
Antibiotic Use and Fatal Outcomes among Critically Ill Patients with COVID-19 in Tacna, Peru

 ,
,  ,
, 

Abstract
:1. Introduction
2. Results
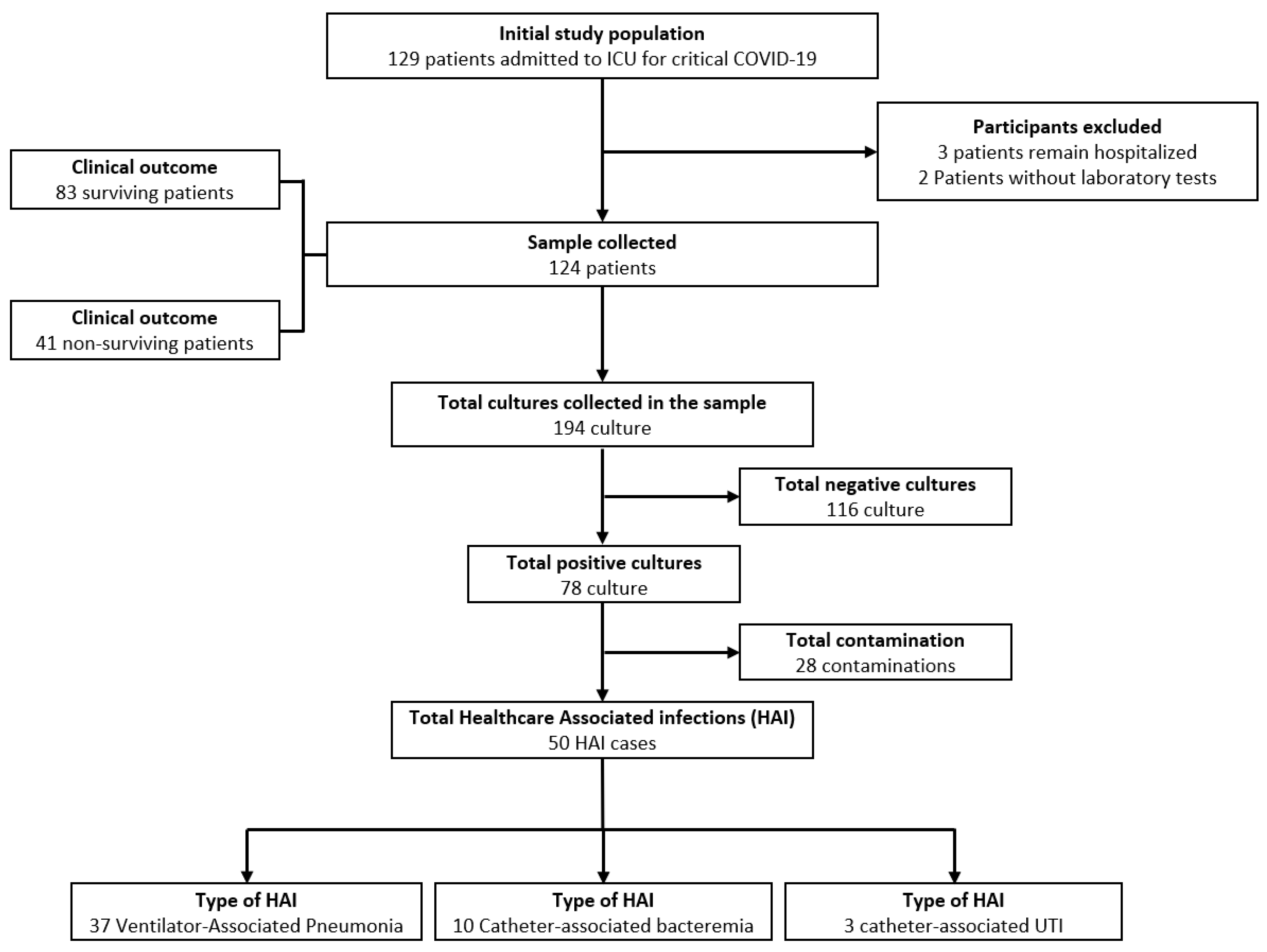
2.1. Patients
2.2. Bivariate Analysis According to Mortality in the Study Population
2.3. Source of Infection and Microbiological Characteristics
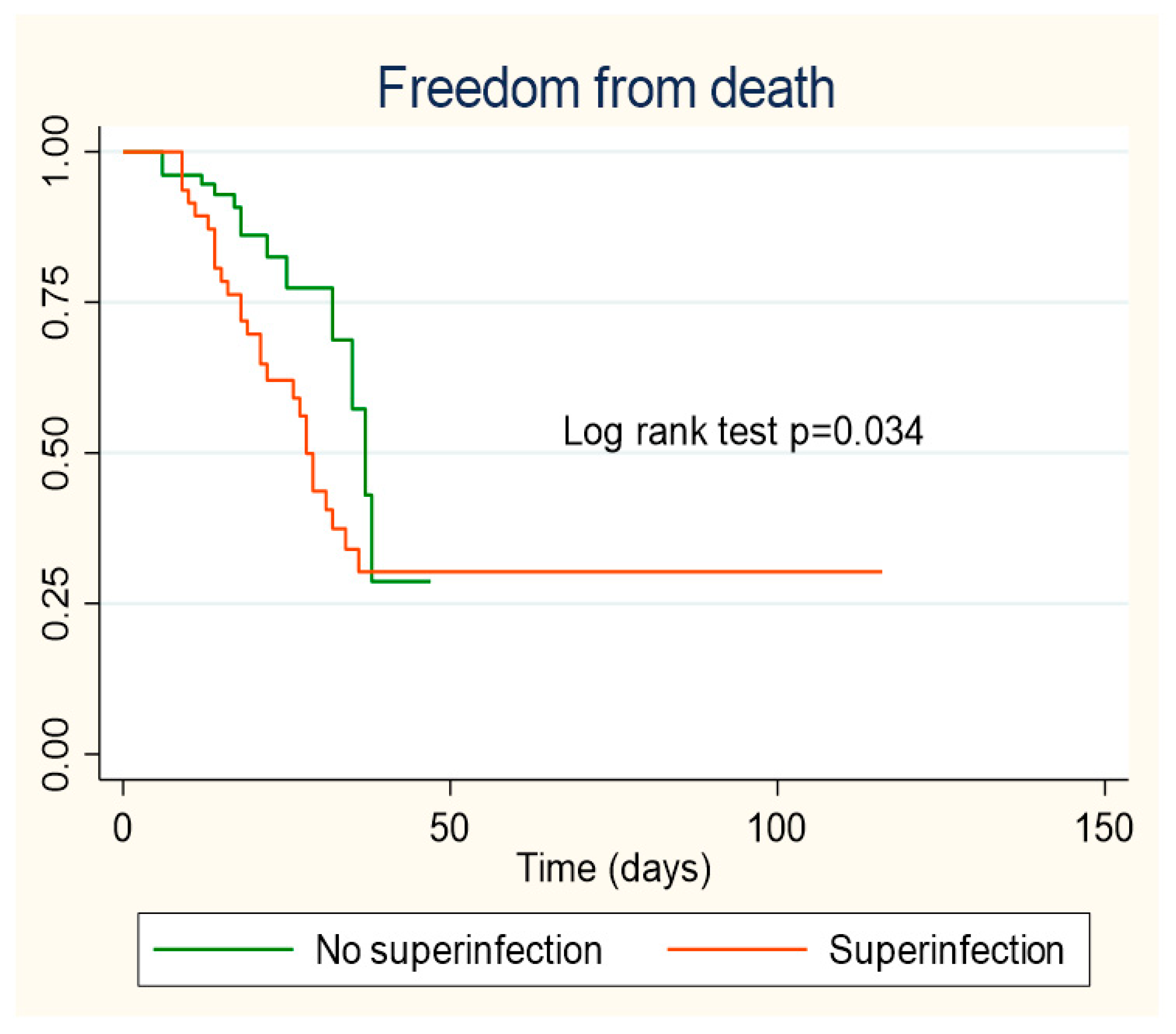
2.4. Survival Estimated by Kaplan–Meier Curves
2.5. Healthcare Infection Associated with Mortality and Acute Renal Failure
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting
4.2. Population and Sample
4.3. Data Collection and Variable Definition
4.3.1. Result Variables
Hospital Mortality
Acute Kidney Failure
4.3.2. Exposure Variables
Ventilator-Associated Pneumonia
Intravascular Catheter-Related Bacteremia
Catheter-Associated Urinary Tract Infection
Bacterial Isolation, Susceptibility, and Resistance
Clinical Characteristics
Auxiliary Reference Tests
Complications during ICU Stay
Treatment Received
4.4. Statistical Analysis
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Giacobbe, D.R.; Battaglini, D.; Enrile, E.M.; Dentone, C.; Vena, A.; Robba, C.; Ball, L.; Bartoletti, M.; Coloretti, I.; Di Bella, S.; et al. Incidence and Prognosis of Ventilator-Associated Pneumonia in Critically Ill Patients with COVID-19: A Multicenter Study. J. Clin. Med. 2021, 10, 555. [Google Scholar] [CrossRef]
