
How German and Italian Laypeople Reason about Distributive Shortages during COVID-19
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Testing Procedure
2.3. Statistical Analyses
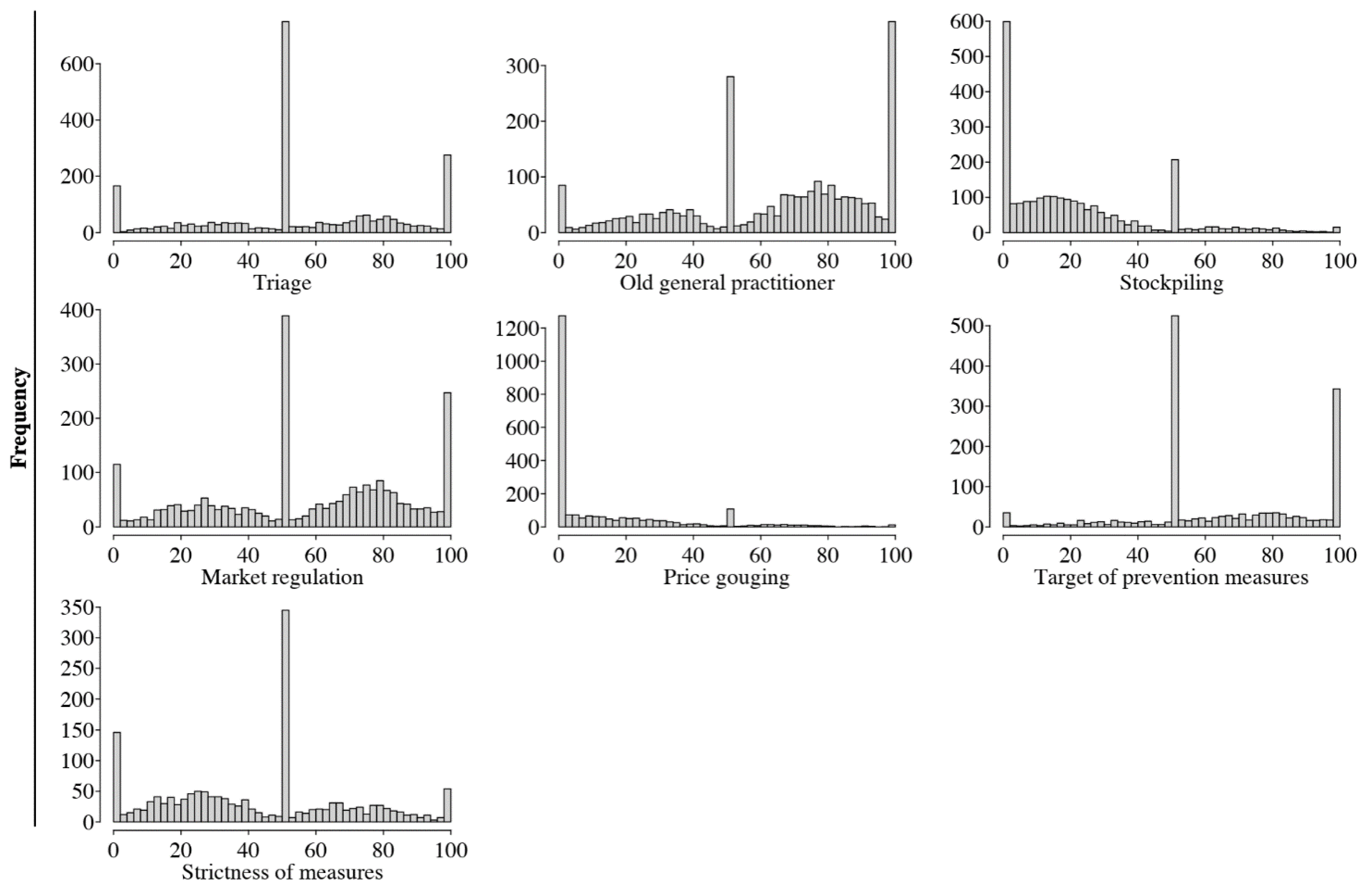
3. Results
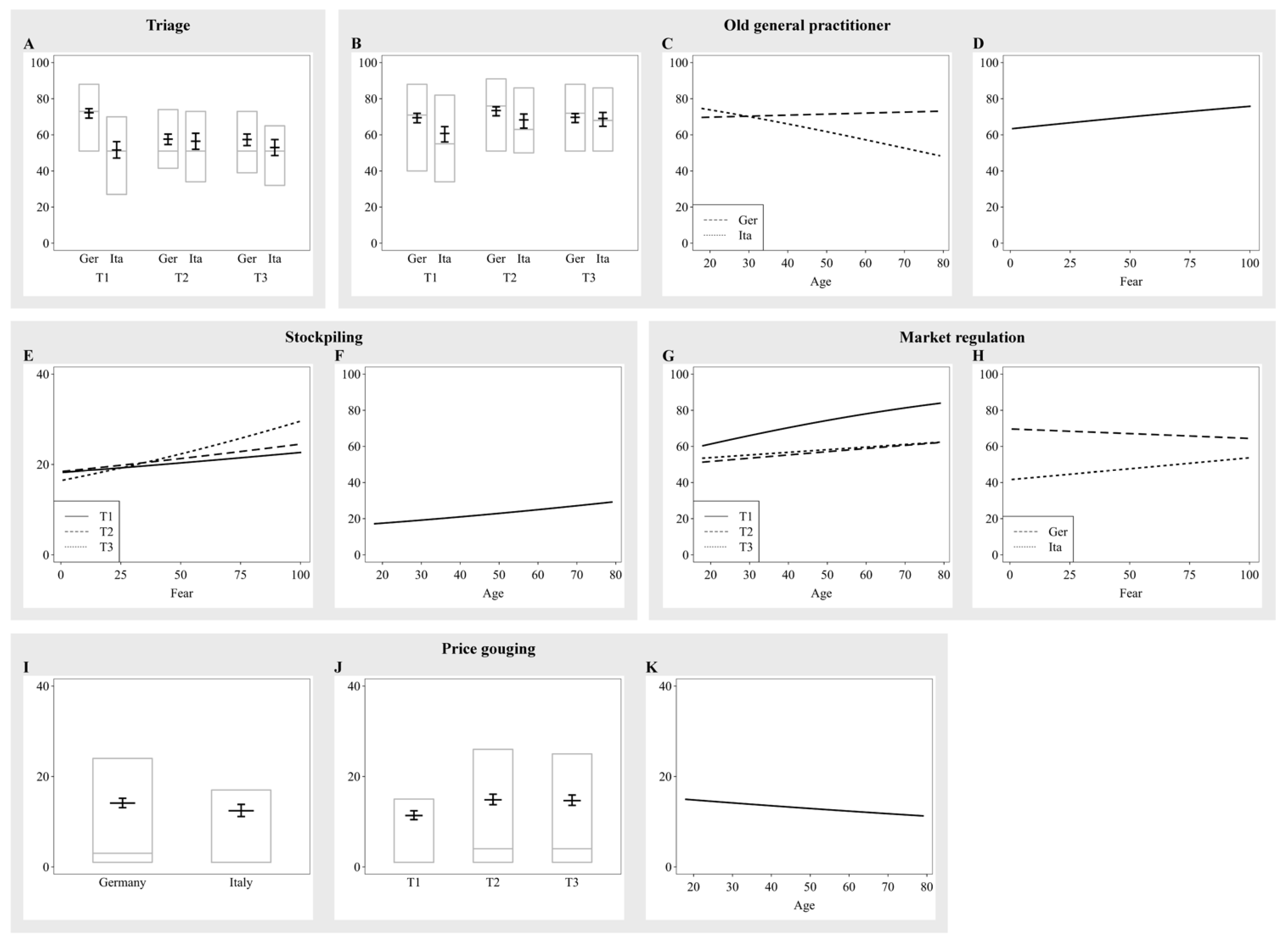
3.1. Triage
3.2. Old General Practitioner Dilemma
3.3. Stockpiling
3.4. Market Regulation
3.5. Price Gouging
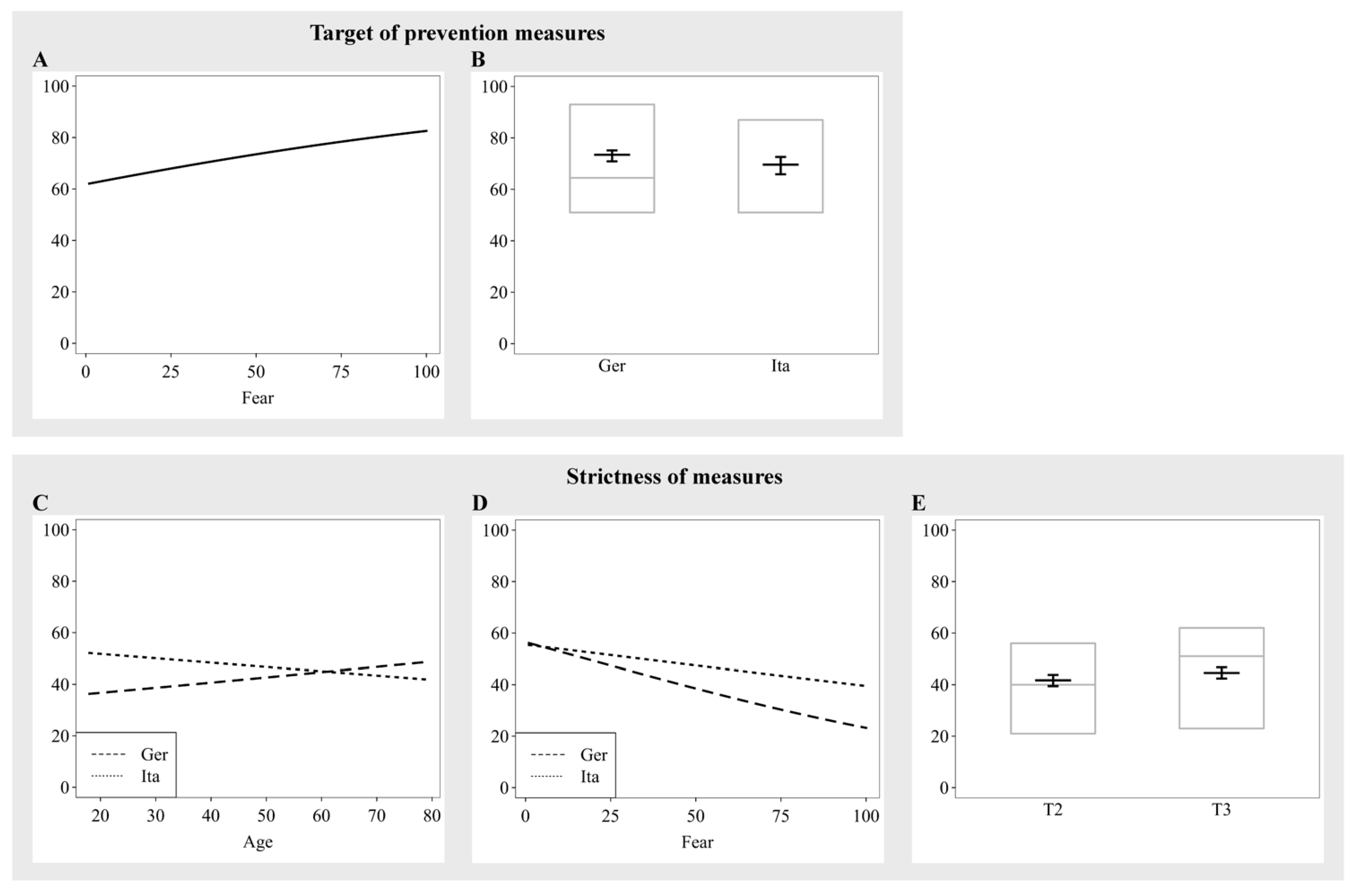
3.6. Target of Prevention Measures
3.7. Strictness of Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 3 March 2021).
- Karabag, S.F. An Unprecedented Global Crisis! The Global, Regional, National, Political, Economic and Commercial Impact of the Coronavirus Pandemic. J. Appl. Econ. Bus. Res. JAEBR 2020, 10, 1–6. [Google Scholar]
- Navarrete, C.D.; McDonald, M.M.; Mott, M.L.; Asher, B. Virtual Morality: Emotion and Action in a Simulated Three-Dimensional “Trolley Problem”. Emotion 2012, 12, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Francis, K.B.; Howard, C.; Howard, I.S.; Gummerum, M.; Ganis, G.; Anderson, G.; Terbeck, S. Virtual Morality: Transitioning from Moral Judgment to Moral Action? PLoS ONE 2016, 11, e0164374. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Borges do Nascimento, I.J.; Cacic, N.; Abdulazeem, H.M.; von Groote, T.C.; Jayarajah, U.; Weerasekara, I.; Esfahani, M.A.; Civile, V.T.; Marusic, A.; Jeroncic, A.; et al. Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis. J. Clin. Med. 2020, 9, 941. [Google Scholar] [CrossRef]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What Next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Boccia, S.; Ricciardi, W.; Ioannidis, J.P.A. What Other Countries Can Learn from Italy During the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 927–928. [Google Scholar] [CrossRef]
- OECD. Health at a Glance; OECD: Paris, France, 2021. [Google Scholar] [CrossRef]
- Waldmann, M.R.; Nagel, J.; Wiegmann, A. Moral Judgment. In The Oxford Handbook of Thinking and Reasoning; Holyoak, K.J., Morrison, R.G., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 274–299. [Google Scholar] [CrossRef]
