
Postpartum Depression after Maternal Isolation during the COVID-19 Pandemic: The MUMI-19 Study (Mothers Undergoing Mental Impact of COVID-19 Pandemic)

Abstract
:1. Background
2. Material and Methods
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nishiura, H.; Jung, S.-M.; Linton, N.M.; Kinoshita, R.; Yang, Y.; Hayashi, K.; Kobayashi, T.; Yuan, B.; Akhmetzhanov, A.R. The Extent of Transmission of Novel Coronavirus in Wuhan, China, 2020. J. Clin. Med. 2020, 9, 330. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. China Coronavirus: WHO Declares International Emergency as Death Toll Exceeds 200. BMJ 2020, 368, m408. [Google Scholar] [CrossRef]
- Yim, I.S.; Tanner Stapleton, L.R.; Guardino, C.M.; Hahn-Holbrook, J.; Dunkel Schetter, C. Biological and Psychosocial Predictors of Postpartum Depression: Systematic Review and Call for Integration. Annu. Rev. Clin. Psychol. 2015, 11, 99–137. [Google Scholar] [CrossRef]
- Banti, S.; Mauri, M.; Oppo, A.; Borri, C.; Rambelli, C.; Ramacciotti, D.; Montagnani, M.S.; Camilleri, V.; Cortopassi, S.; Rucci, P.; et al. From the Third Month of Pregnancy to 1 Year Postpartum. Prevalence, Incidence, Recurrence, and New Onset of Depression. Results from the Perinatal Depression-Research & Screening Unit Study. Compr. Psychiatry 2011, 52, 343–351. [Google Scholar] [CrossRef]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal Depression: A Systematic Review of Prevalence and Incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef]
- Lindahl, V.; Pearson, J.L.; Colpe, L. Prevalence of Suicidality during Pregnancy and the Postpartum. Arch. Womens Ment. Health 2005, 8, 77–87. [Google Scholar] [CrossRef]
- Abdollahi, F.; Lye, M.-S.; Md Zain, A.; Shariff Ghazali, S.; Zarghami, M. Postnatal Depression and Its Associated Factors in Women From Different Cultures. Iran. J. Psychiatry Behav. Sci. 2011, 5, 5–11. [Google Scholar] [PubMed]
- Parsons, C.E.; Young, K.S.; Rochat, T.J.; Kringelbach, M.L.; Stein, A. Postnatal Depression and Its Effects on Child Development: A Review of Evidence from Low- and Middle-Income Countries. Br. Med. Bull. 2012, 101, 57–79. [Google Scholar] [CrossRef]
