
Online Exercise Training Program for Brazilian Older Adults: Effects on Physical Fitness and Health-Related Variables of a Feasibility Study in Times of COVID-19


Abstract
:1. Introduction
2. Materials and Methods
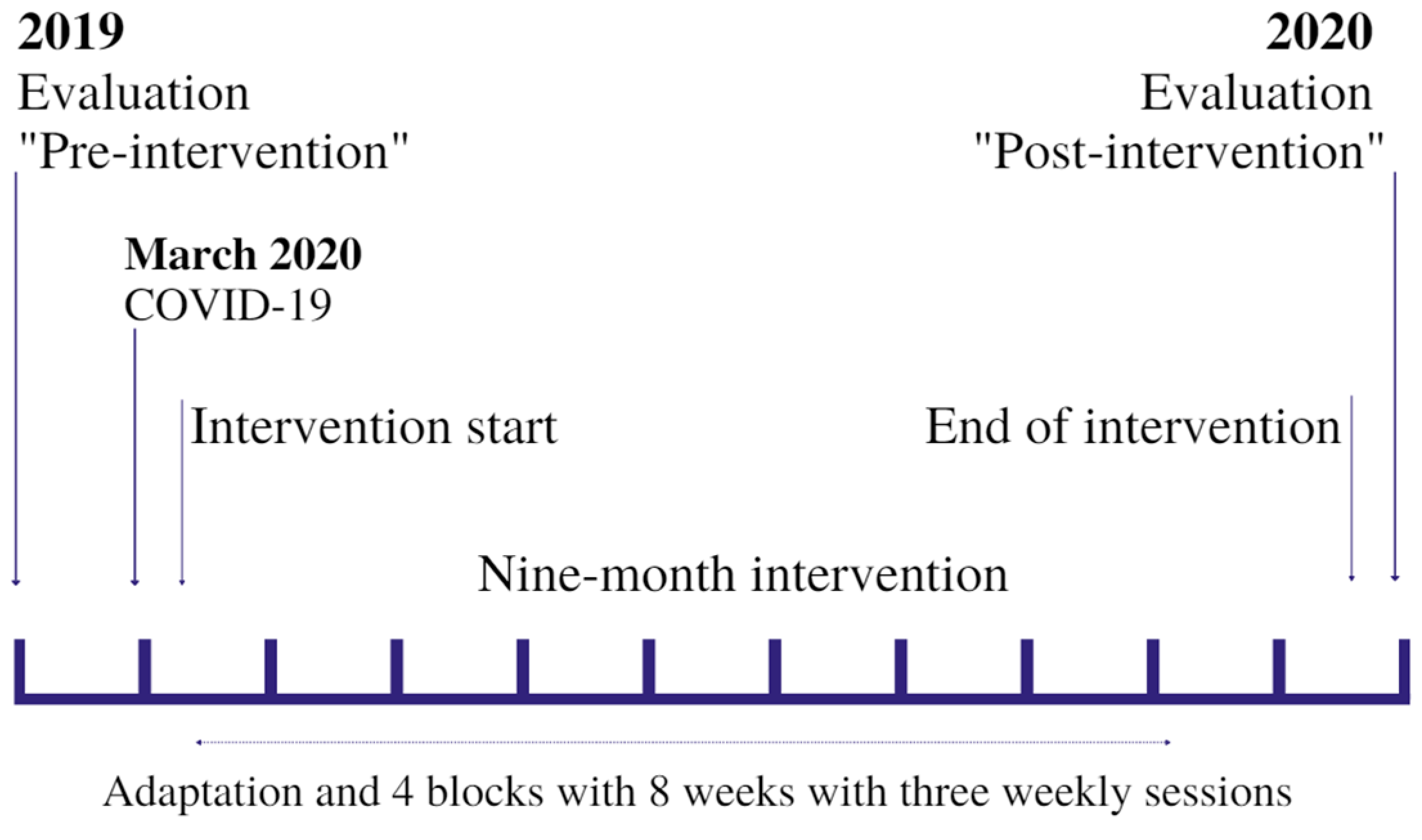
2.1. Study Design
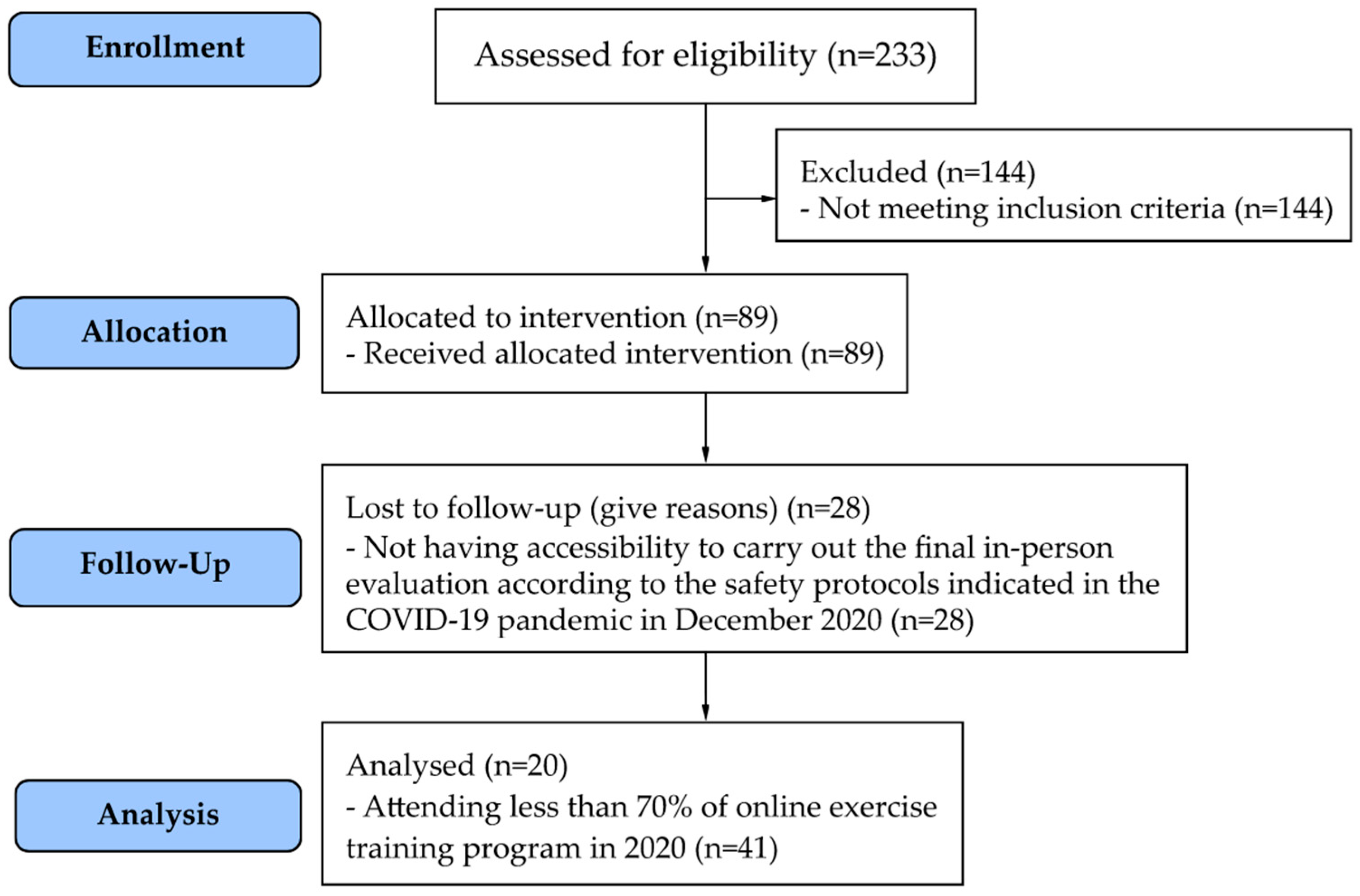
2.2. Participants
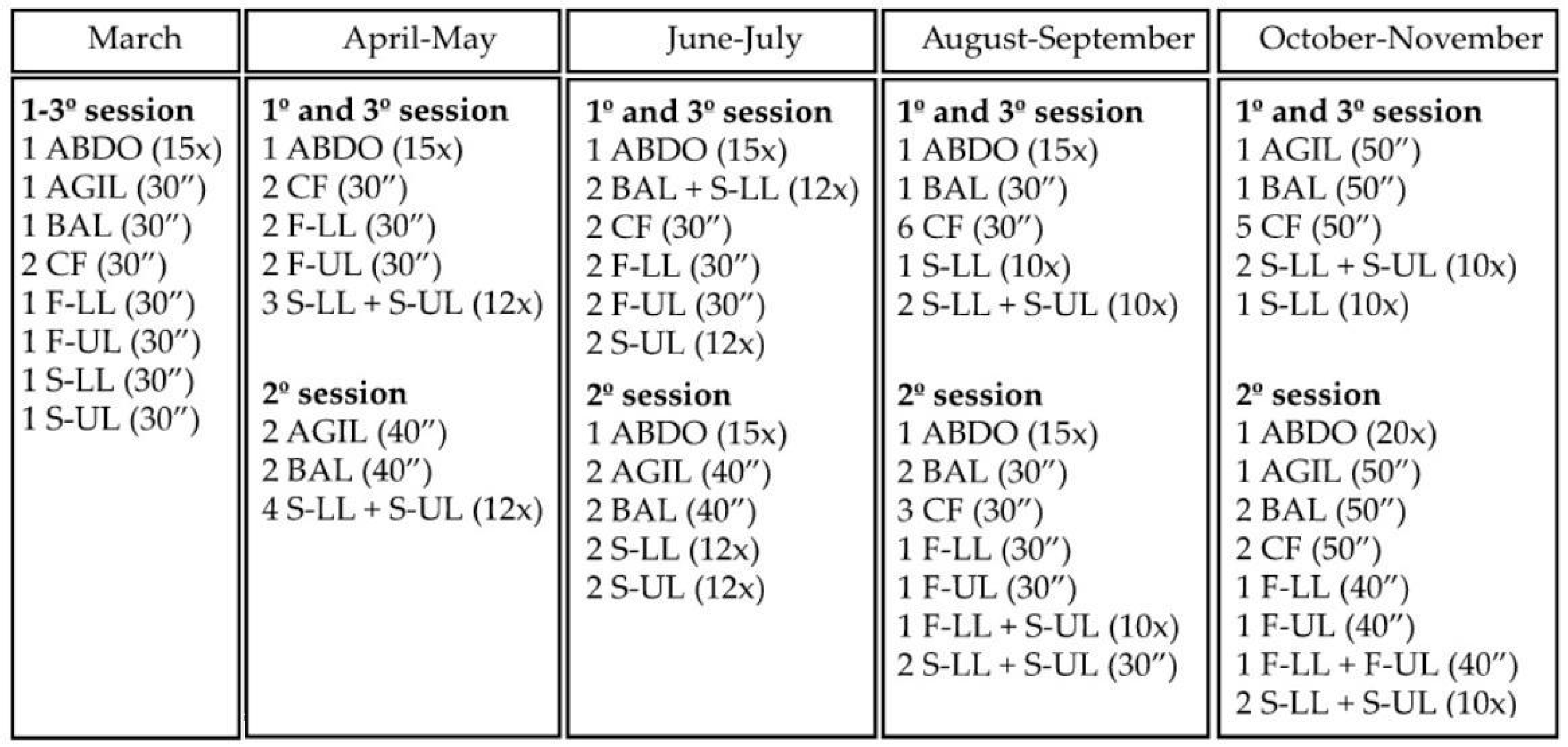
2.3. Intervention
2.4. Instruments
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristic
3.2. Physical Fitness Outcomes
3.3. Health-Related Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of home quarantine on physical activity for older adults living at home during the Covid-19 pandemic: Qualitative interview study (Preprint). JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; Current Guidelines; Health.gov: Washington, DC, USA. Available online: https://health.gov/our-work/nutrition-physical-activity/physical-activity-guidelines/current-guidelines (accessed on 10 March 2022).
- Bouaziz, W.; Lang, P.O.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Vogel, T. Health benefits of multicomponent training programmes in seniors: A systematic review. Int. J. Clin. Pract. 2016, 70, 520–536. [Google Scholar] [CrossRef]
- World Health Organization. Stay Physically Active during Self-Quarantine. Who.int. 2020. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/publications-and-technical-guidance/noncommunicable-diseases/stay-physically-active-during-self-quarantine (accessed on 13 March 2022).
- American College of Sports Medicine. Staying Active During COVID-19-Exercise Is Medicine. 4 August 2020. Available online: https://www.exerciseismedicine.org/staying-active-during-covid-191/ (accessed on 7 March 2022).