- Bauman, C.W.; Mcgraw, A.P.; Bartels, D.M.; Warren, C. Revisiting External Validity: Concerns about Trolley Problems and Other Sacrificial Dilemmas in Moral Psychology. Soc. Pers. Psychol. Compass. 2014, 8, 536–554. [Google Scholar] [CrossRef]
- Körner, A.; Joffe, S.; Deutsch, R. When Skeptical, Stick with the Norm: Low Dilemma Plausibility Increases Deontological Moral Judgments. J. Exp. Soc. Psychol. 2019, 84, 103834. [Google Scholar] [CrossRef]
- Kamm, F.M. Non-Consequentialism, the Person as an End-in-Itself, and the Significance of Status. Philos. Public Aff. 1992, 21, 354–389. [Google Scholar]
- Cohen, D.J.; Ahn, M. A Subjective Utilitarian Theory of Moral Judgment. J. Exp. Psychol. Gen. 2016, 145, 1359–1381. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, N.; Waldmann, M.R. How to Weigh Lives. A Computational Model of Moral Judgment in Multiple-Outcome Structures. Cognition 2022, 218, 104910. [Google Scholar] [CrossRef] [PubMed]
- Mikhail, J. Elements of Moral Cognition: Rawls’ Linguistic Analogy and the Cognitive Science of Moral and Legal Judgment; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar] [CrossRef]
- Savulescu, J.; Persson, I.; Wilkinson, D. Utilitarianism and the Pandemic. Bioethics 2020, 34, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Colì, E.; Norcia, M.; Bruzzone, A. What Do Italians Think about Coronavirus? An Exploratory Study on Social Representations. Pap. Soc. Represent. 2020, 29, 1–29. [Google Scholar]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the Covid-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Health Res. 2020, 17, 3165. [Google Scholar] [CrossRef]
- Pearman, A.; Hughes, M.L.; Smith, E.L.; Neupert, S.D. Age Differences in Risk and Resilience Factors in COVID-19-Related Stress. J. Gerontol. Ser. B 2021, 76, e38–e44. [Google Scholar] [CrossRef]
- Robinson, E.; Daly, M. Explaining the Rise and Fall of Psychological Distress during the COVID-19 Crisis in the United States: Longitudinal Evidence from the Understanding America Study. Br. J. Health Psychol. 2020, 26, 570–587. [Google Scholar] [CrossRef]
