
Anti-Inflammatory Effects of Immunostimulation in Patients with COVID-19 Pneumonia

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients’ Characteristics
2.3. In-Hospital Treatment
2.4. Pidotimod and Historical Control Group
2.5. PBMC Isolation and Stimulation
2.6. Multiplex Cytokine Analyses
2.7. Quantigene Plex Gene Expression Assay
2.8. Neutrophil to Lymphocyte Ratio
2.9. Study Outcomes
2.10. Statistical Analysis
3. Results
3.1. Patients’ Clinical Characteristics
3.2. Clinical Outcomes
3.3. Neutrophil to Lymphocyte Ratio
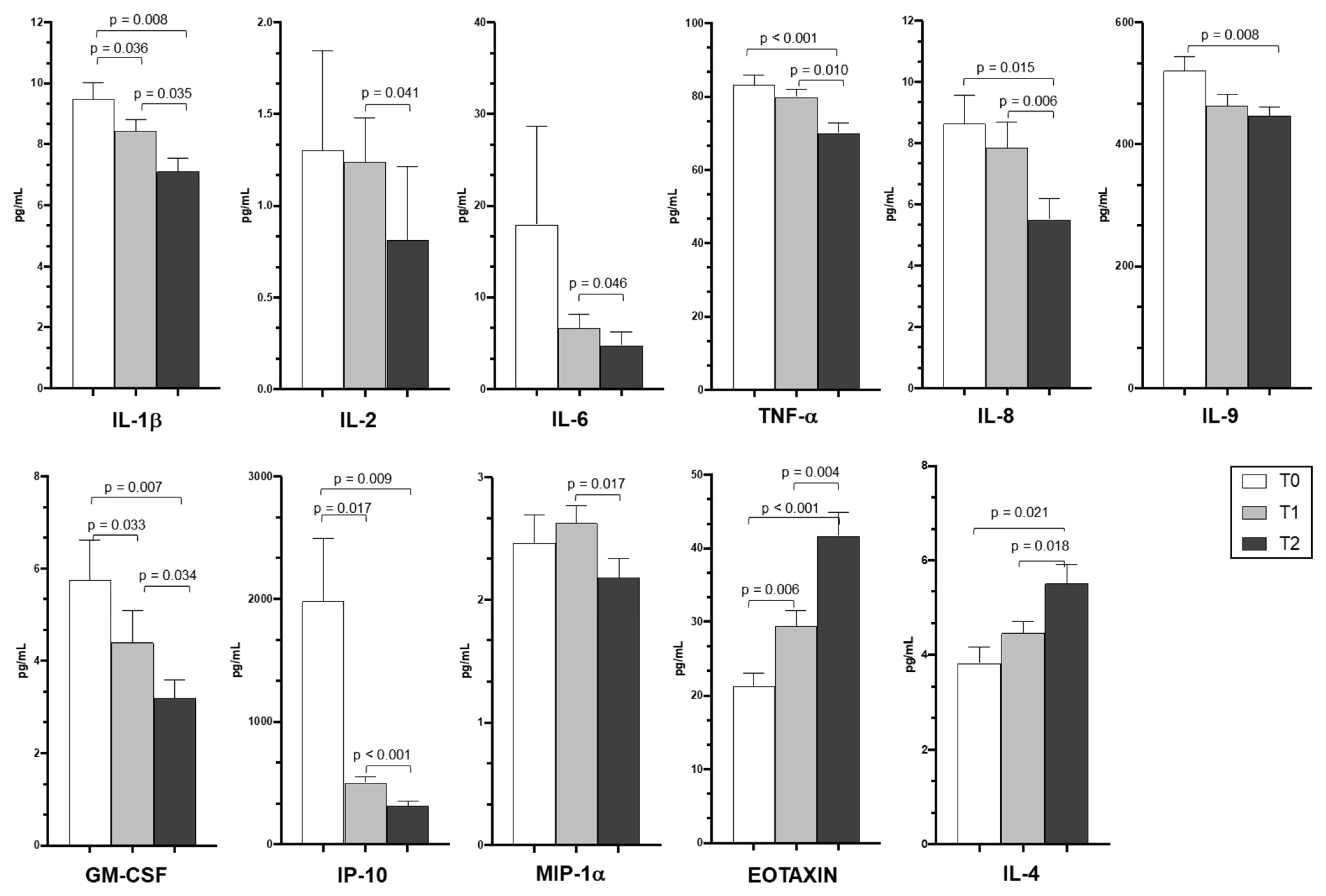
3.4. Cytokine and Chemokine Plasma Levels
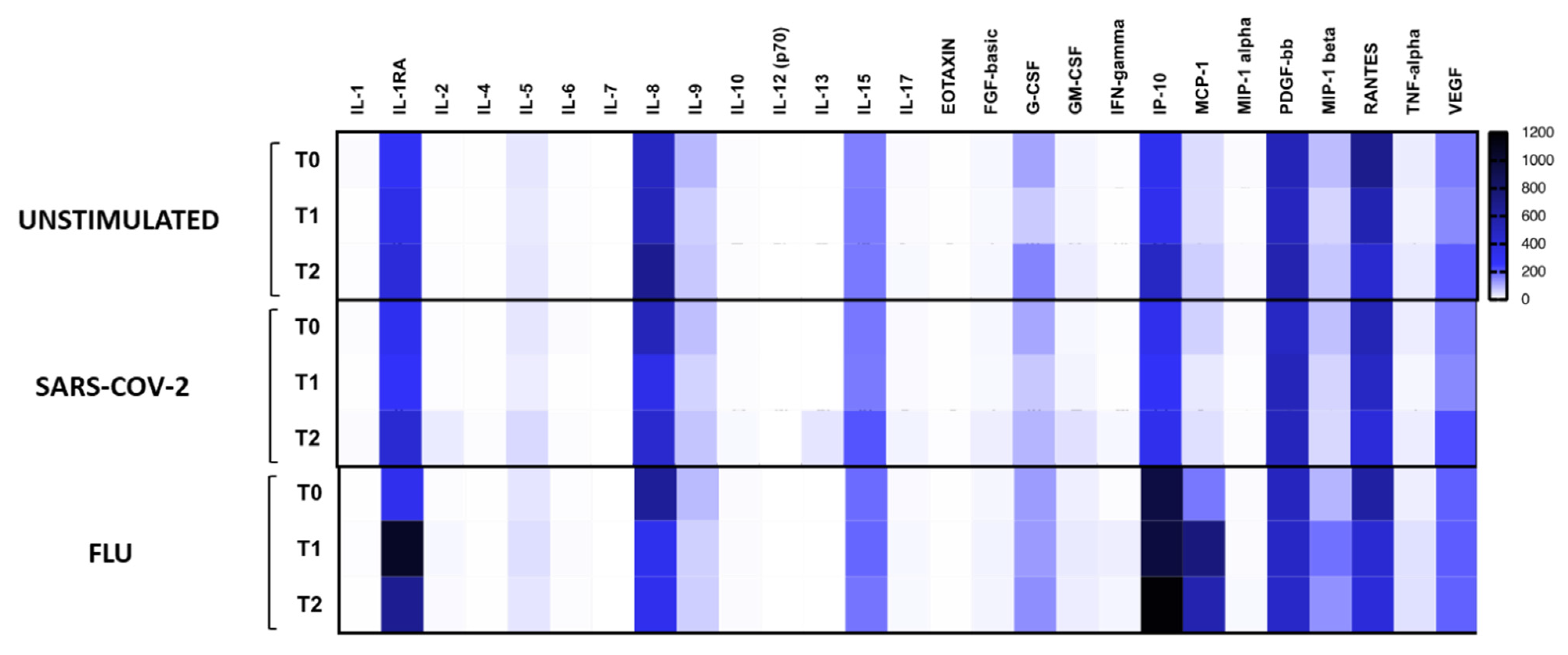
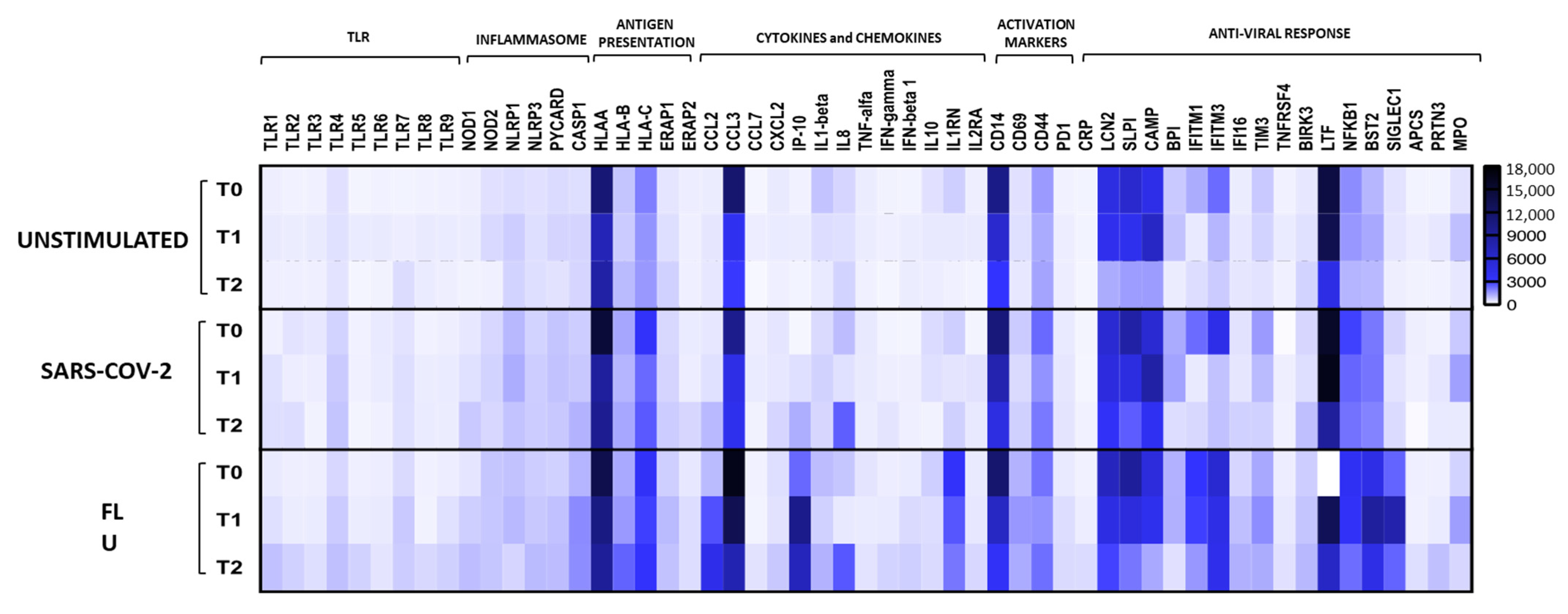
3.5. SARS-CoV-2 Specific Immune Profile
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Radovanovic, D.; Pini, S.; Franceschi, E.; Pecis, M.; Airoldi, A.; Rizzi, M.; Santus, P. Characteristics and outcomes in hospitalized COVID-19 patients during the first 28 days of the spring and autumn pandemic waves in Milan: An observational prospective study. Respir. Med. 2021, 178, 106323. [Google Scholar] [CrossRef] [PubMed]
- Radovanovic, D.; Santus, P.; Coppola, S.; Saad, M.; Pini, S.; Giuliani, F.; Mondoni, M.; Chiumello, D.A. Characteristics, outcomes and global trends of respiratory support in patients hospitalized with COVID-19 pneumonia: A scoping review. Minerva Anestesiol. 2021, 87, 915–926. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. COVID-19 Lombardy ICU Network. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Yang, L.; Xie, X.; Tu, Z.; Fu, J.; Xu, D.; Zhou, Y. The signal pathways and treatment of cytokine storm in COVID-19. Signal Transduct. Target. Ther. 2021, 6, 255. [Google Scholar] [CrossRef]
- Schwarze, J.; Mackenzie, K.J. Novel insights into immune and inflammatory responses to respiratory viruses. Thorax 2013, 68, 108–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrario, B.E.; Garuti, S.; Braido, F.; Canonica, G.W. Pidotimod: The state of art. Clin. Mol. Allergy 2015, 13, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trabattoni, D.; Clerici, M.; Centanni, S.; Mantero, M.; Garziano, M.; Blasi, F. Immunomodulatory effects of pidotimod in adults with community-acquired pneumonia undergoing standard antibiotic therapy. Pulm. Pharmacol. Ther. 2017, 44, 24–29. [Google Scholar] [CrossRef]
