
Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19

 , , , , , ,
, , , , , ,  ,
, 
Abstract
:1. Introduction
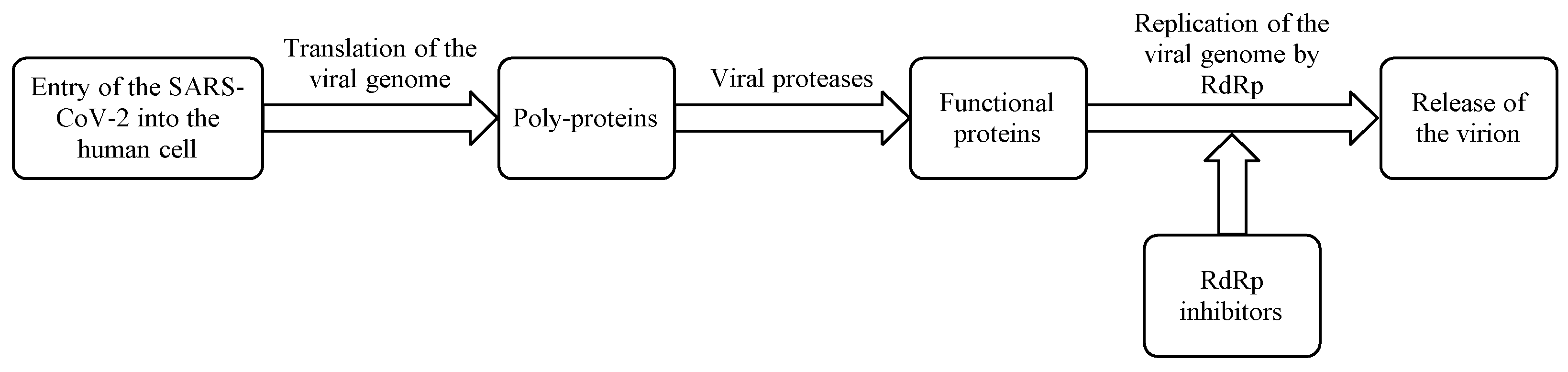
2. RNA-Dependent RNA-Polymerase (RdRp)
3. Molnupiravir
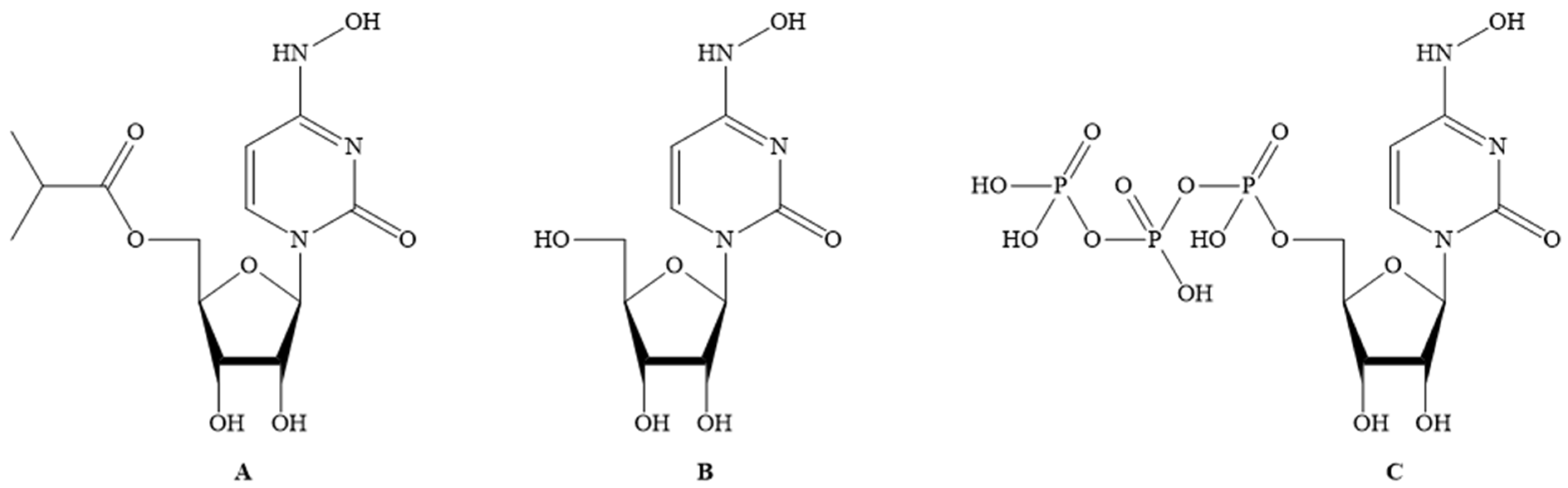
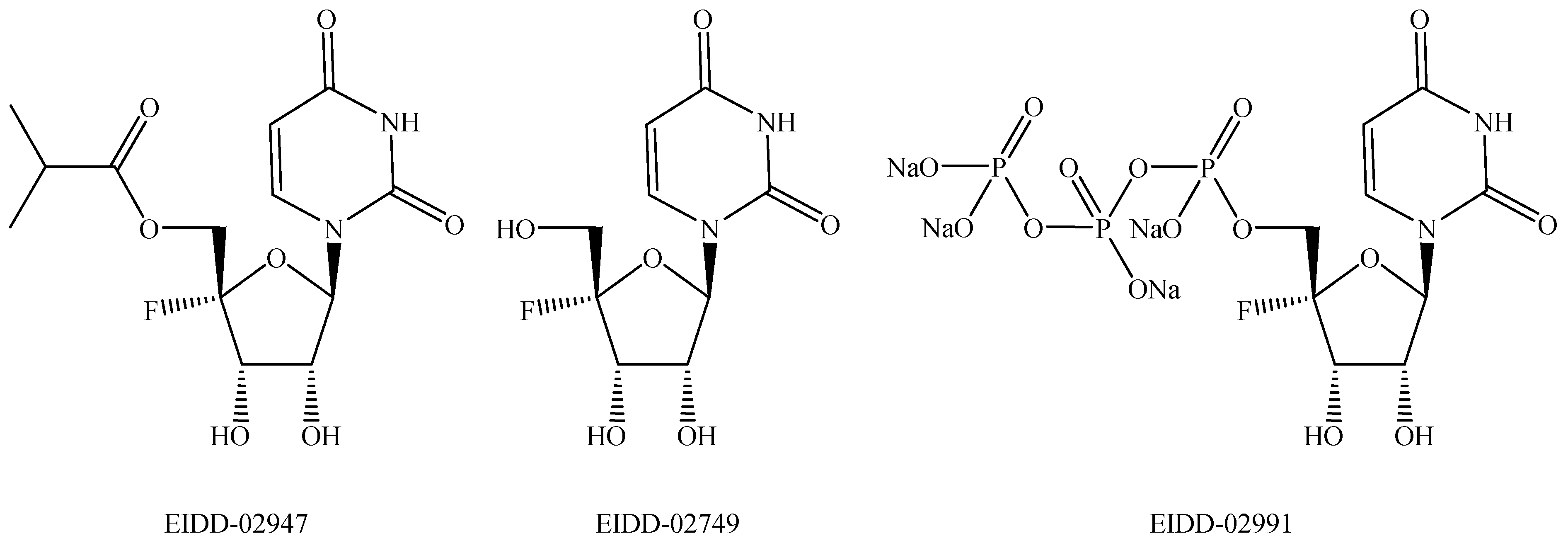
3.1. Mechanism of Action
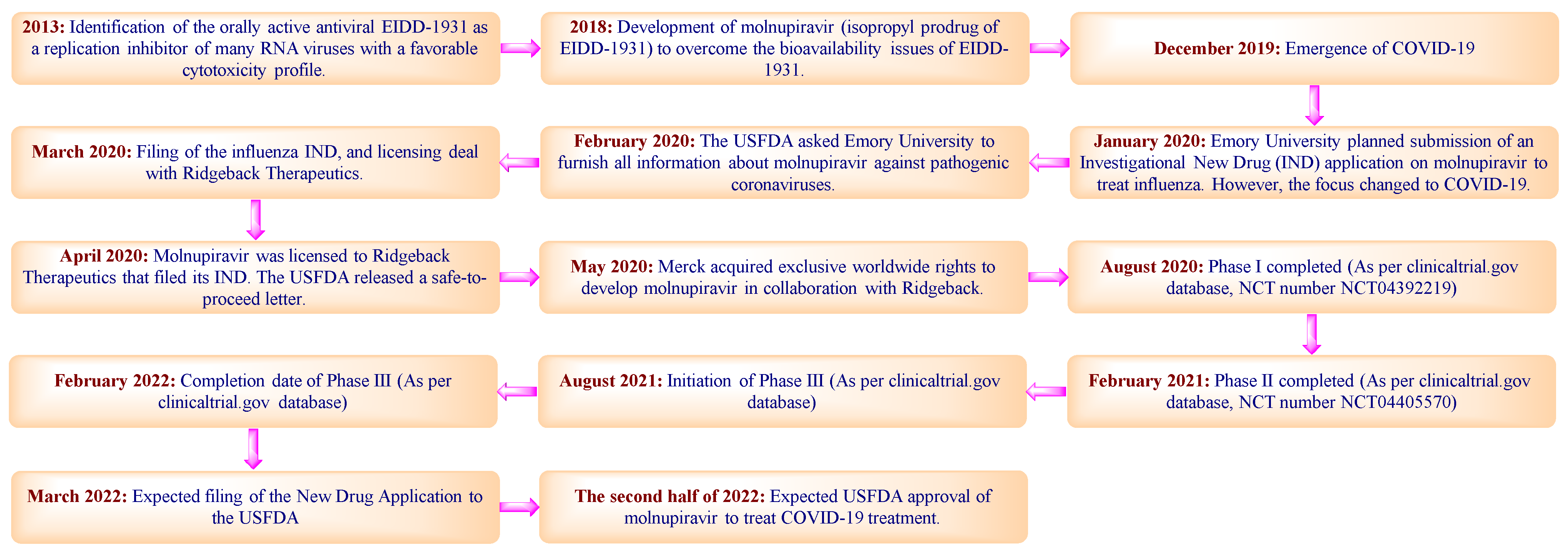
3.2. Discovery and Development
3.2.1. Pre-Clinical Studies
3.2.2. Clinical Studies
3.2.3. Current Clinical Trials
4. Patent Searching
5. Patent Analysis
5.1. Compound Patent
5.2. Polymorph Patent Application
5.3. Process Patent Applications
5.4. Patents Related to EIDD-1931 and EIDD-2061
5.5. Miscellaneous Patent Applications
6. Conclusions
7. Expert Opinion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rufaida, M.T.; Kedwai, I.; Ahsan, F.; Shamim, A.; Shariq, M.; Parveen, S. A dossier on COVID-19 chronicle. J. Basic Clin. Physiol. Pharmacol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://covid19.who.int (accessed on 16 August 2021).
