
Suicidal Ideation and Predictors of Psychological Distress during the COVID-19 Pandemic in Eswatini: A Population-Based Household Telephone Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
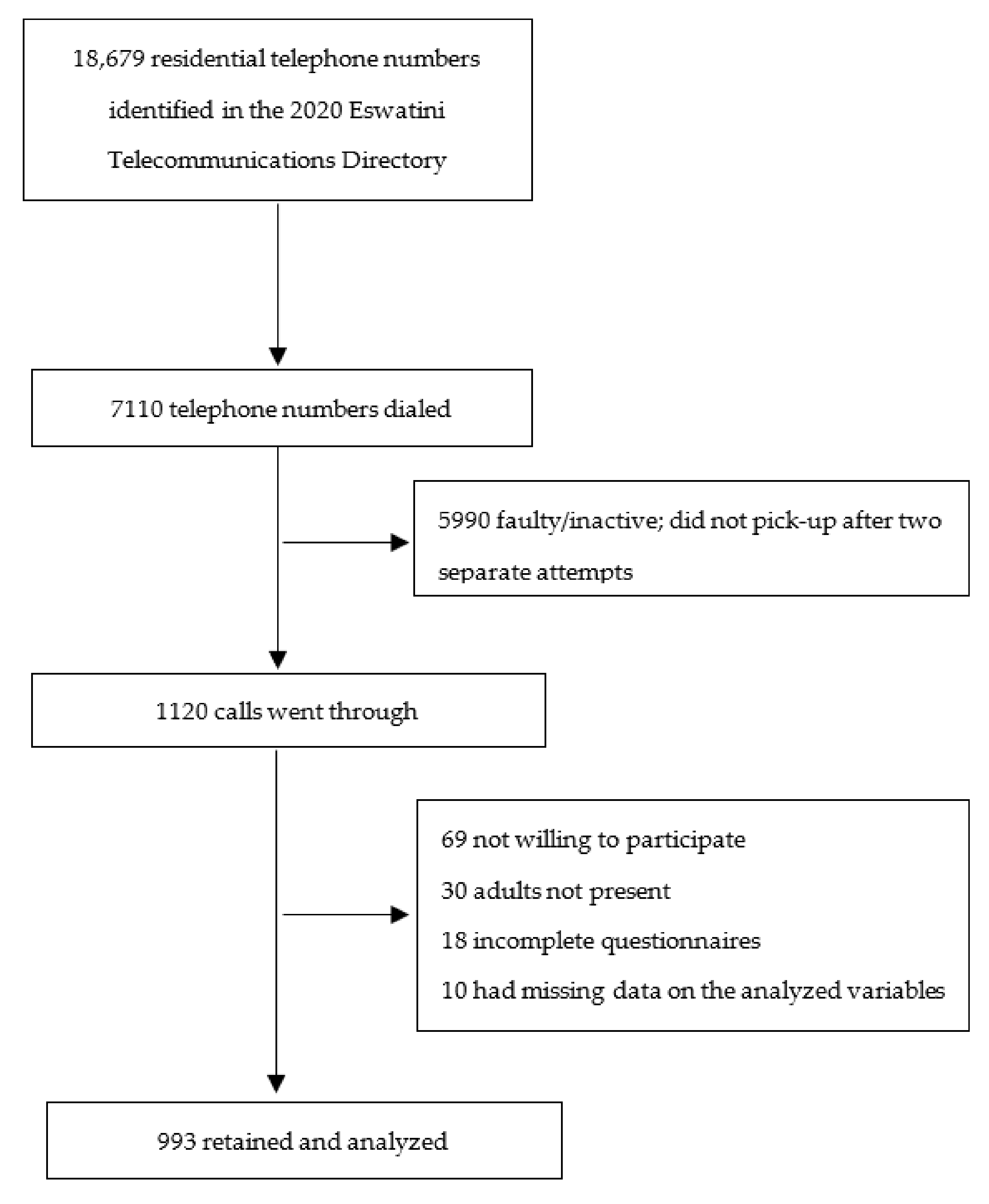
2.2. Study Population and Sampling Procedure
2.3. Sample Size Determination
2.4. Data Collection
2.5. Measures
2.5.1. Outcome Variables
2.5.2. Explanatory Variables
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
3.1. Sample Characteristics
3.2. Prevalence of Psychological Distress and Suicidal Ideation
3.3. Distribution of Participants’ Background Characteristics by Suicidal Ideation
3.4. Perceived COVID-19-Related Stressors
3.5. Predictors of Psychological Distress
3.5.1. Bivariate Analysis Results
3.5.2. Multivariate Analysis Results
3.5.3. Sensitivity Analysis Results
4. Discussion
4.1. Psychological Distress and Suicidal Ideation
4.2. COVID-19-Related Stressors
4.3. Predictors of Psychological Distress
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Health Emergency Dashboard. Coronavirus (COVID-19). Available online: https://covid19.who.int/ (accessed on 14 June 2021).