- Esposito, S.; Garziano, M.; Rainone, V.; Trabattoni, D.; Biasin, M.; Senatore, L.; Marchisio, P.G.; Rossi, M.; Principi, N.; Clerici, M. Immunomodulatory activity of pidotimod administered with standard antibiotic therapy in children hospitalized for community-acquired pneumonia. J. Transl. Med. 2015, 13, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ucciferri, C.; Falasca, K.; Reale, M.; Tamburro, M.; Auricchio, A.; Vignale, F.; Vecchiet, J. Pidotimod and Immunological Activation in Individuals Infected with HIV. Curr. HIV Res. 2021, 19, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Ucciferri, C.; Barone, M.; Vecchiet, J.; Falasca, K. Pidotimod in Paucisymptomatic SARS-CoV2 Infected Patients. Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020048. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Radovanovic, D.; Saderi, L.; Marino, P.; Cogliati, C.; De Filippis, G.; Rizzi, M.; Franceschi, E.; Pini, S.; Giuliani, F.; et al. Severity of respiratory failure at admission and in-hospital mortality in patients with COVID-19: A prospective observational multicentre study. BMJ Open 2020, 10, e043651. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. ARDS Definition Task Force. Acute respiratory distress syndrome: The Berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar]
- Salton, F.; Confalonieri, P.; Meduri, G.U.; Santus, P.; Harari, S.; Scala, R.; Lanini, S.; Vertui, V.; Oggionni, T.; Caminati, A.; et al. Prolonged Low-Dose Methylprednisolone in Patients with Severe COVID-19 Pneumonia. Open Forum Infect. Dis. 2020, 7, ofaa421. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Bruzzi, P.; Barisione, E.; Centanni, S.; Castaldo, N.; Corcione, S.; De Rosa, F.G.; Di Marco, F.; Gori, A.; et al. Clinical Management of Adult Patients with COVID-19 Outside Intensive Care Units: Guidelines from the Italian Society of Anti-Infective Therapy (SITA) and the Italian Society of Pulmonology (SIP). Infect. Dis. Ther. 2021, 10, 1837–1885. