sFlt-1 Is an Independent Predictor of Adverse Maternal Outcomes in Women With SARS-CoV-2 Infection and Hypertensive Disorders of Pregnancy
 Jose Antonio Hernandez-Pacheco1,2†
Jose Antonio Hernandez-Pacheco1,2†  Johnatan Torres-Torres1,3,4†
Johnatan Torres-Torres1,3,4†  Raigam Jafet Martinez-Portilla1,4 Juan Mario Solis-Paredes1
Raigam Jafet Martinez-Portilla1,4 Juan Mario Solis-Paredes1  Guadalupe Estrada-Gutierrez1
Guadalupe Estrada-Gutierrez1  Paloma Mateu-Rogell1,4,5 Miguel Angel Nares-Torices1 Mario Enmanuel Lopez-Marenco1 Keren Rachel Escobedo-Segura3 Alejandro Posadas-Nava3 Jose Rafael Villafan-Bernal4,6 Lourdes Rojas-Zepeda4,7 Norma Patricia Becerra-Navarro2 Manuel Casillas-Barrera2 Mauricio Pichardo-Cuevas2
Paloma Mateu-Rogell1,4,5 Miguel Angel Nares-Torices1 Mario Enmanuel Lopez-Marenco1 Keren Rachel Escobedo-Segura3 Alejandro Posadas-Nava3 Jose Rafael Villafan-Bernal4,6 Lourdes Rojas-Zepeda4,7 Norma Patricia Becerra-Navarro2 Manuel Casillas-Barrera2 Mauricio Pichardo-Cuevas2  Cinthya Muñoz-Manrique1,4 Ivan Alonso Cortes-Ramirez2
Cinthya Muñoz-Manrique1,4 Ivan Alonso Cortes-Ramirez2  Salvador Espino-y-Sosa1,4*
Salvador Espino-y-Sosa1,4*- 1Clinical Research Branch, Instituto Nacional de Perinatología Isidro Espinosa de los Reyes, Mexico City, Mexico
- 2Hospital de la Mujer, Mexico City, Mexico
- 3Hospital General de Mexico Dr. Eduardo Liceaga, Mexico City, Mexico
- 4Iberoamerican Research Network in Obstetrics, Gynecology and Translational Medicine, Mexico City, Mexico
- 5Centro de Investigación en Ciencias de la Salud, FCS, Universidad Anahuac México Campus Norte, Huixquilucan, Mexico
- 6Laboratory of Immunogenomics and Metabolic Diseases, Instituto Nacional de Medicina Genomica, Mexico City, Mexico
- 7Maternal Fetal Medicine Department, Instituto Materno Infantil del Estado de Mexico, Toluca, Mexico
Background: Preeclampsia (PE) and COVID-19 share a common vascular–endothelial physiopathological pathway that may aggravate or worsen women's outcomes when both coexist. This study aims to evaluate the association of sFlt-1 levels and adverse maternal outcomes among positive SARS-CoV-2 pregnant women with and without hypertensive disorders of pregnancy (HDP).
Methods: We performed a multicenter retrospective cohort study of pregnant women with confirmed SARS-CoV-2 infection that required hospital admission. The exposed cohort comprised women with a diagnosis of an HDP. The primary outcome was a composite definition of adverse maternal outcome. The association between predictors and the main and secondary outcomes was assessed using an elastic-net regression which comprised a Lasso and Ridge regression method for automatic variable selection and penalization of non-statistically significant coefficients using a 10-fold cross-validation where the best model if automatically chosen by the lowest Akaike information criterion (AIC) and Bayesian information criteria (BIC).
Results: Among 148 pregnant women with COVID-19, the best predictive model comprised sFlt-1 MoMs [odds ratio (OR): 5.13; 95% CI: 2.19–12.05], and HDP (OR: 32.76; 95% CI: 5.24–205). sFlt-1 MoMs were independently associated with an increased probability of an adverse maternal outcome despite adjusting for HDP.
Conclusions: Our study shows that sFlt-1 is an independent predictor of adverse outcomes in women with SARS-CoV-2 despite hypertension status.
Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (1). Pregnant women have a higher risk of severe COVID-19 (2, 3) caused by higher levels of inflammatory markers (IL-6, TNF-alpha, IFN-gamma, etc.), hypertension, oxidative stress, and thrombotic events causing multiorgan and placental damage with adverse outcomes for the mother and the developing fetus (4–7). Preeclampsia (PE) is defined as hypertension and proteinuria that debuts after 20 weeks gestation (8); its physiopathological pathway is similar to that of COVID-19, with an exaggerated inflammatory response that leads to endothelial damage and cytokine release from mesenchymal stromal cells of preeclamptic placentas (9, 10). SARS-CoV-2 infection is a significant risk factor for preeclampsia in pregnancy. In the participating hospitals, a substantial increase in preeclampsia is observed among women with pregnancy complicated by SARS-CoV-2 infection compared to women with a negative test (National Institute of Perinatology: 18 vs. 9%, General Hospital of Mexico: 12 vs. 5%). At a molecular level, there is an interaction between COVID-19 and PE, characterized by altered levels of angiogenic markers soluble fms-like tyrosine kinase (sFlt-1) and placental growth factor (PlGF) and higher sFlt-1/PlGF ratio (6, 11–13). Serum sFlt-1 is an antiangiogenic protein released from many tissues that antagonizes serum PlGF and vascular endothelial growth factor [VEGF, promoting endothelial dysfunction (14)]. Thus, PE and COVID-19 share a vascular–endothelial physiopathological pathway that may aggravate or worsen women's outcomes when both coexist. We hypothesize that this synergic effect is exemplified in sFlt-1 levels among PE and COVID-19 and that there may be an interaction between hypertensive disorders of pregnancy (HDP), COVID-19, and sFlt-1 levels that is reflected in the incidence of adverse maternal outcomes (15). Therefore, this study aims to evaluate the association between sFlt-1 levels and adverse maternal outcomes among positive SARS-CoV-2 pregnant women controlled by HDP.
Methods
Study Design and Participants
This is a multicenter retrospective cohort study of pregnant women with confirmed SARS-CoV-2 infection that required hospital admission at the Instituto Nacional de Perinatologia Isidro Espinosa de los Reyes, the Hospital de la Mujer, and the Hospital General de Mexico Dr. Eduardo Liceaga. All women with a confirmed SARS-CoV-2 infection by RT-qPCR test that required hospital admission were included. The exposed cohort comprised women with a diagnosis of an HDP that included preeclampsia, eclampsia, and HELLP syndrome according to ACOG criteria (16), between October 2020 and December 2021. Controls were those hospitalized SARS-CoV-2 pregnant women without hypertension in pregnant. The protocol was approved by the Ethics and Research Internal Review Board of the National Institute of Perinatology (2020-1-32) and was conducted ethically under the World Medical Association Declaration of Helsinki. All enrolled women authorized and provided signed informed consent.
Data Collection
The following data were collected from the medical records: age, gestational age at admission, pregestational body mass index (pBMI) (kg/m2), mean arterial pressure (MAP) at admission, and history of previous diseases such as chronic hypertension, pre-gestational diabetes, preeclampsia, and pneumonia. Participants' blood samples were obtained at hospital admission as routine testing, and laboratory results were obtained: platelets, aspartate aminotransferase (AST), alanine aminotransferase (ALT). The blood sample for sFlt-1 and PlGF measurements was also drawn at admission. The time between SARS-CoV-2 diagnosis and hospital discharge.
Measurement of Angiogenic Markers sFlt-1 and PlGF
A blood sample was drawn and immediately centrifuged (1,000 × g/10 min), plasma was aliquoted and stored at −70°C until analysis. Then, the plasma concentration of angiogenic markers PlGF (Elecsys PlGF, Roche®) and sFlt-1 (Elecsys sFlt-1, Roche®) were quantified by electrochemiluminescence using an automated analyzer (Cobas-e411, Roche®) according to the manufacturer's instructions. Biomarkers were log-transformed and converted to their multiples of the median (MoM) (17, 18) according to the Fetal Medicine Foundation algorithms (19).
Outcomes
We constructed a composite endpoint of adverse maternal outcomes that comprised any of the following: (1) Pneumonia (according to the American Thoracic Society criteria). (2) Acute kidney disease is defined as a 50% increase in serum creatinine (sCr) concentration over baseline or a 0.3 mg/dL increase from the lowest value within 48 h or oliguria, which corresponds to KDIGO (Kidney Disease: Improving Global Outcomes) stage 1 AKI or higher (20). The baseline sCr level was defined as the lowest sCr measurement within the previous 7 days or the median of all outpatient sCr values obtained within 7–365 days before hospitalization (21, 22). (3) Multiple organ failure (defined as the alteration of two or more organs with a score of ≥3 according to Sequential Organ Failure Assessment (SOFA) Score) (23). (4) Maternal sepsis (defined as the presence of suspected or confirmed infection plus signs of mild to moderate organ dysfunction (e.g., tachycardia, low blood pressure, tachypnoea, altered mental status, reduced urinary output) (24). (5) Maternal death, (6) preterm rupture of membranes, or (7) threatened preterm labor. The secondary outcome was the composite of adverse fetal and neonatal outcomes that comprised the following: prematurity, small-for-gestational-age neonate, fetal growth restriction, cesarean section due to fetal distress, low Apgar score, Grade IV intraventricular hemorrhage, respiratory distress syndrome, neonatal sepsis, neonatal death, admission to the neonatal intensive care unit.
