.009). Greater improvement was observed in HCTR compared to UC group. QoL domain improvement in HCTR group: QoL—physical domain (p = 0.0003); QoL—physical functioning (p = 0.001); QoL—role functioning related to physical state (p = 0.003); QoL—bodily pain (p = 0.015). | N/I |
| Orzechowski et al. (2021) [28] | Safety measured by frequency of cardiac arrhythmias | Hybrid cardiac telerehabilitation | 12/425 patients were discontinued for non-medical reasons. | N/I | No patients experienced symptomatic arrhythmia requiring the discontinuation of telerehabilitation. Sinus rhythm was detected in 320 (83%), while persistent atrial fibrillation (AF) was present in 66 (17%) patients. Ventricular and atrial premature beats were the most frequently seen arrhythmias, occurring in 76.4% and 27.7% of patients, respectively. Non-sustained ventricular tachycardia (21 occurrences in 8 patients) and paroxysmal atrial fibrillation (6 episodes in 4 patients) were considered uncommon. |
| Piotrowicz et al. (2020) [26] | Quality of life (SF-36) and clinical outcome | Hybrid cardiac telerehabilitation | No patients were exluded or lost to follow-up during 9-week study period. | HCTR significantly improved patients’ quality of life (1.58 (95% CI, 0.74–2.42) vs. 0.00 (95% CI, 0.84 −0.84); p = 0.008) and peak oxygen consumption (0.95 vs. 0.00 mL/kg/min; p = 0.001). | The intervention group did not show improved survival rates (91.9 vs. 92.8 days, with a likelihood of 0.49 (95% CI, 0.46–0.53; p = 0.74)), mortality rates (12.5%, vs. 12.4% (HR 1.03 [95% CI, 0.70–1.51])), or hospitalization rates (HR 0.94 (95 percent CI, 0.79–1.13)). |
| Piotrowicz et al. (2019) [29] | Model (see Table 2) | Hybrid cardiac telerehabilitation | Not applicable | Not applicable | Not applicable |
| Bernocchi et al. (2018) [22] | Primary: Feasibility and efficacy (6MWD) Secondary: Dyspnea; physical activity; disability; QoL (MRC; PASE: Barthel; MLHFQ) | Home-based telerehabilitation | 93% participants performed designed activity at home. Patients’ satisfaction with the program was reportedly very high, with overall mean score 22.3/25. | After 4 months, patients in IG were able to walk further than they did at the beginning: the improvement in 6MWD in IG was 60 (22.2,97.8) m; meanwhile, CG showed no significant improvement (−15 (40.3,9.8)) m. The difference between two groups was significant. IG was associated with significant improvement in the PASE score (p = 0.0175), Barthel (p = 0.01), and MLHFQ score (p = 0.0175) compared to CG at 4 months. | No major side effects were recorded. The IG group was better than CG. Required 113.4 days for the media in IG to reach a hospital or die, compared to 104.7 in the CG (p = 0.048, log-rank test). Cumulative hospitalizations happened in 21 patients (IG) and 37 patients (CG). |
| Peng et al. (2018) [23] | QoL (MLHFQ); 6MWD; resting HR; HADS; LVEF; the NYHA classification | Home-based telehealth exercise training progam | 4 patients were lost to follow-up and 3 were omitted from the intervention. | Patients receiving home-based telehealth were associated with significant improvements in QoL, 6MWD, and resting HR. No significant improvements were observed regarding NYHA classification, LVEF, anxiety, and depression at follow-up. | No significant complications or adverse outcomes reported during the program. |
| Hwang et al. (2017)-a [30] | Primary: 6MWD Secondary: QoL (MLHFQ); patients’ statisfication; attendance rates; adverse events | Home-based telerehabilitation | IG had significantly higher attendance rates than CG, with a mean difference of 6 (95% CI: 2 to 9) sessions. | At Week 12, the IG had a 15 m (95% CI −28 to 59) advantage in the 6MWD (F(1,6) = 1.39; p = 0.24). At week 24, IG had a non-significant 2 m (95% CI −36 to 41) advantage compared to CG. Mean within-group QoL difference was 11 (95% CI: −19 to −3). | The number of adverse events was similar between groups. No patients died, had a heart attack, syncope, or fell during the workout period. Both groups reported modest adverse effects, including angina, diaphoresis, and palpitations. |