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Radovanovic, D.; Billi, F.; Sotgiu, G.; Costanzo, M.; Pilocane, T.; Saderi, L.; Gramegna, A.; Rovellini, A.; Perotto, L.; et al. Helmet CPAP treatment in patients with COVID-19 pneumonia: A multicentre cohort study. Eur. Respir. J. 2020, 56, 2001935. [Google Scholar] [CrossRef]
- Radovanovic, D.; Rizzi, M.; Pini, S. Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. J. Clin. Med. 2020, 9, 1191. [Google Scholar] [CrossRef]
- Radovanovic, D.; Pini, S.; Saad, M.; Perotto, L.; Giuliani, F.; Santus, P. Predictors of weaning from helmet CPAP in patients with COVID-19 pneumonia. Crit. Care 2021, 25, 206. [Google Scholar] [CrossRef] [PubMed]
- Seyit, M.; Avci, E.; Nar, R.; Senol, H.; Yilmaz, A.; Ozen, M.; Oskay, A.; Aybek, H. Neutrophil to lymphocyte ratio, lymphocyte to monocyte ratio and platelet to lymphocyte ratio to predict the severity of COVID-19. Am. J. Emerg. Med. 2020, 45, 569. [Google Scholar] [CrossRef]
- Yang, A.P.; Liu, G.P.; Tao, W.Q.; Lib, H.M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef] [PubMed]
- Ma, A.; Cheng, J.; Yang, J.; Dong, M.; Liao, X.; Kang, Y. Neutrophil-to-lymphocyte ratio as a predictive biomarker for moderate-severe ARDS in severe COVID-19 patients. Crit. Care 2020, 24, 288. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, C.; Mao, Z.; Xiao, M.; Wang, L.; Qi, S.; Zhou, F. Predictive values of neutrophil-to-lymphocyte ratio on disease severity and mortality in COVID-19 patients: A systematic review and meta-analysis. Crit. Care 2020, 24, 647. [Google Scholar] [CrossRef]
- Xu, Z.S.; Shu, T.; Kang, L.; Wu, D.; Zhou, X.; Liao, B.-W.; Sun, X.-L.; Zhou, X.; Wang, Y.-Y. Temporal profiling of plasma cytokines, chemokines and growth factors from mild, severe and fatal COVID-19 patients. Signal Transduct. Target. Ther. 2020, 5, 100. [Google Scholar] [CrossRef]
- Lacy, P. Eosinophil Cytokines in Allergy. In Cytokine Effector Functions in Tissues; Foti, M., Locati, M., Eds.; Academic Press—Elsevier Science Publishing Co. Inc.: New York, NY, USA, 2017; pp. 173–218. [Google Scholar]
