
A Retrospective, Monocentric Study Comparing Co and Secondary Infections in Critically Ill COVID-19 and Influenza Patients

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Clinical Data upon ICU Admission
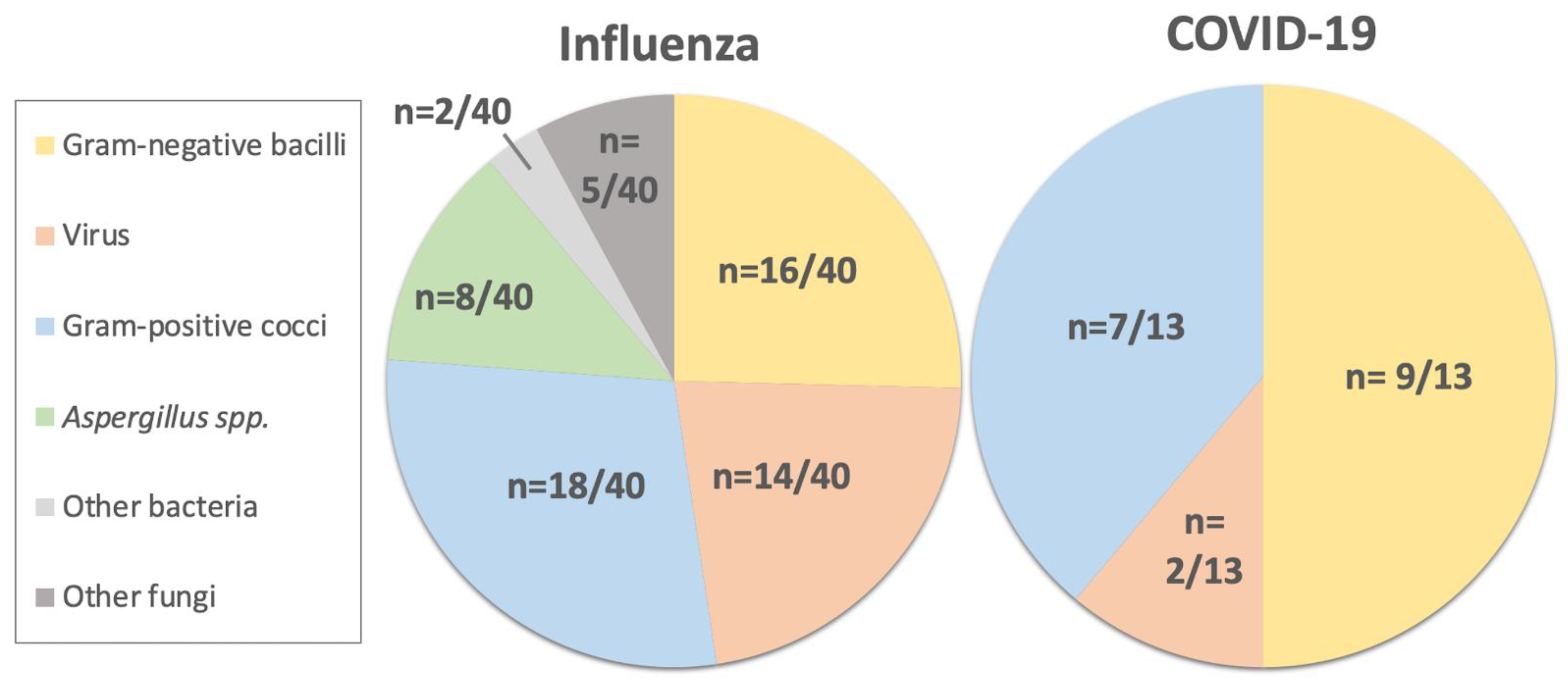
2.3. Co-Infections
2.4. Secondary Infections
2.5. Outcome and Risk Factors for ICU Death
3. Discussion
4. Materials and Methods
4.1. Data Collection
4.2. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mortality Analyses. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 22 August 2021).
