
Effects of Two Short-Term Aerobic Exercises on Cognitive Function in Healthy Older Adults during COVID-19 Confinement in Japan: A Pilot Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
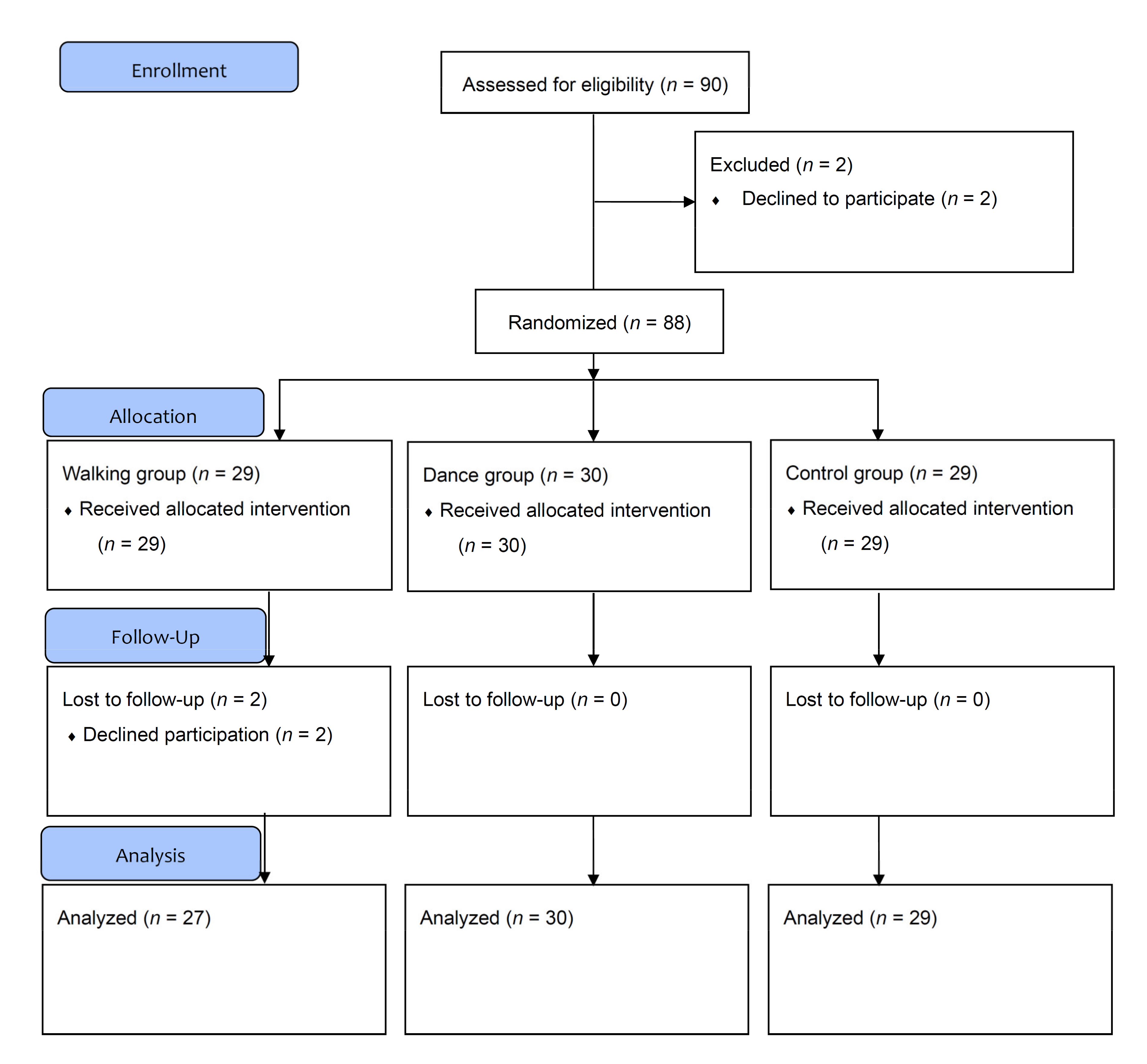
2.1. Trial Design and Setting
2.2. Participants
2.3. Sample Size
2.4. Overview of the Interventions
2.5. Nordic Walking Training (Walking Group)
2.6. Dance Program Training (Dance Group)
2.7. Control Group
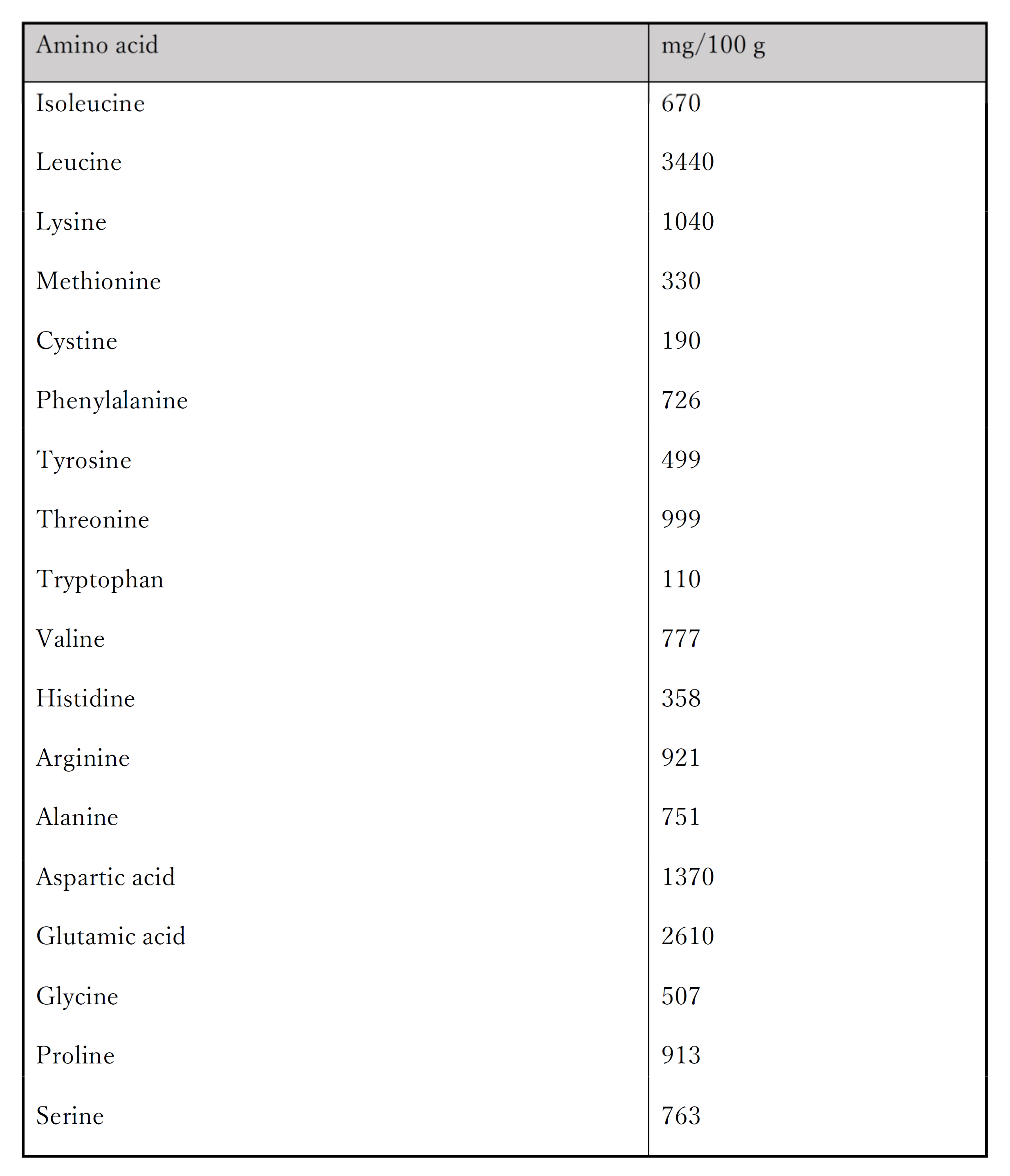
2.8. Protein Intake
2.9. Cognitive Function Measures
2.10. Imitation Ability Measures
2.11. Gait Ability Measures
2.12. Mood State Measures
2.13. Physical Function Measures
2.14. Body Composition Measures
2.15. Other, Frailty, and Sarcopenia Measures
2.16. Statistical Analyses
3. Results
3.1. Background Characteristics
3.2. Cognitive Function
3.3. Mood State
3.4. Imitation Ability
3.5. Gait Ability
3.6. Physical Function
3.7. Body Composition
4. Discussion
4.1. Cognitive Function
4.2. Mood State
4.3. Imitation Ability
4.4. Gait Ability
4.5. Body Composition
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 11 April 2022).