- Couvreur, P.; Louvard, D. COVID-19 and drugs: Pathophysiology and therapeutic approaches. Comptes Rendus Biol. 2021, 344, 27–42. [Google Scholar] [PubMed]
- Falzone, L.; Gattuso, G.; Tsatsakis, A.; Spandidos, D.A.; Libra, M. Current and innovative methods for the diagnosis of COVID-19 infection (Review). Int. J. Mol. Med. 2021, 47, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Bestetti, R.B.; Furlan-Daniel, R.; Silva, V.M.R. Pharmacological treatment of patients with mild to moderate COVID-19: A comprehensive review. Int. J. Environ. Res. Public Health 2021, 18, 7212. [Google Scholar] [CrossRef]
- Das, K.; Pingali, M.S.; Paital, B.; Panda, F.; Pati, S.G.; Singh, A.; Varadwaj, P.K.; Samanta, S.K. A detailed review of the outbreak of COVID-19. Front. Biosci. (Landmark Ed.) 2021, 26, 149–170. [Google Scholar] [PubMed]
- Chen, B.; Liu, M.; Huang, C. Current diagnostic and therapeutic strategies for COVID-19. J. Pharm Analysis 2021, 11, 129–137. [Google Scholar] [CrossRef]
- Imran, M.; Alshrari, A.S.; Asdaq, S.M.B.; Abida. Trends in the development of remdesivir based inventions against COVID-19 and other disorders: A patent review. J. Infect. Public Health 2021, 14, 1075–1086. [Google Scholar] [CrossRef]
- Ghasemnejad-Berenji, M.; Pashapour, S. Favipiravir and COVID-19: A Simplified Summary. Drug Res. (Stuttg) 2021, 71, 166–170. [Google Scholar] [CrossRef]
- Christie, A.; Mbaeyi, S.A.; Walensky, R.P. CDC Interim Recommendations for Fully Vaccinated People: An Important First Step. JAMA 2021, 325, 1501–1502. [Google Scholar] [CrossRef]
- Mei, M.; Tan, X. Current Strategies of Antiviral Drug Discovery for COVID-19. Front. Mol. Biosci. 2021, 8, 671263. [Google Scholar] [CrossRef]
- Khan, S.A.; Al-Balushi, K. Combating COVID-19: The role of drug repurposing and medicinal plants. J. Infect. Public Health 2021, 14, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug repurposing: Progress.; challenges and recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef]
- Wang, Y.; Anirudhan, V.; Du, R.; Cui, Q.; Rong, L. RNA-dependent RNA polymerase of SARS-CoV-2 as a therapeutic target. J. Med. Virol. 2021, 93, 300–310. [Google Scholar] [CrossRef]
- Vicenti, I.; Zazzi, M.; Saladini, F. SARS-CoV-2 RNA-dependent RNA polymerase as a therapeutic target for COVID-19. Expert Opin. Ther. Pat. 2021, 31, 325–337. [Google Scholar] [CrossRef]
- Shu, B.; Gong, P. Structural basis of viral RNA-dependent RNA polymerase catalysis and translocation. Proc. Natl. Acad. Sci. USA 2016, 113, E4005-14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.X.; et al. Compassionate use of remdesivir for patients with severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomized, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental treatment with favipiravir for COVID-19: An open-label control study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Fischer, W.; Eron, J.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. Molnupiravir, an Oral Antiviral Treatment for COVID-19. medRxiv 2021. [Google Scholar] [CrossRef]
- Painter, W.P.; Holman, W.; Bush, J.A.; Almazedi, F.; Malik, H.; Eraut, N.C.J.E.; Morin, M.J.; Szewczyk, L.J.; Painter, G.R. Human Safety, Tolerability, and Pharmacokinetics of Molnupiravir, a Novel Broad-Spectrum Oral Antiviral Agent with Activity Against SARS-CoV-2. Antimicrob. Agents Chemother 2021, 65, e02428-20. [Google Scholar] [CrossRef]
- Toots, M.; Yoon, J.J.; Cox, R.M.; Hart, M.; Sticher, Z.M.; Makhsous, N.; Plesker, R.; Barrena, A.H.; Reddy, P.G.; Mitchell, D.G.; et al. Characterization of orally efficacious influenza drug with high resistance barrier in ferrets and human airway epithelia. Sci. Transl. Med. 2019, 11, eaax5866. [Google Scholar] [CrossRef]