- Evins, G.G.; Theofrastous, J.P.; Galvin, S.L. Postpartum Depression: A Comparison of Screening and Routine Clinical Evaluation. Am. J. Obstet. Gynecol. 2000, 182, 1080–1082. [Google Scholar] [CrossRef]
- Fergerson, S.S.; Jamieson, D.J.; Lindsay, M. Diagnosing Postpartum Depression: Can We Do Better? Am. J. Obstet. Gynecol. 2002, 186, 899–902. [Google Scholar] [CrossRef]
- Guedeney, A.; Bungener, C.; Widlöcher, D. Post-partum blues: A critical review of the literature. Psychiatr. Enfant 1993, 36, 329–354. [Google Scholar]
- Moraes, G.P.d.A.; Lorenzo, L.; Pontes, G.A.R.; Montenegro, M.C.; Cantilino, A. Screening and Diagnosing Postpartum Depression: When and How? Trends Psychiatry Psychother. 2017, 39, 54–61. [Google Scholar] [CrossRef]
- Guedeney, N.; Fermanian, J. Validation Study of the French Version of the Edinburgh Postnatal Depression Scale (EPDS): New Results about Use and Psychometric Properties. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 1998, 13, 83–89. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry J. Ment. Sci. 1987, 150, 782–786. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet Lond. Engl. 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Chmielewska, B.; Barratt, I.; Townsend, R.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Effects of the COVID-19 Pandemic on Maternal and Perinatal Outcomes: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2021, 9, e759–e772. [Google Scholar] [CrossRef]
- Liang, P.; Wang, Y.; Shi, S.; Liu, Y.; Xiong, R. Prevalence and Factors Associated with Postpartum Depression during the COVID-19 Pandemic among Women in Guangzhou, China: A Cross-Sectional Study. BMC Psychiatry 2020, 20, 557. [Google Scholar] [CrossRef]
- Yan, H.; Ding, Y.; Guo, W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychol. 2020, 11, 617001. [Google Scholar] [CrossRef]