- Central Statistics Office. 2017 Population and Housing Census, Volume 3; Government of the Kingdom of Eswatini: Mbabane, Eswatini, 2019.
- Ministry of Health. COVID-19 Daily Update. Available online: https://www.facebook.com/EswatiniGov (accessed on 14 June 2021).
- John Hopkins University and Medicine Coronavirus Resource Center. Cases and Mortality by Country. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 15 May 2021).
- Sukati, S. Govt Stands by its Word on Lockdown Extension. Times of Eswatini. 9 March 2021. Available online: http://www.times.co.sz/news/132089-govt-stands-by-its-word-on-lockdown-extension.html (accessed on 7 February 2021).
- US CDC. Science Brief: Emerging SARS-CoV-2 Variants. Available online: https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/scientific-brief-emerging-variants.html (accessed on 16 March 2021).
- WHO. COVID-19 Disrupting Mental Health Services in Most Countries, WHO Survey. Available online: https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey (accessed on 25 April 2021).
- Yamamoto, T.; Uchiumi, C.; Suzuki, N.; Yoshimoto, J.; Murillo-Rodriguez, E. The psychological impact of ‘mild lockdown’ in Japan during the COVID-19 Pandemic: A nationwide survey under a declared state of emergency. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Dar, K.A.; Iqbal, N.; Mushtaq, A. Intolerance of uncertainty, depression, and anxiety: Examining the indirect and moderating effects of worry. Asian J. Psychiatry 2017, 29, 129–133. [Google Scholar] [CrossRef]
- Shah, S.M.A.; Mohammad, D.; Qureshi, M.F.H.; Abbas, M.Z.; Aleem, S. Prevalence, psychological responses and associated correlates of depression, anxiety and stress in a global population, during the Coronavirus Disease (COVID-19) pandemic. Community Ment. Health J. 2021, 57, 101–110. [Google Scholar] [CrossRef]
- Twenge, J.M.; Joiner, T.E. Mental distress among U.S. Adults during the COVID-19 pandemic. J. Clin. Psychol. 2020, 76, 2170–2182. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Olaseni, A.O.; Akinsola, O.S.; Agberotimi, S.F.; Oguntayo, R. Psychological distress experiences of Nigerians during Covid-19 pandemic; the gender difference. Soc. Sci. Humanit. Open 2020, 2, 100052. [Google Scholar] [CrossRef]
- Kim, A.W.; Nyengerai, T.; Mendenhall, E. Evaluating the mental health impacts of the COVID-19 pandemic: Perceived risk of COVID-19 infection and childhood trauma predict adult depressive symptoms in urban South Africa. Psychol. Med. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- WHO Afro. COVID-19 Halting Crucial Mental Health Services in Africa, WHO Survey. Available online: https://www.afro.who.int/news/covid-19-halting-crucial-mental-health-services-africa-who-survey (accessed on 12 March 2021).