- From the American Association of Neurological Surgeons (AANS); American Society of Neuroradiology (ASNR); Cardiovascular and Interventional Radiology Society of Europe (CIRSE); Canadian Interventional Radiology Association (CIRA); Congress of Neurological Surgeons (CNS); European Society of Minimally Invasive Neurological Therapy (ESMINT); European Society of Neuroradiology (ESNR); European Stroke Organization (ESO); Society for Cardiovascular Angiography and Interventions (SCAI); Society of Interventional Radiology (SIR); et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.J.; Toots, M.; Lee, S.; Lee, M.E.; Ludeke, B.; Luczo, J.M.; Ganti, K.; Cox, R.M.; Sticher, Z.M.; Edpuganti, V.; et al. Orally Efficacious Broad-Spectrum Ribonucleoside Analog Inhibitor of Influenza and Respiratory Syncytial Viruses. Antimicrob. Agents Chemother. 2018, 62, e00766-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Painter, G.R.; Natchus, M.G.; Cohen, O.; Holman, W.; Painter, W.P. Developing a direct acting, orally available antiviral agent in a pandemic: The evolution of molnupiravir as a potential treatment for COVID-19. Curr. Opin. Virol. 2021, 50, 17–22. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, L. Turning the Tide: Natural Products and Natural-Product-Inspired Chemicals as Potential Counters to SARS-CoV-2 Infection. Front. Pharmacol. 2020, 11, 1013. [Google Scholar] [CrossRef] [PubMed]
- Sheahan, T.P.; Sims, A.C.; Zhou, S.; Graham, R.L.; Pruijssers, A.J.; Agostini, M.L.; Leist, S.R.; Schäfer, A.; Dinnon, K.H., 3rd; Stevens, L.J.; et al. An orally bioavailable broad-spectrum antiviral inhibits SARS-CoV-2 in human airway epithelial cell cultures and multiple coronaviruses in mice. Sci. Transl. Med. 2020, 12, eabb5883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, R.M.; Wolf, J.D.; Plemper, R.K. Therapeutic MK-4482/EIDD-2801 Blocks SARS-CoV-2 Transmission in Ferrets. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Painter, G.R.; Bluemling, G.R.; Natchus, M.R.; Guthrie, D.B. N4-hydroxycytidine and Derivatives and Anti-viral Uses Related Thereto. U.S. Patent 2020276219A1, 3 September 2020. [Google Scholar]
- Xuchun, Z.; Yiping, Z.; Chenchen, F. Molnupiravir Crystal form A and Preparation Method Thereof. CN Patent 112778387A, 11 May 2021. [Google Scholar]
- Jian, C.; Changquan, Y.; Chenchen, F. Preparation Method of 4-oxime-5′-(2-methylpropionyl) Uridine. CN Patent 112552288A, 26 March 2021. [Google Scholar]
- Xuchun, Z.; Yiping, Z.; Chenchen, F. Preparation Method of Antiviral Drug Molnbupiravir. CN Patent 112608357A, 6 April 2021. [Google Scholar]
- Prasad, M.K.; Rao, M.A. Process for the Preparation of Molnupiravir. IN Patent 202141018775A, 7 May 2021. [Google Scholar]
- Akira, A.; Kisaburo, U.; Tatsuro, Y. Carbamoyloxycytidines. JP Patent 48000578A, 6 January 1973. [Google Scholar]
- Sledziewska, E.; Janion, C. Mutagenic Specificity of N4-hydroxycytidine. Mutat. Res. 1980, 70, 11–16. [Google Scholar] [CrossRef]
- Schinazi, R.F.; Amblard, F.; Cox, B.D.; Bassit, L.; Zhou, L.; Gavegnano, C. Antiviral Agents for Treating Zika and Dengue Virus Infections. WO Patent 2017165489A1, 28 September 2017. [Google Scholar]
- Painter, G.R.; Guthrie, D.B.; Bluemling, G.R.; Natchus, M.R. N4-hydroxycytidine and Derivatives and Anti-viral Uses Related Thereto. U.S. Patent 10874683B2, 29 December 2020. [Google Scholar]
- Liotta, D.C.; Painter, G.R.; Bluemling, G.R.; Rosa, A.D.L. Nucleotide and Nucleoside Therapeutics Compositions and Uses Related Thereto. WO Patent 2016145142A1, 15 September 2016. [Google Scholar]
- Bluemling, G.R.; Guthrie, D.B.; Natchus, M.G.; Painter, G.R. N4-hydroxycytidine and Derivatives and Anti-viral Uses Related Thereto. AU Patent 2015370004B2, 11 March 2021. [Google Scholar]
- Liotta, D.C.; Painter, G.R.; Bluemling, G.R.; Rosa, A.D.L. Nucleotide and Nucleoside Therapeutic Compositions and Uses Related Thereto. U.S. Patent 10149859B2, 11 December 2018. [Google Scholar]
