
Performance Evaluation of the STANDARDTM Q COVID-19 and PanbioTM COVID-19 Antigen Tests in Detecting SARS-CoV-2 during High Transmission Period in Mozambique

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Data Collection
2.3. Antigen Rapid Assay testing
2.4. Real Time PCR Testing
2.5. Statistical Methods
3. Results
3.1. Patient Population
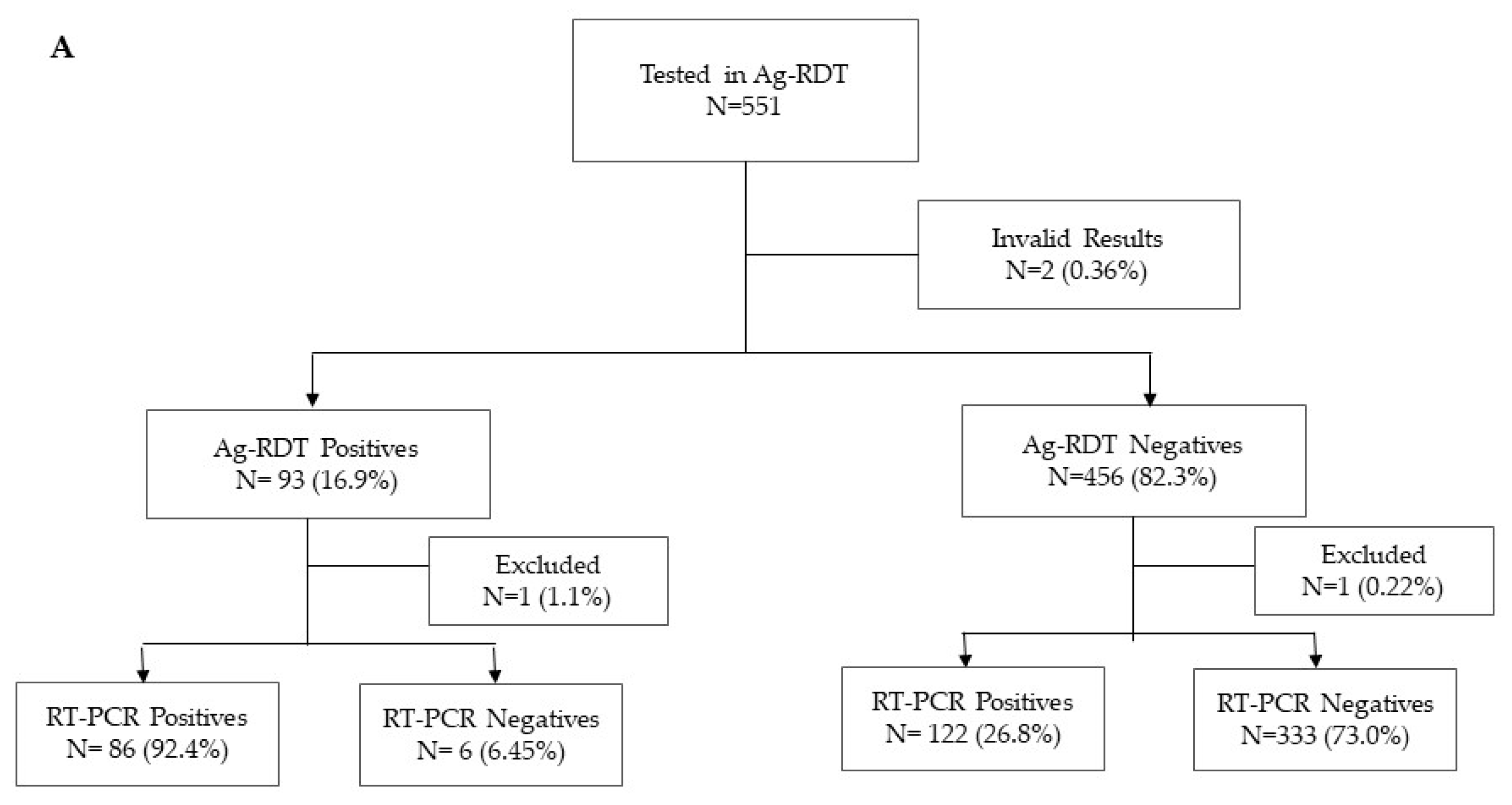
3.2. Diagnostic Performance of PanbioTM COVID-19 Ag Rapid Test
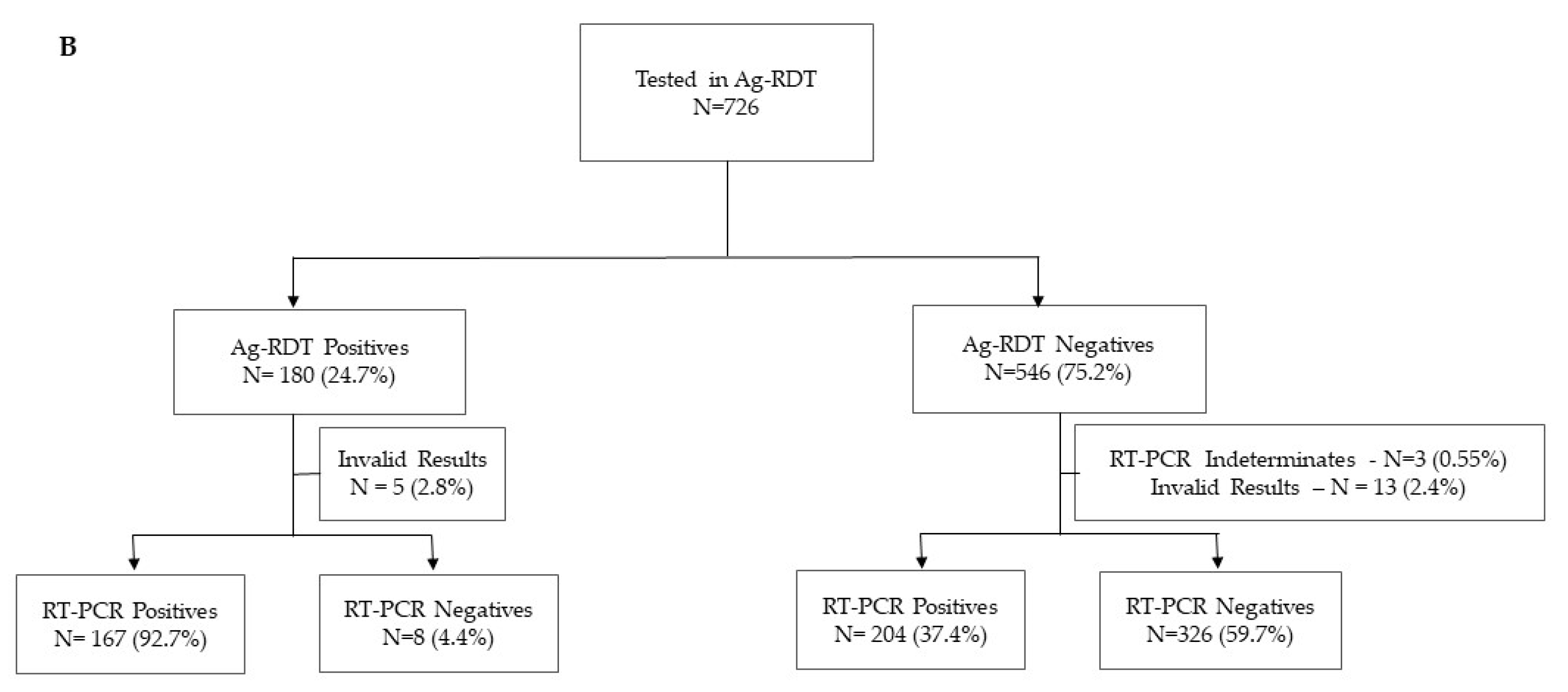
3.3. Diagnostic Performance of STANDARDTM Q COVID-19 Ag Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdullahi, I.N.; Emeribe, A.U.; Akande, A.O.; Ghamba, P.E.; Adekola, H.A.; Ibrahim, Y.; Dangana, A. Roles and Challenges of Coordinated Public Health Laboratory Response against COVID-19 Pandemic in Africa. J. Infect. Dev. Ctries. 2020, 14, 691–695. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Kiyaga, C.; Sendagire, H.; Joseph, E.; McConnell, I.; Grosz, J.; Narayan, V.; Esiru, G.; Elyanu, P.; Akol, Z.; Kirungi, W.; et al. Uganda’s New National Laboratory Sample Transport System: A Successful Model for Improving Access to Diagnostic Services for Early Infant HIV Diagnosis and Other Programs. PLoS ONE 2013, 8, e78609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favresse, J.; Gillot, C.; Oliveira, M.; Cadrobbi, J.; Elsen, M.; Eucher, C.; Laffineur, K.; Rosseels, C.; Van Eeckhoudt, S.; Nicolas, J.-B.; et al. Head-to-Head Comparison of Rapid and Automated Antigen Detection Tests for the Diagnosis of SARS-CoV-2 Infection. JCM 2021, 10, 265. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.K.; Loh, T.P.; Wang, C.-B.; Mueller, R.; Koch, D.; Sethi, S.; Rawlinson, W.D.; Clementi, M.; Erasmus, R.; Leportier, M.; et al. IFCC Interim Guidelines on Serological Testing of Antibodies against SARS-CoV-2. Clin. Chem. Lab. Med. (CCLM) 2020, 58, 2001–2008. [Google Scholar] [CrossRef]
- Iglὁi, Z.; Velzing, J.; Beek, J.; van Vijver, D.; van de Aron, G.; Ensing, R.; Benschop, K.; Han, W.; Boelsums, T.; Koopmans, M.; et al. Clinical Evaluation of the Roche/SD Biosensor Rapid Antigen Test with Symptomatic, Non-Hospitalized Patients in a Municipal Health Service Drive-through Testing Site. medRxiv 2020. [Google Scholar] [CrossRef]
- Bulilete, O.; Lorente, P.; Leiva, A.; Carandell, E.; Oliver, A.; Rojo, E.; Pericas, P.; Llobera, J. COVID-19 Primary Care Research Group PanbioTM Rapid Antigen Test for SARS-CoV-2 Has Acceptable Accuracy in Symptomatic Patients in Primary Health Care. J. Infect. 2021, 82, 391–398. [Google Scholar] [CrossRef]
- Haage, V.; Ferreira de Oliveira-Filho, E.; Moreira-Soto, A.; Kühne, A.; Fischer, C.; Sacks, J.A.; Corman, V.M.; Müller, M.A.; Drosten, C.; Drexler, J.F. Impaired Performance of SARS-CoV-2 Antigen-Detecting Rapid Diagnostic Tests at Elevated and Low Temperatures. J. Clin. Virol. 2021, 138, 104796. [Google Scholar] [CrossRef]