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Hingrat, Q.L.; et al. Clinical and Virological Data of the First Cases of COVID-19 in Europe: A Case Series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-Infections in People with COVID-19: A Systematic Review and Meta-Analysis. J. Infect. 2020, 81, 255–275. [Google Scholar] [CrossRef] [PubMed]
- Soriano, M.C.; Vaquero, C.; Ortiz-Fernández, A.; Caballero, A.; Blandino-Ortiz, A.; de Pablo, R. Low Incidence of Co-Infection, but High Incidence of ICU-Acquired Infections in Critically Ill Patients with COVID-19. J. Infect. 2020, 82, e20–e21. [Google Scholar] [CrossRef] [PubMed]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and Viral Co-Infections in Patients with Severe SARS-CoV-2 Pneumonia Admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef]
- Kreitmann, L.; Monard, C.; Dauwalder, O.; Simon, M.; Argaud, L. Early Bacterial Co-Infection in ARDS Related to COVID-19. Intensive Care Med. 2020, 46, 1787–1789. [Google Scholar] [CrossRef]
- Razazi, K.; Arrestier, R.; Haudebourg, A.F.; Benelli, B.; Carteaux, G.; Decousser, J.-W.; Fourati, S.; Woerther, P.L.; Schlemmer, F.; Charles-Nelson, A.; et al. Risks of Ventilator-Associated Pneumonia and Invasive Pulmonary Aspergillosis in Patients with Viral Acute Respiratory Distress Syndrome Related or Not to Coronavirus 19 Disease. Crit. Care Lond. Engl. 2020, 24, 699. [Google Scholar] [CrossRef]
- Elabbadi, A.; Turpin, M.; Gerotziafas, G.T.; Teulier, M.; Voiriot, G.; Fartoukh, M. Bacterial Coinfection in Critically Ill COVID-19 Patients with Severe Pneumonia. Infection 2021, 49, 559–562. [Google Scholar] [CrossRef]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial Infections Associated to COVID-19 in the Intensive Care Unit: Clinical Characteristics and Outcome. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2021, 40, 495–502. [Google Scholar] [CrossRef]
- Kokkoris, S.; Papachatzakis, I.; Gavrielatou, E.; Ntaidou, T.; Ischaki, E.; Malachias, S.; Vrettou, C.; Nichlos, C.; Kanavou, A.; Zervakis, D.; et al. ICU-Acquired Bloodstream Infections in Critically Ill Patients with COVID-19. J. Hosp. Infect. 2021, 107, 95–97. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial Co-Infection and Secondary Infection in Patients with COVID-19: A Living Rapid Review and Meta-Analysis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.-H.; Dugas, A. The Frequency of Influenza and Bacterial Coinfection: A Systematic Review and Meta-Analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Loeches, I.; Schultz, M.J.; Vincent, J.-L.; Alvarez-Lerma, F.; Bos, L.D.; Solé-Violán, J.; Torres, A.; Rodriguez, A. Increased Incidence of Co-Infection in Critically Ill Patients with Influenza. Intensive Care Med. 2017, 43, 48–58. [Google Scholar] [CrossRef] [PubMed]
- McCullers, J.A. The Co-Pathogenesis of Influenza Viruses with Bacteria in the Lung. Nat. Rev. Microbiol. 2014, 12, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Piroth, L.; Cottenet, J.; Mariet, A.-S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the Characteristics, Morbidity, and Mortality of COVID-19 and Seasonal Influenza: A Nationwide, Population-Based Retrospective Cohort Study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar] [CrossRef]
- Shafran, N.; Shafran, I.; Ben-Zvi, H.; Sofer, S.; Sheena, L.; Krause, I.; Shlomai, A.; Goldberg, E.; Sklan, E.H. Secondary Bacterial Infection in COVID-19 Patients Is a Stronger Predictor for Death Compared to Influenza Patients. Sci. Rep. 2021, 11, 12703. [Google Scholar] [CrossRef]
- D’Onofrio, V.; Van Steenkiste, E.; Meersman, A.; Waumans, L.; Cartuyvels, R.; Van Halem, K.; Messiaen, P.; Gyssens, I.C. Differentiating Influenza from COVID-19 in Patients Presenting with Suspected Sepsis. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2021, 40, 987–995. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://Www.Covid19treatmentguidelines.Nih.Gov/ (accessed on 17 August 2021).