- Loakes, D.; Brown, D.M.; Negishi, K.; Moriyama, K.; Balzarini, J. Inhibition of Viruses. U.S. Patent 7049303B2, 23 May 2006. [Google Scholar]
- Painter, G.R.; Perryman, D.; Bluemling, G.R. 4′-halogen Containing Nucleotide and Nucleoside Therapeutic Compositions and Uses Related Thereto. WO Patent 2019173602A1, 12 September 2019. [Google Scholar]
- Painter, G.R.; Perryman, D.; Bluemling, G.R. 4′-halogen Containing Nucleotide and Nucleoside Therapeutic Compositions and Uses Related Thereto. WO Patent 2021137913A2, 8 July 2021. [Google Scholar]
- Nandi, I.; Mukherjee, T.; Kumar, D.; Jain, A.; Soni, P.; Mistry, G.N.; Jaiswal, N. Transmucosal Pharmaceutical Compositions of Antiviral Drugs. IN Patent 202114023358, 18 June 2021. [Google Scholar]
- Lederman, S. Anti-cd154 Antibodies and Uses Thereof. WO Patent 2021001458A1, 7 January 2021. [Google Scholar]
- Lederman, S.; Daugherty, B. Modified Tff2 Polypeptides. WO Patent 2021038296A2, 4 March 2021. [Google Scholar]
- Li, S.; Yuan, L. Substituted N4-hydroxycytidine Derivatives and Prodrugs Thereof for Use in Anti-novel Coronavirus Therapy. CN Patent 111548384A, 27 April 2021. [Google Scholar]
- Qingyan, B.O.; Yuyan, J.I.N.; Tyagi, G.; Zhu, Y. Method of Treating Virus Infection Using a tlr7 Agonist. WO Patent 2021130195A1, 1 July 2021. [Google Scholar]
- Yuanchao, X.; Gengfu, X.; Yang, H.; Lei, Z.; Hualiang, J.; Jingshan, S. Application of Nucleoside Analogue or Combination Preparation Containing Nucleoside Analogue in Resisting Virus. CN Patent 112778310A, 11 May 2021. [Google Scholar]
- Schinazi, R.F.; Zandi, K.; Amblard, F. Peptidomimetics for the Treatment of Coronavirus and Picornavirus Infections. U.S. Patent 2021008150A1, 14 January 2021. [Google Scholar]
- Cho, A.; Link, J.O.; Xu, J. 2-Imino-5-Oxo-Imidazolidine Inhibitors of HIV Protease. WO Patent 2020214716A1, 22 October 2020. [Google Scholar]
- Peyman, G.A. Method of Treating, Reducing, or Alleviating a Medical Condition in A Patient. U.S. Patent 20210228619A1, 29 July 2021. [Google Scholar]
- Cihlar, T.; Osinusi, A.; Porter, D.L. Methods for Treating Sars Cov-2 Infections. WO Patent 2021154687A1, 5 August 2021. [Google Scholar]
- Chaudhuri, R.K.; Randhawa, M. Multi-Targeted Compositions for Mitigating Acute Respiratory Distress Syndrome. U.S. Patent 20210236529A1, 5 August 2021. [Google Scholar]
- Jordan, P.C.; Stevens, S.K.; Deval, J. Nucleosides for the treatment of respiratory RNA virus infections. Antivir. Chem. Chemother. 2018, 26, 2040206618764483. [Google Scholar] [CrossRef]
- Kabinger, F.; Stiller, C.; Schmitzová, J.; Dienemann, C.; Kokic, G.; Hillen, H.S.; Höbartner, C.; Cramer, P. Mechanism of molnupiravir-induced SARS-CoV-2 mutagenesis. Nat. Struct. Mol. Biol. 2021. [Google Scholar] [CrossRef]
- Zhou, S.; Hill, C.S.; Sarkar, S.; Tse, L.V.; Woodburn, B.M.D.; Schinazi, R.F.; Sheahan, T.P.; Baric, R.S.; Heise, M.T.; Swanstrom, R. β-d-N4-hydroxycytidine Inhibits SARS-CoV-2 Through Lethal Mutagenesis But Is Also Mutagenic To Mammalian Cells. J. Infect. Dis. 2021, 224, 415–419. [Google Scholar] [CrossRef]
- Hiremath, C.N. Abbreviated Profile of Drugs (APOD): Modeling drug safety profiles to prioritize investigational COVID-19 treatments. Heliyon 2021, 7, e07666. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Asdaq, S.M.B.; Khan, S.A.; Unnikrishnan, M.D.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.; AlMotairi, M.; et al. Innovations and Patent Trends in the Development of USFDA Approved Protein Kinase Inhibitors in the Last Two Decades. Pharmaceuticals 2021, 14, 710. [Google Scholar] [CrossRef]
- Paymode, D.J.; Vasudevan, N.; Ahmad, S.; Kadam, A.L.; Cardoso, F.S.P.; Burns, J.M.; Cook, D.W.; Stringham, R.W.; Snead, D.R. Toward a practical, two-step process for molnupiravir: Direct hydroxamination of cytidine followed by selective esterification. Org. Process. Res. Dev. 2021. [Google Scholar] [CrossRef]