- Erceg, N.; Ružojčić, M.; Galic, Z. Misbehaving in the Corona Crisis: The Role of Anxiety and Unfounded Beliefs. PsyArXiv 2020, 5621–5630. [Google Scholar] [CrossRef]
- Sobkow, A.; Zaleskiewicz, T.; Petrova, D.; Garcia-Retamero, R.; Traczyk, J. Worry, Risk Perception, and Controllability Predict Intentions toward COVID-19 Preventive Behaviors. Front. Psychol. 2020, 11, 3226. [Google Scholar] [CrossRef]
- Kapoor, H.; Tagat, A. Worry much? Preventive health behaviours related to worry across countries amid COVID-10. J. Health Psychol. 2022, 27, 1125–1136. [Google Scholar] [CrossRef]
- Ramiz, L.; Contrand, B.; Rojas Castro, M.Y.; Dupuy, M.; Lu, L.; Sztal-Kutas, C.; Lagarde, E. A longitudinal study of mental health before and during COVID-19 lockdown in the French population. Global Health 2021, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 19, 1875–1888. [Google Scholar] [CrossRef] [PubMed]
- Prete, G.; Fontanesi, L.; Porcelli, P.; Tommasi, L. The Psychological Impact of COVID-19 in Italy: Worry Leads to Protective Behavior, but at the Cost of Anxiety. Front. Psychol. 2020, 11, 566659. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Geçer, E.; Akgül, Ö. The Impacts of Vulnerability, Perceived Risk, and Fear on Preventive Behaviours against COVID-19. Psychol. Health Med. 2021, 26, 35–43. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk Factors of Critical & Mortal COVID-19 Cases: A Systematic Literature Review and Meta-Analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of Comorbidities and Its Effects in Coronavirus Disease 2019 Patients: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Gerhold, L. COVID-19: Risk Perception and Coping Strategies. Results from a Survey in Germany. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Rosi, A.; van Vugt, F.T.; Lecce, S.; Ceccato, I.; Vallarino, M.; Rapisarda, F.; Vecchi, T.; Cavallini, E. Risk Perception in a Real-World Situation (COVID-19): How It Changes From 18 to 87 Years Old. Front. Psychol. 2021, 12, 646558. [Google Scholar] [CrossRef]