- Martinez-Guerra, B.A.; Gonzalez-Lara, M.F.; de-Leon-Cividanes, N.A.; Tamez-Torres, K.M.; Roman-Montes, C.M.; Rajme-Lopez, S.; Villalobos-Zapata, G.I.; Lopez-Garcia, N.I.; Martínez-Gamboa, A.; Sifuentes-Osornio, J.; et al. Antimicrobial Resistance Patterns and Antibiotic Use during Hospital Conversion in the COVID-19 Pandemic. Antibiot. Basel 2021, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Moreno, C.; Valderrama-Beltrán, S.; Rodriguez-Morales, A.J. Implications of Antibiotic Use during the COVID-19 Pandemic: The Example of Associated Antimicrobial Resistance in Latin America. Antibiotics 2021, 10, 328. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Vélez, C.; Urrunaga-Pastor, D.; Romero-Cerdán, A.; Peña-Sánchez, E.; Fernández, J.L.; Cossio, J.D.; Marreros Ascoy, G.C.; Benites-Zapata, V.A. Risk factors for mortality in hospitalized patients with COVID-19 from three hospitals in Peru: A retrospective cohort study. F1000Research 2021, 10, 224. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Response Fund. 4 June 2021. Available online: https//covid19.who.int/region/amro/country/pe (accessed on 12 June 2021).