- Fenollar, F.; Bouam, A.; Ballouche, M.; Fuster, L.; Prudent, E.; Colson, P.; Tissot-Dupont, H.; Million, M.; Drancourt, M.; Raoult, D.; et al. Evaluation of the Panbio COVID-19 Rapid Antigen Detection Test Device for the Screening of Patients with COVID-19. J. Clin. Microbiol. 2020, 59, e02589-20. [Google Scholar] [CrossRef]
- Scohy, A.; Anantharajah, A.; Bodéus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low Performance of Rapid Antigen Detection Test as Frontline Testing for COVID-19 Diagnosis. J. Clin. Virol. 2020, 129, 104455. [Google Scholar] [CrossRef]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.W.; Imöhl, M.; Kleines, M. Comparison of the SARS-CoV-2 Rapid Antigen Test to the Real Star SARS-CoV-2 RT PCR Kit. J. Virol. Methods 2021, 288, 114024. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wen, K.; Zhang, J.; Chen, J.; Han, C.; Chen, Y.; Wang, S.; Deng, G.; Zhou, H.; Wu, Y. Accuracy of a Nucleocapsid Protein Antigen Rapid Test in the Diagnosis of SARS-CoV-2 Infection. Clin. Microbiol. Infect. 2021, 27, 289.e1–289.e4. [Google Scholar] [CrossRef] [PubMed]
- Stokes, W.; Berenger, B.M.; Portnoy, D.; Scott, B.; Szelewicki, J.; Singh, T.; Venner, A.A.; Turnbull, L.; Pabbaraju, K.; Shokoples, S.; et al. Clinical Performance of the Abbott Panbio with Nasopharyngeal, Throat, and Saliva Swabs among Symptomatic Individuals with COVID-19. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1721–1726. [Google Scholar] [CrossRef]
- WHO. WHO COVID-19: Case Definitions. WHO 2019-NCoV Surveillance Case Definition 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2020.2 (accessed on 25 April 2021).