- Cohen-Mansfield, J.; Muff, A.; Meschiany, G.; Lev-Ari, S. Adequacy of Web-Based Activities as a Substitute for In-Person Activities for Older Persons during the COVID-19 Pandemic: Survey Study. J. Med. Internet Res. 2021, 23, e25848. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, H.; Har-Nir, I.; Wenhoda, T.; Halperin, I. Staying physically active during the COVID-19 quarantine: Exploring the feasibility of live, online, group training sessions among older adults. Transl. Behav. Med. 2021, 11, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Izawa, K.P. Effectiveness and feasibility of home-based telerehabilitation for community-dwelling elderly people in Southeast Asian countries and regions: A systematic review. Aging Clin. Exp. Res. 2021, 33, 2657–2669. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Fitzgerald, K.; Winters-Stone, K. A cognitively enhanced online Tai Ji Quan training intervention for community-dwelling older adults with mild cognitive impairment: A feasibility trial. BMC Geriatr. 2022, 22, 76. [Google Scholar] [CrossRef]
- Gonçalves, A.K.; Griebler, E.M.; da Silva, W.A.; Sant′Helena, D.P.; da Silva, P.C.; Possamai, V.D.; Martins, V.F. Does a Multicomponent Exercise Program Improve Physical Fitness in Older Adults? Findings from a 5-Year Longitudinal Study. J. Aging Phys. Act. 2021, 29, 814–821. [Google Scholar] [CrossRef]
- Zhao, Y.; Chung, P.-K.; Tong, T.K. Effectiveness of a community-based exercise program on balance performance and fear of falling in older nonfallers at risk for falling: A Randomized, Controlled Study. J. Aging Phys. Act. 2016, 24, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls Efficacy as a Measure of Fear of Falling. J. Gerontol. 1990, 45, P239–P243. [Google Scholar] [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 433–483. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Vitale, J.A.; Bonato, M.; Borghi, S.; Messina, C.; Albano, D.; Corbetta, S.; Sconfienza, L.M.; Banfi, G. Home-Based Resistance Training for Older Subjects during the COVID-19 Outbreak in Italy: Preliminary Results of a Six-Months RCT. Int. J. Environ. Res. Public Health 2020, 17, 9533. [Google Scholar] [CrossRef] [PubMed]
- Yi, D.; Yim, J. Remote home-based exercise program to improve the mental state, balance, and physical function and prevent falls in adults aged 65 years and older during the COVID-19 pandemic in Seoul, Korea. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 21, e935496. [Google Scholar] [CrossRef]
- Todde, F.; Melis, F.; Mura, R.; Pau, M.; Fois, F.; Magnani, S.; Ibba, G.; Crisafulli, A.; Tocco, F. A 12-Week Vigorous Exercise Protocol in a Healthy Group of Persons over 65: Study of Physical Function by means of the Senior Fitness Test. BioMed Res. Int. 2016, 2016, 7639842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, V.F.; Gonçalves, A.K.; Griebler, E.M.; Possamai, V.D.; Sant’Helena, D.P.; Silva, P.C.; Silva, W.A. Health-related quality of life of older Brazilians from a physical program: A 5-year longitudinal study. Int. J. Dev. Res. 2020, 10, 39240–39246. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Dewey, J.E.; Gandek, B. How to Score and Interpret Single-Item Health Status Measures: A Manual for Users of the SF-8 Health Survey; Quality Metric Inc.: Lincoln, UK, 2001. [Google Scholar]
- Sato, Y.; Ouchi, J.; Hayashi, Y.; Matsubara, M.; Yamamoto, M.; Sanada, H.; Wada, N. Health-related Quality of Life of Community-dwelling Elderly during the COVID-19 Pandemic. Rigakuryoho Kagaku 2020, 35, 813–818. [Google Scholar] [CrossRef]