- Rothe, K.; Lahmer, T.; Rasch, S.; Schneider, J.; Spinner, C.D.; Wallnöfer, F.; Wurst, M.; Schmid, R.M.; Waschulzik, B.; Fuest, K.; et al. Dexamethasone Therapy and Rates of Secondary Pulmonary and Bloodstream Infections in Critically Ill COVID-19 Patients. Multidiscip. Respir. Med. 2021, 16, 793. [Google Scholar] [CrossRef]
- Rubio-Rivas, M.; Forero, C.G.; Mora-Luján, J.M.; Montero, A.; Formiga, F.; Homs, N.A.; Albà-Albalate, J.; Sánchez, L.; Rello, J.; Corbella, X. Beneficial and Harmful Outcomes of Tocilizumab in Severe COVID-19: A Systematic Review and Meta-analysis. Pharmacotherapy 2021, 41, 884–906. [Google Scholar] [CrossRef]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of Invasive Pulmonary Aspergillosis Among Intubated Patients With COVID-19: A Prospective Study. Clin. Infect. Dis. 2020, 73, e3606–e3614. [Google Scholar] [CrossRef]
- Timsit, J.-F.; Bassetti, M.; Cremer, O.; Daikos, G.; de Waele, J.; Kallil, A.; Kipnis, E.; Kollef, M.; Laupland, K.; Paiva, J.-A.; et al. Rationalizing Antimicrobial Therapy in the ICU: A Narrative Review. Intensive Care Med. 2019, 45, 172–189. [Google Scholar] [CrossRef]
- Steensels, D.; Reynders, M.; Descheemaeker, P.; Curran, M.D.; Jacobs, F.; Denis, O.; Delforge, M.-L.; Montesinos, I. Clinical Evaluation of a Multi-Parameter Customized Respiratory TaqMan(®) Array Card Compared to Conventional Methods in Immunocompromised Patients. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2015, 72, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data from 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Moreno, R.P.; Metnitz, P.G.H.; Almeida, E.; Jordan, B.; Bauer, P.; Campos, R.A.; Iapichino, G.; Edbrooke, D.; Capuzzo, M.; Le Gall, J.-R. SAPS 3—From Evaluation of the Patient to Evaluation of the Intensive Care Unit. Part 2: Development of a Prognostic Model for Hospital Mortality at ICU Admission. Intensive Care Med. 2005, 31, 1345–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.L. Serial Evaluation of the SOFA Score to Predict Outcome in Critically Ill Patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [Green Version]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of Influenza-Associated Pulmonary Aspergillosis in ICU Patients and Proposal for a Case Definition: An Expert Opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef]
- R Core Team. R A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, References-Scientific Research Publishing; 2019; Available online: https://www.scirp.org/%28S%28i43dyn45teexjx455qlt3d2q%29%29/reference/referencespapers.aspx?referenceid=2631126 (accessed on 19 August 2021).
- Therapeutics and COVID-19: Living Guideline. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-therapeutics-2021.3 (accessed on 9 January 2022).