- Bhuiyan, A.K.M.; Sakib, N.; Pakpour, A.; Griffiths, M.; Mamun, M. COVID-19-related suicides in Bangladesh due to lockdown and economic factors: Case study evidence. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed]
- Every-Palmer, S.; Jenkins, M.; Gendall, P.; Hoek, J.; Beaglehole, B.; Bell, C.; Williman, J.; Rapsey, C.; Stanley, J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLoS ONE 2020, 15, e0241658. [Google Scholar] [CrossRef]
- Yasir Arafat, S.M. Current challenges of suicide and future directions of management in Bangladesh: A systematic review. Glob. Psychiatry 2018, 2, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Turna, J.; Zhang, J.; Lamberti, N.; Patterson, B.; Simpson, W.; Francisco, A.P.; Bergmann, C.G.; Ameringen, M.V. Anxiety, depression and stress during the COVID-19 pandemic: Results from a cross-sectional survey. J. Psychiatr. Res. 2021, 137, 96–103. [Google Scholar] [CrossRef]
- Rahman, M.A.; Hoque, N.; Alif, S.M.; Salehin, M.; Islam, S.M.S.; Banik, B.; Sharif, A.; Nazim, N.B.; Sultana, F.; Cross, W. Factors associated with psychological distress, fear and coping strategies during the COVID-19 pandemic in Australia. Glob. Health 2020, 16, 95. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef] [Green Version]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Wang, Y.; Kala, M.P.; Jafar, T.H. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: A systematic review and meta-analysis. PLoS ONE 2021, 15, e0244630. [Google Scholar] [CrossRef]
- Duran, S.; Erkin, Ö. Psychologic distress and sleep quality among adults in Turkey during the COVID-19 pandemic. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2021, 107, 110254. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.K.; Oyetunji, T.P.; Prakash, A.J.; Ogunmola, O.A.; Tripathy, S.; Lawal, M.M.; Sanusi, Z.K.; Arafat, S.M.Y. Mental health research in the lower-middle-income countries of Africa and Asia during the COVID-19 pandemic: A scoping review. Neurol. Psychiatry Brain Res. 2020, 38, 54–64. [Google Scholar] [CrossRef]
- Adepoju, P. Africa turns to telemedicine to close mental health gap. Lancet Digit. Health 2020, 2, e571–e572. [Google Scholar] [CrossRef]
- Government of the Kingdom of Eswatini. Swaziland HIV Incidence Measurement Survey 2 (2016–2017). Final Report; Government of the Kingdom of Eswatini: Mbabane, Eswatini, 2019.
- Pathmanathan, I.; Pasipamire, M.; Pals, S.; Dokubo, E.K.; Preko, P.; Ao, T.; Mazibuko, S.; Ongole, J.; Dhlamini, T.; Haumba, S. High uptake of antiretroviral therapy among HIV-positive TB patients receiving co-located services in Swaziland. PLoS ONE 2018, 13, e0196831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health. WHO STEPS Noncommunicable Disease Risk Factor Surveillance Report; Ministry of Health: Mbabane, Swaziland, 2014.
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Swaziland Household Income and Expenditure Survey. 2016/2017 Swaziland Household Income and Expenditure Survey (EHIES); Central Statistical Office: Mbabane, Swaziland, 2017.
- Dlamini, L.P.; Mahanya, S.; Dlamini, S.D.; Shongwe, M.C. Prevalence and factors associated with postpartum depression at a primary health care facility in Eswatini. South Afr. J. Psychiatry 2019, 25. [Google Scholar] [CrossRef]
- Dlamini, S.B.; Shongwe, M.C. Exploring mental health nurses’ perceptions on factors contributing to psychiatric readmissions in Eswatini: A qualitative study. Int. J. Afr. Nurs. Sci. 2019, 11, 100157. [Google Scholar] [CrossRef]
- United Nations Development Programme. Rapid Socioeconomic Assessment of COVID-19 in Eswatini. 2020. Available online: https://www.sz.undp.org/content/dam/swaziland/docs/COVID-19%20REPORT%20-%20Rapid%20Socio-economic%20Assessment%20of%20Covid%2019%20in%20Eswatini.pdf (accessed on 7 February 2021).