- Oskovi-Kaplan, Z.A.; Buyuk, G.N.; Ozgu-Erdinc, A.S.; Keskin, H.L.; Ozbas, A.; Moraloglu Tekin, O. The Effect of COVID-19 Pandemic and Social Restrictions on Depression Rates and Maternal Attachment in Immediate Postpartum Women: A Preliminary Study. Psychiatr. Q. 2020, 92, 675–682. [Google Scholar] [CrossRef]
- COVID-19: Une Enquête pour Suivre L’évolution des Comportements et de la Santé Mentale Pendant L’épidémie. Available online: https://www.santepubliquefrance.fr/etudes-et-enquetes/coviprev-une-enquete-pour-suivre-l-evolution-des-comporte-ments-et-de-la-sante-mentale-pendant-l-epidemie-de-covid-19/coviprev-resultats-detailles-des-vagues-1-a-15-23-mars-23-septembre-2020 (accessed on 20 December 2020).
- Cameron, E.E.; Sedov, I.D.; Tomfohr-Madsen, L.M. Prevalence of Paternal Depression in Pregnancy and the Postpartum: An Updated Meta-Analysis. J. Affect. Disord. 2016, 206, 189–203. [Google Scholar] [CrossRef]
- Goodman, J.H. Paternal Postpartum Depression, Its Relationship to Maternal Postpartum Depression, and Implications for Family Health. J. Adv. Nurs. 2004, 45, 26–35. [Google Scholar] [CrossRef]
- Ballard, C.G.; Davis, R.; Cullen, P.C.; Mohan, R.N.; Dean, C. Prevalence of Postnatal Psychiatric Morbidity in Mothers and Fathers. Br. J. Psychiatry J. Ment. Sci. 1994, 164, 782–788. [Google Scholar] [CrossRef]
- Mangrio, E.; Persson, K.; Bramhagen, A.-C. Sociodemographic, Physical, Mental and Social Factors in the Cessation of Breastfeeding before 6 Months: A Systematic Review. Scand. J. Caring Sci. 2018, 32, 451–465. [Google Scholar] [CrossRef]
- Henderson, J.J.; Evans, S.F.; Straton, J.A.Y.; Priest, S.R.; Hagan, R. Impact of Postnatal Depression on Breastfeeding Duration. Birth 2003, 30, 175–180. [Google Scholar] [CrossRef]
- Peters, E.; Wehkamp, K.-H.; Felberbaum, R.E.; Krüger, D.; Linder, R. Breastfeeding Duration Is Determined by Only a Few Factors. Eur. J. Public Health 2006, 16, 162–167. [Google Scholar] [CrossRef]
- Bertholdt, C.; Epstein, J.; Banasiak, C.; Ligier, F.; Dahlhoff, S.; Olieric, M.F.; Mottet, N.; Beaumont, M.; Morel, O. Birth Experience during COVID-19 Confinement (CONFINE): Protocol for a Multicentre Prospective Study. BMJ Open 2020, 10, e043057. [Google Scholar] [CrossRef]