- Barari, S.; Caria, S.; Davola, A.; Falco, P.; Fetzer, T.; Fiorin, S.; Hensel, L.; Ivchenko, A.; Jachimowicz, J.; King, G.; et al. Evaluating COVID-19 Public Health Messaging in Italy: Self-Reported Compliance and Growing Mental Health Concerns. medRxiv 2020, 1–19. [Google Scholar] [CrossRef]
- Lüdecke, D.; von dem Knesebeck, O. Protective Behavior in Course of the COVID-19 Outbreak—Survey Results from Germany. Front. Public Health 2020, 8, 572561. [Google Scholar] [CrossRef]
- Kulesza, W.; Doliński, D.; Muniak, P.; Derakhshan, A.; Rizulla, A.; Banach, M. We Are Infected with the New, Mutated Virus UO-COVID-19. Arch. Med. Sci. 2020, 17, 1706. [Google Scholar] [CrossRef]
- Dolinski, D.; Dolinska, B.; Zmaczynska-Witek, B.; Banach, M.; Kulesza, W. Unrealistic Optimism in the Time of Coronavirus Pandemic: May It Help to Kill, If So—Whom: Disease or the Person? J. Clin. Med. 2020, 9, 1464. [Google Scholar] [CrossRef] [PubMed]
- Bottemanne, H.; Morlaàs, O.; Fossati, P.; Schmidt, L. Does the Coronavirus Epidemic Take Advantage of Human Optimism Bias? Front. Psychol. 2020, 11, 2001. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized Anxiety Disorder, Depressive Symptoms and Sleep Quality during COVID-19 Epidemic in China: A Web-Based Cross-Sectional Survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Iserson, K.V.; Moskop, J.C. Triage in Medicine, Part I: Concept, History, and Types. Ann. Emerg. Med. 2007, 49, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, L. Facing Covid-19 in Italy—Ethics, Logistics, and Therapeutics on the Epidemic’s Front Line. N. Engl. J. Med. 2020, 382, 1873–1875. [Google Scholar] [CrossRef] [PubMed]
- Moskop, J.C.; Iserson, K.V. Triage in Medicine, Part II: Underlying Values and Principles. Ann. Emerg. Med. 2007, 49, 282–287. [Google Scholar] [CrossRef]
- Balmer, C.; Pollina, E. Italy’s Lombardy Asks Retired Health Workers to Join Coronavirus Fight. World Economic Forum, Reuters. Available online: https://www.weforum.org/agenda/2020/03/italys-lombardy-etired-health-workers-coronavirus-covid19-pandemic (accessed on 28 July 2022).