{kind=link}
| COVID-19 | Influenza | p-Value | |
|---|---|---|---|
| N = 57 | N = 55 | ||
| Sex—male | 41 (72) | 30 (54) | 0.056 |
| Age (years) | 61 (53–70) | 65 (54–77) | 0.108 |
| Comorbidities | |||
| Current smokers, n (%) | 6 (10) | 23 (42) | <0.001 |
| Obesity | n = 54; 19 (35) | n = 46; 14 (29) | 0.534 |
| BMI (kg/m²) | n = 54; 28 (24–31) | n = 46; 28 (24–33) | 0.841 |
| Arterial hypertension, n (%) | 37 (65) | 34 (62) | 0.734 |
| Chronic cardiomyopathy, n (%) | 9 (16) | 23 (42) | 0.002 |
| Chronic pulmonary disease, n (%) | 17 (30) | 27 (49) | 0.037 |
| Chronic kidney failure, n (%) | 4 (7) | 13 (24) | 0.014 |
| Diabetes, n (%) | 11 (19) | 16 (29) | 0.226 |
| Active neoplasia, n (%) | 3 (5) | 3 (5) | 0.999 |
| Charlson Comorbidity Index, n (%) | 3 (1–5) | 4 (3–6) | 0.077 |
| Immunosuppressive therapy, n (%) | 6 (10) | 24 (44) | <0.001 |
| Chronic steroids, n (%) | 4 (7) | 16 (29) | 0.002 |
| Solid organ transplant, n (%) | 3 (5) | 6 (11) | 0.317 |
| (a) | |||
| COVID-19 | Influenza | p-Value | |
| N = 57 | N = 55 | ||
| Reason for ICU admission | |||
| Respiratory failure, n (%) | 51 (89) | 47 (86) | 0.52 |
| Medical reason, n (%) | 6 (11) | 7 (13) | 0.716 |
| Surgical reason, n (%) | 0 (0) | 1 (2) | 0.477 |
| Hospital to ICU admission, days | 1 (0–4) | 2 (0–11) | 0.012 |
| Baseline SOFA | 7 (3–9) | 6 (3–10) | 0.943 |
| Baseline SAPS 3 | 55 (46–68) | 62 (52–71) | 0.07 |
| Baseline PaO₂/FiO₂ ratio | 140 (100–194) | 152 (112–213) | 0.432 |
| CT features | n = 48 | n = 27 | |
| Ground glass, n (%) | 46 (96) | 15 (56) | <0.001 |
| Condensations, n (%) | 28 (58) | 19 (73) | 0.209 |
| Biological data | |||
| Leukocytes, 10³/mm3 | 8.69 (6.52–11.09) | 11.03 (8.42–15.00) | 0.035 |
| Lymphocytes count, 10³/mm3 | 0.89 (0.57–1.32) | 0.54 (0.34–1.04) | 0.028 |
| CRP, mg/L | 144 (94–230) | 63 (41–125) | <0.001 |
| Creatinine, mg/dL | 1.1 (0.8–1.6) | 1.2 (0.9–1.8) | 0.522 |
| LDH, IU/L | 506 (360–620) | 303 (239–431) | <0.001 |
| Antibiotherapy before ICU admission, n (%) | 18 (32) | 30 (54) | 0.04 |
| Antibiotherapy during the first 48 h, n (%) | 22 (39) | 44 (80) | <0.001 |
| (b) | |||
| COVID-19 | Influenza | p-Value | |
| N = 57 | N = 55 | ||
| Bacteriological samples within 48 h of admission | |||
| Total respiratory samples, n (%) | 34 (60) | 46 (84) | 0.005 |
| Sputum or ETA, n (%) | 29 (51) | 36 (67) | 0.091 |
| BAL, n (%) | 25 (44) | 12 (22) | 0.016 |
| Multiplex respiratory PCR panel, n (%) | 23 (40) | 21 (39) | 0.875 |
| Influenza test (PCR or Ag), n (%) | 42 (74) | 55 (100) | <0.001 |
| Blood cultures, n (%) | 54 (95) | 36 (66) | <0.001 |
| Urine cultures, n (%) | 54 (95) | 20 (38) | <0.001 |
| Bacteriological data | |||
| Total co-infections, n (%) | 13 (23) | 40 (73) | <0.001 |
| Respiratory co-infections, n (%) * | 9 (16) | 35 (64) | <0.001 |