- WHO Regional Office for Europe. COVID-19 Snapshot MOnitoring (COSMO Standard): Monitoring knowledge, risk perceptions, preventive behaviours, and public trust in the current coronavirus outbreak—WHO standard protocol. PsychArchives 2020. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Sung, H.-Y.; Max, W.; Shi, Y.; Ong, M. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef]
- Kessler, R.C.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Bromet, E.; Cuitan, M.; Furukawa, T.A.; Gureje, O.; Hinkov, H.; Hu, C.-Y.; et al. Screening for serious mental illness in the general population with the K6 screening scale: Results from the WHO World Mental Health (WMH) survey initiative. Int. J. Methods Psychiatr. Res. 2010, 19, 4–22. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, Y.; Jiang, J.; Valdimarsdóttir, U.A.; Fall, K.; Fang, F.; Song, H.; Lu, D.; Zhang, W. Psychological distress among health professional students during the COVID-19 outbreak. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.; Jiang, J.; Feng, Y.; Lu, D.; Zhang, W.; Song, H. COVID-19 outbreak–related psychological distress among healthcare trainees: A cross-sectional study in China. BMJ Open 2020, 10, e041671. [Google Scholar] [CrossRef]
- Tanji, F.; Tomata, Y.; Sekiguchi, T.; Tsuji, I. Period of residence in prefabricated temporary housing and psychological distress after the Great East Japan Earthquake: A longitudinal study. BMJ Open 2018, 8, e018211. [Google Scholar] [CrossRef]
- Nakaya, N.; Nakamura, T.; Tsuchiya, N.; Narita, A.; Tsuji, I.; Hozawa, A.; Tomita, H. Prospect of future housing and risk of psychological distress at 1 year after an earthquake disaster. Psychiatry Clin. Neurosci. 2016, 70, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Ali, G.-C.; Ryan, G.; De Silva, M.J. Validated screening tools for common mental disorders in low and middle income countries: A systematic review. PLoS ONE 2016, 11, e0156939. [Google Scholar] [CrossRef]
- Mamun, M.A.; Rayhan, I.; Akter, K.; Griffiths, M.D. Prevalence and predisposing factors of suicidal ideation among the university students in Bangladesh: A single-site survey. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, M.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24–30, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1049. [Google Scholar] [CrossRef]
- Wang, H.; Xia, Q.; Xiong, Z.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z. The psychological distress and coping styles in the early stages of the 2019 coronavirus disease (COVID-19) epidemic in the general mainland Chinese population: A web-based survey. PLoS ONE 2020, 15, e0233410. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, S.M.; Witthöft, M. Health anxiety, cyberchondria, and coping in the current COVID-19 pandemic: Which factors are related to coronavirus anxiety? J. Anxiety Disord. 2020, 73, 102239. [Google Scholar] [CrossRef]
- Chandola, T.; Kumari, M.; Booker, C.L.; Benzeval, M. The mental health impact of COVID-19 and lockdown-related stressors among adults in the UK. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef]
- Stata Statistical Software: Release 15; StataCorp LP: College Station, TX, USA, 2017.
- Valliant, R.; Dever, J.A. Survey Weights: A Step-by-Step Guide to Calculation; Stata Press: College Station, TX, USA, 2018. [Google Scholar]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Wilber, S.T.; Fu, R. Risk ratios and odds ratios for common events in cross-sectional and cohort studies. Acad. Emerg. Med. 2010, 17, 649–651. [Google Scholar] [CrossRef]