Statistical Analysis
Groups were divided into an exposed and non-exposed cohort. Continuous variables were analyzed using the U-Mann Whitney test and expressed as the median and interquartile range (IQR); categorical data were analyzed using Chi-square or Fisher's exact test and expressed as number and percentage. The association between predictors and the primary and secondary outcomes was assessed using an elastic-net regression comprised of Lasso and Ridge regression for automatic variable selection and penalization of non-statistically significant coefficients using 10-fold cross-validation. The best model is automatically chosen by the lowest Akaike information criterion (AIC) and Bayesian information criteria (BIC). Predictive probabilities of an adverse outcome were calculated for the multivariate model adjusted by possible confounders selected by the elastic-net regression using the interaction between sFlt-1 concentration and hypertensive disorders of pregnancy (HDP) in a full factorial model for graph purposes. P-values <0.05 were considered statistically significant. (StataCorp. 2020. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC.).
Results
Description of the Cohort and Characteristics of the Study Population
One hundred forty-eight women with a positive RT-qPCR test for SARS-CoV-2 infection admitted to the hospital were included, of which 56 (37.8%) had an HDP. The mean maternal age was 30 (range: 15–45) years. When we compared by high blood pressure group in pregnancy, there were significant differences in mean arterial pressure (MAP), platelet count, ALT, AST, troponin, myoglobin, sFlt-1 MoMs, and sFlt/PlGF ratio (Table 1). Women with HDP had a higher incidence of pneumonia, acute kidney injury, lower birth weight, and a composite of adverse maternal outcomes (Table 2).
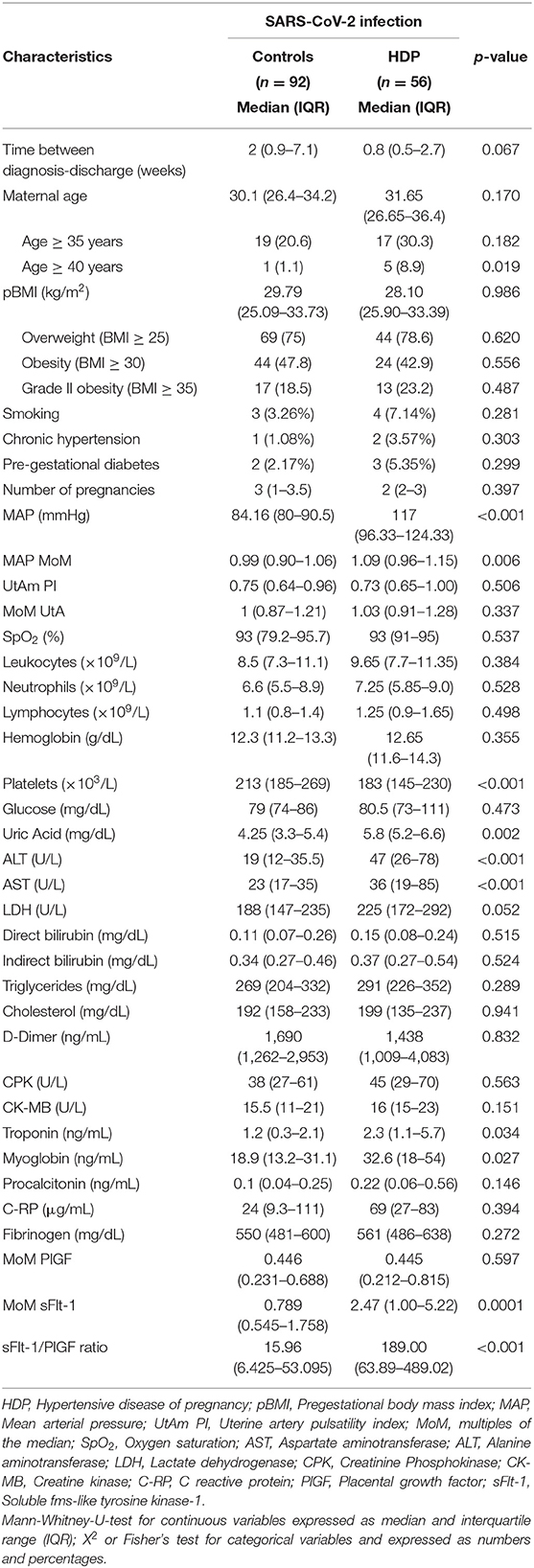
Table 1. Characteristics of the included population.