- Bostrom, A.; Böhm, G.; Hayes, A.L.; O’Connor, R.E. Credible Threat: Perceptions of Pandemic Coronavirus, Climate Change and the Morality and Management of Global Risks. Front. Psychol. 2020, 11, 578562. [Google Scholar] [CrossRef]
- Swann, W.B.; Gómez, Á.; Buhrmester, M.D.; López-Rodríguez, L.; Jiménez, J.; Vázquez, A. Contemplating the Ultimate Sacrifice: Identity Fusion Channels pro-Group Affect, Cognition, and Moral Decision Making. J. Pers. Soc. Psychol. 2014, 106, 713–727. [Google Scholar] [CrossRef]
- Bahník, Š.; Efendic, E.; Vranka, M.A. Sacrificing Oneself or Another: The Difference between Prescriptive and Normative Judgments in Moral Evaluation. Psychol. Rep. 2021, 124, 108–130. [Google Scholar] [CrossRef]
- Hardin, G. The Tragedy of the Commons. Science 1968, 162, 1243–1248. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, K.B.; Jacobs, B.W.; Singhal, V.R. Stock Market Reaction to Supply Chain Disruptions from the 2011 Great East Japan Earthquake. Manuf. Serv. Oper. 2020, 22, 683–699. [Google Scholar] [CrossRef]
- Hu, X.; Gurnani, H.; Wang, L. Managing Risk of Supply Disruptions: Incentives for Capacity Restoration. Prod. Oper. Manag. 2013, 22, 137–150. [Google Scholar] [CrossRef]
- Tse, D.; Lau, V.W.; Hong, Y.Y.; Bligh, M.C.; Kakarika, M. Prosociality and hoarding amid the COVID-19 pandemic: A tale of four countries. J. Community Appl. Soc. Psychol. 2022, 32, 507–520. [Google Scholar] [CrossRef]
- Statistisches Bundesamt. Corona-Krise: Experimentelle Daten zeigen aktuelles Kaufverhalten [Corona Crisis: Experimental Data Show Current Buying Behavior]. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2020/05/PD20_178_61.html%3Bjsessionid%3D1ECD957F54DDDE696E8C7D1256534DA2.internet8711 (accessed on 25 March 2021).
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of COVID-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Chen, Y.; Rajabifard, A.; Sabri, S.; Potts, K.E.; Laylavi, F.; Xie, Y.; Zhang, Y. A Discussion of Irrational Stockpiling Behaviour during Crisis. J. Saf. Sci. Resil. 2020, 1, 57–58. [Google Scholar] [CrossRef]
- Bavel, J.J.V.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using Social and Behavioural Science to Support COVID-19 Pandemic Response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Fischer, M.; Twardawski, M.; Steindorf, L.; Thielmann, I. Stockpiling during the COVID-19 Pandemic as a Real-Life Social Dilemma: A Person-Situation Perspective. J. Res. Personal. 2021, 91, 104075. [Google Scholar] [CrossRef]
- OECD. Exploitative Pricing in the Time of COVID-19; OECD: Paris, France, 2020; Available online: https://www.oecd.org/daf/competition/Exploitative-pricing-in-the-time-of-COVID-19.pdf (accessed on 28 July 2022).