- Scheim, A.I.; Perez-Brumer, A.G.; Bauer, G.R. Gender-concordant identity documents and mental health among transgender adults in the USA: A cross-sectional study. Lancet Public Health 2020, 5, e196–e203. [Google Scholar] [CrossRef]
- Green, T.; Flash, S.; Reiss, A.L. Sex differences in psychiatric disorders: What we can learn from sex chromosome aneuploidies. Neuropsychopharmacology 2019, 44, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef]
- Yu, H.; Li, M.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z.; Xiong, Z. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry 2020, 20, 426. [Google Scholar] [CrossRef]
- Newby, J.M.; O’Moore, K.; Tang, S.; Christensen, H.; Faasse, K. Acute mental health responses during the COVID-19 pandemic in Australia. PLoS ONE 2020, 15, e0236562. [Google Scholar] [CrossRef]
- Winkler, P.; Formanek, T.; Mlada, K.; Kagstrom, A.; Mohrova, Z.; Mohr, P.; Csemy, L. Increase in prevalence of current mental disorders in the context of COVID-19: Analysis of repeated nationwide cross-sectional surveys. Epidemiol. Psychiatr. Sci. 2020, 29, e173. [Google Scholar] [CrossRef]
- Agbo, A.A. Cronbach’s alpha: Review of limitations and associated recommendations. J. Psychol. Afr. 2010, 20, 233–239. [Google Scholar] [CrossRef]
- Lee, S.; Tsang, A.; Ng, K.L.; Ma, Y.L.; Guo, W.; Mak, A.; Kwok, K. Performance of the 6-item Kessler scale for measuring serious mental illness in Hong Kong. Compr. Psychiatry 2012, 53, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Allbright, M.C.; Dailey, N.S. Trends in suicidal ideation over the first three months of COVID-19 lockdowns. Psychiatry Res. 2020, 293, 113390. [Google Scholar] [CrossRef]
- Kahil, K.; Cheaito, M.A.; El Hayek, R.; Nofal, M.; El Halabi, S.; Kudva, K.G.; Pereira-Sanchez, V.; El Hayek, S. Suicide during COVID-19 and other major international respiratory outbreaks: A systematic review. Asian J. Psychiatry 2021, 56, 102509. [Google Scholar] [CrossRef] [PubMed]
- Horigian, V.E.; Schmidt, R.D.; Feaster, D.J. Loneliness, mental health, and substance use among US young adults during COVID-19. J. Psychoact. Drugs 2021, 53, 1–9. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyashanu, M.; Simbanegavi, P.; Gibson, L. Exploring the impact of COVID-19 pandemic lockdown on informal settlements in Tshwane Gauteng Province, South Africa. Glob. Public Health 2020, 15, 1443–1453. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of prevalence and associated factors of anxiety and depression among people affected by versus people unaffected by quarantine during the COVID-19 epidemic in Southwestern China. Med. Sci. Monit. 2020, 26, e924609-1–e924609-12. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, E.; Frongillo, E.A.; Chandra, P. Do social programmes contribute to mental well-being? The long-term impact of unemployment on depression in the United States. Int. J. Epidemiol. 2001, 30, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkowitz, S.A.; Basu, S. Unmet social needs and worse mental health after expiration of COVID-19 federal pandemic unemployment compensation. Health Aff. 2021, 40, 426–434. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Unweighted n | Unweighted (%) | Weighted (%; 95% CI) |
|---|---|---|---|
| Age in years | |||
| 18–24 | 233 | 23.5 | 32.4 (32.4, 32.4) |
| 25–59 | 587 | 59.1 | 48.7 (48.7, 48.7) |
| 60–92 | 173 | 17.4 | 18.9 (18.9, 18.90 |
| Sex | |||
| Female | 718 | 72.3 | 52.3 (52.3, 52.3) |
| Male | 275 | 27.7 | 47.7 (47.7, 47.7) |
| Marital status | |||
| Single | 448 | 45.1 | 49.5 (46.4, 52.6) |
| Married/cohabiting | 478 | 48.1 | 45.8 (42.5, 49.1) |
| Widowed/divorced/separated | 67 | 6.8 | 4.7 (3.3, 6.7) |