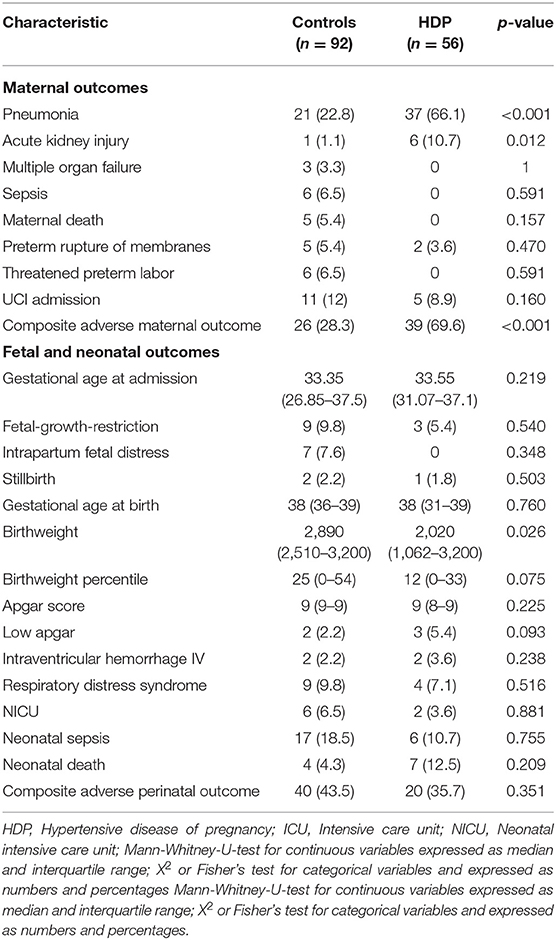
Table 2. Maternal, fetal, and neonate outcomes for SARS-CoV-2 participants.
Association Between sFlt-1 and Composite Adverse Maternal Outcomes
According to AIC and BIC criteria, the best predictive model comprised sFlt-1 MoMs, HDP, ALT values, MAP, and sFlt-1/PlGF ratio (Table 3). After adjusting for each other, sFlt-1 MoM, HDP, the interaction between sFlt-1 MoM/HDP, and MAP were the only significant predictors of a composite of adverse maternal outcomes (Naeguelkerke R2: 0.42).
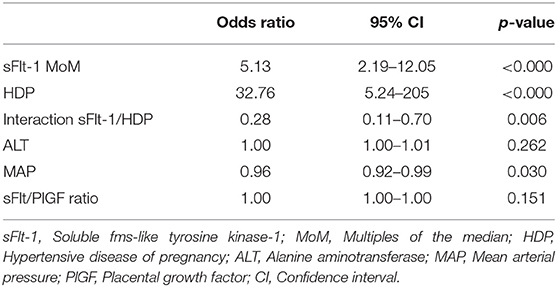
Table 3. Multivariate factorial model for adverse maternal outcome.
We observed a different correlation between sFlt-1 and AMO probability when comparing HDP and control groups. At low concentrations of sFlt-1, we found a significantly different risk for adverse maternal outcomes between the study groups (at 0.4 MoMs, 9 vs. 58%), as sFlt-1 concentrations increase, the difference in the probability of AMO decreases between groups; this equals at 2.8 multiples of the median (75%). Higher levels of sFlt-1 were independently associated with an increased probability of adverse maternal outcomes in both groups, but, as shown in Figure 1, the predictive capability is better in women without HDP as in this group a significant increase in the probability of adverse events as sFlt-1 levels increase (from 9% at 0.4 MoMs to 80% at 3 MoMs). This is not the case in women with HDP in whom the risk for adverse events is slightly increased as marker concentrations increase (from 59% at 0.4 MoMs to 77% at 3 MoMs). While in the group of patients with HDP the concentration of sFlt-1 does not adequately discriminate the risk of adverse maternal events, in the group of women without HDP its usefulness in identifying this risk is notable (Figure 1).