| Bacteremia, n (%) * | 2 (3) | 7 (13) | 0.091 |
| Urinary tract infection, n (%) * | 2 (3) | 1 (2) | 0.317 |
| Pathogens of documented co-infections ** | |||
| Gram-positive coccus, n (%) | 7 (54) | 18 (45) | 0.579 |
| Staphylococcus aureus, n (%) | 1 (14) | 9 (50) | |
| Streptococcus pneumoniae, n (%) | 3 (43) | 5 (28) | |
| Other Streptococcus spp., n (%) | 3 (43) | 3 (17) | |
| Other, n (%) | 0 (0) | 1 (5) | |
| Gram-negative bacillus, n (%) | 9 (69) | 16 (40) | 0.607 |
| Escherichia coli, n (%) | 3 (33) | 1 (6) | |
| Klebsiella spp., n (%) | 1 (11) | 4 (25) | |
| Pseudomonas aeruginosa, n (%) | 0 (0) | 1 (6) | |
| Haemophilus influenzae, n (%) | 3 (33) | 5 (31) | |
| Other, n (%) | 2 (22) | 5 (31) | |
| Virus, n (%) | 2 (14) | 14 (35) | 0.181 |
| Adenovirus, n (%) | 2 (100) | 0 (0) | |
| Cytomegalovirus, n (%) | 0 (0) | 4 (29) | |
| Coronavirus (other than COVID-19), n (%) | 0 (0) | 4 (29) | |
| Other, n (%) | 0 (0) | 8 (57) | |
| Aspergillus sp., n (%) | 0 (0) | 8 (20) | 0.002 |
| COVID-19 | Influenza | |||
|---|---|---|---|---|
| n = 57 | n = 55 | |||
| OR (CI95%) | p-Value | OR (CI95%) | p-Value | |
| Sex | 0.53 (0.14–2.07) | 0.347 | 1.07 (0.32–3.54) | 0.912 |
| Age (years) | 0.99 (0.94–1.04) | 0.597 | 0.94 (0.89–0.99) | 0.026 |
| Current smokers | 1.82 (0.23–10.68) | 0.521 | 2.49 (0.72–10.2) | 0.17 |
| Chronic pulmonary disease | 1.06 (0.25–3.92) | 0.932 | 0.79 (0.24–2.61) | 0.7 |
| Obesity (BMI ≥ 30 kg/m2) | 1.21 (0.32–4.29) | 0.772 | 0.45 (0.12–1.65) | 0.219 |
| Arterial hypertension | 0.54 (0.15–1.97) | 0.345 | 0.31 (0.06–1.14) | 0.099 |
| Diabetes | * | 0.053 | 0.33 (0.09–1.17) | 0.085 |
| Charlson Comorbidity index | 1.01 (0.79–1.26) | 0.964 | 0.66 (0.44–0.92) | 0.022 |
| Immunosuppressive therapy | 6.07 (1.15–35.73) | 0.033 | 6.74 (1.15–128.77) | 0.08 |
| Solid organ transplant | 1.75 (0.08–19.85) | 0.659 | 2.00 (0.29–40.14) | 0.543 |
| Baseline SOFA | 1.16 (1–1.38) | 0.066 | 1.01 (0.88–1.18) | 0.866 |
| Baseline SAPS 3 | 1 (0.97–1.04) | 0.878 | 1.00 (0.96–1.04) | 0.856 |
| Baseline PaO₂/FiO₂ ratio | 1 (0.99–1.01) | 0.749 | 1.00 (0.99–1) | 0.153 |
| Influenza | 9.03 (3.94–22.02) | <0.001 | ||
| COVID-19 | Influenza | p-Value | |
|---|---|---|---|
| N = 57 | N = 55 | ||
| Total number of infectious events | 60 | 29 | - |
| Secondary infections | |||
| Event 1, n (%) | 37 (65) | 16 (29) | <0.001 |
| Time to onset (day) | 8 (2–23) | 6.5 (0–17) | 0.484 |
| Bacteremia, n (%) * | 13 (35) | 4 (25) | 0.538 |
| Respiratory infections, n (%) * | 35 (95) | 13 (81) | 0.155 |
| Others, n (%) * | 3 (8) | 3 (19) | 0.351 |
| Types of pathogens ** | |||
| Gram-positive cocci, n (%) | 6 (16) | 2 (20) | >0.999 |
| Gram-negative bacilli, n (%) | 34 (92) | 9 (90) | >0.999 |
| Virus, n (%) | 0 (0) | 0 (0) | >0.999 |
| Aspergillus sp., n (%) | 1 (3) | 7 (44) | <0.001 |