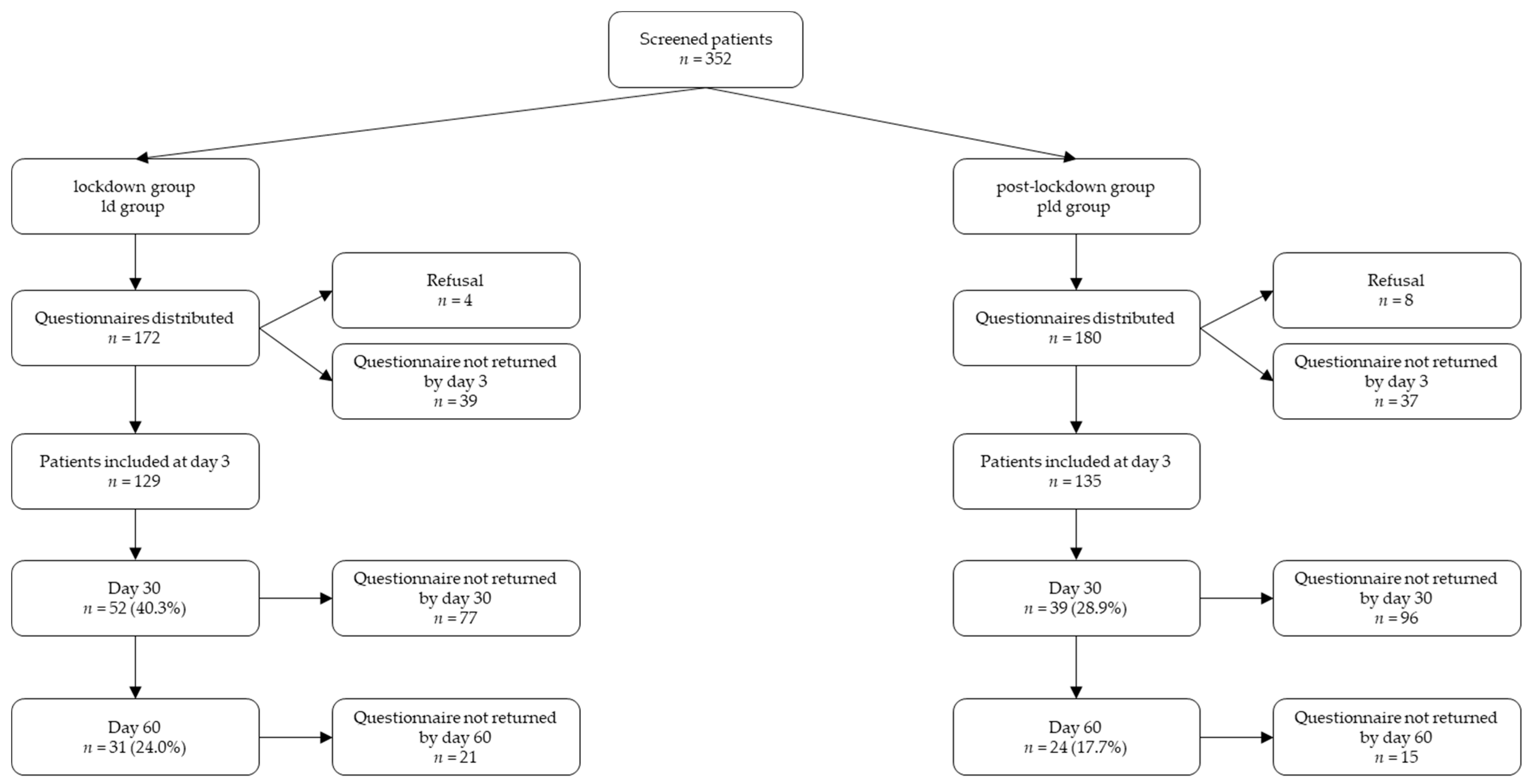{kind=link}
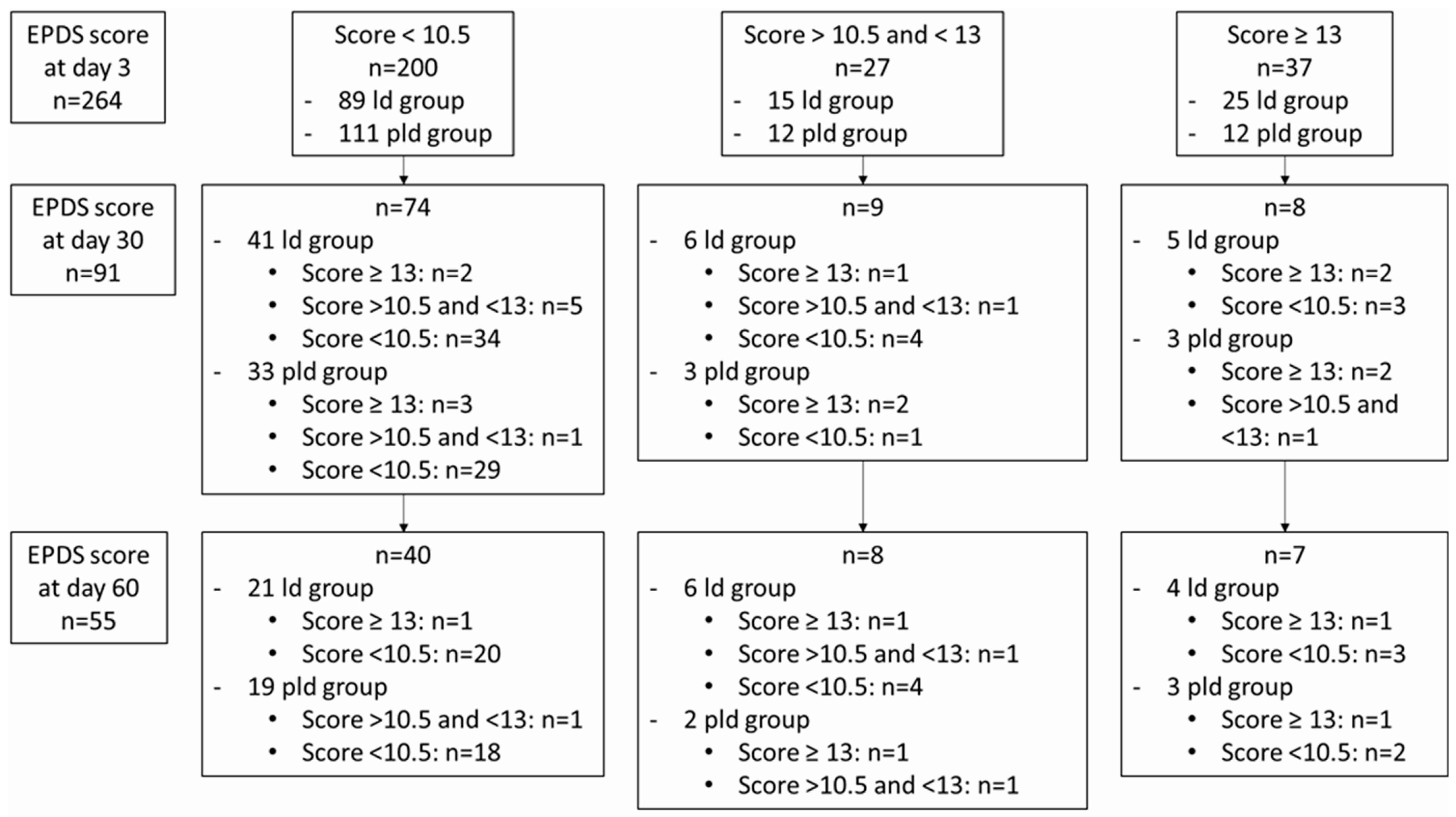{kind=link}
| Total | Lockdown Group (ld Group) | Post Lockdown Group (pld Group) | p | |
|---|---|---|---|---|
| (n = 264) | (n = 129) | (n = 135) | ||
| Age (years) | n = 255 | n = 126 | n = 129 | |
| Mean age ± SD | 30.9 (±5.5) | 30.8 (±5.5) | 30.9 (±5.5) | 0.953 |
| ≤24 | 38 (14.9%) | 18 (14.3%) | 20 (15.5%) | |
| 25–29 | 61 (23.9%) | 32 (25.4%) | 29 (22.5%) | |
| 30–34 | 85 (33.3%) | 41 (32.5%) | 44 (34.1%) | |
| >34 | 71 (27.8%) | 35 (27.8%) | 36 (27.9%) | |
| Parity | n = 254 | n = 126 | n = 128 | |
| Nulliparity | 125 (49.2%) | 67 (53.2%) | 58 (45.3%) | 0.259 |
| Parity ≥ 1 | 129 (50.8%) | 59 (46.8%) | 70 (54.7%) | |
| History of violence during childhood | n = 258 | n = 126 | n = 132 | 0.240 |
| Psychological | 15 (5.8%) | 11 (8.7%) | 4 (3.0%) | |
| Physical | 8 (3.1%) | 3 (2.4%) | 5 (3.8%) | |
| Physical and psychological | 8 (3.1%) | 4 (3.2%) | 4 (3.0%) | |
| History of medical affection impacting pregnancy | 49/254 (19.3%) | 22/126 (17.5%) | 27/128 (21.1%) | 0.565 |
| Presence of psychiatric history | 17/257 (6.6%) | 7/125 (5.6%) | 10/132 (7.6%) | 0.700 |
| Presence of familial psychiatric history | 27/258 (10.5%) | 14/126 (11.1%) | 13/132 (9.8%) | 0.898 |
| Presence of a difficult obstetrical history | 29/254 (11.4%) | 8/126 (6.3%) | 21/128 (16.4%) | 0.020 |
| Precarious situation | 13/258 (5.0%) | 9/126 (7.1%) | 4/132 (3.0%) | 0.221 |
| Homeless patient | 9/258 (3.5%) | 5/126 (4.0%) | 4/133 (3.0%) | 0.744 |
| Presence of marital difficulties | 10/257 (3.9%) | 6/126 (4.8%) | 4/131 (3.1%) | 0.534 |
| Insufficient patient social support | 5/255 (2.0%) | 4/122 (3.3%) | 1/133 (0.8%) | 0.196 |
| Existence of a migratory pathway for the patient | 27/250 (10.8%) | 17/122 (13.9%) | 10/128 (7.8%) | 0.175 |
| Toxic use | 30/259 (11.6%) | 16/126 (12.7%) | 14/133 (10.5%) | 0.725 |
| Current unwanted pregnancy | 22/260 (8.5%) | 16/127 (12.6%) | 6/133 (4.5%) | 0.034 |