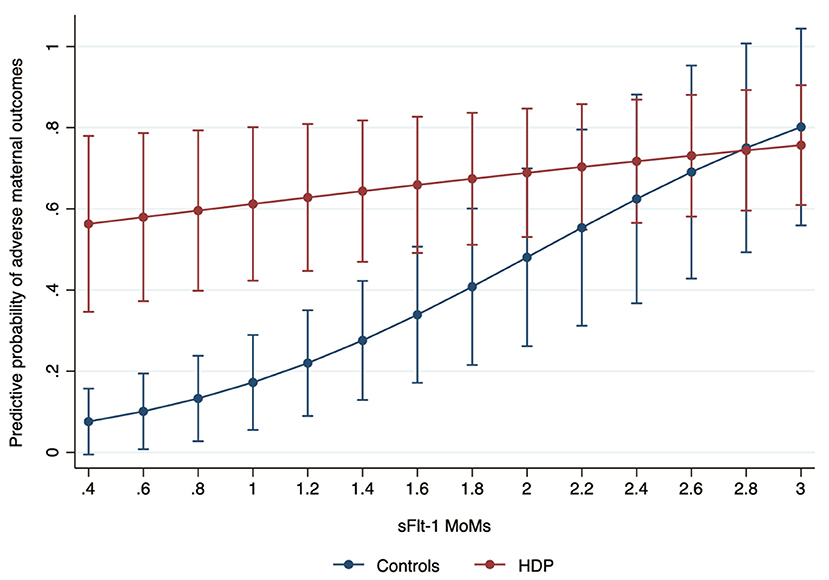
Figure 1. Predictive probability of an adverse maternal outcome among women with hypertensive disease of pregnancy (HDP) according to sFlt-1 MoM levels.
Discussion
Main Findings
The main finding of this study is that sFlt-1 is an independent predictor of adverse maternal outcomes after adjusting for confounders. Also, the probability of an adverse outcome increases as sFlt-1 MoM levels increase in women without HDP.
Comparison With Existing Literature
Several studies have shown an additive adverse effect when COVID-19 and PE coexist (25–27). A recent meta-analysis described that SARS-CoV-2 infection during pregnancy increases the risk of preeclampsia (28).
In preeclamptic women, sFlt-1 levels and sFlt-1/PlGF ratio are higher in complications, such as pulmonary edema, acute renal failure, cerebral hemorrhage, and stillbirth (29, 30). In the present study, we found that pregnant patients complicated with SARS-CoV-2 infection-related hypertensive disorders of pregnancy have higher plasma levels of sFlt-1 than SARS-CoV-2 infection without HDP. SARS-CoV-2 infection initiates in the upper respiratory tract, using the transmembrane protein ACE-2 of host cells (31). However, the kidney, liver, heart, and placenta also express the ACE-2 protein (32). The viral components within endothelium and accumulation of inflammatory cells may lead to multi-organic endothelitis, because of excessive host response (11, 33–36).
In our population, SARS-CoV-2 infection is an independent inflammation factor, added to the pre-existing due to preeclampsia; the significant increases in sFlt-1 concentrations can explain this compared with women with SARS-CoV-2 infection without preeclampsia. Previously, we suggested that interaction between viral spike protein (S) of SARS-CoV-2 and ACE-2 reduces ACE-2 levels in the cell membrane and generates an imbalance of Ang-II/Ang1-7, causing acute hypoxia, which induction and overproduction of sFlt-1, leading to systemic endothelial damage (15, 37).
We suggest that increased sFlt-1 levels in our patients are due to the synthesis by other organs and tissues than the placenta, and the rising of complications in pregnancy patients positive for SARS-CoV-2 and hypertensive disorders; this can be explained by the presence of ACE-2 receptors in kidney, facilitating invasion and viral replication, that culminate in a direct injury, and increased proteinuria. So, upregulating ACE-2 expression in hepatocytes and the cholangiocytes leads to elevated liver enzymes (38, 39). This study provides new evidence that sFtl-1 is an independent marker of adverse maternal outcomes in women with COVID-19 after adjusting for hypertension in pregnancy.
Strengths and Limitations of Study
The strengths of our study were that COVID-19 cases were consecutively recruited in a study with a specialized database built for research purposes, minimizing potential biases. In addition, baseline clinical characteristics between pregnant women with HDP and non-HDP were similar, diminishing the probability of selection bias.
Although sFlt-1 MoM has good performance in providing a short-term prediction of adverse maternal outcomes, the results need clinical validation in independent cohorts. Further evaluation of a risk cut-off for adverse maternal outcomes should be implemented in prospective cohorts.