- Hughes, D.T. Quest for a cure: Potential small-molecule treatments for COVID-19, Part 2. Org. Process. Res. Dev. 2021, 25, 1089–1111. [Google Scholar] [CrossRef]
- Datla, A.; Nagre, P.; Tamore, J.; Prabhu, M.S.; Trivikram, S.; Kadam, S.V.; Degaonkar, G.S.; Muralidharan, K.; Rupraj, N. Scalable Two Step Synthesis of Molnupiravir. IN Patent 202121014827A, 20 August 2021. [Google Scholar]
- Datla, A.; Nagre, P.; Tamore, J.; Prabhu, M.S.; Trivikram, S. Chemo-Enzymatic Process for Synthesis of Molnupiravir. IN Patent 202121005152A, 20 August 2021. [Google Scholar]
- Reddy, D.R.S.; Reddy, P.S.; Rao, G.V.G. Improved Process for Molnupiravir. IN Patent 202141011933A, 23 July 2021. [Google Scholar]
- Schooley, R.T.; Carlin, A.F.; Beadle, J.R.; Valiaeva, N.; Zhang, X.Q.; Clark, A.E.; McMillan, R.E.; Leibel, S.L.; McVicar, R.N.; Xie, J.; et al. Rethinking remdesivir: Synthesis, antiviral activity and pharmacokinetics of oral lipid prodrugs. Antimicrob. Agents Chemother. 2021, AAC0115521. [Google Scholar] [CrossRef]
- Available online: https://www.merck.com/news/merck-announces-supply-agreement-with-u-s-government-for-molnupiravir-an-investigational-oral-antiviral-candidate-for-treatment-of-mild-to-moderate-covid-19/ (accessed on 12 August 2021).
- Anonymous. An EUA for Bamlanivimab-A Monoclonal Antibody for COVID-19. JAMA 2021, 325, 880–881. [Google Scholar] [CrossRef]
- Pavan, M.; Bolcato, G.; Bassani, D.; Sturlese, M.; Moro, S. Supervised Molecular Dynamics (SuMD) Insights into the mechanism of action of SARS-CoV-2 main protease inhibitor PF-07321332. J. Enzyme Inhib. Med. Chem. 2021, 36, 1646–1650. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug’s Name | Dosage Forms (Route/Dose) | Indications (Marketing Status) | Countries |
|---|---|---|---|
| Remdesivir (Veklury®) | Solution/Powder (Intravenous/200 mg loading dose, followed by 100 mg once daily for 5 to 10 days for adults) | COVID-19 patients of ≥12 years requiring hospitalization (Prescription) | Approved in >50 countries including USA, KSA, UAE and European Union |
| Favipiravir (FabiFlu®) | Film-coated tablet (Oral/1800 mg/dose twice a day on the first day; followed by 800 mg/dose twice a day for 7–10 days for adults) | COVID-19 (Prescription) | Approved in many countries, including China, India, Russia and Japan |
| Type of Study | Total Participants | Dose | Pharmacokinetic Data |
|---|---|---|---|
| Interventional, phase 1, randomized, double-blind, placebo-controlled study | 130 | (i) A total of 64 subjects received a single oral dose of 50 to 1600 mg molnupiravir or placebo in the single-ascending-dose part. | Mean Cmax up to 13.2 ng/mL and median tmax 0.25 and 0.75 h for doses in between 600–1600 mg. Excretion in urine (0.002%) for >800 mg dose. Geometric mean terminal elimination half-lives (t1/2) = 0.91–1.29 h postdose of drug up to 800 mg dose. Median t1/2 for 1200 and 1600 mg doses = 1.75 and 1.50 h |
| (ii) A total of 55 subjects received twice-daily (BID) doses of 50 to 800 mg molnupiravir or placebo for 5.5 days in the multiple-ascending-dose part. | Median tmax in all dose cohorts of between 1.00 and 1.75 h postdose across both Days 1 and 6. At the 800-mg BID dose level, the mean t1/2 = 7.08 h AUCτ = 0.938–1.16; Cmax= 0.843–1.10 at all dose levels | ||
| (iii) A total of 10 subjects received a single dose of 200 mg in the fed state followed by a single dose of 200 mg molnupiravir in the fasted state after a washout period of 14 days, or vice versa. | Mean Cmax—approximately 36% lower in the fed state compared to the fasted state AUCinf—similar for both fed and fasted states Mean t1/2 in fed and fasted treatments = 1.09 and 0.977 h | ||