- WHO SARS-CoV-2 Antigen Rapid Diagnostic Test Training Package. Available online: https://extranet.who.int/hslp/content/sars-cov-2-antigen-rapid-diagnostic-test-training-package (accessed on 27 August 2021).
- U.S. Food and Drug Administration Guidance for Industry and FDA Staff—Statistical Guidance on Reporting Results from Studies Evaluating Diagnostic Tests; US Food and Drug Administration: Silver Spring, MD, USA, 2007. Available online: https://www.fda.gov/media/71147/download (accessed on 27 August 2021).
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Strömer, A.; Rose, R.; Schäfer, M.; Schön, F.; Vollersen, A.; Lorentz, T.; Fickenscher, H.; Krumbholz, A. Performance of a Point-of-Care Test for the Rapid Detection of SARS-CoV-2 Antigen. Microorganisms 2020, 9, 58. [Google Scholar] [CrossRef]
- Khalid, M.F.; Selvam, K.; Jeffry, A.J.N.; Salmi, M.F.; Najib, M.A.; Norhayati, M.N.; Aziah, I. Performance of Rapid Antigen Tests for COVID-19 Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Ristić, M.; Nikolić, N.; Čabarkapa, V.; Turkulov, V.; Petrović, V. Validation of the STANDARD Q COVID-19 Antigen Test in Vojvodina, Serbia. PLoS ONE 2021, 16, e0247606. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Mboma, O.; Rieke, E.; Ahmad-Nejad, P.; Wirth, S.; Aydin, M. Diagnostic Performance of SARS-CoV-2 Rapid Antigen Test in a Large, German Cohort. Children 2021, 8, 682. [Google Scholar] [CrossRef]
- Jegerlehner, S.; Suter-Riniker, F.; Jent, P.; Bittel, P.; Nagler, M. Diagnostic Accuracy of a SARS-CoV-2 Rapid Antigen Test in Real-Life Clinical Settings. Int. J. Infect. Dis. 2021, 109, 118–122. [Google Scholar] [CrossRef]
- Torres, I.; Poujois, S.; Albert, E.; Colomina, J.; Navarro, D. Evaluation of a Rapid Antigen Test (PanbioTM COVID-19 Ag Rapid Test Device) for SARS-CoV-2 Detection in Asymptomatic Close Contacts of COVID-19 Patients. Clin. Microbiol. Infect. 2021, 27, 636.e1–636.e4. [Google Scholar] [CrossRef] [PubMed]
- Bours, M.J.L. Bayes’ Rule in Diagnosis. J. Clin. Epidemiol. 2021, 131, 158–160. [Google Scholar] [CrossRef]
- FDA. Potential for False Positive Results with Antigen Tests for Rapid Detection of SARS-CoV-2—Letter to Clinical Laboratory Staff and Health Care Providers. 2020. Available online: https://www.fda.gov/medical-devices/letters-health-care-providers/potential-false-positive-results-antigen-tests-rapid-detection-sars-cov-2-letter-clinical-laboratory (accessed on 10 June 2021).