- Baskaran, V.; Lawrence, H.; Lansbury, L.E.; Webb, K.; Safavi, S.; Zainuddin, N.I.; Huq, T.; Eggleston, C.; Ellis, J.; Thakker, C.; et al. Coinfection in critically ill patients with COVID-19: An observational cohort study from England. J. Med. Microbiol. 2021, 70, 001350. [Google Scholar] [CrossRef]
- Szakmany, T.; Tuckwell, W.; Harte, E.; Wetherall, N.; Ramachandran, S.; Price, S.; Breen, H.; Killick, C.; Cheema, Y.; King, C.; et al. Differences in Inflammatory Marker Kinetics between the First and Second Wave of COVID-19 Patients Admitted to the ICU: A Retrospective, Single-Center Study. J. Clin. Med. 2021, 10, 3290. [Google Scholar] [CrossRef] [PubMed]
- Chong, W.H.; Saha, B.K.; Ananthakrishnan Ramani Chopra, A. State-of-the-art review of secondary pulmonary infections in patients with COVID-19 pneumonia. Infection 2021, 11, 1–15. [Google Scholar] [CrossRef]
- Yu, Y.; Xu, D.; Fu, S.; Zhang, J.; Yang, X.; Xu, L.; Xu, J.; Wu, Y.; Huang, C.; Ouyang, Y.; et al. Patients with COVID-19 in 19 ICUs in Wuhan, China: A cross-sectional study. Crit. Care 2020, 24, 219. [Google Scholar] [CrossRef] [PubMed]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502. [Google Scholar] [CrossRef]
- He, S.; Liu, W.; Jiang, M.; Huang, P.; Xiang, Z.; Deng, D.; Chen, P.; Xie, L. Clinical characteristics of COVID-19 patients with clinically diagnosed bacterial co-infection: A multi-center study. PLoS ONE 2021, 16, e0249668. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Battaglini, D.; Ball, L.; Brunetti, I.; Bruzzone, B.; Codda, G.; Crea, F.; De Maria, A.; Dentone, C.; Di Biagio, A.; et al. Bloodstream infections in critically ill patients with COVID-19. Eu. J. Clin. Investig. 2020, 50, e13319. [Google Scholar] [CrossRef] [PubMed]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2, bacterial coinfections, and AMR: The deadly trio in COVID-19? EMBO Mol. Med. 2020, 12, e12560. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, M.; Nicolini, L.A.; Signori, A.; Di Biagio, A.; Sepulcri, C.; Russo, C.; Dettori, S.; Berruti, M.; Sormani, M.P.; Giacobbe, D.R.; et al. Tocilizumab and steroid treatment in patients with COVID-19 pneumonia. PLoS ONE 2020, 15, e0237831. [Google Scholar] [CrossRef]
- Thibault, R.; Seguin, P.; Tamion, F.; Pichard, C.; Singer, P. Nutrition of the COVID-19 patient in the intensive care unit (ICU): A practical guidance. Crit. Care 2020, 24, 447. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. COVID-19 Lombardy ICU Network. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Hueda Zavaleta, M.; Copaja-Corzo, C.; Bardales-Silva, F.; Flores-Palacios, R.; BarretoRocchetti, L.; Benites Zapata, V.A. Factores asociados a la muerte por COVID-19 en pacientes admitidos en un hospital público en Tacna, Perú. Rev. Peru. Med. Exp. Salud Publica 2021, 38. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of coinfection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 58, 711–712. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Pink, I.; Raupach, D.; Fuge, J.; Vonberg, R.P.; Hoeper, M.M.; Welte, T.; Rademacher, J. C-reactive protein and procalcitonin for antimicrobial stewardship in COVID-19. Infection 2021, 20, 1–9. [Google Scholar] [CrossRef]
- Buehler, P.K.; Zinkernagel, A.S.; Hofmaenner, D.A.; Garcia, P.D.W.; Acevedo, C.T.; Gómez-Mejia, A.; Shambat, S.M.; Andreoni, F.; Maibach, M.A.; Bartussek, J.; et al. Bacterial pulmonary superinfections are associated with longer duration of ventilation in critically ill COVID-19 patients. Cell Rep. Med. 2021, 2, 100229. [Google Scholar] [CrossRef] [PubMed]