- Rowe, J.W.; Kahn, R.L. Successful Aging. Gerontologist 1997, 37, 433–440. [Google Scholar] [CrossRef]
- Braver, T.S.; Barch, D.M. A theory of cognitive control, aging cognition, and neuromodulation. Neurosci. Biobehav. Rev. 2002, 26, 809–817. [Google Scholar] [CrossRef]
- Hedden, T.; Gabrieli, J.D.E. Insights into the ageing mind: A view from cognitive neuroscience. Nat. Rev. Neurosci. 2004, 5, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.K.; Troyer, A.K.; Maione, A.M.; Murphy, K.J. The impact of memory change on daily life in normal aging and mild cognitive impairment. Gerontologist 2016, 56, 877–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, C.R.; Knopman, D.S.; Jagust, W.J.; Shaw, L.M.; Aisen, P.S.; Weiner, M.W.; Petersen, R.C.; Trojanowski, J.Q. Hypothetical model of dynamic biomarkers of the Alzheimer’s Pathological Cascade. Lancet Neurol. 2010, 9, 119–128. [Google Scholar] [CrossRef] [Green Version]
- Mosconi, L.; Tsui, W.H.; Herholz, K.; Pupi, A.; Drzezga, A.; Lucignani, G.; Reiman, E.M.; Holthoff, V.; Kalbe, E.; Sorbi, S.; et al. Multicenter standardized 18F-FDG PET diagnosis of mild cognitive impairment, Alzheimer’s disease, and other dementias. J. Nucl. Med. 2008, 49, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. The Situation of Users of Nursing Care Insurance Facilities. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kaigo/service16/dl/kekka-gaiyou_05.pdf (accessed on 14 April 2022).
- Heyn, P.; Abreu, B.C.; Ottenbacher, K.J. The effects of exercise training on elderly persons with cognitive impairment and dementia: A meta-analysis. Arch. Phys. Med. Rehabil. 2004, 85, 1694–1704. [Google Scholar] [CrossRef]
- Larson, E.B.; Wang, L.; Bowen, J.D.; McCormick, W.C.; Teri, L.; Crane, P.; Kukull, W. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann. Intern. Med. 2006, 144, 73–81. [Google Scholar] [CrossRef]
- Hötting, K.; Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 2013, 37, 2243–2257. [Google Scholar] [CrossRef]
- Coelho, F.G.D.M.; Gobbi, S.; Andreatto, C.A.A.; Corazza, D.I.; Pedroso, R.V.; Santos-Galduróz, R.F. Physical exercise modulates peripheral levels of brain-derived neurotrophic factor (BDNF): A systematic review of experimental studies in the elderly. Arch. Gerontol. Geriatr. 2013, 56, 10–15. [Google Scholar] [CrossRef]
- Neeper, S.A.; Gómez-Pinilla, F.; Choi, J.; Cotman, C.W. Physical activity increases mRNA for brain-derived neurotrophic factor and nerve growth factor in rat brain. Brain Res. 1996, 726, 49–56. [Google Scholar] [CrossRef]
- Bae, S.; Lee, S.; Harada, K.; Makino, K.; Chiba, I.; Katayama, O.; Shinkai, Y.; Park, H.; Shimada, H. Engagement in lifestyle activities is associated with increased alzheimer’s disease-associated cortical thickness and cognitive performance in older adults. J. Clin. Med. 2020, 9, 1424. [Google Scholar] [CrossRef]
- Cheng, S.T. Cognitive Reserve and the Prevention of Dementia: The role of physical and cognitive activities. Curr. Psychiatry Rep. 2016, 18, 85. [Google Scholar] [CrossRef] [Green Version]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, E.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1166–1170. [Google Scholar] [CrossRef] [Green Version]
- Gaitán, J.M.; Boots, E.A.; Dougherty, R.J.; Oh, J.M.; Ma, Y.; Edwards, D.F.; Christian, B.T.; Cook, D.B.; Okonkwo, O.C. Brain glucose metabolism, cognition, and cardiorespiratory fitness following exercise training in adults at risk for Alzheimer’s disease. Brain Plast. 2019, 5, 83–95. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, C.M.; Pereira, J.R.; de Andrade, L.P.; Garuffi, M.; Talib, L.L.; Forlenza, O.V.; Cancela, J.M.; Cominetti, M.R.; Stella, F. Physical exercise in MCI elderly promotes reduction of pro-inflammatory cytokines and improvements on cognition and BDNF peripheral levels. Curr. Alzheimer Res. 2014, 11, 799–805. [Google Scholar] [CrossRef]
- The Japanese Neurological Association. Dementia Disease Clinical Practice Guidelines; Igaku-Shoin Ltd.: Tokyo, Japan, 2017; Available online: https://www.igaku-shoin.co.jp/book/detail/91798 (accessed on 14 April 2022).
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [Green Version]
- Candela, F.; Zucchetti, G.; Magistro, D.; Rabaglietti, E. The Effects of a physical activity program and a cognitive training program on the long-term memory and selective attention of older adults: A comparative study. Act. Adapt. Aging 2015, 39, 77–91. [Google Scholar] [CrossRef] [Green Version]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Weinstein, A.M.; Voss, M.W.; Prakash, R.S.; Chaddock, L.; Szabo, A.; White, S.M.; Wojcicki, T.R.; Mailey, E.; McAuley, E.; Kramer, A.F.; et al. The association between aerobic fitness and executive function is mediated by prefrontal cortex volume. Brain Behav. Immun. 2012, 26, 811–819. [Google Scholar] [CrossRef] [Green Version]
- Gheysen, F.; Poppe, L.; Desmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef] [Green Version]
- Law, L.L.F.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: A systematic review. Ageing Res. Rev. 2014, 15, 61–75. [Google Scholar] [CrossRef]
- Sánchez-González, J.L.; Sánchez-Rodríguez, J.L.; Martín-Vallejo, J.; Martel-Martel, A.; González-Sarmiento, R. Effects of physical exercise on cognition and telomere length in healthy older women. Brain Sci. 2021, 11, 1417. [Google Scholar] [CrossRef] [PubMed]
- Noor, F.M.; Islam, M.M. Prevalence and associated risk factors of mortality among COVID-19 patients: A meta-analysis. J. Commun. Health. 2020, 45, 1270–1282. [Google Scholar] [CrossRef]
- Ghram, A.; Briki, W.; Mansoor, H.; Al-Mohannadi, A.S.; Lavie, C.J.; Chamari, K. Home-based exercise can be beneficial for counteracting sedentary behavior and physical inactivity during the COVID-19 pandemic in older adults. Postgrad. Med. 2021, 133, 469–480. [Google Scholar] [CrossRef]
- Turk, Z.; Vidensek, S.; Micetic Turk, D. Nordic walking: A new form of physical activity in the elderly. Acta Med. Croat. 2007, 61, 33–36. [Google Scholar]
- Figueiredo, S.; Finch, L.; Mai, J.; Ahmed, S.; Huang, A.; Mayo, N.E. Nordic walking for geriatric rehabilitation: A randomized pilot trial. Disabil. Rehabil. 2013, 35, 968–975. [Google Scholar] [CrossRef]