| (iv) One subject in the multiple-ascending-dose part received 800 mg molnupiravir BID for three days. | It was discontinued by the investigators. |
| Sponsor (Status) | Phase (Number Enrolled) (Interventions) | NCT Number (Other IDs) | Start Date (SD)/Completion Date (CD)/Last Update (LU) |
|---|---|---|---|
| Merck Sharp & Dohme Corp. (Active, not recruiting) | 2/3 (304) (Molnupiravir/Placebo) | NCT04575584 (4482-001, 2020-003367-26, MK-4482-001, PHRR201210-003189, jRCT2031200404) | SD: 19 October 2020 CD: 10 August 2021 LU: 7 May 2021 |
| Merck Sharp & Dohme Corp.(Recruiting) | 2/3 (1850) (Molnupiravir/Placebo) | NCT04575597 (4482-002, 2020-003368-24, MK-4482-002, PHRR201209-003186, RCT2031210148) | SD: 19 October 2020 CD: 19 April 2022 LU: 5 August 2021 |
| Merck Sharp & Dohme Corp. (Not yet recruiting) | 3 (1332) (Molnupiravir/Placebo) | NCT04939428 (4482-013, 2021-000904-39, MK-4482-013) | SD: 16 August 2021 CD: 3 April 2022 LU: 4 August 2021 |
| Ridgeback Biotherapeutics (Recruiting) | 2 (96) (EIDD-2801/Placebo) | NCT04405739 (EIDD-2801-2004) | SD: 16 June 2020 CD: 8 December 2021 LU: 20 May 2021 |
| Ridgeback Biotherapeutics (Completed) | 1 (130) (EIDD-2801/Placebo) | NCT04392219 (EIDD-2801-1001, 2020-001407-17) | SD: 10 April 2020 CD: 11 August 2020 LU: 19 July 2021 |
| Ridgeback Biotherapeutics (Completed) | 2 (204) (EIDD-2801/Placebo) | NCT04405570 (EIDD-2801-2003) | SD: 16 June 2020 CD: 21 February 2021 LU: 23 February 2021 |
| University of Liverpool (Recruiting) | 1/2 (600) (EIDD-2801/Nitazoxanide/VIR-7832/VIR-7831/Placebo) | NCT04746183 (UoL001542) | SD: 3 July 2020 CD: 30 April 2022 LU: 20 May 2021 |
| Patent/Application Number (Priority Number and Priority Date) (Application Number and Application Date) | Assignee (Equivalent Publications on 12 September 2021) | International Patent Classification | Status (Database) |
|---|---|---|---|
| US2020276219A1 (US201762595907P, 7 December 2017; US2018064503W, 7 December 2018; US201816755779A, 7 December 2018; US201862626998P, 6 February 2018; US201862760434P, 13 November 2018) (US201816755779A, 7 December 2018) | Emory University (AU2018378832B2, BR112020010581A2, CA3082191A1, CN111372592A, EP3706762A1, GB2581936B, JP6804790B1, KR102248165B1, PH12020550607A1, SG11202004403QA, WO2019113462A1) | A61K31/7068; A61P31/12 | Notice of Allowance Mailed as per USPTO (New patent number will be assigned soon) |
| CN112778387A (CN202110055824A, 15 January 2021) (CN202110055824A, 15 January 2021) | Hangzhou Kechao Biotechnology Co., Ltd. (None) | C07H1/00, C07H19/067 | Request for examination filed (Espacenet) |
| CN112552288A (CN202110188342A, 19 February 2021) (CN202110188342A, 19 February 2021) | Nanjing Huaguan Biotechnology Co., Ltd. (None) | C07D405/04 | Request for examination filed (Espacenet) |
| CN112608357A (CN202011515642A, 21 December 2020) (CN202011515642A, 21 December2020) | Hangzhou Kechao Biotechnology Co., Ltd. (None) | C07H1/00, C07H19/067, C12P17/16 | Request for examination filed (Espacenet) |
| IN202141018775A (IN2021-41018775, 23 April 2021) (IN2021-41018775, 23 April 2021) | Divi’s Laboratories Ltd. (None) | C07H0001000000, A61P0031220000, C07D0277640000, C07D0207340000, C07D0317280000 | Under Examination (Indian Patent Office) |
| JP48000578A (JP 1971-36614, 28 May 1971) | Mitsui Toatsu Chemicals Company Limited (None) | No information in Sci-finder | Expired (Based on the filing date mentioned on Sci-finder) |
| WO2017165489A1 (US201662312225P, 23 March 2016) (US2017023537W, 22 March 2017) | Emory University (None) | A61K31/4706, A61K31/635, A61P31/14 | No entry in any national phase (Espacenet) |
| US10874683B2 (US201662306163P, 10 March 2016; US2017021759W, 10 March 2017; US201716083177A, 10 March 2017) (US201716083177A, 10 March 2017) | Emory University (WO2017156380A1) | A61K31/7068, A61P31/14, A01N43/04, A61K31/70, C07H19/067, C07H19/10, A61K9/00 | Patented case (USPTO) |