- Ripa, M.; Galli, L.; Poli, A.; Oltolini, C.; Spagnuolo, V.; Mastrangelo, A.; Muccini, C.; Monti, G.; De Luca, G.; Landoni, G.; et al. COVID-BioB study group. Secondary infections in patients hospitalized with COVID-19: Incidence and predictive factors. Clin. Microbiol. Infect. 2021, 27, 451–457. [Google Scholar] [CrossRef]
- Lugito, N.P.H. Is procalcitonin a part of human immunological response to SARS-CoV-2 infection or “just” a marker of bacterial coinfection? Curr. Res. Transl. Med. 2021, 69, 103289. [Google Scholar] [CrossRef] [PubMed]
- Foschi, C.; Zignoli, A.; Gaibani, P.; Vocale, C.; Rossini, G.; Lafratta, S.; Liberatore, A.; Turello, G.; Lazzarotto, T.; Ambretti, S. Respiratory bacterial coinfections in intensive care unit-hospitalized COVID-19 patients: Conventional culture vs BioFire FilmArray pneumonia Plus panel. J. Microbiol. Methods 2021, 186, 106259. [Google Scholar] [CrossRef]
- Ng, J.H.; Bijol, V.; Sparks, M.A.; Sise, M.E.; Izzedine, H.; Jhaveri, K.D. Pathophysiology and Pathology of Acute Kidney Injury in Patients with COVID-19. Adv. Chronic Kidney Dis. 2020, 27, 365–376. [Google Scholar] [CrossRef]
- Sharma, P.; Uppal, N.N.; Wanchoo, R.; Shah, H.H.; Yang, Y.; Parikh, R.; Khanin, Y.; Madireddy, V.; Larsen, C.P.; Jhaveri, K.D.; et al. COVID-19-Associated Kidney Injury: A Case Series of Kidney Biopsy Findings. J. Am. Soc. Nephrol. 2020, 31, 1948–1958. [Google Scholar] [CrossRef]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; et al. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef] [PubMed]
- Golmai, P.; Larsen, C.P.; DeVita, M.V.; Wahl, S.J.; Weins, A.; Rennke, H.G.; Bijol, V.; Rosenstock, J.L. Histopathologic and Ultrastructural Findings in Postmortem Kidney Biopsy Material in 12 Patients with AKI and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1944–1947. [Google Scholar] [CrossRef]
- Santoriello, D.; Khairallah, P.; Bomback, A.S.; Xu, K.; Kudose, S.; Batal, I.; Barasch, J.; Radhakrishnan, J.; D’Agati, V.; Markowitz, G. Postmortem Kidney Pathology Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 2158–2167. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. COVID-19 Clinical Management: Living Guidance. 25 January 2021. Available online: https//www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 6 June 2021).
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Campogiani, L.; Tejada, S.; Ferreira-Coimbra, J.; Restrepo, M.I.; Rello, J. Evidence supporting recommendations from international guidelines on treatment, diagnosis, and prevention of HAP and VAP in adults. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 483–491. [Google Scholar] [CrossRef]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef] [PubMed]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Housman, B.; Jacobi, A.; Carollo, A.; Nobel, T.; Eber, C.; Acquah, S.; Powell, C.; Kaufman, A.; Lee, D.S.; Nicastri, D.; et al. COVID-19 ventilator barotrauma management: Less is more. Ann. Transl. Med. 2020, 8, 1575. [Google Scholar] [CrossRef] [PubMed]
- Morassi, M.; Bagatto, D.; Cobelli, M.; D′Agostini, S.; Gigli, G.L.; Bnà, C.; Vogrig, A. Stroke in patients with SARS-CoV-2 infection: Case series. J. Neurol. 2020, 267, 2185–2192. [Google Scholar] [CrossRef]
- Wilkins, T.; Wheeler, B.; Carpenter, M. Upper Gastrointestinal Bleeding in Adults: Evaluation and Management. Am. Fam. Physician 2020, 101, 294–300. [Google Scholar] [PubMed]
- Turagam, M.K.; Musikantow, D.; Goldman, M.E.; Bassily-Marcus, A.; Chu, E.; Shivamurthy, P.; Lampert, J.; Kawamura, I.; Bokhari, M.; Whang, W.; et al. Malignant Arrhythmias in Patients With COVID-19: Incidence, Mechanisms, and Outcomes. Circ. Arrhythm. Electrophysiol. 2020, 13, e008920. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.W.; Holmberg, M.J.; Berg, K.M.; Donnino, M.W.; Granfeldt, A. In-Hospital Cardiac Arrest: A Review. JAMA 2019, 321, 1200–1210. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | All Patients (n = 124) | Survivors (n = 83) | Non-Survivors (n = 41) | p Value |