- Kshtriya, S.; Barnstaple, R.; Rabinovich, D.B.; DeSouza, J.F.X. Dance and Aging: A critical review of findings in neuroscience. Am. J. Dance Ther. 2015, 37, 81–112. [Google Scholar] [CrossRef]
- Machacova, K.; Vankova, H.; Volicer, L.; Veleta, P.; Holmerova, I. Dance as prevention of late life functional decline among nursing home residents. J. Appl. Gerontol. 2017, 36, 1453–1470. [Google Scholar] [CrossRef] [PubMed]
- Sharp, K.; Hewitt, J. Dance as an Intervention for People with Parkinson’s disease: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2014, 47, 445–456. [Google Scholar] [CrossRef]
- Vankova, H.; Holmerova, I.; Machacova, K.; Volicer, L.; Veleta, P.; Celko, A.M. The effect of dance on depressive symptoms in nursing home residents. J. Am. Med. Dir. Assoc. 2014, 15, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.M. Dance, aging, and neuroplasticity: An integrative review. Neurocase 2021, 27, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Garcia, A.; Villafaina, S.; Collado-Mateo, D.; Leon-Llamas, J.L.; Gusi, N. Effect of dance therapies on motor-cognitive dual-task performance in middle-aged and older adults: A systematic review and meta-analysis. Disabil. Rehabil. 2021, 43, 3147–3158. [Google Scholar] [CrossRef] [PubMed]
- Kattenstroth, J.C.; Kalisch, T.; Holt, S.; Tegenthoff, M.; Dinse, H.R. Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front. Aging Neurosci. 2013, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Müller, P.; Rehfeld, K.; Schmicker, M.; Hökelmann, A.; Dordevic, M.; Lessmann, V.; Brigadski, T.; Kaufmann, J.; Müller, N.G. Evolution of neuroplasticity in response to physical activity in old age: The case for dancing. Front. Aging Neurosci. 2017, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Rehfeld, K.; Müller, P.; Aye, N.; Schmicker, M.; Dordevic, M.; Kaufmann, J.; Hökelmann, A.; Müller, N.G. Dancing or fitness sport? the effects of two training programs on hippocampal plasticity and balance abilities in healthy seniors. Front. Hum. Neurosci. 2017, 11, 305. [Google Scholar] [CrossRef]
- Rehfeld, K.; Lüders, A.; Hökelmann, A.; Lessmann, V.; Kaufmann, J.; Brigadski, T.; Müller, P.; Müller, N.G. Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS ONE 2018, 13, e0196636. [Google Scholar] [CrossRef] [Green Version]
- Giacosa, C.; Karpati, F.J.; Foster, N.E.V.; Penhune, V.B.; Hyde, K.L. Dance and music training have different effects on white matter diffusivity in sensorimotor pathways. NeuroImage 2016, 135, 273–286. [Google Scholar] [CrossRef]
- Rektorova, I.; Klobusiakova, P.; Balazova, Z.; Kropacova, S.; Sejnoha Minsterova, A.; Grmela, R.; Skotakova, A.; Rektor, I. Brain structure changes in nondemented seniors after six-month dance-exercise intervention. Acta Neurol. Scand. 2020, 141, 90–97. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Rehfeld, K.; Hökelmann, A.; Schega, L. The effect of a six-month dancing program on motor-cognitive dual-task performance in older adults. J. Aging Phys. Act. 2015, 23, 647–652. [Google Scholar] [CrossRef]
- Park, J.E. Apraxia: Review and update. J. Clin. Neurol. 2017, 13, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Breen, L.; Phillips, S.M. Skeletal muscle protein metabolism in the elderly: Interventions to counteract the “anabolic resistance” of ageing. Nutr. Metab. 2011, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, A.; Okuyama, T.; Mori, H.; Sato, K.; Ichiki, M.; Nouchi, R. Drum communication program intervention in older adults with cognitive impairment and dementia at nursing home: Preliminary evidence from pilot randomized controlled trial. Front. Aging Neurosci. 2020, 12, 142. [Google Scholar] [CrossRef]
- Kirwan, R.; McCullough, D.; Butler, T.; Perez De Heredia, F.; Davies, I.G.; Stewart, C. Sarcopenia during COVID-19 lockdown restrictions: Long-term health effects of short-term muscle loss. GeroScience 2020, 42, 1547–1578. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. Withdrawn: CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2010, 8, 604–612. [Google Scholar] [CrossRef]
- Sugishita, M.; Koshizuka, Y.; Sudou, S.; Sugishita, K.; Hemmi, I.; Karasawa, S.; Ihara, M.; Asada, T.; Mihara, B. The Validity and reliability of the japanese version of the Mini-Mental State Examination MMSE-J with the original procedure of the attention and calculation task. Jpn. J. Cogn. Neurosci. 2018, 20, 91–110. [Google Scholar]
- Takeshima, N.; Islam, M.M.; Rogers, M.E.; Rogers, N.L.; Sengoku, N.; Koizumi, D.; Kitabayashi, Y.; Imai, A.; Naruse, A. Effects of nordic walking compared to conventional walking and band-based resistance exercise on fitness in older adults. J. Sports Sci. Med. 2013, 12, 422. [Google Scholar]
- Istvandity, L. Combining music and reminiscence therapy interventions for wellbeing in elderly populations: A systematic review. Complement. Ther. Clin. Pract. 2017, 28, 18–25. [Google Scholar] [CrossRef]
- Karageorghis, C.I.; Jones, L.; Low, D.C. Relationship between exercise heart rate and music tempo preference. Res. Q. Exer. Sport. 2006, 77, 240–250. [Google Scholar] [CrossRef]
- Farshidfar, F.; Shulgina, V.; Myrie, S.B. Nutritional supplementations and administration considerations for sarcopenia in older adults. Nutr. Aging 2015, 3, 147–170. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.R.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A frontal assessment battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Jia, S.; Zhou, Z.; Hou, C.; Zheng, W.; Rong, P.; Jiao, J. The gesture imitation in Alzheimer’s disease dementia and amnestic mild cognitive impairment. J. Alzheimers Dis. 2016, 53, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, H.; Maki, Y.; Yamagami, T. Yamaguchi fox-pigeon imitation test: A rapid test for dementia. Dem. Geriatr. Cogn. Disord. 2010, 29, 254–258. [Google Scholar] [CrossRef]
- Japan Society for Higher Brain Dysfunction. Standard Performance Test for Apraxia (SPTA); Shinkoh Igaku Shuppansha Co., Ltd.: Tokyo, Japan, 1999; Available online: http://shinkoh-igaku.jp/cgi-bin/order_inspection/spta/ordermail.cgi (accessed on 14 April 2022).