Clinical Interpretation
sFlt-1 levels could be used as a routine marker for all women with COVID-19 without hypertension at hospital admission. The risk of adverse maternal outcomes remains high among women with HDP complicated with COVID-19 and this justifies closer monitoring; surveillance should be implemented also in women with higher levels of sFlt-1 that do not present HDP at admission. A risk calculator could be helpful in the initial selection of women with COVID-19 to standardize conduct (Supplementary Material), while women with HDP should always be closely monitorized because of their higher risk for adverse events due to the interaction between hypertension and COVID-19.
Conclusion
Our study shows that sFlt-1 is an independent predictor of adverse outcomes in women with SARS-CoV-2 despite hypertension status.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics and Research Internal Review Board of the National Institute of Perinatology (2020-1-32). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SE-y-S, JH-P, JT-T, and RM-P: study conception and design. PM-R, MN-T, ML-M, KE-S, NB-N, IC-R, MC-B, and MP-C: data collection. RM-P, GE-G, JV-B, and CM-M: analysis and interpretation of results. LR-Z and RM-P: statistical analysis. JH-P, JT-T, and SE-y-S: draft manuscript preparation. JS-P and AP-N: molecular studies. SE-y-S: oversight and leadership responsibility for the research activity planning and execution. JH-P and JT-T: management and coordination responsibility for the research activity planning and execution. All authors: reviewed the results and approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.894633/full#supplementary-material
References
1. Peepal P, Rath TS, Nayak S, Pendyala S. Maternal and neonatal outcomes among women with and without severe acute respiratory syndrome corona virus-2 infection: a retrospective analytical study. J Mother Child. (2022). 25:77–85. doi: 10.34763/jmotherandchild.20212502.d-21-00021
2. Martinez-Portilla RJ, Sotiriadis A, Chatzakis C, Torres-Torres J, Espino Y, Sosa S, et al. Pregnant women with SARS-CoV-2 infection are at higher risk of death and pneumonia: propensity score matched analysis of a nationwide prospective cohort (COV19Mx). Ultrasound Obstet Gynecol. (2021) 57:224–31. doi: 10.1002/uog.23575
3. Torres-Torres J, Martinez-Portilla RJ, Espino YSS, Estrada-Gutierrez G, Solis-Paredes JM, Villafan-Bernal JR, et al. Comorbidity, poverty and social vulnerability as risk factors for mortality in pregnant women with confirmed SARS-CoV-2 infection: analysis of 13 062 positive pregnancies including 176 maternal deaths in Mexico. Ultrasound Obstet Gynecol. (2022) 59:76–82. doi: 10.1002/uog.24797
4. Huntley BJF, Mulder IA, Di Mascio D, Vintzileos WS, Vintzileos AM, Berghella V, et al. Adverse pregnancy outcomes among individuals with and without severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): a systematic review and meta-analysis. Obstet Gynecol. (2021) 137:585–96. doi: 10.1097/AOG.0000000000004320
5. Wei SQ, Bilodeau-Bertrand M, Liu S, Auger N. The impact of COVID-19 on pregnancy outcomes: a systematic review and meta-analysis. CMAJ. (2021) 193:E540–E8. doi: 10.1503/cmaj.202604
6. Agostinis C, Mangogna A, Balduit A, Aghamajidi A, Ricci G, Kishore U, et al. COVID-19, pre-eclampsia, and complement system. Front Immunol. (2021) 12:775168. doi: 10.3389/fimmu.2021.775168
7. Marín R, Pujol FH, Rojas D, Sobrevia L. SARS- CoV-2 infection and oxidative stress in early-onset preeclampsia. Biochim Biophys Acta Mol Basis Dis. (2022) 1868:166321. doi: 10.1016/j.bbadis.2021.166321
8. Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S, et al. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. (2018) 13:291–310. doi: 10.1016/j.preghy.2018.05.004
9. Jayaram A, Buhimschi IA, Aldasoqi H, Hartwig J, Owens T, Elam GL, et al. Who said differentiating preeclampsia from COVID-19 infection was easy? Pregnancy Hypertens. (2021). 6:8–10. doi: 10.1016/j.preghy.2021.07.248
10. Todros T, Masturzo B, De Francia S. COVID-19 infection: ACE2, pregnancy and preeclampsia. Eur J Obstet Gynecol Reprod Biol. (2020) 253:330. doi: 10.1016/j.ejogrb.2020.08.007
11. Dupont V, Kanagaratnam L, Goury A, Poitevin G, Bard M, Julien G, et al. Excess soluble fms-like tyrosine kinase 1 correlates with endothelial dysfunction and organ failure in critically ill coronavirus disease 2019. Patients Clin Infect Dis. (2021) 72:1834–7. doi: 10.1093/cid/ciaa1007
12. Phoswa WN, Khaliq OP. The role of oxidative stress in hypertensive disorders of pregnancy (preeclampsia, gestational hypertension) and metabolic disorder of pregnancy (gestational diabetes mellitus). Oxid Med Cell Longev. (2021) 2021:5581570. doi: 10.1155/2021/5581570
13. Soldavini CM, Di Martino D, Sabattini E, Ornaghi S, Sterpi V, Erra R, et al. sFlt-1/PlGF ratio in hypertensive disorders of pregnancy in patients affected by COVID-19. Pregnancy Hypertens. (2022) 27:103–9. doi: 10.1016/j.preghy.2021.12.001
14. Zeisler H, Llurba E, Chantraine F, Vatish M, Staff AC, Sennström M, et al. Predictive value of the sFlt-1:PlGF ratio in women with suspected preeclampsia. N Engl J Med. (2016) 374:13–22. doi: 10.1056/NEJMoa1414838
15. Torres-Torres J, Espino-Y-Sosa S, Poon LC, Solis-Paredes JM, Estrada-Gutierrez G, Espejel-Nuñez A, et al. Increased levels of soluble fms-like tyrosine kinase-1 are associated with adverse outcomes in pregnant women with COVID-19. Ultrasound Obstet Gynecol. (2022) 59:202–8. doi: 10.1002/uog.24798
16. Gestational hypertension and preeclampsia: ACOG practice bulletin number 222. Obstet Gynecol. (2020) 135:e237–60. doi: 10.1097/AOG.0000000000003891
17. Tsiakkas A, Duvdevani N, Wright A, Wright D, Nicolaides KH. Serum soluble fms-like tyrosine kinase-1 in the three trimesters of pregnancy: effects of maternal characteristics and medical history. Ultrasound Obstet Gynecol. (2015) 45:584–90. doi: 10.1002/uog.14817
18. Tsiakkas A, Duvdevani N, Wright A, Wright D, Nicolaides KH. Serum placental growth factor in the three trimesters of pregnancy: effects of maternal characteristics and medical history. Ultrasound Obstet Gynecol. (2015) 45:591–8. doi: 10.1002/uog.14811
19. Calculation of MoMs. Available online at: https://fetalmedicine.org/research/mom (accessed February 15, 2022).
20. Walther CP, Podoll AS, Finkel KW. Summary of clinical practice guidelines for acute kidney injury. Hosp Pract 1995. (2014) 42:7–14. doi: 10.3810/hp.2014.02.1086
21. Hoste EAJ, Kellum JA, Selby NM, Zarbock A, Palevsky PM, Bagshaw SM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. (2018) 14:607–25. doi: 10.1038/s41581-018-0052-0
22. Ostermann M, Bellomo R, Burdmann EA, Doi K, Endre ZH, Goldstein SL, et al. Controversies in acute kidney injury: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. (2020) 98:294–309. doi: 10.1016/j.kint.2020.04.020
23. Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. (2019) 23:374. doi: 10.1186/s13054-019-2663-7
24. World Health Organization. Statement on Maternal Sepsis Sepsis: A Leading Cause of Maternal Deaths. Geneva: World Health Organization (2017).