- Horspool, A.M.; Kieffer, T.; Russ, B.P.; DeJong, M.A.; Wolf, M.A.; Karakiozis, J.M.; Hickey, B.J.; Fagone, P.; Tacker, D.H.; Bevere, J.R.; et al. Interplay of Antibody and Cytokine Production Reveals CXCL13 as a Potential Novel Biomarker of Lethal SARS-CoV-2 Infection. mSphere 2021, 6, e01324-20. [Google Scholar] [CrossRef]
- Santus, P.; Saad, M.; Damiani, G.; Patella, V.; Radovanovic, D. Current and future targeted therapies for severe asthma: Managing treatment with biologics based on phenotypes and biomarkers. Pharmacol. Res. 2019, 146, 104296. [Google Scholar] [CrossRef]
- de Paula, C.B.; de Azevedo, M.L.V.; Nagashima, S.; Martins, A.P.; Malaquias, M.A.; dos Santos Miggiolaro, A.F.; Júnior, J.D.; Avelino, G.; do Carmo, L.A.; Carstens, L.B.; et al. IL-4/IL-13 remodeling pathway of COVID-19 lung injury. Sci. Rep. 2020, 10, 18689. [Google Scholar] [CrossRef]
- Totura, A.L.; Baric, R.S. SARS coronavirus pathogenesis: Host innate immune responses and viral antagonism of interferon. Curr. Opin. Virol. 2012, 2, 264–275. [Google Scholar] [CrossRef]
- Qu, S.; Dai, C.; Qiu, M. Effects of pidotimod soluble powder and immune enhancement of Newcastle disease vaccine in chickens. Immunol. Lett. 2017, 187, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Zuccotti, G.V.; Mameli, C.; Trabattoni, D.; Beretta, S.; Biasin, M.; Guazzarotti, L.; Clerici, M. Immunomodulating activity of Pidotimod in children with Down syndrome. J. Biol. Regul. Homeost. Agents 2013, 27, 253–258. [Google Scholar] [PubMed]
- Jimeno, S.; Ventura, P.S.; Castellano, J.M.; García-Adasme, S.I.; Miranda, M.; Touza, P.; Lllana, I.; López-Escobar, A. Prognostic implications of neutrophil-lymphocyte ratio in COVID-19. Eur. J. Clin. Investig. 2021, 51, e13404. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pidotimod (N = 16) | Controls (N = 16) | p-Value | |
|---|---|---|---|
| Males, n (%) | 8 (50) | 8 (50) | 1.000 |
| Age, years | 60 (55–71) | 61 (54–69) | 0.867 |
| Arterial hypertension, n (%) | 9 (56) | 8 (50) | 0.719 |
| Diabetes mellitus, n (%) | 4 (25) | 4 (25) | 1.000 |