- Chiaramonte, R.; Cioni, M. Critical spatiotemporal gait parameters for individuals with dementia: A systematic review and meta-analysis. Hong Kong Physiother. J. 2021, 41, 1–14. [Google Scholar] [CrossRef]
- Brink, T.L.; Yesavage, J.A.; Lum, O.; Heersema, P.H.; Adey, M.; Rose, T.L. Screening tests for geriatric depression. Clin. Gerontol. 1982, 1, 37–43. [Google Scholar] [CrossRef]
- The Whoqol Group. The World Health Organization Quality of Life Assessment (WHOQOL): Development and general psychometric properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar] [CrossRef]
- Sugishita, K.; Sugishita, M.; Hemmi, I.; Asada, T.; Tanigawa, T. A Validity and reliability study of the Japanese Version of the Geriatric Depression Scale 15 (GDS-15-J). Clin. Gerontol. 2017, 40, 233–240. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B.; Short, A. A Short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Wallmann, H.W.; Evans, N.S.; Day, C.; Neelly, K.R. Interrater reliability of the five-times-sit-to-stand test. Home Health Care Manag. Pract. 2013, 25, 13–17. [Google Scholar] [CrossRef]
- Horak, F.B.; Nashner, L.M. Central programming of postural movements: Adaptation to altered support-surface configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef]
- Svoboda, Z.; Bizovska, L.; Gonosova, Z.; Linduska, P.; Kovacikova, Z.; Vuillerme, N. Effect of aging on the association between ankle muscle strength and the control of bipedal stance. PLoS ONE 2019, 14, e0223434. [Google Scholar] [CrossRef] [Green Version]
- Tavakkoli Oskouei, S.; Malliaras, P.; Jansons, P.; Hill, K.; Soh, S.E.; Jaberzadeh, S.; Perraton, L. Is ankle plantar flexor strength associated with balance and walking speed in healthy people? A systematic review and meta-analysis. Phys. Ther. 2021, 101, pzab018. [Google Scholar] [CrossRef]
- Kemoun, G.; Thoumie, P.; Boisson, D.; Guieu, J.D. Ankle Dorsiflexion Delay Can Predict Falls in the Elderly. J. Rehabil. Med. 2002, 34, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Buckinx, F.; Reginster, J.Y.; Dardenne, N.; Croisiser, J.L.; Kaux, J.F.; Beaudart, C.; Slomian, J.; Bruyère, O. Concordance between muscle mass assessed by bioelectrical impedance analysis and by dual energy x-ray absorptiometry: A cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 60. [Google Scholar] [CrossRef] [Green Version]
- Mazess, R.B.; Barden, H.S.; Bisek, J.P.; Hanson, J. Dual-Energy X-Ray Absorptiometry for Total-Body and Regional Bone-Mineral and Soft-Tissue Composition. Am. J. Clin. Nutr. 1990, 51, 1106–1112. [Google Scholar] [CrossRef]
- Leelahagul, P.; Putadechakum, S.; Tanphaichitr, V. The effects of soluble dietary fibre from the thai herb, sweet basil seed, on human body composition. Asia Pac. J. Clin. Nutr. 1992, 1, 169–174. [Google Scholar]
- Roubenoff, R. Applications of bioelectrical impedance analysis for body composition to epidemiologic studies. Am. J. Clin. Nutr. 1996, 64, 459S–462S. [Google Scholar] [CrossRef]
- Foster, K.R.; Lukaski, H.C. Whole-body impedance–What does it measure? Am. J. Clin. Nutr. 1996, 64, 388S–396S. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.; Dev, R.; Pimental, L.; Park, M.; Cerana, M.A.; Liu, D.; Bruera, E. Association between multi-frequency phase angle and survival in patients with advanced cancer. J. Pain Symptom Manag. 2017, 53, 571–577. [Google Scholar] [CrossRef] [Green Version]
- Matias, C.N.; Nunes, C.L.; Francisco, S.; Tomeleri, C.M.; Cyrino, E.S.; Sardinha, L.B.; Silva, A.M. Phase angle predicts physical function in older adults. Arch. Gerontol. Geriatr. 2020, 90, 104151. [Google Scholar] [CrossRef]
- Nunes, J.P.; Ribeiro, A.S.; Silva, A.M.; Schoenfeld, B.J.; Dos Santos, L.; Cunha, P.M.; Nascimento, M.A.; Tomeleri, C.M.; Nabuco, H.C.G.; Antunes, M.; et al. Improvements in phase angle are related with muscle quality index after resistance training in older women. J. Aging Phys. Act. 2019, 27, 515–520. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Cavaglieri, C.R.; De Souza, M.F.; Cavalcante, E.F.; Antunes, M.; Nabbuco, H.C.G.; Venturini, D.; Barbosa, D.S.; Silva, A.M.; Cyrino, E.S. Phase angle is related with inflammatory and oxidative stress biomarkers in older women. Exp. Gerontol. 2018, 102, 12–18. [Google Scholar] [CrossRef]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG Index of competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur. J. Intern. Med. 2016, 31, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Prado, C.M.; Bell, J.J.; Gonzalez, M.C. Untangling malnutrition, physical dysfunction, sarcopenia, frailty and cachexia in ageing. In Interdisciplinary Nutritional Management and Care for Older Adults; Springer: Cham, Switzerland, 2021; pp. 99–113. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Wheeler, B.; Torchiano, M.; Torchiano, M. Package “lmPerm”. R Package Version. 2020. Available online: https://cran.r-project.org/web/packages/lmPerm/lmPerm.pdf (accessed on 14 April 2022).
- Wheeler, R.E.; Torchiano, M. Permutation tests for linear models in R. Compr. R Arch. Network 2010, 1, 3–35. [Google Scholar]