| Hwang et al. (2017)-b [33] | Experience and perspective | Home-based telerehabilitation | Participants described telerehabilitation program as easily accessible, safe, and structured. | Participants called for better audio quality and connectivity, as well as computer instruction for individuals who were new to computers. Most participants preferred a combination of face-to-face and online delivery. | N/I |
| Piotrowicz et al. (2016) [31] | Depression (BDI with cut-off point 20); LF/HF; physical capacity improvement | Hybrid cardiac telerehabilitation with Nordic walking training | All patients in intervention group completed telerehabilitation program. | Depression: IG (8.76 ± 6.73 to 6.70 ± 5.53; p = 0.0006) CG (11.57 ± 8.18 9.09 ± 7.34; p = 0.0490). Depressive symptoms were substantially reduced in both groups (TG, p = 0.0006; CG, p = 0.0490). LF/HF: IG (2.06 ± 1.14 to 1.19 ± 0.80; p < 0.0001) CG (2.01 ± 1.35 to 2.42 ± 1.39; p > 0.05). Between-group differences were significant (p = 0.0001). Peak VO2: IG (16.83 ± 3.72 to 19.14 ± 4.20 mL/kg per minute; p < 0.0001). Favorable results in CG were not observed. The differences between groups were significant (p < 0.0001). | N/I |
| Piotrowicz et al. (2015)-a [32] | Safety, efficacy, adherence, and acceptance Primary: VO2 peak Secondary: workload duration (t) in 6MWT; QoL (SF-36); safety; adherence and acceptance | Home-based telemonitored Nordic walking in HF patients with CIEDs (i.e., cardiac resynchronization therapy, implantable cardioverter–defibrillator) | All patients completed the program. The adherence was very high: 94.7% patients were adherent, while others were partially adherent. Moreover, 99% participants in IG reported that the device was very easy or easy to use, and 90% had no problems coordinating the exercise. | Nordic walking telerehabilitation training resulted in significant improvement in: VO2 peak (16.1 ± 4.0 vs. 18.4 ± 4.1 mL/kg/min), test duration (471 ± 141 vs. 577 ± 158 s), 6MWD (428 ± 93 vs. 480 ± 87 m), and QoL (79.0 ± 31.3 vs. 70.8 ± 30.3). The improvement differences between IG and CG were significant in ΔVO2 peak (Δ2.0 ± 2.4 vs. Δ−0.2 ± 2.1), Δtest duration (Δ108 ± 108 vs. Δ0.94 ± 109, and Δ6MWT (Δ53.8 ± 63.9 vs. Δ22.0 ± 68.7). | Patients felt safer during telemonitored training than self-exercise without supervision. No deaths, hospitalization, or additional CIED interventions were reported. |
| Piotrowicz et al. (2015)-b [27] | QoL (SF-36) | Hybrid cardiac telerehabilitation | 59/75 patients completed the program. | IG provided similar improvement in overall QoL score to CG group. IG (79.3 ± 25.6 to 70.5 ± 25.4, p = 0.007) vs. CG (81.6 ± 27.3 to 69.2 ± 26.4, p = 0.004). Significant improvement in IG: physical function (23.2 ± 11.32 to 21.60 ± 9.65, p = 0.049) mental health (8.05 ± 3.81 to 7.15 ± 4.03, p = 0.012) vitality (8.44 ± 3.36 to 7.25 ± 3.78, p = 0.001) Significant improvement in CG: physical function (25.39 ± 10.89 to 23.20 ± 10.71, p = 0.044) role limitation caused by physical problems (13.80 ± 7.46 to 11.39 ± 8.43, p = 0.034) bodily pain (2.74 ± 2.54 to 2.00 ± 2.07, p = 0.011) social function (2.22 ± 1.98 to 1.63 ± 1.54, p = 0.005) mental health (7.52 ± 4.51 to 5.89 ± 3.58, p = 0.009) vitality (7.94 ± 4.17 to 6.76 ± 3.17, p = 0.0197) | N/I |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maulana, S.; Trisyani, Y.; Mirwanti, R.; Amirah, S.; Kohar, K.; Priyatmoko Putri, A.I.; Novianti, E. The Potential of Cardiac Telerehabilitation as Delivery Rehabilitation Care Model in Heart Failure during COVID-19 and Transmissible Disease Outbreak: A Systematic Scoping Review of the Latest RCTs. Medicina 2022, 58, 1321. https://doi.org/10.3390/medicina58101321
Maulana S, Trisyani Y, Mirwanti R, Amirah S, Kohar K, Priyatmoko Putri AI, Novianti E. The Potential of Cardiac Telerehabilitation as Delivery Rehabilitation Care Model in Heart Failure during COVID-19 and Transmissible Disease Outbreak: A Systematic Scoping Review of the Latest RCTs. Medicina. 2022; 58(10):1321. https://doi.org/10.3390/medicina58101321
Chicago/Turabian StyleMaulana, Sidik, Yanny Trisyani, Ristina Mirwanti, Shakira Amirah, Kelvin Kohar, Aprilia Inggritika Priyatmoko Putri, and Evi Novianti. 2022. "The Potential of Cardiac Telerehabilitation as Delivery Rehabilitation Care Model in Heart Failure during COVID-19 and Transmissible Disease Outbreak: A Systematic Scoping Review of the Latest RCTs" Medicina 58, no. 10: 1321. https://doi.org/10.3390/medicina58101321