25. Mendoza M, Garcia-Ruiz I, Maiz N, Rodo C, Garcia-Manau P, Serrano B, et al. Pre-eclampsia-like syndrome induced by severe COVID-19: a prospective observational study. Bjog. (2020) 127:1374–80. doi: 10.1111/1471-0528.16339
26. Nolan JP, Monsieurs KG, Bossaert L, Böttiger BW, Greif R, Lott C, et al. European Resuscitation Council COVID-19 guidelines executive summary. Resuscitation. (2020) 153:45–55. doi: 10.1016/j.resuscitation.2020.06.001
27. Rolnik DL. Can COVID-19 in pregnancy cause pre-eclampsia? Bjog. (2020) 127:1381. doi: 10.1111/1471-0528.16369
28. Conde-Agudelo A, Romero R. SARS-CoV-2 infection during pregnancy and risk of preeclampsia: a systematic review and meta-analysis. Am J Obstet Gynecol. (2022) 226:68–89.e3. doi: 10.1016/j.ajog.2021.07.009
29. Herraiz I Llurba E Verlohren S Galindo A Spanish Spanish Group for the Study of Angiogenic Markers in Preeclampsi. Update on the diagnosis and prognosis of preeclampsia with the aid of the sFlt-1/ PlGF ratio in singleton pregnancies. Fetal Diagn Ther. (2018) 43:81–9. doi: 10.1159/000477903
30. Mirkovic L, Tulic I, Stankovic S, Soldatovic I. Prediction of adverse maternal outcomes of early severe preeclampsia. Pregnancy Hypertens. (2020) 22:144–50. doi: 10.1016/j.preghy.2020.09.009
31. Zamorano Cuervo N, Grandvaux N. ACE2: Evidence of role as entry receptor for SARS-CoV-2 and implications in comorbidities. Elife. (2020) 9:e61390. doi: 10.7554/eLife.61390
32. Ouyang Y, Bagalkot T, Fitzgerald W, Sadovsky E, Chu T, Martínez-Marchal A, et al. Term human placental trophoblasts express SARS-CoV-2 entry factors ACE2, TMPRSS2, and furin. mSphere. (2021) 6:1–14. doi: 10.1128/mSphere.00250-21
33. Shapiro NI, Schuetz P, Yano K, Sorasaki M, Parikh SM, Jones AE, et al. The association of endothelial cell signaling, severity of illness, and organ dysfunction in sepsis. Crit Care. (2010) 14:R182. doi: 10.1186/cc9290
34. Yano K, Liaw PC, Mullington JM, Shih S-C, Okada H, Bodyak N, et al. Vascular endothelial growth factor is an important determinant of sepsis morbidity and mortality. J Exp Med. (2006) 203:1447–58. doi: 10.1084/jem.20060375
35. Yoo S-A, Kim M, Kang M-C, Kong J-S, Kim K-M, Lee S, et al. Placental growth factor regulates the generation of T17 cells to link angiogenesis with autoimmunity. Nat Immunol. (2019) 20:1348–59. doi: 10.1038/s41590-019-0456-4
36. Torres-Torres J, Martinez-Portilla RJ, Espino YSS, Solis-Paredes JM, Hernández-Pacheco JA, Mateu-Rogell P, et al. Maternal death by COVID-19 associated with elevated troponin T levels. Viruses. (2022) 14:271. doi: 10.3390/v14020271
37. Espino-Y-Sosa S, Martinez-Portilla RJ, Torres-Torres J, Solis-Paredes JM, Estrada-Gutierrez G, Hernandez-Pacheco JA, et al. Novel ratio soluble fms-like tyrosine kinase-1/angiotensin-II (sFlt-1/ANG-II) in pregnant women is associated with critical illness in COVID-19. Viruses. (2021) 13:906. doi: 10.3390/v13101906
38. Mizuiri S, Ohashi Y. ACE and ACE2 in kidney disease. World J Nephrol. (2015) 4:74–82. doi: 10.5527/wjn.v4.i1.74
Keywords: endothelial dysfunction, preeclampsia, placental growth factor, soluble fms-like tyrosine kinase-1, SARS-CoV-2, COVID-19
Citation: Hernandez-Pacheco JA, Torres-Torres J, Martinez-Portilla RJ, Solis-Paredes JM, Estrada-Gutierrez G, Mateu-Rogell P, Nares-Torices MA, Lopez-Marenco ME, Escobedo-Segura KR, Posadas-Nava A, Villafan-Bernal JR, Rojas-Zepeda L, Becerra-Navarro NP, Casillas-Barrera M, Pichardo-Cuevas M, Muñoz-Manrique C, Cortes-Ramirez IA and Espino-y-Sosa S (2022) sFlt-1 Is an Independent Predictor of Adverse Maternal Outcomes in Women With SARS-CoV-2 Infection and Hypertensive Disorders of Pregnancy. Front. Med. 9:894633. doi: 10.3389/fmed.2022.894633
Received: 12 March 2022; Accepted: 31 March 2022;
Published: 09 May 2022.
Edited by:
Min Chen, The Third Affiliated Hospital of Guangzhou Medical University, ChinaReviewed by:
Mingming Zheng, Nanjing Drum Tower Hospital, ChinaXueyu Chen, Shenzhen Maternity and Child Healthcare Hospital, China
Copyright © 2022 Hernandez-Pacheco, Torres-Torres, Martinez-Portilla, Solis-Paredes, Estrada-Gutierrez, Mateu-Rogell, Nares-Torices, Lopez-Marenco, Escobedo-Segura, Posadas-Nava, Villafan-Bernal, Rojas-Zepeda, Becerra-Navarro, Casillas-Barrera, Pichardo-Cuevas, Muñoz-Manrique, Cortes-Ramirez and Espino-y-Sosa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Salvador Espino-y-Sosa, salvadorespino@gmail.com
†These authors have contributed equally to this work and share first authorship