| Ischaemic heart disease, n (%) | 3 (19) | 3 (19) | 1.000 |
| COPD, n (%) | 2 (13) | 1 (6) | 0.310 |
| From symptoms onset to admission, days | 6 (4–10) | 8 (5–11) | 0.323 |
| Variables at admission | |||
| PaO2, mmHg | 73 (66–90) | 90 (83–140) | 0.005 |
| PaO2/FiO2, mmHg | 218 (165–289) | 244 (168–294) | 0.669 |
| PaO2/FiO2 200–300 mmHg, n (%) | 7 (44) | 6 (37) | 0.719 |
| PaO2/FiO2 100–200 mmHg, n (%) | 9 (56) | 10 (63) | 0.719 |
| CPAP, n (%) | 4 (40) | 6 (37) | 0.446 |
| Glasgow coma scale, score | 15 (15–15) | 15 (15–15) | 0.780 |
| C reactive protein, mg/L | 50 (24–138) | 69 (41–148) | 0.381 |
| D-dimer, mg/L FEU | 558 (421–811) | 787 (574–1362) | 0.070 |
| From admission to PDT start, days | 1 (1–1.5) | -- | -- |
| From symptoms to PDT start, days | 7 (5–11.5) | -- | -- |
| Variables 7 days post admission | |||
| PaO2, mmHg | 74 (66–87) | 72 (67–83) | 0.953 |
| PaO2/FiO2, mmHg | 342 (288–380) | 273 (196–338) | 0.033 |
| PaO2/FiO2 200–300 mmHg, n (%) | 0 | 4 (25) | 0.033 |
| PaO2/FiO2 <200 mmHg, n (%) | 5 (31) | 6 (37) | 0.710 |
| C reactive protein, mg/L | 50 (24–138) | 69 (41–148) | 0.381 |
| D-dimer, mg/L FEU | 661 (409–951) | 764 (585–1183) | 0.196 |
| In-hospital treatments | |||
| Systemic corticosteroids | 15 (94) | 12 (75) | 0.144 |
| Antibiotics, n (%) | 3 (19) | 8 (50) | 0.063 |
| LMWH, n (%) | 16 (100) | 16 (100) | 0.310 |
| Prophylactic dose, n (%) | 11 (69) * | 14 (87) * | 0.200 |
| Therapeutic dose, n (%) | 6 (37) | 4 (25) | 0.446 |
| Clinical outcomes | |||
| CPAP at 7 days, n (%) | 1 (6) | 4 (25) | 0.144 |
| Invasive mechanical ventilation, n (%) | 0 | 1 (6) | 0.310 |
| Tranferred to ICU, n (%) | 0 | 1 (6) | 0.310 |
| Lenght of stay, days | 10 (8–14) | 11 (8–21) | 0.770 |
| From symptoms to discharge, days | 17 (13–23) | 18 (16–31) | 0.358 |
| Death HDRU, n (%) | 0 | 0 | -- |
| Death ICU, n (%) | 0 | 1 (6) | 0.310 |
| Discharged to low intensity, n (%) | 1 (12) | 7 (44) | 0.014 |
| Pidotimod (N = 16) | Controls (N = 16) | p-Value | |
|---|---|---|---|
| At admission | |||
| WBC count at admission, ×106/µL | 7450 (5990–10,840) | 6010 (5380–11,740) | 0.520 |