| Pregnancy difficult to obtain | 37/230 (16.1%) | 18/107 (16.8%) | 19/133 (15.4%) | 0.918 |
| Pregnancy difficult to achieve | 89/251 (35.5%) | 44/123 (35.8%) | 45/128 (35.2%) | 0.999 |
| Presence of per-partum stress | 107/250 (42.8%) | 50/120 (41.7%) | 57/130 (43.8%) | 0.826 |
| Type of delivery | n = 252 | n = 126 | n = 128 | 0.970 |
| Spontaneous vaginal delivery | 164 (64.6%) | 82 (65.1%) | 82 (64.1%) | |
| Vacuum extraction | 22 (8.7%) | 8 (6.3%) | 14 (10.9%) | |
| Forceps | 4 (1.6%) | 2 (1.6%) | 2 (1.6%) | |
| Spatulas | 10 (3.9%) | 6 (4.8%) | 4 (3.1%) | |
| C-section | 52 (20.5%) | 26 (20.6%) | 26 (20.3%) | |
| Complications after delivery | n = 259 | n = 129 | n = 130 | 0.438 |
| Preterm birth | 8 (3.1%) | 3 (2.3%) | 5 (3.8%) | |
| Obstetrical anal sphincter injury (stage 3 or 4) | 1 (0.4%) | 0 | 1 (0.8%) | |
| Severe delivery hemorrhage > 1000 mL | 7 (2.7%) | 2 (1.6%) | 5 (3.8%) | |
| Uterine rupture | 1 (0.4%) | 1 (0.8%) | 0 | |
| Traumatic experience of childbirth | 32/254 (12.6%) | 19/123 (15.4%) | 13/131 (9.9%) | 0.256 |
| Absence of partner at delivery | n = 256 | n = 125 | n = 132 | 0.004 |
| Unwanted absence | 27 (10.5%) | 18 (14.5%) | 9 (6.8%) | |
| Desired absence | 9 (3.5%) | 8 (6.5%) | 1 (0.8%) | |
| Mother/child separation at birth | 20/255 (7.8%) | 10/125 (8.1%) | 10/132 (7.6%) | 0.999 |
| Length of stay in the maternity | n = 192 | n = 90 | n = 102 | 0.993 |
| Mean length (d ± SD) | 3.8 (±1.5) | 3.7 (±1.1) | 3.9 (±1.8) | |
| >3 days | 97 (50.5%) | 46/90 (51.1%) | 51/102 (50.0%) |
| Lockdown Group (ld Group) | Post Lockdown Group (pld Group) | p | |
|---|---|---|---|
| EPDS at day 3 | n = 129 | n = 135 | 0.015 |
| EPDS < 10.5 | 89 (69.0%) | 111 (82.2%) | |
| EPDS > 10.5 | 40 (31.0%) | 24 (17.8%) | |
| EPDS ≥ 13 | 25 (19.4%) | 12 (8.9%) | |
| EPDS at day 30 | n = 52 | n = 39 | 0.999 |
| EPDS < 10.5 | 41 (78.8%) | 30 (76.9%) | |
| EPDS > 10.5 | 11 (21.2%) | 9 (33.1%) | |
| EPDS ≥ 13 | 5 (9.6%) | 7 (17.9%) | |
| EPDS at day 60 | n = 31 | n = 24 | 0.718 |
| EPDS < 10.5 | 27 (87.1%) | 20 (83.3%) | |
| EPDS > 10.5 | 4 (12.9%) | 4 (16.7%) | |