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Age, years * | 54.47 (±12.03) | 54.16 (±11.93) | 61 (±10.92) | 0.002a |
| Age range, years | ||||
| <50 (%) | 39 (31.45) | 31 (79.49) | 8 (20.51) | 0.058 b |
| 50–59 (%) | 38 (30.65) | 26 (68.42) | 12 (31.58) | |
| ≥60 (%) | 47 (37.90) | 26 (55.32) | 21 (44.68) | |
| Sex | 0.388 b | |||
| Female (%) | 22 (17.74) | 13 (59.09) | 9 (40.91) | |
| Male (%) | 102 (82.26) | 70 (68.63) | 32 (31.37) | |
| Number of comorbidities ** | 1 (1–2) | 1 (1–2) | 2 (1–3) | <0.001c |
| Comorbidities (%) | ||||
| None | 18 (14.52) | 18 (100) | 0 (0) | 0.001b |
| 1 | 49 (39.52) | 35 (71.43) | 14 (28.57) | |
| 2 or more | 57 (45.97) | 30 (52.63) | 27 (47.37) | |
| Obesity | 76 (61.29) | 50 (65.79) | 26 (34.21) | 0.733 b |
| Diabetes | 35 (28.23) | 19 (54.29) | 16 (45.71) | 0.060 b |
| Hypertension | 35 (28.23) | 18 (51.43) | 17 (48.57) | 0.021b |
| Heart failure | 8 (6.45) | 0 (0) | 8 (100) | <0.001d |
| Asthma | 24 (19.35) | 12 (50) | 12 (50) | 0.050b |
| Chronic kidney disease | 7 (5.65) | 0 (0) | 7 (100) | <0.001d |
| Cancer | 1 (0.81) | 1 (100) | 0 (0) | 0.990 d |
| Immunosuppression | 17 (13.82) | 6 (35.29) | 11 (64.71) | 0.003b |
| Length of hospital stay (days) | 19 (14–27.5) | 20 (14–26) | 18 (14–28) | 0.638 c |
| Time in ICU (days) ** | 10 (6–16.5) | 9 (5–13) | 12 (10–24) | 0.001c |
| Time in MV (days) ** | 10 (5–16.5) | 7 (4–12) | 14 (11–25) | <0.001c |
| Time from ICU admission to superinfection (days) ** | 8 (6–17) | 9 (6–17) | 8 (5–15) | 0.680 c |
| Laboratory Characteristics | ||||
| SatO2 (%) ** | 87 (80–89) | 88 (85–90) | 85 (77–89) | 0.008c |
| Ratio PaO2/FiO2 ** | 249.5 (175–294) | 264 (215–306) | 218 (132–260) | 0.002c |
| Leukocytes (cells/mm3) ** | 10,100 (7000–13,000) | 10,000 (7000–12,135) | 10,700 (7410–16,580) | 0.232 c |
| Percentages of lymphocytes (%) ** | 7 (5–10) | 7 (6–11) | 7 (4–9) | 0.076 c |
| Platelets (cells/mm3) ** | 296,000 (234,500–360,000) | 318,000 (254,000–369,000) | 243,000 (204,000–325,000) | 0.002c |
| PCR (mg/dL) ** | 12.52 (6.62–17.43) | 10.56 (4.72–18) | 14.23 (10.78–17.25) | 0.032c |
| Procalcitonin (ng/mL) ** | 0.12 (0.03–0.385) | 0.07 (0.03–0.24) | 0.22 (0.126–0.7) | <0.001c |
| LDH (U/L) ** | 742.5 (578–984) | 700 (565–861) | 970 (642–1286) | 0.001c |
| CPK-Total (U/L) ** | 100 (52.5–190.5) | 87 (45–161) | 161 (79–233) | 0.004c |
| CPK-MB (U/L) ** | 25.25 (20–35) | 24.6 (19.6–32) | 30 (22–52) | 0.025c |
| GOT (U/L) ** | 50.5 (28–75.5) | 50 (28–75) | 54 (28–84) | 0.614 c |
| GPT (U/L) ** | 62.5 (37–116) | 66 (44–133) | 57 (34–82) | 0.021c |
| Total bilirubin (mg/dL) ** | 0.63 (0.39–0.895) | 0.6 (0.37–0.89) | 0.63 (0.47–0.96) | 0.353 c |
| Creatinine (mg/dL) ** | 0.875 (0.73–1.1) | 0.84 (0.7–1.05) | 0.97 (0.84–1.29) | 0.003c |
| Variable | All Patients (n = 124) | Survivors (n = 83) | Non-Survivors (n = 41) | p Value |
|---|---|---|---|---|
| Complications in ICU | ||||
| Healthcare-associated infection (%) | <0.001a | |||
| No | 74 (59.68) | 62 (83.78) | 12 (16.22) | |
| Yes | 50 (40.32) | 21 (42) | 29 (58) | |
| Type of superinfection | ||||
| MV-associated pneumonia (%) | <0.001a | |||
| No | 87 (70.16) | 67 (77.01) | 20 (22.99) | |
| Yes | 37 (29.84) | 16 (43.24) | 21 (56.76) | |
| Catheter-associated bacteremia (%) | 0.080 b | |||
| No | 114 (91.94) | 79 (69.30) | 35 (30.70) | |
| Yes | 10 (8.06) | 4 (40) | 6 (60) | |