| Neutrophil count, ×106/µL | 8580 (5150–11,010) | 8740 (4800–11,890) | 0.670 |
| Lymphocyte count, ×106/µL | 750 (590–1350) | 820 (610–1610) | 0.520 |
| NLR | 7.45 (2.7–12.9) | 6.85 (4.1–10.3) | 0.809 |
| NLR ≥ 6.5 | 10 (62) | 8 (50) | 0.476 |
| Pidotimod start | |||
| WBC count at admission, ×106/µL | 6820 (5950–9890) | 6420 (5360–10,900) | 0.773 |
| Neutrophil count, ×106/µL | 5480 (4030–8740) | 5310 (4220–9010) | 0.865 |
| Lymphocyte count, ×106/µL | 1100 (590–1370) | 990 (730–1540) | 0.538 |
| NLR | 6.35 (2.3–9.3) | 5.4 (4.8–7.1) | 0.081 |
| NLR ≥ 6.5 | 8 (50) | 8 (50) | 1.000 |
| 7 days post Pidotimod start | |||
| WBC count at admission, ×106/µL | 9090 (8000–10,982) | 7330 (5420–12,032) | 1.000 |
| Neutrophil count, ×106/µL | 6920 (5280–7480) | 6180 (4020–11,810) | 0.076 |
| Lymphocyte count, ×106/µL | 2055 (1360–3255) | 1000 (750–1510) | 0.003 |
| NLR | 2.9 (1.7–4.6) | 5.5 (3.4–7.1) | 0.037 |
| NLR ≥ 6.5 | 1 (6) | 6 (37.5) | 0.033 |
| A | Unstimulated | SARS-CoV-2 | FLU | ||||||
| T0 vs. T1 | T0 vs. T2 | T1 vs. T2 | T0 vs. T1 | T0 vs. T2 | T1 vs. T2 | T0 vs. T1 | T0 vs. T2 | T1 vs. T2 | |
| IL-1RA | ns | ns | ns | ns | ns | ns | 0.0026671 | 0.050791 | ns |
| IL-4 | ns | ns | ns | ns | ns | ns | ns | ns | ns |
| IL-5 | ns | ns | ns | 0.0107572 | ns | ns | ns | ns | ns |
| IL-6 | ns | ns | ns | ns | ns | ns | 0.0520084 | ns | ns |
| IL-8 | ns | ns | ns | ns | ns | ns | 0.0304641 | 0.0212915 | ns |
| IL-9 | 0.0468253 | ns | ns | ns | ns | ns | ns | ns | ns |
| FGF-basic | ns | ns | ns | ns | ns | ns | 0.0410918 | ns | ns |
| G-CSF | ns | ns | 0.025881 | 0.0533785 | ns | ns | ns | ns | ns |
| GM-CSF | ns | ns | ns | ns | ns | ns | 0.0520894 | ns | ns |
| IFN-γ | ns | ns | ns | ns | ns | ns | 0.0057612 | 0.0265163 | ns |
| MCP-1 | ns | ns | ns | ns | ns | ns | 0.0025601 | 0.0519345 | ns |
| MIP-1α | ns | ns | 0.0419556 | 0.0369439 | ns | ns | ns | ns | ns |
| MIP-1β | ns | ns | ns | ns | 0.0474791 | ns | ns | ns | ns |
| TNF-α | ns | ns | ns | 0.0110859 | ns | ns | ns | ns | ns |
| VEGF | ns | ns | ns | ns | ns | 0.0524005 | ns | ns | ns |
| B | Unstimulated | SARS-CoV-2 | FLU | ||||||