| EPDS ≥ 13 | 3 (9.7%) | 2 (8.3%) | |
| Combined variable EPDS at day 30 and/or day 60 | n = 56 | n = 41 | 0.661 |
| EPDS < 10.5 | 43 (76.9%) | 29 (70.7%) | |
| EPDS > 10.5 | 13 (23.1%) | 12 (29.3%) |
| Total | Lockdown Group (ld group) | Post Lockdown Group (pld group) | p | |
|---|---|---|---|---|
| (n = 264) | (n = 129) | (n = 135) | ||
| Feelings of inability to care for the child | 35/250 (14.0%) | 29/121 (24.0%) | 6/129 (4.7%) | <0.001 |
| Experiences of early motherhood | n = 253 | n = 124 | n = 129 | <0.001 |
| Ruined | 71 (28.1%) | 69 (55.6%) | 2 (1.6%) | |
| Neither wasted nor ideal | 112 (44.3%) | 55 (44.4%) | 57 (44.2%) | |
| Ideal | 70 (27.7%) | 0 | 70 (54.3%) | |
| Apprehension of a gap with the partner at home | 28/246 (11.4%) | 21/119 (17.6%) | 7/127 (5.5%) | 0.050 |
| Suffering expressed by the partner | 69/240 (28.7%) | 56/116 (48.3%) | 13/124 (10.5%) | <0.001 |
| Breastfeeding | n = 250 | n = 122 | n = 128 | 0.638 |
| Easy breastfeeding | 142 (56.8%) | 73 (59.8%) | 69 (53.9%) | |
| Difficult breastfeeding | 62 (24.8%) | 28(23.0%) | 34 (26.6%) | |
| Artificial feeding | 46 (18.4%) | 21 (17.2%) | 25 (19.5%) | |
| Consultation with psychologist desired | 26/253 (10.3%) | 16/123 (13.0%) | 10/130 (7.7%) | 0.236 |
| Done | 19/26 (73%) | 12/16 (75.0%) | 7/10 (70.0%) | 0.273 |
| Early release | 78/246 (31.7%) | 52/119 (43.7%) | 26/127 (20.5%) | <0.001 |
| Odds Ratio [95% CI] | p | |
|---|---|---|
| Confined group membership | 0.7 [0.3–1.8] | 0.501 |
| Age | ||
| <24 | 0.5 [0.0–6.1] | 0.621 |
| 25–29 | ref | |
| 30–34 | 0.5 [0.2–1.6] | 0.240 |
| >34 | 0.4 [0.1–1.3] | 0.119 |
| Parity ≥ 1 | 0.2 [0.1–0.6] | 0.003 |
| History of violence during childhood | ||
| psychological | 6.4 [1.1–37.6] | 0.040 |
| physical | 1.6 [0.1–18.6] | 0.707 |
| History of medical affection impacting pregnancy | 1.2 [0.3–4.3] | 0.778 |
| Presence of psychiatric history | 2.3 [0.5–11.0] | 0.303 |
| Presence of familial psychiatric history | 0.4 [0.1–1.9] | 0.236 |
| Presence of a difficult obstetrical history | 1.5 [0.3–8.8] | 0.652 |
| Precarious situation | 6.1 [0.5–70.3] | 0.148 |