- Halaweh, H.; Willen, C.; Grimby-Ekman, A.; Svantesson, U. Physical Activity and Health-Related Quality of Life among Community Dwelling Elderly. J. Clin. Med. Res. 2015, 7, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, J.; Borges-Machado, F.; Pizarro, A.N.; Bohn, L.; Barros, D. Home Confinement in Previously Active Older Adults: A Cross-Sectional Analysis of Physical Fitness and Physical Activity Behavior and Their Relationship with Depressive Symptoms. Front. Psychol. 2021, 12, 643832. [Google Scholar] [CrossRef] [PubMed]
- Maggi, G.; Baldassarre, I.; Barbaro, A.; Cavallo, N.D.; Cropano, M.; Nappo, R.; Santangelo, G. Mental health status of Italian elderly subjects during and after quarantine for the COVID-19 pandemic: A cross-sectional and longitudinal study. Psychogeriatrics 2021, 21, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Chen, W.; Xin, X.; Yin, Y.; Hu, J.; Lv, H.; Li, W.; Deng, X.; Zhu, C.; Zhu, J.; et al. Epidemiologic characteristics of traumatic fractures in elderly patients during the outbreak of coronavirus disease 2019 in China. Int. Orthop. 2020, 44, 1565–1570. [Google Scholar] [CrossRef]
- Briguglio, M.; Giorgino, R.; Dell’Osso, B.; Cesari, M.; Porta, M.; Lattanzio, F.; Banfi, G.; Peretti, G.M. Consequences for the Elderly After COVID-19 Isolation: FEaR (Frail Elderly amid Restrictions). Front. Psychol. 2020, 11, 565052. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | 2019 | 2020 | p | d | ∆ | |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||||
| Physical Fitness | Lower limb strength (rep) | 18.3 ± 5.1 | 19.6 ± 5.4 | 0.150 | 0.24 | 1.25 |
| Upper limb strength (rep) | 20.1 ± 3.9 | 22.8 ± 5.2 | 0.001 * | 0.59 | 2.75 | |
| Lower limb flexibility (cm) | −0.7 ± 10.7 | −0.1 ± 12.7 | 0.760 | 0.05 | 0.55 | |
| Upper limb flexibility (cm) | −4.6 ± 9.6 | −3.2 ± 10.6 | 0.290 | 0.14 | 1.46 | |
| Balance and agility (s) | 4.3 ± 0.5 | 4.9 ± 0.5 | <0.001 * | 1.16 | 0.64 | |
| Cardiorespiratory fitness (rep) | 95.2 ± 17.5 | 99.6 ± 13.9 | 0.180 | 0.28 | 4.40 | |
| Quality of life-related | Geriatric Depression Scale (pts) | 1.8 ± 2.2 | 2.5 ± 1.8 | 0.120 | −0.31 | 0.65 |
| Falls Efficacy Scale (pts) | 22.6 ± 5.8 | 23.2 ± 4.9 | 0.530 | −0.12 | 0.65 | |
| SF-36/physical functioning (pts) | 87.0 ± 16.9 | 71.4 ± 23.4 | <0.001 * | 0.76 | −15.60 | |
| SF-36/role-physical (pts) | 93.7 ± 13.7 | 69.1 ± 40.5 | 0.001 * | 0.81 | −24.65 | |
| SF-36/bodily pain (pts) | 67.0 ± 20.2 | 69.2 ± 22.8 | 0.642 | −0.09 | 2.15 | |
| SF-36/general health (pts) | 88.2 ± 37.1 | 71.9 ± 16.4 | 0.058 | 0.55 | −16.25 | |
| SF-36/vitality (pts) | 77.7 ± 17.5 | 77.0 ± 18.2 | 0.742 | 0.03 | −0.75 | |
| SF-36/social functioning (pts) | 88.1 ± 16.9 | 88.6 ± 19.4 | 0.878 | −0.02 | 0.50 | |
| SF-36/role-emotional (pts) | 86.5 ± 27.5 | 72.1 ± 36.3 | 0.018 * | 0.44 | −14.46 | |
| SF-36/mental health (pts) | 83.4 ± 16.4 | 82.0 ± 18.1 | 0.551 | 0.08 | −1.40 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Silva, W.A.; Martins, V.F.; Haas, A.N.; Gonçalves, A.K. Online Exercise Training Program for Brazilian Older Adults: Effects on Physical Fitness and Health-Related Variables of a Feasibility Study in Times of COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 14042. https://doi.org/10.3390/ijerph192114042
da Silva WA, Martins VF, Haas AN, Gonçalves AK. Online Exercise Training Program for Brazilian Older Adults: Effects on Physical Fitness and Health-Related Variables of a Feasibility Study in Times of COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(21):14042. https://doi.org/10.3390/ijerph192114042
Chicago/Turabian Styleda Silva, Wagner Albo, Valéria Feijó Martins, Aline Nogueira Haas, and Andréa Kruger Gonçalves. 2022. "Online Exercise Training Program for Brazilian Older Adults: Effects on Physical Fitness and Health-Related Variables of a Feasibility Study in Times of COVID-19" International Journal of Environmental Research and Public Health 19, no. 21: 14042. https://doi.org/10.3390/ijerph192114042