- Dorn, F.; Fuest, C.; Göttert, M.; Krolage, C.; Lautenbacher, S.; Link, S.; Peichl, A.; Reif, M.; Sauer, S.; Stöckli, M.; et al. Die Volkswirtschaftlichen Kosten Des Corona-Shutdown Für Deutschland: Eine Szenarienrechnung. Ifo Schnelld. 2020, 15, 29–35. [Google Scholar]
- Wiedemann, P.M.; Dorl, W. Be Alarmed. Some Reflections about the COVID-19 Risk Communication in Germany. J. Risk Res. 2020, 23, 1036–1046. [Google Scholar] [CrossRef]
- Fancourt, D.; Steptoe, A.; Wright, L. The Cummings Effect: Politics, Trust, and Behaviours during the COVID-19 Pandemic. Lancet 2020, 396, 464–465. [Google Scholar] [CrossRef]
- Brüne, M.; Wilson, D.R. Evolutionary Perspectives on Human Behavior during the Coronavirus Pandemic. Evol. Med. Public Health 2020, 2020, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Arslan, R.C.; Walther, M.P.; Tata, C.S. Formr: A Study Framework Allowing for Automated Feedback Generation and Complex Longitudinal Experience-Sampling Studies Using R. Behav. Res. Methods 2020, 52, 376–387. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Dobson, A.J.; Barnett, A.G. An Introduction to Generalized Linear Models, 4th ed.; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Barr, D.J.; Levy, R.; Scheepers, C.; Tily, H.J. Random Effects Structure for Confirmatory Hypothesis Testing: Keep It Maximal. J. Mem. Lang. 2013, 68, 255–278. [Google Scholar] [CrossRef]
- Field, A.; Miles, J.; Field, Z. Discovering Statistics Using R, 5th ed.; SAGE Publications: Beverly Hills, CA, USA, 2018. [Google Scholar]
- Dhar, R. Consumer Preference for a No-Choice Option. J. Consum. Res. 1997, 24, 215–231. [Google Scholar] [CrossRef]
- Redelmeier, D.A.; Shafir, E. Medical Decision Making in Situations That Offer Multiple Alternatives. JAMA 1995, 273, 302–305. [Google Scholar] [CrossRef]
- Flaatten, H.; Van Heerden, V.; Jung, C.; Beil, M.; Leaver, S.; Rhodes, A.; Guidet, B.; DeLange, D.W. The Good, the Bad and the Ugly: Pandemic Priority Decisions and Triage. J. Med. Ethics 2021, 47, e75. [Google Scholar] [CrossRef]
- Biddison, E.L.D.; Gwon, H.S.; Schoch-Spana, M.; Regenberg, A.C.; Juliano, C.; Faden, R.R.; Toner, E.S. Scarce Resource Allocation during Disasters: A Mixed-Method Community Engagement Study. Chest 2018, 153, 187–195. [Google Scholar] [CrossRef]
- Mannelli, C.; Mannelli, C. Whose Life to Save? Scarce Resources Allocation in the COVID-19 Outbreak. J. Med. Ethics 2020, 46, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Bernhard, R.M.; Barak-Corren, N.; Bazerman, M.H.; Greene, J.D. Veil-of-Ignorance Reasoning Mitigates Self-Serving Bias in Resource Allocation during the COVID-19 Crisis. Judgm. Decis. Mak. 2021, 16, 1–19. [Google Scholar] [CrossRef]
- Bocian, K.; Wojciszke, B. Self-Interest Bias in Moral Judgments of Others’ Actions. Pers. Soc. Psychol. Bull. 2014, 40, 898–909. [Google Scholar] [CrossRef]
- Kriss, P.H.; Loewenstein, G.; Wang, X.; Weber, R.A. Behind the Veil of Ignorance: Self-Serving Bias in Climate Change Negotiations. Judgm. Decis. Mak. 2011, 6, 602–615. [Google Scholar] [CrossRef]
- Cannistra, S.A.; Haffty, B.G.; Ballman, K. Challenges Faced by Medical Journals during the COVID-19 Pandemic. J. Clin. Oncol. 2020, 38, 2206–2207. [Google Scholar] [CrossRef]
- Gayle, H.; Foege, W.; Brown, L.; Kahn, B. Framework for Equitable Allocation of COVID-19 Vaccine; National Academies Press (US): Washington, DC, USA, 2020. [Google Scholar] [CrossRef]
- Simons, J.; Vaughan, J. Sacrifice and Risk in the Time of COVID-19. Future Healthc. J. 2020, 7, 158–160. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Kar, S.K.; Menon, V.; Kaliamoorthy, C.; Mukherjee, S.; Alradie-Mohamed, A.; Sharma, P.; Marthoenis, M.; Kabir, R. Panic Buying: An Insight from the Content Analysis of Media Reports during COVID-19 Pandemic. Neurol. Psychiatry Brain Res. 2020, 37, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Garbe, L.; Rau, R.; Toppe, T. Influence of Perceived Threat of COVID-19 and HEXACO Personality Traits on Toilet Paper Stockpiling. PLoS ONE 2020, 15, e0234232. [Google Scholar] [CrossRef]