- Wikramaratna, P.S.; Paton, R.S.; Ghafari, M.; Lourenço, J. Estimating the False-Negative Test Probability of SARS-CoV-2 by RT-PCR. Eurosurveillance 2020, 25, 2000568. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Wedderburn, C.J.; Garcia, P.J.; Boeras, D.; Fongwen, N.; Nkengasong, J.; Sall, A.; Tanuri, A.; Heymann, D.L. Serology Testing in the COVID-19 Pandemic Response. Lancet Infect. Dis. 2020, 20, e245–e249. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Panbio COVID-19 Ag | Standard Q COVID-19 Ag | |||||
|---|---|---|---|---|---|---|---|
| N = 1277 | % Total | N = 551 | % Total | N = 726 | % Total | ||
| Ag-TDR | Negative | 1002 | 78.47 | 456 | 82.76 | 546 | 75.21 |
| Positive | 273 | 21.38 | 93 | 16.88 | 180 | 24.79 | |
| Invalid | 2 | 0.16 | 2 | 0.36 | 0 | 0 | |
| RT-PCR | Negative | 674 | 52.78 | 340 | 61.71 | 334 | 46.01 |
| Positive | 580 | 45.41 | 209 | 37.93 | 371 | 51.10 | |
| Excluded | 20 | 1.57 | 2 | 0.36 | 18 | 2.48 | |
| Indeterminate | 3 | 0.23 | 0 | 0 | 3 | 0.41 | |
| Health Facilities | CS de Marracuene | 298 | 23.33 | 19 | 3.45 | 279 | 38.43 |
| HG Mavalane | 179 | 14.01 | 111 | 20.15 | 68 | 9.37 | |
| HG Chamanculo | 372 | 29.13 | 237 | 43.01 | 135 | 18.6 | |
| HP Matola | 428 | 33.51 | 184 | 33.39 | 244 | 33.61 | |
| Age | Median in years | 38.0 | NA | 42 | NA | 38.0 | NA |
| Sex | Female | 694 | 54.35 | 303 | 54.99 | 391 | 53.86 |
| Male | 583 | 45.65 | 248 | 45.01 | 335 | 46.14 | |
| Symptoms | Yes | 1075 | 84.18 | 480 | 87.11 | 595 | 81.96 |
| No | 202 | 15.82 | 71 | 12.89 | 131 | 18.04 | |
| Onset symptoms | ≤7 days | 817 | 76.00 | 364 | 75.83 | 453 | 76.13 |
| >7 days | 252 | 23.44 | 116 | 24.17 | 136 | 22.86 | |
| No information | 6 | 0.56 | 0 | 0 | 6 | 1.01 | |
| Sensitivity | Specificity | Positive Pred. Value | Negative Pred. Value | Misclassification | Observed Agreement | Chance Agreement | Cohen’s Kappa | ||
|---|---|---|---|---|---|---|---|---|---|
| Panbio COVID-19 Ag | Overall | 41.3% (34.6–48.4%) | 98.2% (96.2–99.3%) | 93.3% (88.8–97.8%) | 52.9% (48.6–57.1%) | 23.4% (19.9–27.2%) | 76.6% (31.9–80.1%) | 56.7% | 0.45 (0.44–0.46) |
| With symptoms | 43.2% (36.0–50.5%) | 97.9% (95.5–99.2%) | 93.0% (88.4–97.7%) | 55.3% (50.8–59.8%) | 23.9% (20.2–28.0%) | 76.1% (32.0–79.8%) | 55.4% | 0.46 (0.45–0.47) | |
| Without symptoms | 22.2% (6.4–47.6%) | 100.0% (93.3–NA) | 100.0% (100.0–NA) | 30.4% (19.4–41.4%) | 19.7% (11.2–30.9%) | 80.3% (25.4–88.8%) | 71.9% | 0.29 (0.04–0.56) | |
| Onset symptoms ≤ 5 d 1 | 53.3% (42.6–63.7%) | 97.4% (93.5–99.3%) | 91.3% (84.7–98.0%) | 56.5% (50.2–62.8%) | 19.0% (14.3–24.5%) | 81.0% (32.4–85.7%) | 56.5% | 0.55 (0.53–0.57) | |
| Onset symptoms ≤ 7 d | 49.6% (41.1–58.2%) | 97.7% (94.8–99.3%) | 93.1% (88.1–98.0%) | 57.3% (52.2–62.4%) | 20.8% (16.7–25.3%) | 79.2% (32.6–83.3%) | 55.4% | 0.52 (0.51–0.53) | |
| Onset symptoms > 7 d | 25.5% (14.3–39.6%) | 98.4% (91.6–100.0%) | 92.9% (79.4–100.0%) | 50.4% (41.0–59.8%) | 33.9% (25.3–43.3%) | 66.1% (25.7–74.4%) | 54.7% | 0.25 (0.19–0.30) | |