- Kulason, K.; Nouchi, R.; Hoshikawa, Y.; Noda, M.; Okada, Y.; Kawashima, R. The beneficial effects of cognitive training with simple calculation and reading aloud (SCRA) in the Elderly Postoperative Population: A Pilot Randomized Controlled Trial. Front. Aging Neurosci. 2018, 10, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouchi, R.; Taki, Y.; Takeuchi, H.; Hashizume, H.; Nozawa, T.; Kambara, T.; Sekiguchi, A.; Miyauchi, C.M.; Kotozaki, Y.; Nouchi, H.; et al. Brain training game boosts executive functions, working memory, and processing speed in the young adults: A randomized controlled trial. PLoS ONE 2013, 8, e55518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouchi, R.; Kobayashi, A.; Nouchi, H.; Kawashima, R. Newly developed TV-based cognitive training games improve car driving skills, cognitive functions, and mood in healthy older adults: Evidence from a randomized controlled trial. Front. Aging Neurosci. 2019, 11, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storey, J.D. A direct approach to false discovery rates. J. R. Stat. Soc. B 2002, 64, 479–498. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Science; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Cawthon, P.M.; Stone, K.L.; Hillier, T.A.; Cauley, J.A.; Hochberg, M.C.; Rodondi, N.; et al. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch. Intern. Med. 2008, 168, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Hewston, P.; Kennedy, C.C.; Borhan, S.; Merom, D.; Santaguida, P.; Ioannidis, G.; Marr, S.; Santesso, N.; Thabane, L.; Bray, S.; et al. Effects of dance on cognitive function in older adults: A systematic review and meta-analysis. Age Ageing 2021, 50, 1084–1092. [Google Scholar] [CrossRef]
- Lundin-Olsson, L.; Nyberg, L.; Gustafson, Y. ‘Stops walking when talking’ as a predictor of falls in elderly people. Lancet 1997, 349, 617. [Google Scholar] [CrossRef]
- Plummer, P.; Zukowski, L.A.; Giuliani, C.; Hall, A.M.; Zurakowski, D. Effects of physical exercise interventions on gait-related dual-task interference in older adults: A systematic review and meta-analysis. Gerontology 2015, 62, 94–117. [Google Scholar] [CrossRef]
- Xiong, J.; Ye, M.; Wang, L.; Zheng, G. Effects of physical exercise on executive function in cognitively healthy older adults: A systematic review and meta-analysis of randomized controlled trials: Physical exercise for executive function. Int. J. Nurs. Stud. 2021, 114, 103810. [Google Scholar] [CrossRef]
- Merom, D.; Grunseit, A.; Eramudugolla, R.; Jefferis, B.; Mcneill, J.; Anstey, K.J. Cognitive benefits of social dancing and walking in old age: The dancing mind randomized controlled trial. Front. Aging Neurosci. 2016, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Fraisse, P. Rhythm and tempo. Psychol. Music. 1982, 1, 149–180. [Google Scholar]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. The influence of the COVID-19 pandemic on physical activity and new incidence of frailty among initially non-frail older adults in japan: A follow-up online survey. J. Nutr. Health Aging 2021, 25, 751–756. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. Effect of the COVID-19 epidemic on physical activity in community-dwelling older adults in japan: A cross-sectional online survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef]
- Muiños, M.; Ballesteros, S. Does dance counteract age-related cognitive and brain declines in middle-aged and older adults? A systematic review. Neurosci. Biobehav. Rev. 2021, 121, 259–276. [Google Scholar] [CrossRef]
- Wu, C.; Yi, Q.; Zheng, X.; Cui, S.; Chen, B.; Lu, L.; Tang, C. Effects of mind-body exercises on cognitive function in older adults: A meta-analysis. J. Am. Geriatr. Soc. 2019, 67, 749–758. [Google Scholar] [CrossRef]
- Etgen, T.; Sander, D.; Huntgeburth, U.; Poppert, H.; Förstl, H.; Bickel, H. Physical activity and incident cognitive impairment in elderly persons: The INVADE study. Arch. Intern. Med. 2010, 170, 186–193. [Google Scholar] [CrossRef]
- Dawes, P.; Cruickshanks, K.J.; Fischer, M.E.; Klein, B.E.K.; Klein, R.; Nondahl, D.M. Hearing-aid use and long-term health outcomes: Hearing handicap, mental health, social engagement, cognitive function, physical health, and mortality. Int. J. Audiol. 2015, 54, 838–844. [Google Scholar] [CrossRef] [Green Version]
- Penninkilampi, R.; Casey, A.N.; Singh, M.F.; Brodaty, H. The association between social engagement, loneliness, and risk of dementia: A systematic review and meta-analysis. J. Alzheimers Dis. 2018, 66, 1619–1633. [Google Scholar] [CrossRef]
- Schellenberg, E.G. Music lessons enhance IQ. Psychol. Sci. 2004, 15, 511–514. [Google Scholar] [CrossRef]
- Moreno, S.; Farzan, F. Music training and inhibitory control: A multidimensional model. Ann. N. Y. Acad. Sci. 2015, 1337, 147–152. [Google Scholar] [CrossRef]
- Chen, F.T.; Etnier, J.L.; Chan, K.H.; Chiu, P.K.; Hung, T.M.; Chang, Y.K. Effects of exercise training interventions on executive function in older adults: A systematic review and meta-analysis. Sports Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef]
- Nouchi, R.; Taki, Y.; Takeuchi, H.; Sekiguchi, A.; Hashizume, H.; Nozawa, T.; Nouchi, H.; Kawashima, R. Four weeks of combination exercise training improved executive functions, episodic memory, and processing speed in healthy elderly people: Evidence from a randomized controlled trial. Age 2014, 36, 787–799. [Google Scholar] [CrossRef] [Green Version]
- Netz, Y.; Wu, M.J.; Becker, B.J.; Tenenbaum, G. Physical activity and psychological well-being in advanced age: A meta-analysis of intervention studies. Psychol. Aging 2005, 20, 272–284. [Google Scholar] [CrossRef] [Green Version]
- Elavsky, S.; McAuley, E.; Motl, R.W.; Konopack, J.F.; Marquez, D.X.; Hu, L.; Jerome, G.J.; Diener, E. Physical activity enhances long-term quality of life in older adults: Efficacy, esteem, and affective influences. Ann. Behav. Med. 2005, 30, 138–145. [Google Scholar] [CrossRef]
- Park, M.; Anaza, E.; Shin, H.; Pack, S.M.; Chitiyo, M. Relationship between physical activity and quality of life in older adults: A meta-analysis. J. Phys. Educ. Sport. 2020, 20, 3467–3477. [Google Scholar] [CrossRef]