| Religion | |||
| Christian | 975 | 98.2 | 97.0 (95.0, 98.3) |
| Other/atheist | 18 | 1.8 | 3.0 (1.7, 5.0) |
| Highest education level attended | |||
| Never schooled | 24 | 2.4 | 2.9 (1.8, 4.8) |
| Primary/Sebenta a | 65 | 6.6 | 7.6 (5.7, 10.0) |
| Secondary | 130 | 13.1 | 13.6 (11.0, 16.7) |
| High school | 349 | 35.2 | 39.3 (35.5, 43.3) |
| Tertiary | 425 | 42.8 | 36.6 (32.9, 40.5) |
| Residential area | |||
| Rural | 400 | 40.3 | 73.1 (73.1, 73.1) |
| Urban | 593 | 59.7 | 26.9 (26.9, 26.9) |
| Subjective socioeconomic status | |||
| Very poor/poor | 92 | 9.3 | 9.6 (7.5, 12.2) |
| Middle | 793 | 79.9 | 80.0 (76.5, 83.1) |
| Very rich/rich | 30 | 3.0 | 2.9 (1.7, 4.7) |
| Can’t tell | 78 | 7.9 | 7.6 (5.7, 10.0) |
| Region | |||
| Hhohho | 302 | 30.4 | 29.8 (29.8, 29.8) |
| Manzini | 334 | 33.6 | 33.8 (33.8, 33.8) |
| Shiselweni | 173 | 17.4 | 17.7 (17.7, 17.7) |
| Lubombo | 184 | 18.5 | 18.7 (18.7, 18.7) |
| Self/family member lost job or business means due to pandemic | |||
| Yes | 352 | 35.5 | 36.2 (32.3, 40.2) |
| No | 641 | 64.6 | 63.8 (59.8, 67.7) |
| Know people diagnosed with COVID-19 | |||
| Yes | 68 | 6.9 | 4.8 (3.4, 6.7) |
| No | 925 | 93.2 | 95.2 (93.3, 96.6) |
| Received food/financial relief from the government during the lockdown | |||
| Yes | 99 | 10.0 | 11.4 (9.0, 14.4) |
| No/not sure | 894 | 90.0 | 88.6 (85.6, 91.0) |
| Feel well informed about COVID-19 | |||
| Yes | 642 | 64.7 | 64.9 (60.9, 68.7) |
| No | 131 | 13.2 | 14.5 (11.8, 17.7) |
| Not sure | 220 | 22.2 | 20.6 (17.6, 24.0) |
| Perceived ability to avoid contracting coronavirus | |||
| Very easy/easy | 382 | 38.5 | 40.0 (36.1, 44.2) |
| Moderate | 158 | 15.9 | 15.9 (13.1, 19.1) |
| Very difficult/difficult | 453 | 45.6 | 44.1 (40.0, 48.2) |
| Perceived probability of contracting coronavirus | |||
| Very low/low | 317 | 31.9 | 31.2 (27.5, 35.1) |
| Moderate | 194 | 19.5 | 19.3 (16.3, 22.7) |
| Very high/high | 462 | 46.5 | 47.8 (43.8, 51.9) |
| Not sure | 20 | 2.0 | 1.7 (0.9, 3.1) |
| Perceived severity if sick with COVID-19 | |||
| Not severe/less severe | 313 | 31.5 | 31.7 (28.1, 35.6) |
| Moderate | 236 | 23.8 | 21.7 (18.5, 25.2) |
| Very severe/severe | 313 | 31.5 | 33.4 (29.8, 37.3) |
| Not sure | 131 | 13.2 | 13.2 (10.7, 16.3) |
| Prevalence of suicidal ideation | |||
| Had suicidal thoughts | 17 | 1.7 | 1.5 (0.8, 2.7) |
| No suicidal thoughts | 976 | 98.3 | 98.5 (97.3, 99.2) |
| Prevalence of psychological distress | |||
| None/low (K6 0–4) | 499 | 50.3 | 52.8 (48.7, 56.9) |
| Moderate (K6 5–12) | 415 | 41.8 | 41.7 (37.7, 45.8) |
| Severe (K6 ≥13) | 79 | 8.0 | 5.4 (3.9, 7.5) |
| Background Characteristic | No Suicidal Thoughts n (Weighted Percentage (%)) | Having Suicidal Thoughts n (Weighted Percentage (%)) |
|---|---|---|
| Age in years | ||
| 18–24 | 228 (32.4) | 5 (33.8) |
| 25–59 | 576 (48.6) | 11 (56.9) |
| 60–92 | 172 (19.0) | 1 (9.4) |
| Sex | ||
| Male | 271 (47.9) | 4 (32.7) |
| Female | 705 (52.1) | 13 (67.3) |
| Marital status | ||
| Single | 437 (49.1) | 11 (74.7) |
| Married/cohabiting | 473 (46.1) | 5 (25.3) |
| Widowed/divorced/separated | 66 (4.8) | 1 (0.001) |
| Highest educational level attended | ||
| Never schooled | 24 (3.0) | 0 (0.0) |
| Primary/Sebenta a | 65 (7.7) | 0 (0.0) |
| Secondary | 128 (13.7) | 2 (6.9) |
| High school | 342 (39.2) | 7 (47.4) |
| Tertiary education | 417 (36.5) | 8 (45.7) |
| Area of residence | ||
| Urban | 582 (26.8) | 11 (39.5) |
| Rural | 394 (73.3) | 6 (60.6) |
| Subjective socioeconomic status | ||
| Very poor/poor | 91 (9.5) | 1 (11.2) |
| Middle | 782 (80.1) | 11 (74.5) |
| Very rich/rich | 29 (28.9) | 1 (0.001) |
| Can’t tell | 74 (7.5) | 4 (14.3) |
| Region of residence | ||