| WO2016145142A1 (US201562130942P, 10 March 2015) (US2016021688W, 10 March 2016) | Emory University (None) | A61K31/7068, A61K31/7072, C07H19/10 | No entry in any national phase (Espacenet) |
| AU2015370004B2 (US201462096915P, 26 December 2014; US2015066144W, 16 December 2015; US201562201140P, 5 August 2015) (AU2015370004A, 16 December 2015) | Emory University (BR112017013858A2, CA2972259A1, CN107427529A, EA201791460A1, EP3236972A1, IL252997A, JP2018500354A, KR20170123308A, SG11201705069YA, US2019022116A1, US2021060050A1, WO2016106050A1) | A61K31/7068; A61P31/18; A61P35/00; C07H19/067 | Granted patent (Espacenet) |
| US10149859B2 (US201361876473P, 11 September 2013; US2014054930W, 10 September 2014; US201414917681A, 10 September 2014; US201461923317P, 3 January 2014; US201461986577P, 30 April 2014) (US201414917681A, 10 September 2014) | Emory University (EP3043803A1; JP6762873B2; TW201542581A; UY35732A; WO2015038596A1) | A61K31/7068, A61K45/06, A61K9/127, C07H19/10, C07H19/06 | Patented case (USPTO) |
| US7049303B2 (GB0126701A, 7 November 2001; US20700502A, 30 July 2002) (US20700502A, 30 July 2002) | Medical Research Council (AU2002337388A1; EP1441744A2; JP2005507944A; WO03039450A2) | A01N43/90, A61K31/519, A61K31/52, A61K31/675, A61K31/7068, A61K31/7076, A61P31/14, C07H19/067, C07H19/16, C07H19/167, A61K31/70 | Patent Expired Due to NonPayment of Maintenance Fees (USPTO) |
| WO2019173602A1 (US201862639725P, 7 March 2018) (US2019021168W, 7 March 2019) | Emory University (AU2019231725A1, BR112020018209A2, CA3093222A1, CN112074506A, EP3762372A1, GB2589205A, KR20200140274A, PH12020551404A1, SG11202008527WA) | A61K31/505, C07D239/10, C07D307/12, C07D405/04 | National phase entry in AU, BR, CA, CN, EP, GB, KR, PH and SG (Espacenet) |
| WO2021137913A2 (US201962912165P, 8 October 2019) (US2020054857W, 8 October 2020) | Emory University (None) | C07H19/16; | No entry in any national phase (Espacenet) |
| IN202114023358 (IN202011038103, 3 September 2020) (IN202114023358, 25 May 2021) | Jubilant Generics Limited (None) | A61K0009200000, A61K0009000000, A61K0009480000, C07D0401120000, A61K0009160000 | Under Examination (Indian Patent Office) |
| IN202121014827A (IN202121014827, 31 March 2021) | Fermenta Biotech Limited (None) | G06F021-62, C07C051-367, C07C209-08, H04L029-06, C07C227-02 | Publication (Indian Patent Office) |
| IN202121005152A (IN202121005152, 6 February 2021) | Fermenta Biotech Limited (None) | C07C067-327, C07C037-20, C07D319-06, C12P041-00, C40B050-14 | Publication (Indian Patent Office) |
| IN202141011933A (IN202141011933, 20 March 2021) | Optimus Drugs Private Limited (None) | C12N007-00, C01B021-02, C07K016-46, C07K014-755, B01J037-30 | Publication (Indian Patent Office) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imran, M.; Kumar Arora, M.; Asdaq, S.M.B.; Khan, S.A.; Alaqel, S.I.; Alshammari, M.K.; Alshehri, M.M.; Alshrari, A.S.; Mateq Ali, A.; Al-shammeri, A.M.; et al. Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19. Molecules 2021, 26, 5795. https://doi.org/10.3390/molecules26195795
Imran M, Kumar Arora M, Asdaq SMB, Khan SA, Alaqel SI, Alshammari MK, Alshehri MM, Alshrari AS, Mateq Ali A, Al-shammeri AM, et al. Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19. Molecules. 2021; 26(19):5795. https://doi.org/10.3390/molecules26195795
Chicago/Turabian StyleImran, Mohd., Mandeep Kumar Arora, Syed Mohammed Basheeruddin Asdaq, Shah Alam Khan, Saleh I. Alaqel, Mohammed Kanan Alshammari, Mohammed M. Alshehri, Ahmed Subeh Alshrari, Alreshidi Mateq Ali, Ahmed Muteb Al-shammeri, and et al. 2021. "Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19" Molecules 26, no. 19: 5795. https://doi.org/10.3390/molecules26195795