- Hansen, P.; Main, C.; Hartling, L. Dance intervention affects social connections and body appreciation among older adults in the long term despite COVID-19 social isolation: A mixed methods pilot study. Front. Psychol. 2021, 12, 635938. [Google Scholar] [CrossRef]
- Vuorinen, E.; Laine, M.; Rinne, J. Common Pattern of language impairment in vascular dementia and in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2000, 14, 81–86. [Google Scholar] [CrossRef]
- Wheaton, L.A.; Hallett, M. Ideomotor apraxia: A review. J. Neurol. Sci. 2007, 260, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tabuchi, H.; Konishi, M.; Saito, N.; Kato, M.; Mimura, M. Reverse fox test for detecting visuospatial dysfunction corresponding to parietal hypoperfusion in mild Alzheimer’s disease. Am. J. Alzheimers Dis. Other Demen. 2014, 29, 177–182. [Google Scholar] [CrossRef]
- Rousseaux, M.; Rénier, J.; Anicet, L.; Pasquier, F.; Mackowiak-Cordoliani, M.A. Gesture comprehension, knowledge and production in Alzheimer’s disease. Eur. J. Neurol. 2012, 19, 1037–1044. [Google Scholar] [CrossRef]
- Boyke, J.; Driemeyer, J.; Gaser, C.; Buchel, C.; May, A.; Brain, T.I. Training-induced brain structure changes in the elderly. J. Neurosci. 2008, 28, 7031–7035. [Google Scholar] [CrossRef] [PubMed]
- Kocur, P.; Wiernicka, M.; Wilski, M.; Kaminska, E.; Furmaniuk, L.; Maslowska, M.F.; Lewandowski, J. Does nordic walking improves the postural control and gait parameters of women between the age 65 and 74: A randomized trial. J. Phys. Ther. Sci. 2015, 27, 3733–3737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchet, O.; Annweiler, C.; Montero-Odasso, M.; Fantino, B.; Herrmann, F.R.; Allali, G. Gait control: A specific subdomain of executive function? J. Neuroeng. Rehabil. 2012, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.F.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef]
- Eyigor, S.; Karapolat, H.; Durmaz, B.; Ibisoglu, U.; Cakir, S. A randomized controlled trial of turkish folklore dance on the physical performance, balance, depression and quality of life in older women. Arch. Gerontol. Geriatr. 2009, 48, 84–88. [Google Scholar] [CrossRef]
- Keogh, J.W.; Kilding, A.; Pidgeon, P.; Ashley, L.; Gillis, D. Physical benefits of dancing for healthy older adults: A review. J. Aging Phys. Act. 2009, 17, 479–500. [Google Scholar] [CrossRef] [Green Version]
- Granacher, U.; Muehlbauer, T.; Bridenbaugh, S.A.; Wolf, M.; Roth, R.; Gschwind, Y.; Wolf, I.; Mata, R.; Kressig, R.W. Effects of a salsa dance training on balance and strength performance in older adults. Gerontology 2012, 58, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Adlerton, A.K.; Moritz, U. Does calf-muscle fatigue affect standing balance? Scand. J. Med. Sci. Sports. 1996, 6, 211–215. [Google Scholar] [CrossRef]
- Hamner, S.R.; Seth, A.; Delp, S.L. Muscle contributions to propulsion and support during running. J. Biomech. 2010, 43, 2709–2716. [Google Scholar] [CrossRef] [Green Version]
- Ossowski, Z.M.; Skrobot, W.; Aschenbrenner, P.; Cesnaitiene, V.J.; Smaruj, M. Effects of short-term nordic walking training on sarcopenia-related parameters in women with low bone mass: A preliminary study. Clin. Interv. Aging 2016, 11, 1763–1771. [Google Scholar] [CrossRef] [Green Version]
- Yamada, M.; Arai, H.; Yoshimura, K.; Kajiwara, Y.; Sonoda, T.; Nishiguchi, S.; Aoyama, T. Nutritional Supplementation during resistance training improved skeletal muscle mass in community-dwelling frail older adults. J. Frailty Aging 2012, 1, 64–70. [Google Scholar] [CrossRef]
- Lee, Y.; Kwon, O.; Shin, C.S.; Lee, S.M. Use of bioelectrical impedance analysis for the assessment of nutritional status in critically ill patients. Clin. Nutr. Res. 2015, 4, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Foster, P.P. How does dancing promote brain reconditioning in the elderly? Front. Aging Neurosci. 2013, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Tian, Q.; Chastan, N.; Thambisetty, M.; Resnick, S.M.; Ferrucci, L.; Studenski, S.A. Bimanual gesture imitation links to cognition and olfaction. J. Am. Geriatr. Soc. 2019, 67, 2581–2586. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Criterion | Walking Group | Dance Group | Control Group | ||||
|---|---|---|---|---|---|---|---|
| (n = 29) | (n = 30) | (n = 29) | |||||
| Mean (SD) | Range | Mean (SD) | Range | Mean (SD) | Range | ANOVA p-Value | |
| Age, years | 67.93 (5.81) | 60–80 | 67.20 (5.39) | 60–82 | 68.31 (5.87) | 61–79 | 0.7997 |
| Sex (female: male) | 7:22 | 13:17 | 6:23 | ||||
| MMSE total score | 28.17 (1.28) | 25–30 | 28.60 (1.33) | 26–30 | 27.83 (1.65) | 25–30 | 0.3674 |
| Education, years | 15.93 (1.65) | 12–20 | 15.37 (1.56) | 12–18 | 15.45 (1.48) | 10–18 | 0.2428 |
| Number of family members | 2.41 (0.91) | 1–4 | 2.17 (0.83) | 1–4 | 2.00 (0.76) | 1–4 | 0.1707 |
| IADL (13 categories) | 11.97 (0.98) | 10–13 | 12.10 (0.88) | 10–13 | 11.90 (0.77) | 10–13 | 0.7666 |
| Calf circumference (cm) | 35.84 (3.01) | 30.00–43.25 | 36.01 (2.83) | 29.80–42.50 | 35.28 (2.08) | 31.50–40.25 | 0.4260 |
| Work status (No job:Work part-time:Work full-time) | 16:5:8 | 15:7:8 | 15:6:8 | ||||
| Exercise habits (No or Light:Moderate:Heavy) | 15:6:8 | 22:3:5 | 13:7:9 | ||||
| Lifestyle diseases (None:With) | 16:13 | 21:9 | 19:10 | ||||
| Diabetes (None:With) | 27:2 | 28:2 | 29:0 | ||||
| Weight loss | 29:0 | 28:2 | 29:0 | ||||
| A felling of fatigue | 28:1 | 27:3 | 27:2 | ||||
| Hip Arthroplasty (None:One-Leg:Both-Legs) | 29:0:0 | 30:0:0 | 28:1:0 | ||||