| Event 2, n (%) | 18 (32) | 7(13) | 0.017 |
| Time to onset (day) | 18 (11–29) | 16 (8–21) | 0.048 |
| Bacteremia, n (%) * | 4 (22) | 2 (29) | >0.999 |
| Respiratory infections, n (%) * | 13 (72) | 5 (71) | >0.999 |
| Others, n (%) * | 2 (11) | 0 (0) | >0.999 |
| Types of pathogens ** | |||
| Gram-positive cocci, n (%) | 3 (18) | 0 (0) | >0.999 |
| Gram-negative bacilli, n (%) | 16 (94) | 4 (100) | >0.999 |
| Virus, n (%) | 1 (6) | 1 (14) | 0.49 |
| Aspergillus sp., n (%) | 0 (0) | 0 (0) | >0.999 |
| Other fungi, n (%) | 0 (0) | 2 (40) | 0.039 |
| Event 3, n (%) | 5 (9) | 6 (11) | 0.704 |
| Time to onset (day) | 23 (18–31) | 22 (15–69) | 0.583 |
| Bacteremia, n (%) * | 5 (100) | 1 (33) | 0.061 |
| Respiratory infections, n (%) * | 2 (40) | 5 (83) | 0.242 |
| Others, n (%) * | 0 (0) | 0 (0) | >0.999 |
| Types of pathogens ** | |||
| Gram-positive cocci, n (%) | 2 (50) | 1 (20) | 0.524 |
| Gram-negative bacilli, n (%) | 4 (100) | 5 (100) | >0.999 |
| Virus, n (%) | 1 (20) | 3 (50) | 0.546 |
| Aspergillus sp., n (%) | 0 (0) | 2 (33) | 0.456 |
| Other fungi, n (%) | 0 (0) | 2 (33) | 0.456 |
| COVID-19 n = 57 | Influenza n = 55 | |||
|---|---|---|---|---|
| OR (CI95%) | p-Value | OR (CI95%) | p-Value | |
| Sex | 2.42 (0.73–8.11) | 0.146 | 1.1 (0.34–3.65) | 0.871 |
| Age (years) | 0.98 (0.94–1.03) | 0.472 | 0.97 (0.93–1.01) | 0.139 |
| Current smokers | 1.09 (0.19–8.42) | 0.924 | 1.12 (0.34–3.63) | 0.852 |
| Chronic pulmonary disease | 0.99 (0.31–3.39) | 0.983 | 0.51 (0.15–1.66) | 0.274 |
| Obesity | 4.82 (1.33–23.19) | 0.026 | 0.82 (0.2–2.96) | 0.768 |
| Arterial hypertension | 1.39 (0.44–4.31) | 0.568 | 0.72 (0.22–2.41) | 0.587 |
| Diabetes | * | 0.548 | 0.46 (0.09–1.75) | 0.286 |
| Charlson Comorbidity Index | 0.87 (0.7–1.07) | 0.196 | 0.85 (0.61–1.17) | 0.32 |
| Immunosuppressive therapy | 1.41 (0.27–10.52) | 0.701 | 1.52 (0.39–5.46) | 0.529 |
| Solid organ transplant | * | 0.545 | 0.45 (0.02–3.14) | 0.487 |
| Baseline SOFA | 1.21 (1.04–1.45) | 0.018 | 1.01 (0.86–1.17) | 0.922 |
| Baseline SAPS 3 | 0.99 (0.96–1.02) | 0.482 | 1.03 (0.99–1.07) | 0.192 |
| Baseline PaO₂/FiO₂ ratio | 0.99 (0.98–0.99) | 0.004 | 1 (0.99–1) | 0.425 |
| Vasopressors | 19.43 (4.8–104.01) | <0.001 | 3.92 (0.91–27.31) | 0.098 |
| ECMO | * | 0.005 | 22.8 (3.38–457.75) | 0.006 |
| Co-infections | 0.54 (0.15–1.97) | 0.345 | 3.5 (0.81–24.45) | 0.131 |
| Influenza | 0.22 (0.1–0.48) | <0.001 | ||
| COVID-19 | Influenza | p-Value | |
|---|---|---|---|
| N = 57 | N = 55 | ||
| Supportive measures | |||
| Optiflow, n (%) | 8 (14) | 15 (27) | 0.083 |
| NIV/CPAP, n (%) | 32 (56) | 31 (56) | 0.981 |
| Invasive mechanical ventilation, n (%) | 41 (72) | 36 (65) | 0.591 |
| Prone positioning, n (%) | 35 (61) | 9 (16) | <0.001 |
| ECMO, n (%) | 13 (23) | 7 (13) | 0.164 |
| Vasopressors, n (%) | 41 (72) | 39 (71) | 0.905 |