- Yoshino, S.; Shimotsukasa, T.; Hashimoto, Y.; Oshio, A. The Association between Personality Traits and Hoarding Behavior during the COVID-19 Pandemic in Japan. Pers. Individ. Differ. 2021, 179, 110927. [Google Scholar] [CrossRef]
- Dinić, B.; Bodroža, B. “MY Precious… Toilet Paper”: Stockpiling during the COVID-19 Pandemic Is Related to Selfishness, but not to fear. Primenj. Psihol. 2020, 13, 489–504. [Google Scholar] [CrossRef]
- Dammeyer, J. An Explorative Study of the Individual Differences Associated with Consumer Stockpiling during the Early Stages of the 2020 Coronavirus Outbreak in Europe. Pers. Individ. Differ. 2020, 167, 110263. [Google Scholar] [CrossRef]
- Benker, B. Stockpiling as Resilience: Defending and Contextualising Extra Food Procurement during Lockdown. Appetite 2021, 156, 104981. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.M.Y.; Kar, S.K.; Marthoenis, M.; Sharma, P.; Hoque Apu, E.; Kabir, R. Psychological Underpinning of Panic Buying during Pandemic (COVID-19). Psychiatry Res. 2020, 289, 113061. [Google Scholar] [CrossRef] [PubMed]
- Diehl, M.; Owen, S.K.; Youngblade, L.M. Agency and Communion Attributes in Adults’ Spontaneous Self-Representations. Int. J. Behav. Dev. 2004, 28, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Walker, L.J.; Frimer, J.A. Developmental Trajectories of Agency and Communion in Moral Motivation. Merrill-Palmer Q. 2015, 61, 412–439. [Google Scholar] [CrossRef]
- Roth, A.E. Repugnance as a Constraint on Markets. J. Econ. Perspect. 2007, 21, 37–58. [Google Scholar] [CrossRef]
- Kahneman, D.; Knetsch, J.L.; Thaler, R.H. Fairness as a Constraint on Profit Seeking: Entitlements in the Market. Am. Econ. Rev. 1986, 76, 728–741. [Google Scholar]
- Leuker, C.; Samartzidis, L.; Hertwig, R. What Makes a Market Transaction Morally Repugnant? Cognition 2021, 212, 104644. [Google Scholar] [CrossRef]
- Moodley, K.; Blockman, M.; Al, E. Hard Choices: Ethical Challenges in Phase 1 of COVID-19 Vaccine Roll-out in South Africa. S. Afr. Med. J. 2021, 111, 554–558. [Google Scholar] [CrossRef]
- Gostin, L.O.; Friedman, E.A.; Wetter, S.A. Responding to Covid-19: How to Navigate a Public Health Emergency Legally and Ethically. Hastings Cent. Rep. 2020, 50, 8–12. [Google Scholar] [CrossRef]
- Chiriboga, D.; Garay, J.; Buss, P.; Madrigal, R.S.; Rispel, L.C. Health Inequity during the COVID-19 Pandemic: A Cry for Ethical Global Leadership. Lancet 2020, 395, 1690–1691. [Google Scholar] [CrossRef]
- Liu, S.; Heinzel, S.; Haucke, M.N.; Heinz, A. Increased Psychological Distress, Loneliness, and Unemployment in the Spread of COVID-19 over 6 Months in Germany. Medicina 2021, 57, 53. [Google Scholar] [CrossRef] [PubMed]
- Kooistra, E.B.; Reinders Folmer, C.; Kuiper, M.E.; Olthuis, E.; Brownlee, M.; Fine, A.; van Rooij, B. Mitigating COVID-19 in a Nationally Representative UK Sample: Personal Abilities and Obligation to Obey the Law Shape Compliance with Mitigation Measures (11 May 2020). SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Dudel, C.; Riffe, T.; Acosta, E.; van Raalte, A.; Strozza, C.; Myrskylä, M. Monitoring Trends and Differences in COVID-19 Case-Fatality Rates Using Decomposition Methods: Contributions of Age Structure and Age-Specific Fatality. PLoS ONE 2020, 15, e0238904. [Google Scholar] [CrossRef] [PubMed]
- Sudharsanan, N.; Didzun, O.; Bärnighausen, T.; Geldsetzer, P. The Contribution of the Age Distribution of Cases to COVID-19 Case Fatality across Countries: A Nine-Country Demographic Study. Ann. Intern. Med. 2020, 173, 714–720. [Google Scholar] [CrossRef]
- Verma, A.; Prakash, S. Impact of COVID-19 on Environment and Society. J. Glob. Biosci. 2020, 9, 7352–7363. Available online: https://www.mutagens.co.in/jgb/vol.09/05/090506.pdf (accessed on 28 July 2022).