| Knee Injury (None:OA of One-Leg:OA of Both-Legs:ACL of One-Leg:ACL of Both-Legs) | 17:6:3:3:0 | 15:8:6:1:0 | 13:13:2:1:0 | ||||
| Cognitive Function Measures | |||||||
| MoCA total score | 26.76 (1.68) | 23–30 | 26.63 (1.83) | 22–30 | 27.00 (1.79) | 21–30 | 0.6036 |
| Visuospatial/Executive | 4.10 (0.86) | 2–5 | 4.03 (0.93) | 2–5 | 4.28 (0.92) | 2–5 | 0.5736 |
| Naming | 2.97 (0.19) | 2–3 | 3.00 (0.00) | 3 | 2.97 (0.19) | 2–3 | 0.5979 |
| Attention | 5.86 (0.44) | 4–6 | 5.63 (0.61) | 4–6 | 5.83 (0.38) | 5–6 | 0.1613 |
| Language | 1.79 (0.90) | 0–3 | 2.03 (1.13) | 0–7 | 1.79 (0.82) | 0–3 | 0.5415 |
| Abstraction | 1.72 (0.53) | 0–2 | 1.70 (0.47) | 1–2 | 1.66 (0.48) | 1–2 | 0.8641 |
| Delayed Recall | 4.41 (0.82) | 2–5 | 4.53 (0.63) | 3–5 | 4.48 (0.69) | 3–5 | 0.8142 |
| Orientation | 5.90 (0.31) | 5–6 | 5.87 (0.35) | 5–6 | 5.97(0.19) | 5–6 | 0.4102 |
| FAB total score | 15.79 (1.37) | 13–18 | 16.13 (1.55) | 11–18 | 16.14 (1.46) | 13–18 | 0.3696 |
| Similarities (conceptualization) | 2.21 (0.73) | 0–3 | 2.30 (0.70) | 0–3 | 2.31 (0.60) | 1–3 | 0.8154 |
| Lexical Fluency (mental flexibility) | 2.76 (0.51) | 1–3 | 2.83 (0.38) | 2–3 | 2.69 (0.60) | 1–3 | 0.5526 |
| Motor Series (programming) | 2.69 (0.47) | 2–3 | 2.83 (0.53) | 1–3 | 2.79 (0.41) | 2–3 | 0.4916 |
| Conflicting Instructions (sensitivity to interference) | 2.72 (0.65) | 1–3 | 2.77 (0.50) | 1–3 | 2.79 (0.49) | 1–3 | 0.8913 |
| Go–No-Go (inhibitory control) | 2.41 (0.78) | 0–3 | 2.40 (0.81) | 0–3 | 2.59 (0.82) | 0–3 | 0.6183 |
| Prehension Behavior (environmental autonomy) | 3.00 (0.00) | 3 | 3.00 (0.00) | 3 | 2.97 (0.19) | 2–3 | 0.3658 |
| Mood State Measures | |||||||
| GDS score | 1.31 (1.75) | 0–8 | 2.50 (2.00) | 0–7 | 2.24 (2.49) | 0–9 | 0.0976 |
| WHO-QOL score | 106.66 (10.60) | 83–124 | 96.70 (9.75) | 80–119 | 101.41 (11.38) | 73–123 | 0.0756 |
| Imitation | |||||||
| Imitation gesture total score | 1.66 (2.51) | 0–10 | 1.30 (1.95) | 0–6 | 2.03 (2.76) | 0–10 | 0.5530 |
| Gait Ability Measures | |||||||
| Fast gait speed 10 m (s) | 5.22 (1.07) | 3.46–9.11 | 5.19 (0.72) | 3.47–6.36 | 5.03 (0.79) | 3.09–6.54 | 0.4188 |
| Step (cm) | 88.69 (13.83) | 62.40–139.80 | 88.57 (13.13) | 71.30–123.20 | 87.93 (10.06) | 66.10–109.00 | 0.9690 |
| RMS | 1.17 (0.33) | 0.37–1.78 | 1.27 (0.40) | 0.42–1.93 | 1.32 (0.46) | 0.49–2.21 | 0.3414 |
| Walking cycles | 0.05 (0.05) | 0.00–0.26 | 0.04 (0.03) | 0.00–0.14 | 0.05 (0.03) | 0.01–0.13 | 0.5262 |
| Physical Function Measures | |||||||
| Hand grip dominant average (kg) | 29.42 (9.08) | 15.15–53.60 | 26.54 (9.24) | 6.50–40.05 | 26.84 (8.26) | 9.70–42.00 | 0.3987 |
| Toe strength max average (kg) | 15.37 (5.62) | 3.10–26.80 | 15.92 (6.14) | 4.20–28.90 | 17.21 (5.14) | 8.60–29.10 | 0.2143 |
| Feet side-by-side (s) | 10.00 (0.00) | 10 | 10.00 (0.00) | 10 | 10.00 (0.00) | 10 | |
| Semi-Tandem stance (s) | 10.00 (0.00) | 10 | 10.00 (0.00) | 10 | 10.00 (0.00) | 10 | |
| Tandem stance (s) | 10.00 (0.00) | 10 | 10.00 (0.00) | 10 | 10.00 (0.00) | 10 | |
| One-leg stand max average (s) | 75.23 (40.89) | 10.59–120.00 | 84.84 (40.88) | 3.50–120.00 | 82.75 (44.94) | 7.00–120.00 | 0.4981 |
| FTSST (s) | 9.22 (2.93) | 5.50–18.10 | 8.65 (2.51) | 4.20–14.92 | 8.65 (2.57) | 4.80–14.90 | 0.4112 |
| Shoulder Flexion Active dominant (°) | 158.10 (12.85) | 115–175 | 163.00 (8.05) | 145–180 | 160.00 (9.16) | 145–180 | 0.1834 |
| Heel up (°) | 37.40 (4.77) | 26.57–50.19 | 38.65 (6.01) | 12.43–45.00 | 39.03 (3.58) | 29.36–46.02 | 0.4199 |
| Toe up (°) | 13.54 (4.95) | 3.81–25.64 | 13.88 (4.15) | 1.91–20.56 | 14.52 (3.88) | 4.16–21.16 | 0.6824 |
| Body Composition Measures | |||||||
| Body height (cm) | 166.13 (7.35) | 153.00–179.50 | 162.77 (9.00) | 146.40–179.00 | 164.09 (7.93) | 148.00–177.00 | 0.3427 |
| Body weight (kg) | 63.9 (12.90) | 42.30–96.00 | 60.62 (12.73) | 40.00–92.20 | 60.80 (10.07) | 41.80–78.70 | 0.3255 |
| Body muscle mass (kg) | 45.80 (8.29) | 34.10–68.90 | 43.25 (8.91) | 28.90–59.60 | 44.22 (7.10) | 32.20–58.20 | 0.4622 |
| Fat mass (kg) | 15.29 (6.36) | 3.70–35.2 | 14.73 (6.89) | 3.90–28.9 | 13.86 (5.07) | 4.50–24.60 | 0.3764 |
| Body ECW/TBW | 0.38 (0.01) | 0.37–0.39 | 0.38 (0.00) | 0.38–0.39 | 0.38 (0.01) | 0.37–0.40 | 0.5532 |
| Phase Angle | 5.23 (0.62) | 3.74–6.46 | 5.12 (0.52) | 4.23–6.16 | 5.12 (0.60) | 3.70–7.05 | 0.7242 |
| Protein (kg) | 9.52 (1.75) | 7.10–14.30 | 8.98 (1.87) | 6.00–12.3 | 9.20 (1.50) | 6.70–12.40 | 0.4733 |
| BMI (kg/m2) | 23.05 (3.68) | 15.80–31.80 | 22.74 (3.48) | 16.40–29.80 | 22.49 (3.06) | 17.20–28.90 | 0.5277 |
| SMI (kg/m2) | 7.33 (1.02) | 5.80–10.10 | 7.05 (1.10) | 5.40–9.00 | 7.13 (0.86) | 5.20–8.70 | 0.4733 |
| Criterion | Walking Group | Dance Group | Control Group | F Value | ANCOVA Permutation p-Value | Adjusted by FDR p-Value | Effect Size (η2) | Post hoc Scheffé Test | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 27) | (n = 30) | (n = 29) | Walking vs. Control p-Value (95% CI) | Dance vs. Control p-Value (95% CI) | Walking vs. Dance p-Value (95% CI) | ||||||||
| Mean | SD | Mean | SD | Mean | SD | ||||||||
| Cognitive Function Measures | |||||||||||||
| MoCA total score | 0.7037 | 1.9178 | 2.0667 | 1.8557 | −0.2414 | 2.1983 | 9.681 | 0.0000 | 0.0000 * | 0.19 | 0.1233 (2.4910–−0.2350) | 0.0000 (1.2007–3.4154) * | 0.0135 (−2.4910–−0.2350) * |
| Visuospatial/Executive | −0.0741 | 0.8738 | 0.5333 | 0.9371 | −0.2069 | 1.1765 | 4.518 | 0.0074 | 0.0280 * | 0.10 | 0.8413 (−0.4302–0.6958) | 0.0050 (0.1920–1.2885) * | 0.0296 (−1.1659–−0.0489) * |
| Naming | 0.0370 | 0.1925 | 0.0000 | 0.0000 | −0.0690 | 0.3714 | 3.088 | 0.0819 | 0.1455 | 0.07 | |||
| Attention | −0.1852 | 0.8338 | 0.3000 | 0.5350 | −0.2069 | 0.6750 | 2.875 | 0.0740 | 0.1398 | 0.07 | |||