| T0 vs. T1 | T0 vs. T2 | T1 vs. T2 | T0 vs. T1 | T0 vs. T2 | T1 vs. T2 | T0 vs. T1 | T0 vs. T2 | T1 vs. T2 | |
| TLR1 | ns | ns | ns | ns | ns | ns | ns | 0.0181312 | 0.0520254 |
| TLR8 | ns | ns | ns | ns | ns | ns | ns | 0.0373754 | 0.0170549 |
| HLAA | ns | ns | ns | 0.0366873 | ns | ns | ns | ns | ns |
| CCL3 | ns | 0.0446018 | ns | 0.0513275 | 0.0417868 | ns | ns | ns | ns |
| CXCL10 | ns | ns | ns | ns | ns | ns | 0.0127521 | ns | ns |
| IL10 | ns | ns | ns | ns | 0.0276853 | 0.0035351 | ns | ns | ns |
| CD14 | ns | 0.0089948 | 0.0274998 | ns | 0.0039326 | 0.0350016 | 0.0290724 | 0.0017886 | 0.0113182 |
| SLPI | ns | 0.0492902 | ns | ns | ns | ns | ns | 0.0433022 | ns |
| CAMP | ns | ns | ns | ns | ns | ns | ns | ns | 0.0535916 |
| BPI | ns | ns | 0.0540071 | ns | ns | ns | ns | ns | ns |
| IFITM1 | ns | ns | ns | ns | ns | 0.0407747 | ns | ns | ns |
| HAVCR2 | ns | ns | ns | ns | ns | 0.0474798 | ns | ns | ns |
| BIRK3 | ns | ns | ns | ns | ns | 0.0266934 | ns | ns | ns |
| NFKB1 | ns | 0.0248691 | ns | ns | ns | ns | ns | 0.0058548 | 0.0509105 |
| SIGLEC1 | ns | ns | ns | ns | ns | ns | 0.013669 | ns | 0.0138821 |
| MPO | ns | ns | ns | ns | ns | 0.0253309 | ns | ns | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santus, P.; Radovanovic, D.; Garziano, M.; Pini, S.; Croce, G.; Fuccia, G.; Spitaleri, D.; Biasin, M.; Clerici, M.; Trabattoni, D. Anti-Inflammatory Effects of Immunostimulation in Patients with COVID-19 Pneumonia. J. Clin. Med. 2021, 10, 5765. https://doi.org/10.3390/jcm10245765
Santus P, Radovanovic D, Garziano M, Pini S, Croce G, Fuccia G, Spitaleri D, Biasin M, Clerici M, Trabattoni D. Anti-Inflammatory Effects of Immunostimulation in Patients with COVID-19 Pneumonia. Journal of Clinical Medicine. 2021; 10(24):5765. https://doi.org/10.3390/jcm10245765
Chicago/Turabian StyleSantus, Pierachille, Dejan Radovanovic, Micaela Garziano, Stefano Pini, Giuseppe Croce, Giuseppe Fuccia, Debora Spitaleri, Mara Biasin, Mario Clerici, and Daria Trabattoni. 2021. "Anti-Inflammatory Effects of Immunostimulation in Patients with COVID-19 Pneumonia" Journal of Clinical Medicine 10, no. 24: 5765. https://doi.org/10.3390/jcm10245765