| Hhohho | 295 (29.5) | 7 (49.8) |
| Lubombo | 183 (18.8) | 1 (11.4) |
| Manzini | 330 (34.1) | 4 (18.1) |
| Shiselweni | 168 (17.6) | 5 (20.8) |
| Feel well informed about COVID-19 | ||
| Yes | 628 (64.6) | 14 (87.8) |
| No | 130 (14.6) | 1 (5.2) |
| Not sure | 218 (20.8) | 2 (6.9) |
| Perceived ability to avoid contracting COVID-19 | ||
| Very easy/easy | 374 (39.8) | 8 (54.1) |
| Moderate | 156 (16.0) | 2 (7.6) |
| Very difficult/difficult | 446 (44.2) | 7 (38.3) |
| Perceived probability of contracting COVID-19 | ||
| Very low/low | 315 (31.5) | 2 (11.4) |
| Moderate/ | 189 (19.1) | 5 (31.4) |
| Very high/high | 453 (47.8) | 9 (50.3) |
| Not sure | 19 (1.6) | 1 (6.9) |
| Perceived severity if sick with COVID-19 | ||
| Not severe/less severe | 307 (31.7) | 6 (32.9) |
| Moderate | 234 (21.9) | 2 (6.8) |
| Very severe/severe | 309 (33.6) | 4 (22.9) |
| Not sure | 126 (12.9) | 5 (37.4) |
| Self/family member lost job/business due to pandemic | ||
| Yes | 348 (36.2) | 4 (32.1) |
| No | 628 (63.8) | 13 (67.9) |
| Knows people diagnosed with COVID-19 * | ||
| Yes | 64 (4.7) | 4 (9.7) |
| No | 912 (95.3) | 13 (90.3) |
| Burdened by the lockdown itself | ||
| Yes | 210 (20.8) | 2 (17.2) |
| No | 766 (79.2) | 15 (82.8) |
| Received COVID-19 food/financial relief from the government during lockdown | ||
| Yes | 98 (11.6) | 1 (0.7) |
| No/Not sure | 878 (88.4) | 16 (99.3) |
| Felt lonely during the lockdown | ||
| Never/rarely | 747 (78.4) | 13 (87.1) |
| Sometimes/Most of the time/always | 229 (21.6) | 4 (12.9) |
| Psychological distress | ||
| None/low (K6 scores: 0–4) | 489 (52.7) | 10 (63.0) |
| Moderate/severe (K6 scores: ≥5) | 487 (47.3) | 7 (37.0) |
| Variable | Unweighted n | Unweighted Percentage (%) | Weighted Percentage (%; 95% CI) |
|---|---|---|---|
| Afraid of COVID-19 | |||
| Yes | 235 | 23.7 | 23.9 (20.6, 27.6) |
| No | 739 | 74.4 | 74.3 (70.6, 77.8) |
| Not sure | 19 | 1.9 | 1.8 (0.9, 3.5) |
| Felt burdened by the lockdown itself | 212 | 21.4 | 20.8 (17.7, 24.3) |
| Worried about risk of contracting COVID-19 | 141 | 14.2 | 15.0 (12.2, 18.4) |
| Experienced at least one form of abuse during the lockdown a | 41 | 4.1 | 4.4 (3.0, 6.6) |
| Sometimes/most of the time/always felt lonely during lockdown | 233 | 23.5 | 21.4 (18.2, 25.1) |
| Sometimes/most of the time/always worried about the pandemic such that can’t sleep at night | 237 | 23.9 | 22.4 (19.1, 26.0) |
| Fears about b: | |||
| being separated from family | 254 | 25.6 | 25.2 (21.8, 28.8) |
| being hospitalized due to COVID-19 | 222 | 22.4 | 22.0 (18.8, 25.5) |
| dying from COVID-19 | 505 | 50.9 | 53.1 (49.0, 57.1) |
| Seriously in need of b: | |||
| money during the lockdown | 198 | 19.9 | 19.8 (16.7, 23.3) |
| medication during the lockdown | 65 | 6.6 | 6.4 (4.7, 8.5) |
| food during the lockdown | 574 | 57.8 | 58.4 (54.4, 62.2) |
| Concerned about b: | |||
| loss of income/job/business | 171 | 17.2 | 15.7 (13.0, 18.9) |
| difficulty to keep away from crowds | 48 | 4.8 | 5.1 (3.6, 7.3) |
| nonavailability of transport | 37 | 3.7 | 3.5 (2.3, 5.3) |
| misinformation/fake news | 36 | 3.6 | 2.6 (1.7, 4.2) |
| inability to pay rent | 25 | 2.5 | 3.1 (1.9, 5.0) |
| Variable | None/Low Distress n (wt Percentage (%) a) | Moderate/Severe Distress n (wt Percentage (%) a) | CRR (95% CI) | ARR (95% CI) |
|---|---|---|---|---|
| Age in years (ref: 25–59) | ||||
| 18–24 | 111 (30.1) | 122 (35.0) | 1.11 (0.92, 1.35) | 1.34 (1.05, 1.70) * |
| 60–92 | 98 (20.1) | 75 (17.6) | 0.96 (0.74, 1.23) | 0.96 (0.76, 1.21) |
| Male (ref: Female) | 158 (50.8) | 117 (44.2) | 0.87 (0.73, 1.04) | 0.97 (0.82, 1.15) |
| Marital status (ref: Single) | ||||