| Language | 0.7037 | 0.9121 | 0.4333 | 1.1943 | 0.2069 | 0.7736 | 3.456 | 0.0040 | 0.0170 * | 0.08 | 0.0271 (0.0458–0.9478) * | 0.4411 (−0.2128–0.6656) | 0.3262 (−0.1770–0.7178) |
| Abstraction | 0.0370 | 0.6493 | 0.2000 | 0.4842 | 0.1379 | 0.4411 | 1.599 | 0.1965 | 0.2784 | 0.04 | |||
| Delayed Recall | 0.1852 | 1.0014 | 0.3667 | 0.6687 | 0.2414 | 0.9124 | 1.903 | 0.0856 | 0.1455 | 0.05 | |||
| Orientation | 0.0000 | 0.3922 | 0.0667 | 0.3651 | −0.3103 | 0.6603 | 3.521 | 0.0138 | 0.0427 * | 0.08 | 0.0256 (0.0309–0.5897) * | 0.0038 (0.1049–0.6491) * | 0.8356 (−0.3438–0.2105) |
| FAB total score | 0.2963 | 1.0309 | 0.7333 | 1.5522 | −0.5862 | 1.6801 | 7.211 | 0.0004 | 0.0034 * | 0.15 | 0.0369 (0.0432–−1.7218) * | 0.0006 (0.5022–−2.1369) * | 0.4282 (−1.2600–0.3955) |
| Similarities (conceptualization) | 0.0741 | 0.6156 | 0.0000 | 0.8305 | 0.0000 | 0.4629 | 0.001 | 1.0000 | 1.0000 | 0.00 | |||
| Lexical Fluency (mental flexibility) | 0.0741 | 0.6752 | 0.1333 | 0.3457 | 0.0345 | 0.6805 | 1.450 | 0.1604 | 0.2371 | 0.03 | |||
| Motor Series (programming) | −0.2963 | 0.8689 | 0.0333 | 0.7184 | −0.2759 | 0.8822 | 3.175 | 0.0414 | 0.1005 | 0.07 | |||
| Conflicting Instructions (sensitivity to interference) | 0.1481 | 0.6624 | 0.2000 | 0.5509 | 0.0690 | 0.5299 | 1.353 | 0.4661 | 0.6052 | 0.03 | |||
| Go–No-Go (inhibitory control) | 0.2963 | 0.9929 | 0.3667 | 0.8503 | −0.4138 | 1.1807 | 4.672 | 0.0128 | 0.0427 * | 0.10 | 0.0060 (0.1736–1.2466) * | 0.0017 (0.2580–1.3029) * | 0.9471 (−0.6025–0.4618) |
| Prehension Behavior (environmental autonomy) | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.2673 | 0.996 | 0.8945 | 0.9811 | 0.02 | |||
| Mood State Measures | |||||||||||||
| GDS score | −0.1481 | 1.5116 | −1.0000 | 1.7019 | −0.5862 | 1.5004 | 0.625 | 0.6154 | 0.7215 | 0.02 | |||
| WHO-QOL score | 0.0370 | 5.9387 | 2.4667 | 8.5772 | −1.8966 | 4.9594 | 2.849 | 0.0282 | 0.0799 † | 0.07 | 0.5388 (−2.3865–6.2537) | 0.0402 (0.1564–8.570) * | 0.3724 (−6.7149–1.8556) |
| Imitation | |||||||||||||
| Imitation gesture total score | 1.5556 | 2.4859 | −0.6333 | 2.0424 | 0.5517 | 2.8609 | 2.849 | 0.0000 | 0.0000 * | 0.23 | 0.1834 (−0.3412–2.3489) | 0.0847 (−2.4948–0.1247) | 0.0005 (0.8547–3.5231) * |
| Gait | |||||||||||||
| Fast gait speed 10 m (s) | −0.0200 | 0.7200 | −0.5450 | 0.5807 | −0.3066 | 0.5805 | 4.760 | 0.0036 | 0.0170 * | 0.11 | 0.1820 (−0.0958–0.6637) | 0.2798 (0.6082–0.1313) | 0.0038 (0.1457–0.8991) * |
| Step (cm) | −2.0704 | 12.5372 | −1.9967 | 10.5704 | −1.0483 | 13.2590 | 0.075 | 1.0000 | 1.0000 | 0.00 | |||
| RMS (1/m) | −0.0304 | 0.2789 | −0.2048 | 0.3577 | −0.2384 | 0.4310 | 0.198 | 0.1257 | 0.1943 | 0.04 | |||
| Walking cycles | −0.0128 | 0.0459 | 0.0125 | 0.0403 | 0.0106 | 0.0389 | 2.902 | 0.0322 | 0.0842 † | 0.07 | 0.0132 (−0.0426–−0.0041) * | 0.9658 (−0.0168–0.0207) | 0.0059 (−0.0444–−0.0062) * |
| Motor Function Measures | |||||||||||||
| Hand grip dominant average (kg) | 0.5574 | 4.5520 | 1.8067 | 6.7980 | 0.6069 | 3.2131 | 1.951 | 0.0511 | 0.1086 | 0.06 | |||
| Toe strength max average (kg) | 2.7600 | 3.1700 | 2.1700 | 3.9100 | 1.9500 | 2.9300 | 0.446 | 0.4904 | 0.6052 | 0.01 | |||
| One-leg stand max average (s) | 19.6600 | 29.2000 | 9.0700 | 22.8000 | 3.4400 | 14.0200 | 6.935 | 0.0006 | 0.0041 * | 0.08 | 0.0186 (2.2494–30.1941) * | 0.5892 (−7.9775–19.2341) | 0.1690 (−3.2662–24.4531) |
| FTSST (s) | −0.0226 | 0.7199 | −2.5300 | 2.1900 | −1.6200 | 2.0700 | 3.100 | 0.0568 | 0.1136 | 0.07 | |||
| Shoulder Flexion Active dominant (°) | 5.7407 | 12.3805 | 5.0000 | 8.9056 | 1.5517 | 7.0841 | 1.662 | 0.1214 | 0.1943 | 0.04 | |||
| Heel Lift (°) | 1.6825 | 2.9691 | 2.1503 | 5.3196 | −0.5263 | 2.2597 | 5.904 | 0.0000 | 0.0000 * | 0.13 | 0.0083 (0.4832–3.9343) * | 0.0008 (0.9963–4.3569) * | 0.7930 (−2.1795–1.2438) |
| Toe Lift (°) | 1.3790 | 3.9333 | 2.7775 | 3.7821 | 0.4742 | 4.0792 | 2.805 | 0.0490 | 0.1086 | 0.07 | |||
| Body Composition Measures | |||||||||||||
| Body weight (kg) | −0.0667 | 1.1774 | 0.1533 | 0.7592 | 0.1069 | 0.8242 | 0.457 | 0.9263 | 0.9842 | 0.01 | |||
| Body muscle mass (kg) | −0.5370 | 1.2013 | −0.1833 | 0.7391 | −0.2276 | 0.9640 | 1.065 | 0.2898 | 0.3941 | 0.03 | |||
| Fat mass (kg) | 0.4630 | 1.2564 | 0.3067 | 0.8354 | 0.3414 | 0.8060 | 0.565 | 0.8916 | 0.9811 | 0.01 | |||
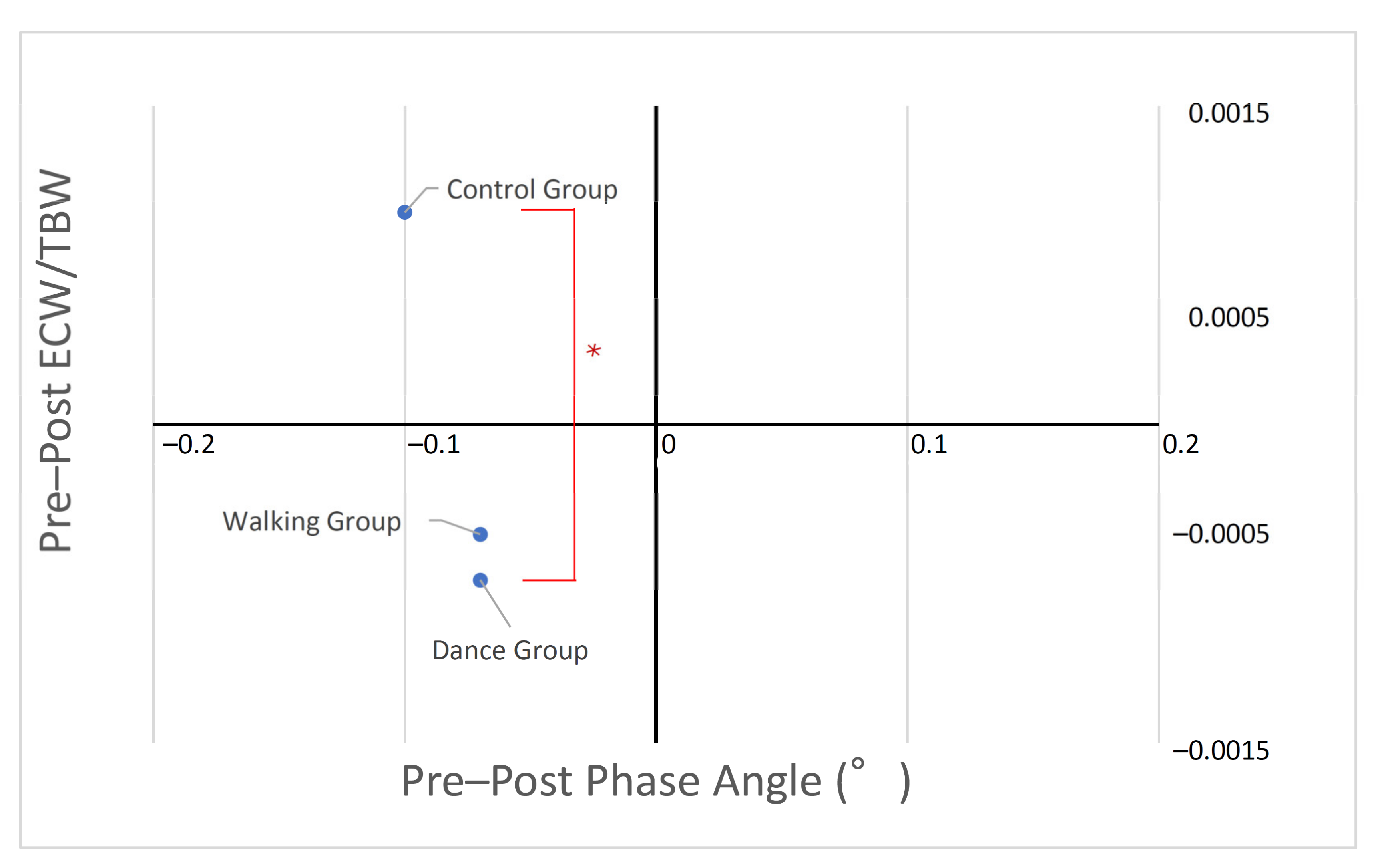
| Body ECW/TBW | −0.0005 | 0.0025 | −0.0007 | 0.0028 | 0.0010 | 0.0025 | 4.658 | 0.0010 | 0.0057 * | 0.11 | 0.0859 (−0.0032–0.0001) | 0.0356 (−0.0034–−0.0001) * | 0.9498 (−0.0015–0.0019) |
| Phase Angle (°) | −0.0700 | 0.2000 | −0.0700 | 0.3300 | −0.1000 | 0.2800 | 0.565 | 0.4984 | 0.6052 | 0.01 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyazaki, A.; Okuyama, T.; Mori, H.; Sato, K.; Kumamoto, K.; Hiyama, A. Effects of Two Short-Term Aerobic Exercises on Cognitive Function in Healthy Older Adults during COVID-19 Confinement in Japan: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 6202. https://doi.org/10.3390/ijerph19106202
Miyazaki A, Okuyama T, Mori H, Sato K, Kumamoto K, Hiyama A. Effects of Two Short-Term Aerobic Exercises on Cognitive Function in Healthy Older Adults during COVID-19 Confinement in Japan: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(10):6202. https://doi.org/10.3390/ijerph19106202
Chicago/Turabian StyleMiyazaki, Atsuko, Takashi Okuyama, Hayato Mori, Kazuhisa Sato, Keigo Kumamoto, and Atsushi Hiyama. 2022. "Effects of Two Short-Term Aerobic Exercises on Cognitive Function in Healthy Older Adults during COVID-19 Confinement in Japan: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 10: 6202. https://doi.org/10.3390/ijerph19106202