| Homeless patient | NA | NA |
| Presence of marital difficulties | NA | NA |
| Existence of a migratory pathway for the patient | 0.5 [0.1–3.9] | 0.472 |
| Toxic use | 0.8 [0.2–3.3] | 0.794 |
| Current unwanted pregnancy | 0.5 [0.1–3.9] | 0.472 |
| Pregnancy difficult to achieve | 1.4 [0.4–5.2] | 0.613 |
| Current pregnancy at risk | 1.0 [0.4–2.8] | 0.995 |
| Presence of per-partum stress | 4.5 [1.6–12.6] | 0.004 |
| Type of delivery | ||
| Caesarean section | 0.6 [0.2–2.0] | 0.406 |
| Instrumental delivery | 1.1 [0.3–3.7] | 0.863 |
| Complications after delivery | ||
| Preterm birth | 3.0 [0.2–50.0] | 0.444 |
| Severe delivery hemorrhage > 1000 mL | 1.5 [0.1–17.4] | 0.746 |
| Traumatic experience of childbirth | 5.1 [1.4–17.8] | 0.012 |
| Unwanted absence of partner at the delivery | 0.5 [0.1–4.0] | 0.479 |
| Mother/child separation at birth | 0.9 [0.1–9.5] | 0.961 |
| Length of stay in the maternity ≥ 3 days | 0.9 [0.3–2.3] | 0.808 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boudiaf, L.; Dupont, F.; Gras-Le Guen, C.; Sauvaget, A.; Leroy, M.; Thubert, T.; Winer, N.; Dochez, V. Postpartum Depression after Maternal Isolation during the COVID-19 Pandemic: The MUMI-19 Study (Mothers Undergoing Mental Impact of COVID-19 Pandemic). J. Clin. Med. 2022, 11, 5504. https://doi.org/10.3390/jcm11195504
Boudiaf L, Dupont F, Gras-Le Guen C, Sauvaget A, Leroy M, Thubert T, Winer N, Dochez V. Postpartum Depression after Maternal Isolation during the COVID-19 Pandemic: The MUMI-19 Study (Mothers Undergoing Mental Impact of COVID-19 Pandemic). Journal of Clinical Medicine. 2022; 11(19):5504. https://doi.org/10.3390/jcm11195504
Chicago/Turabian StyleBoudiaf, Lina, Françoise Dupont, Christèle Gras-Le Guen, Anne Sauvaget, Maxime Leroy, Thibault Thubert, Norbert Winer, and Vincent Dochez. 2022. "Postpartum Depression after Maternal Isolation during the COVID-19 Pandemic: The MUMI-19 Study (Mothers Undergoing Mental Impact of COVID-19 Pandemic)" Journal of Clinical Medicine 11, no. 19: 5504. https://doi.org/10.3390/jcm11195504