| Renal replacement therapy, n (%) | 16 (28) | 9 (16) | 0.137 |
| ICU stay (days) | 15 (4–29) | 5 (2–10) | 0.001 |
| Mechanical ventilation duration (days) | 11 (0–22) | 4 (1–18) | 0.716 |
| ICU mortality (%), n (%) | 20 (35) | 23 (41) | 0.464 |
| COVID-19 n = 57 | Influenza n = 55 | |||
|---|---|---|---|---|
| OR (CI95%) | p-Value | OR (CI95%) | p-Value | |
| Sex | 1.92 (0.556–7.81) | 0.323 | 1.56 (0.529–0.72) | 0.426 |
| Age (years) | 1.001 (0.764–1.05) | 0.745 | 101 (0.975–1.05) | 0.563 |
| Current smokers | 0.917 (0.119–5.18) | 0.924 | 0.438 (0.136–1.32) | 0.15 |
| Chronic pulmonary disease | 0.29 (0.06–1.06) | 0.082 | 0.5 (0.164–1.47) | 0.213 |
| Obesity (BMI ≥ 30 kg/m2) | 5.44 (1.71–18.77) | 0.005 | 0.958 (0.273–32) | 0.945 |
| Arterial hypertension | 4.82 (1.33–23.19) | 0.026 | 0.496 (0.16–1.49) | 0.215 |
| Diabetes | 4.44 (1.15–19.48) | 0.035 | 0.051 (0.003–0.293) | 0.006 |
| Charlson Comorbidity Index | 1.37 (1.1–1.8) | 0.012 | 0.858 (0.648–1.17) | 0.264 |
| Immunosuppressive therapy | 2 (0.333–11.84) | 0.425 | 0.533 (0.171–1.58) | 0.264 |
| Solid organ transplant | 0.012 * | 0.245 (0.012–1.67) | 0.215 | |
| Baseline SOFA | 1.22 (1.05–1.44) | 0.012 | 1.18 (1.035–1.38) | 0.019 |
| Baseline SAPS | 1.04 (1.001–1.09) | 0.038 | 1.06 (1.02–1.11) | 0.011 |
| Baseline PaO₂/FiO₂ ratio | 0.998 (0.991–1.004) | 0.463 | 0.988 (0.977–0.996) | 0.008 |
| Vasopressors | 12.95 (2.29–245.19) | 0.018 | 4.56 (1.24–22.22) | 0.034 |
| ECMO | 3.45 (0.936–13.62) | 0.065 | 2.04 (0.406–11.3) | 0.386 |
| Co-infections | 0.778 (0.187–2.87) | 0.711 | 4 (1.08–19.55) | 0.054 |
| Secondary infections | 3.05 (0.91–12.24) | 0.087 | 1.60 (0.49–5.26) | 0.432 |
| Number of surinfections | 1.415 (0.825–2.5) | 0.211 | 1.14 (0.685–1.9) | 0.606 |
| Drug multiresistance bacteria | * | >0.999 * | 0.463 (0.021–3.95) | 0.519 |
| Influenza | 1.32 (0.62–2.87) | 0.465 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcoux, D.; Etienne, I.; Van Muylem, A.; Bogossian, E.G.; Yin, N.; Taccone, F.S.; Hites, M. A Retrospective, Monocentric Study Comparing Co and Secondary Infections in Critically Ill COVID-19 and Influenza Patients. Antibiotics 2022, 11, 704. https://doi.org/10.3390/antibiotics11060704
Marcoux D, Etienne I, Van Muylem A, Bogossian EG, Yin N, Taccone FS, Hites M. A Retrospective, Monocentric Study Comparing Co and Secondary Infections in Critically Ill COVID-19 and Influenza Patients. Antibiotics. 2022; 11(6):704. https://doi.org/10.3390/antibiotics11060704
Chicago/Turabian StyleMarcoux, Diane, Isabelle Etienne, Alain Van Muylem, Elisa Gouvea Bogossian, Nicolas Yin, Fabio Silvio Taccone, and Maya Hites. 2022. "A Retrospective, Monocentric Study Comparing Co and Secondary Infections in Critically Ill COVID-19 and Influenza Patients" Antibiotics 11, no. 6: 704. https://doi.org/10.3390/antibiotics11060704