| Catheter-associated UTI (%) | 0.254 b | |||
| No | 121 (97.58) | 82 (67.77) | 39 (32.23) | |
| Yes | 3 (2.42) | 1 (33.33) | 2 (66.67) | |
| Bacterial resistance (%) | ||||
| No MDR/XDR | 0.301 b | |||
| No | 120 (96.77) | 79 (65.83) | 41 (34.17) | |
| Yes | 4 (3.23) | 4 (100) | 0 (0) | |
| MDR | 0.092 b | |||
| No | 118 (95.16) | 81 (68.64) | 37 (31.36) | |
| Yes | 6 (4.84) | 2 (33.33) | 4 (66.67) | |
| XDR | <0.001a | |||
| No | 84 (67.74) | 68 (80.95) | 16 (19.05) | |
| Yes | 40 (32.26) | 15 (37.50) | 25 (62.50) | |
| Sepsis (%) | 0.002a | |||
| No | 41 (33.06) | 35 (85.37) | 6 (14.63) | |
| Yes | 83 (66.94) | 48 (57.83) | 35 (42.17) | |
| Septic shock (%) | <0.001a | |||
| No | 77 (62.10) | 64 (83.12) | 13 (16.88) | |
| Yes | 47 (37.90) | 19 (40.43) | 28 (59.57) | |
| ARDS (%) | 124 (100) | 83 (66.94) | 41 (33.06) | - |
| Acute kidney injury (%) | <0.001a | |||
| No | 101 (81.45) | 79 (78.22) | 22 (21.78) | |
| Yes | 23 (18.55) | 4 (17.39) | 19 (82.61) | |
| Gastrointestinal bleeding (%) | 0.034b | |||
| No | 121 (97.58) | 83 (68.60) | 38 (31.40) | |
| Yes | 3 (2.42) | 0 (0) | 3 (100) | |
| Barotrauma (%) | 0.108 b | |||
| No | 122 (98.39) | 83 (68.03) | 39 (31.97) | |
| Yes | 2 (1.61) | 0 (0) | 2 (100) | |
| Stroke (%) | 0.108 b | |||
| No | 122 (98.39) | 83 (68.03) | 39 (31.97) | |
| Yes | 2 (1.61) | 0 (0) | 2 (100) | |
| Arrhythmia (%) | <0.001a | |||
| No | 117 (94.35) | 83 (70.94) | 34 (29.06) | |
| Yes | 7 (5.65) | 0 (0) | 7 (100) | |
| Cardiac arrest (%) | <0.001a | |||
| No | 94 (75.81) | 82 (87.23) | 12 (12.77) | |
| Yes | 30 (24.19) | 1 (3.33) | 29 (96.67) | |
| Number of complications * | 2 (1–3.5) | 3 (2–4) | 2 (1–3) | 0.001c |
| Received antibiotic therapy (%) | 0.998 b | |||
| No | 1 (0.81) | 1 (100) | 0 (0) | |
| Yes | 123 (99.19) | 82 (66.67) | 41 (33.33) | |
| Antibiotic Therapy Received | ||||
| Ceftriaxone (%) | 0.003a | |||
| No | 87 (70.16) | 51 (58.62) | 36 (41.38) | |
| Yes | 37 (29.84) | 32 (86.49) | 5 (13.51) | |
| Azithromycin (%) | 0.029a | |||
| No | 115 (92.74) | 74 (64.35) | 41 (35.65) | |
| Yes | 9 (7.26) | 9 (100) | 0 (0) | |
| Piperacillin/Tazobactam (%) | 0.280 a | |||
| No | 69 (55.65) | 49 (71.01) | 20 (28.99) | |
| Yes | 55 (44.35) | 34 (61.82) | 21 (38.18) | |
| Meropenem (%) | 0.036a | |||
| No | 93 (75) | 67 (72.04) | 26 (27.96) | |
| Yes | 31 (25) | 16 (51.61) | 15 (48.39) | |
| Vancomycin (%) | 0.475 a | |||
| No | 81 (65.32) | 56 (69.14) | 25 (30.86) | |
| Yes | 43 (34.68) | 27 (62.79) | 16 (37.21) | |
| Linezolid (%) | 0.105 b | |||
| No | 120 (96.77) | 82 (68.33) | 38 (31.67) | |
| Yes | 4 (3.23) | 1 (25) | 3 (75) | |
| Colistin (%) | 0.998 a | |||
| No | 123 (99.19) | 82 (66.67) | 41 (33.33) | |
| Yes | 1 (0.81) | 1 (100) | 0 (0) | |
| Received corticosteroid therapy (%) | 0.998 b | |||
| No | 2 (1.63) | 1 (50) | 1 (50) | |
| Yes | 121 (98.37) | 81 (66.94) | 40 (33.06) | |
| Corticosteroid Therapy Received | ||||
| Dexamethasone 4 mg (%) | 0.598 b | |||
| No | 120 (96.77) | 81 (67.5) | 39 (32.5) | |
| Yes | 4 (3.23) | 2 (50) | 2 (50) | |
| Dexamethasone 6 mg (%) | <0.001a | |||
| No | 78 (62.9) | 42 (53.85) | 36 (46.15) | |
| Yes | 46 (37.10) | 41 (89.13) | 5 (10.87) | |
| Methylprednisolone 100 mg (%) | 0.001a | |||
| No | 57 (45.97) | 47 (82.46) | 10 (17.54) | |
| Yes | 67 (54.03) | 36 (53.73) | 31 (46.27) | |
| Methylprednisolone 500 mg (%) | 0.998 b | |||
| No | 116 (93.55) | 78 (67.24) | 38 (32.76) | |
| Yes | 8 (6.45) | 5 (62.50) | 3 (37.50) | |
| Received colchicine therapy (%) | 0.010a | |||
| No | 88 (70.97) | 65 (73.86) | 23 (23.14) | |
| Yes | 36 (29.03) | 18 (50) | 18 (50) | |