- Wang, Q.; Su, M. A preliminary assessment of the impact of COVID-19 on environment—A case study of China, Science of the Total Environment. Sci. Total Environ. 2020, 728, 138915. [Google Scholar] [CrossRef]
- Manzanedo, R.D.; Manning, P. COVID-19: Lessons for the Climate Change Emergency. Sci. Total Environ. 2020, 742, 140563. [Google Scholar] [CrossRef]
- Baayen, R.H.; Davidson, D.J.; Bates, D.M. Mixed-Effects Modeling with Crossed Random Effects for Subjects and Items. J. Mem. Lang. 2008, 59, 390–412. [Google Scholar] [CrossRef]
- Pecoraro, F.; Luzi, D.; Clemente, F. The Efficiency in the Ordinary Hospital Bed Management: A Comparative Analysis in Four European Countries before the COVID-19 Outbreak. PLoS ONE 2021, 16, e0248867. [Google Scholar] [CrossRef]
- McKibbin, W.; Fernando, R. The Economic Impact of COVID-19. In Economics in the Time of COVID-19; Baldwin, R., di Mauro, B.W., Eds.; Center for Economic and Policy Research: Washington, DC, USA, 2020; pp. 45–51. [Google Scholar]
- Winter, T.; Riordan, B.C.; Pakpour, A.H.; Griffiths, M.D.; Mason, A.; Poulgrain, J.W.; Scarf, D. Evaluation of the English Version of the Fear of COVID-19 Scale and Its Relationship with Behavior Change and Political Beliefs. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed]
- Storopoli, J.; Braga da Silva Neto, W.L.; Mesch, G.S. Confidence in Social Institutions, Perceived Vulnerability and the Adoption of Recommended Protective Behaviors in Brazil during the COVID-19 Pandemic. Soc. Sci. Med. 2020, 265, 113477. [Google Scholar] [CrossRef]
- Bargain, O.; Aminjonov, U. Trust and Compliance to Public Health Policies in Times of COVID-19. J. Public Econ. 2020, 192, 104316. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.F.; Brumpton, M.; Macintyre, A.; Arapoc, J.; Savage, D.A.; Skali, A.; Stadelmann, D.; Torgler, B. How Confidence in Health Care Systems Affects Mobility and Compliance during the COVID-19 Pandemic. PLoS ONE 2020, 15, e0240644. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Jiang, Y.; Shi, Q.; Zhang, L.; Kong, D.; Qian, M.; Chu, J. Impact of Covid-19 on Anxiety, Stress, and Coping Styles in Nurses in Emergency Departments and Fever Clinics: A Cross-Sectional Survey. Risk Manag. Healthc. Policy 2021, 14, 585–594. [Google Scholar] [CrossRef]
- del Rio, C.; Collins, L.F.; Malani, P. Long-Term Health Consequences of COVID-19. JAMA 2020, 324, 1723. [Google Scholar] [CrossRef]
- Fuchs-Schündeln, N.; Krueger, D.; Ludwig, A.; Popova, I. The Long-Term Distributional and Welfare Effects of Covid-19 School Closures; National Bureau of Economic Research: Cambridge, MA, USA, 2020; Volume 53. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Question | Description |
|---|---|
| In the situation of the current Corona pandemic, hospitals are currently overfilled. 1000 Patients with symptoms show up but immediate treatment is only available for 500 patients. How should patients be prioritized? 0 = Young ones and otherwise healthy ones should be prioritized as they have a higher chance of survival, so the treatment is most likely more effective. 100 = Older ones and people with pre-existing conditions should be prioritized and given health care first as they are at a higher risk of dying; however, their risk of dying even with the treatment is a lot higher. |
| The pandemic hit and markets are running out of medical supplies (masks, disinfections) and canned food. How acceptable is it to stock up on medical supplies and food for you personally even though this might lead to shortages for other people? 0 = Very unacceptable 100 = Very acceptable |
| A registered general practitioner is already 65 years old. In his medical practice, he usually treats many patients including vulnerable patient groups. He is now considering closing his practice during the pandemic as he is at high risk due to his age. How acceptable is it for him to close down the practice? 0 = Very unacceptable 100 = Very acceptable |
| Should Wufa be able to raise prices for disinfectants and medical masks during the pandemic as there is an increased demand, thereby increasing its own profit margin? 0 = Definitely no 100 = Definitely yes |
| Wufa is a medical company specialized in the production of disinfectants and medical masks. Should they be restricted from selling their products to the public and only be able to sell to medical institutions during the pandemic? 0 = Definitely no 100 = Definitely yes |
| Added moral scenarios in T2 and T3 | |
| In your opinion, how strict should the measures that are taken as a result of corona (e.g., exit restriction) be? 0 = Lock-down measures should be strictly enforced to protect high-risk groups and contain the pandemic (e.g., closure of schools and day-care, no restaurant/café opening, no events) 100 = The measures should be relaxed completely in order to limit the economic losses and minimize the social impact on the population as a whole |
| How targeted to a specific group do you think the protective measures to reduce corona infection (e.g., travel/exit restrictions, social distancing, compulsory masks) should be? 0 = Only people who belong to the high-risk group (older people, people with previous illnesses) should distance themselves socially and thus protect themselves from infection. 50 = There should be a basic level of restriction for all (e.g., no major events) but specific restrictions to high-risk populations 100 = The restrictions should apply to everyone |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demel, R.; Grassi, F.; Rafiee, Y.; Waldmann, M.R.; Schacht, A. How German and Italian Laypeople Reason about Distributive Shortages during COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 12067. https://doi.org/10.3390/ijerph191912067
Demel R, Grassi F, Rafiee Y, Waldmann MR, Schacht A. How German and Italian Laypeople Reason about Distributive Shortages during COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(19):12067. https://doi.org/10.3390/ijerph191912067
Chicago/Turabian StyleDemel, Ronja, Francesco Grassi, Yasaman Rafiee, Michael R. Waldmann, and Annekathrin Schacht. 2022. "How German and Italian Laypeople Reason about Distributive Shortages during COVID-19" International Journal of Environmental Research and Public Health 19, no. 19: 12067. https://doi.org/10.3390/ijerph191912067