| Standard Q COVID-19 Ag | Overall | 45.0% (39.9–50.2%) | 97.6% (95.3–99.0%) | 95.4% (92.3–98.5%) | 66.4% (62.3–70.4%) | 30.2% (26.7–33.6%) | 69.8% (33.8–73.3%) | 48.6% | 0.41 (0.41–0.42) |
| With symptoms | 49.4% (43.8–55.0%) | 97.6% (94.8–99.1%) | 96.4% (93.6–99.2%) | 71.5% (67.2–75.9%) | 29.8% (26.0–33.6%) | 70.2% (35.1–74.0%) | 47.2% | 0.44 (0.43–0.44) | |
| Without symptoms | 13.3% (5.1–26.8%) | 97.6% (91.7–99.7%) | 75.0% (45.0–100.0%) | 37.6% (29.0–46.3%) | 31.8% (23.9–40.6%) | 68.2% (24.8–76.1%) | 63.2% | 0.14 (0.05–0.22) | |
| Onset symptoms ≤ 5 d | 61.9% (53.9–69.4%) | 97.9% (94.1–99.6%) | 97.1% (93.8–100.0%) | 73.8% (67.8–79.9%) | 21.0% (16.6–26.0%) | 78.8% (36.9–83.4%) | 49.1% | 0.58 (0.57–0.59) | |
| Onset symptoms ≤ 7 d | 54.5% (47.9–61.0%) | 98.0% (95.1–99.5%) | 96.9% (94.0–99.9%) | 71.1% (66.0–76.2%) | 25.2% (21.2–29.5%) | 74.8% (35.7–78.8%) | 48.6% | 0.51 (0.49–0.52) | |
| Onset symptoms > 7 d | 35.2% (25.3–46.1%) | 95.6% (84.9–99.5%) | 93.9% (85.8–100.0%) | 74.3% (65.7–82.8%) | 44.4% (35.8–53.2%) | 55.6% (27.6–64.2%) | 41.9% | 0.24 (0.21–0.27) |
| ≤15 | ≤25 | ≥26 | ||
|---|---|---|---|---|
| Panbio COVID-19 Ag | Overall | 90.8% (59/65) | 52.7% (77/146) | 11.9% (7/59) |
| With symptoms | 90.3% (56/62) | 52.9% (73/138) | 14.3% (7/49) | |
| Without symptoms | 100% (3/3) | 50% (4/4) | 0% (0/10) | |
| Onset symptoms ≤ 5 d | 90.2% (37/41) | 64.6% (42/65) | 13.0% (3/23) | |
| Onset symptoms ≤ 7 d | 89.9% (49/51) | 61.5% (59/96) | 15.8% (6/38) | |
| Onset symptoms > 7 d | 100% (7/7) | 35.7% (10/38) | 0% (0/10) | |
| Standard Q COVID-19 Ag | Overall | 87.0% (109/124) | 55.4% (153/276) | 12.1% (14/116) |
| With symptoms | 89.2% (107/120) | 60.0% (147/245) | 13.9% (14/81) | |
| Without symptoms | 50.0% (2/2) | 0% (0/15) | 0% (0/15) | |
| Onset symptoms ≤ 5 d | 94.5% (70/74) | 80% (93/125) | 13.3% (6/45) | |
| Onset symptoms ≤ 7 d | 92.5% (87/94) | 66.3% (118/178) | 13.4% (9/67) | |
| Onset symptoms > 7 d | 64.7% (11/17) | 50% (26/52) | 12.1% (4/33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sitoe, N.; Sambo, J.; Nguenha, N.; Chilaule, J.; Chelene, I.; Loquiha, O.; Mudenyanga, C.; Viegas, S.; Cunningham, J.; Jani, I. Performance Evaluation of the STANDARDTM Q COVID-19 and PanbioTM COVID-19 Antigen Tests in Detecting SARS-CoV-2 during High Transmission Period in Mozambique. Diagnostics 2022, 12, 475. https://doi.org/10.3390/diagnostics12020475
Sitoe N, Sambo J, Nguenha N, Chilaule J, Chelene I, Loquiha O, Mudenyanga C, Viegas S, Cunningham J, Jani I. Performance Evaluation of the STANDARDTM Q COVID-19 and PanbioTM COVID-19 Antigen Tests in Detecting SARS-CoV-2 during High Transmission Period in Mozambique. Diagnostics. 2022; 12(2):475. https://doi.org/10.3390/diagnostics12020475
Chicago/Turabian StyleSitoe, Nádia, Júlia Sambo, Neuza Nguenha, Jorfelia Chilaule, Imelda Chelene, Osvaldo Loquiha, Chishamiso Mudenyanga, Sofia Viegas, Jane Cunningham, and Ilesh Jani. 2022. "Performance Evaluation of the STANDARDTM Q COVID-19 and PanbioTM COVID-19 Antigen Tests in Detecting SARS-CoV-2 during High Transmission Period in Mozambique" Diagnostics 12, no. 2: 475. https://doi.org/10.3390/diagnostics12020475