| Received tocilizumab therapy (%) | 0.111 a | |||
| No | 98 (79.03) | 69 (70.41) | 29 (29.59) | |
| Yes | 26 (20.97) | 14 (53.85) | 12 (46.15) | |
| Received dialysis therapy (%) | <0.001a | |||
| No | 109 (87.90) | 81 (74.31) | 28 (25.69) | |
| Yes | 15 (12.10) | 2 (13.33) | 13 (86.67) | |
| Received vasopressor therapy (%) | <0.001a | |||
| No | 64 (51.61) | 55 (85.94) | 9 (14.06) | |
| Yes | 60 (48.39) | 28 (46.67) | 32 (53.33) |
| Variable | No Healthcare-Associated Infection (n = 41) | Healthcare-Associated Infection (n = 83) | p Value |
|---|---|---|---|
| Demographic Characteristics | |||
| Age (years) * (%) | 53.67 (±12.31) | 60.62 (±10.38) | 0.001a |
| <50 years (%) | 30 (76.92) | 9 (23.08) | 0.025b |
| 50–59 years (%) | 21 (55.26) | 17 (44.74) | |
| ≥60 years (%) | 23 (48.94) | 24 (51.06) | |
| Sex | 0.370 b | ||
| Female (%) | 15 (68.18) | 7 (31.82) | |
| Male (%) | 59 (57.84) | 43 (42.16) | |
| Number of comorbidities ** | 1 (1–2) | 1 (1–3) | 0.422 c |
| No comorbidity (%) | 13 (72.22) | 5 (27.78) | 0.449 b |
| Only 1 (%) | 27 (55.10) | 22 (44.90) | |
| More than 2 (%) | 34 (59.65) | 23 (40.35) | |
| Obesity (%) | 46 (60.53) | 30 (39.47) | 0.808 b |
| Diabetes (%) | 20 (57.14) | 15 (42.86) | 0.718 b |
| Hypertension (%) | 19 (54.29) | 16 (45.71) | 0.443 b |
| Heart failure (%) | 5 (62.50) | 3 (37.50) | 0.998 d |
| Asthma (%) | 15 (62.50) | 9 (37.50) | 0.754 b |
| Chronic kidney disease (%) | 1 (14.29) | 6 (85.71) | 0.017d |
| Cancer (%) | 1 (100) | 0 (0) | 0.998 d |
| Immunosuppression (%) | 9 (52.94) | 8 (47.06) | 0.512 b |
| Length of hospital stay (days) ** | 17.5 (13–23) | 21.5 (16–32) | 0.003c |
| Time in ICU (days) ** | 8 (4–12) | 13 (10–23) | 0.001c |
| Time in MV (days) ** | 7 (4–11) | 14.5 (10–27) | <0.001c |
| Laboratory Characteristics | |||
| SatO2 (%) ** | 87.5 (84–90) | 85 (78–89) | 0.055 c |
| PaO2/FiO2 ratio ** | 261 (220–307) | 224.5 (136–276) | 0.002c |
| Leukocytes (cells/mm3) ** | 9990 (7000–11,000) | 11,865 (8590–16,810) | 0.011c |
| Percentage of lymphocytes (%) ** | 8 (6–11) | 6.2 (3.7–10) | 0.042c |
| Platelets (cells/mm3) ** | 308,500 (245,000–362,000) | 276,000 (210,000–356,000) | 0.134 c |
| CRP (mg/dL) ** | 11.5 (5.22–17.35) | 13.59 (9.92–17.95) | 0.189 c |
| Procalcitonin (ng/mL) ** | 0.06 (0.03–0.17) | 0.3 (0.126–0.69) | <0.001c |
| LDH (U/L) ** | 691.5 (552–854) | 853 (639–1160) | 0.001c |
| CPK-Total (U/L) ** | 87 (47–161) | 132.5 (66–225) | 0.028c |
| CPK-MB (U/L) ** | 25 (19.9–35) | 27.75 (20–40) | 0.469 c |
| Total bilirubin (mg/dL) ** | 0.68 (0.39–0.90) | 0.615 (0.39–0.83) | 0.624 c |
| Creatinine (mg/dL) ** | 0.84 (0.7–0.98) | 0.96 (0.79–1.25) | 0.002c |
| Treatment Administered | |||
| Received antibiotic therapy (%) | 0.998 d | ||
| No | 1 (100) | 0 (0) | |
| Yes | 73 (59.35) | 50 (40.65) | |
| Antibiotic therapy received | |||
| Ceftriaxone (%) | 0.006b | ||
| No | 45 (51.72) | 42 (48.28) | |
| Yes | 29 (78.38) | 8 (21.62) | |
| Azithromycin (%) | 0.083 d | ||
| No | 66 (57.39) | 49 (42.61) | |
| Yes | 8 (88.89) | 1 (11.11) | |
| Piperacillin/Tazobactam (%) | 0.076 b | ||
| No | 46 (66.67) | 23 (33.33) | |
| Yes | 28 (50.91) | 27 (49.09) | |
| Meropenem (%) | 0.291 b | ||
| No | 58 (62.37) | 35 (37.63) | |
| Yes | 16 (51.61) | 15 (48.39) | |
| Vancomycin (%) | 0.799 b | ||
| No | 49 (60.49) | 32 (39.51) | |
| Yes | 25 (58.14) | 18 (41.86) | |
| Linezolid (%) | 0.998 d | ||
| No | 72 (60) | 48 (40) | |
| Yes | 2 (50) | 2 (50) | |
| Colistin (%) | 0.998 d | ||
| No | 73 (59.35) | 50 (40.65) | |
| Yes | 1 (100) | 0 (0) | |
| Received corticosteroid therapy (%) | 0.085 d | ||
| No | 0 (0) | 2 (100) | |
| Yes | 73 (60.33) | 48 (39.67) | |
| Corticotherapy Received | |||