| Married/cohabiting | 248 (46.4) | 230 (45.1) | 1.00 (0.83, 1.20) | 1.37 (1.09, 1.72) ** |
| Widowed/divorced/separated | 29 (3.5) | 38 (6.1) | 1.31 (0.94, 1.81) | 1.28 (0.94, 1.76) |
| Highest educational level attended (ref: Tertiary) | ||||
| Never schooled | 14 (3.4) | 10 (2.5) | 1.00 (0.52, 1.91) | - |
| Primary/Sebenta | 33 (8.8) | 32 (6.2) | 0.98 (0.65, 1.48) | - |
| Secondary | 53 (9.6) | 77 (18.0) | 1.58 (1.24, 2.02) *** | - |
| High school | 164 (36.3) | 185 (42.6) | 1.29 (1.05, 1.60) * | - |
| Urban (ref: Rural) | 277 (25.0) | 316 (29.1) | 1.11 (0.94, 1.32) | |
| Subjective socioeconomic status (ref: Can’t tell) | ||||
| Very poor/poor | 36 (8.2) | 56 (11.1) | 1.29 (0.84, 1.97) | - |
| Middle | 406 (80.0) | 387 (80.0) | 1.11 (0.77, 1.60) | - |
| Very rich/rich | 17 (3.5) | 13 (2.1) | 0.82 (0.38, 1.75) | - |
| Region (ref: Lubombo) | ||||
| Hhohho | 119 (23.8) | 183 (36.7) | 1.76 (1.31, 2.36) *** | 1.63 (1.24, 2.15) ** |
| Manzini | 161 (33.3) | 173 (34.4) | 1.45 (1.07, 1.97) * | 1.42 (1.07, 1.89) * |
| Shiselweni | 102 (19.2) | 71 (15.9) | 1.29 (0.91, 1.81) | 1.28 (0.93, 1.77) |
| Feel well informed about COVID-19 (ref: Yes) | ||||
| No | 40 (8.6) | 91 (21.1) | 1.62 (1.35, 1.95) *** | 1.59 (1.32, 1.91) *** |
| Not sure | 102 (20.5) | 118 (20.7) | 1.12 (0.90, 1.40) | 1.05 (0.86, 1.29) |
| Perceived ability to avoid contracting COVID-19 (ref: Moderate) | ||||
| Very easy/easy | 220 (45.6) | 162 (33.8) | 0.99 (0.74, 1.34) | - |
| Very difficult/difficult | 189 (36.4) | 264 (52.7) | 1.41 (1.07, 1.85) * | - |
| Perceived probability of contracting COVID-19 (ref: Very low/low) | ||||
| Moderate/ | 94 (17.3) | 100 (21.5) | 1.27 (0.99, 1.63) | - |
| Very high/high | 224 (46.0) | 238 (49.8) | 1.19 (0.96, 1.47) | - |
| Not sure | 9 (2.1) | 11 (1.2) | 0.81 (0.37, 1.79) | - |
| Perceived severity if sick with COVID-19 (ref: Not severe/less severe) | ||||
| Moderate | 127 (23.9) | 109 (19.2) | 1.00 (0.77, 1.31) | - |
| Very severe/severe | 133 (27.6) | 180 (39.9) | 1.35 (1.08, 1.67) ** | - |
| Not sure | 66 (13.7) | 65 (12.7) | 1.08 (0.80, 1.47) | - |
| Self/family member lost job/business due to the pandemic (Ref: No) | 149 (32.9) | 203 (39.8) | 1.17 (0.98, 1.39) | - |
| Knows people diagnosed with COVID-19 (ref: No) | 30 (4.0) | 38 (5.6) | 1.18 (0.85, 1.64) | - |
| Burdened by the lockdown itself (ref: Not) | 86 (16.1) | 126 (26.0) | 1.34 (1.11, 1.61) ** | 1.33 (1.11, 1.59) ** |
| Received COVID-19 food/financial relief from the government during the lockdown (ref: No/not sure) | 38 (8.7) | 61 (14.5) | 1.31 (1.05, 1.64) * | 1.35 (1.10, 1.65) ** |
| Sometimes/most of the time/always felt lonely during the lockdown (ref: Never/rarely felt lonely) | 41 (8.6) | 192 (35.8) | 2.05 (1.75, 2.38) *** | 2.01 (1.23, 2.34) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shongwe, M.C.; Huang, S.-L. Suicidal Ideation and Predictors of Psychological Distress during the COVID-19 Pandemic in Eswatini: A Population-Based Household Telephone Survey. Int. J. Environ. Res. Public Health 2021, 18, 6700. https://doi.org/10.3390/ijerph18136700
Shongwe MC, Huang S-L. Suicidal Ideation and Predictors of Psychological Distress during the COVID-19 Pandemic in Eswatini: A Population-Based Household Telephone Survey. International Journal of Environmental Research and Public Health. 2021; 18(13):6700. https://doi.org/10.3390/ijerph18136700
Chicago/Turabian StyleShongwe, Mduduzi Colani, and Song-Lih Huang. 2021. "Suicidal Ideation and Predictors of Psychological Distress during the COVID-19 Pandemic in Eswatini: A Population-Based Household Telephone Survey" International Journal of Environmental Research and Public Health 18, no. 13: 6700. https://doi.org/10.3390/ijerph18136700