| Dexamethasone 4 mg (%) | 0.647 d | ||
| No | 71 (59.17) | 49 (40.83) | |
| Yes | 3 (75) | 1 (25) | |
| Dexamethasone 6 mg (%) | 0.013b | ||
| No | 40 (51.28) | 38 (48.72) | |
| Yes | 34 (73.91) | 12 (26.09) | |
| Methylprednisolone 100 mg (%) | 0.067 b | ||
| No | 39 (68.42) | 18 (31.58) | |
| Yes | 35 (52.24) | 32 (47.76) | |
| Methylprednisolone 500 mg (%) | 0.266 d | ||
| No | 71 (61.21) | 45 (38.79) | |
| Yes | 3 (37.50) | 5 (62.50) | |
| Received colchicine therapy (%) | 0.071 b | ||
| No | 57 (64.77) | 31 (35.23) | |
| Yes | 17 (47.22) | 19 (52.78) | |
| Received tocilizumab therapy (%) | 0.258 b | ||
| No | 61 (62.24) | 37 (37.76) | |
| Yes | 13 (50) | 13 (50) | |
| Received dialysis therapy (%) | 0.001b | ||
| No | 71 (65.14) | 38 (34.86) | |
| Yes | 3 (20) | 12 (80) | |
| Received vasopressor therapy (%) | 0.004b | ||
| No | 46 (71.88) | 18 (28.13) | |
| Yes | 28 (46.67) | 32 (53.33) |
| Crude Model | Adjusted Model | |||
|---|---|---|---|---|
| Variable | cHR (95% CI) | pValue | aHR (95% CI) | pValue |
| Healthcare-associated infection | 2.216 (1.12–4.39) | 0.023 | 2.733 (1.33–5.60) | 0.006 |
| Age ≥ 60 years | 1.045 (0.45–2.40) | 0.917 | 0.937 (0.32–2.72) | 0.905 |
| Male | 0.685 (0.33–1.44) | 0.320 | 0.582 (0.35–1.80) | 0.582 |
| Obesity | 1.581 (0.82–3.02) | 0.166 | 2.605 (1.11–6.07) | 0.027 |
| Diabetes | 1.804 (0.95–3.40) | 0.068 | 1.903 (0.90–4.00) | 0.090 |
| Hypertension | 1.375 (0.73–2.57) | 0.319 | 1.172 (0.51–2.65) | 0.703 |
| Asthma | 1.461 (0.74–2.88) | 0.273 | 1.463 (0.66–3.23) | 0.346 |
| Heart failure | 2.670 (1.22–5.83) | 0.014 | 4.701 (1.58–13.97) | 0.005 |
| PaO2/FiO2 | ||||
| +300 | Ref | Ref | ||
| 200–300 | 2.559 (0.75–8.66) | 0.131 | 4.256 (1.14–15.80) | 0.044 |
| 100–200 | 3.917 (1.05–14.51) | 0.041 | 3.796 (1.01–14.47) | 0.050 |
| −100 | 5.011 (1.37–18.25) | 0.015 | 5.503 (1.34–22.52) | 0.018 |
| Crude Model | Adjusted Mode | |||
| Variable | cRR (95% CI) | pValue | aRR (95% CI) | pValue |
| Healthcare-associated infection | 3.594 (1.60–8.05) | 0.002 | 3.093 (1.42–6.72) | 0.004 |
| Age ≥ 60 years | 1.797 (0.75–4.30) | 0.188 | 1.370 (0.50–3.69) | 0.533 |
| Male | 1.509 (0.49–4.64) | 0.472 | 1.935 (0.56–6.59) | 0.291 |
| Obesity | 1.533 (0.68–3.43) | 0.298 | 2.537 (1.16–5.54) | 0.019 |
| Diabetes | 1.525 (0.73–3.16) | 0.257 | 1.091 (0.49–2.40) | 0.828 |
| Hypertension | 2.151 (1.06–4.35) | 0.033 | 1.504 (0.66–3.40) | 0.327 |
| Asthma | 1.715 (0.80–3.67) | 0.165 | 2.358 (1.19–4.96) | 0.024 |
| Heart failure | 2.9 (1.29–6.47) | 0.009 | 2.045 (0.67–6.21) | 0.207 |
| PaO2/FiO2 | ||||
| +300 | Ref | Ref | ||
| 200–300 | 2.306 (0.54–9.74) | 0.256 | 1.946 (0.51–7.35) | 0.326 |
| 100–200 | 2.052 (0.37–11.18) | 0.406 | 1.169 (0.23–5.92) | 0.850 |
| −100 | 6.117 (1.46–25.55) | 0.013 | 3.972 (0.97–16.22) | 0.055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Copaja-Corzo, C.; Hueda-Zavaleta, M.; Benites-Zapata, V.A.; Rodriguez-Morales, A.J. Antibiotic Use and Fatal Outcomes among Critically Ill Patients with COVID-19 in Tacna, Peru. Antibiotics 2021, 10, 959. https://doi.org/10.3390/antibiotics10080959
Copaja-Corzo C, Hueda-Zavaleta M, Benites-Zapata VA, Rodriguez-Morales AJ. Antibiotic Use and Fatal Outcomes among Critically Ill Patients with COVID-19 in Tacna, Peru. Antibiotics. 2021; 10(8):959. https://doi.org/10.3390/antibiotics10080959
Chicago/Turabian StyleCopaja-Corzo, Cesar, Miguel Hueda-Zavaleta, Vicente A. Benites-Zapata, and Alfonso J. Rodriguez-Morales. 2021. "Antibiotic Use and Fatal Outcomes among Critically Ill Patients with COVID-19 in Tacna, Peru" Antibiotics 10, no. 8: 959. https://doi.org/10.3390/antibiotics10080959