
Individual Stress Burden and Mental Health in Health Care Workers during the COVID-19 Pandemic: Moderating and Mediating Effects of Resilience

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Sample Characteristics
2.3. Measures
2.3.1. Mental Health
2.3.2. Subjective Stress Burden Levels
2.3.3. Resilience
2.3.4. Sociodemographic, Occupational, and COVID-19-Related Variables
2.4. Statistical Analysis
3. Results
3.1. Associations between Sociodemographic/Occupational Characteristics and Resilience
3.2. Relationship between Resilience, Subjective Stress Burden in the Pandemic and Mental Health
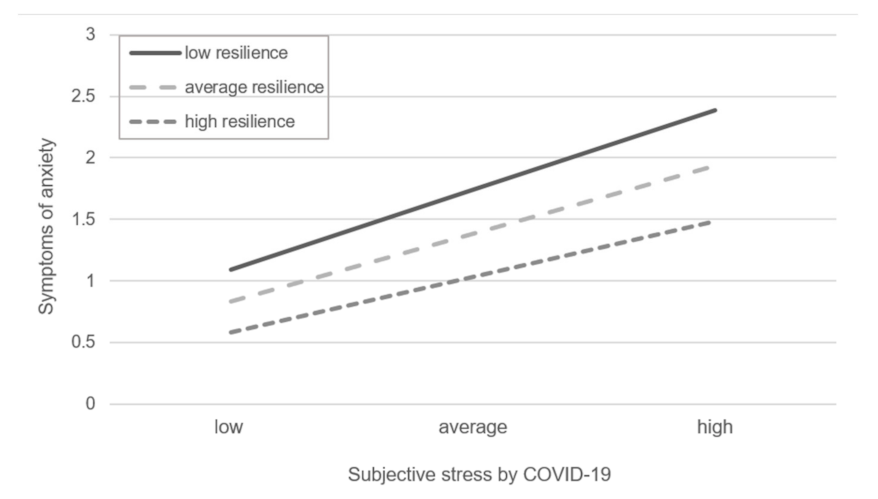
3.2.1. Moderating Effects of Resilience
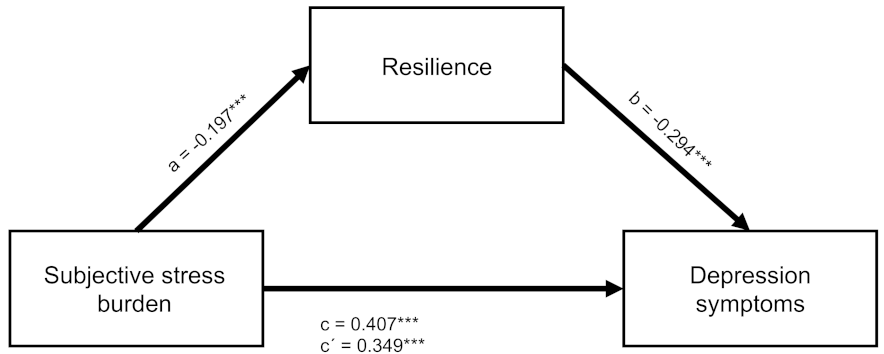
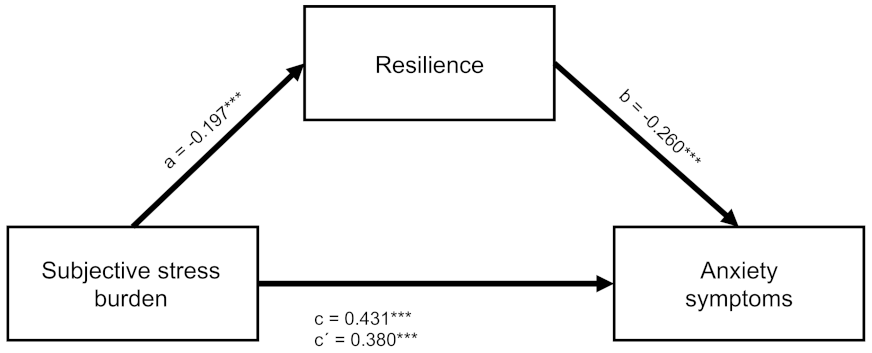
3.2.2. Mediating Effects of Resilience
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Gilan, D.; Röthke, N.; Blessin, M.; Kunzler, A.; Stoffers-Winterling, J.; Müssig, M.; Yuen, K.S.L.; Tüscher, O.; Thrul, J.; Kreuter, F.; et al. Psychomorbidity, resilience, and exacerbating and protective factors during the SARS-CoV-2-pandemic. Dtsch Arztebl Int. 2020, 117, 625–630. Available online: https://www.aerzteblatt.de/10.3238/arztebl.2020.0625 (accessed on 9 December 2020). [CrossRef] [PubMed]
- De Georgeo, M.R.; De Georgeo, J.M.; Egan, T.M.; Klee, K.P.; Schwemm, M.S.; Bye-Kollbaum, H.; Kinser, A.J. Containing SARS-CoV-2 in hospitals facing finite PPE, limited testing, and physical space variability: Navigating resource constrained enhanced traffic control bundling. J. Microbiol. Immunol. 2020, 54, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N. Mental health of health-care workers in the COVID-19 era. Nat. Rev. Nephrol. 2020, 16, 425–426. [Google Scholar] [CrossRef]
- Serrano-Ripoll, M.J.; Meneses-Echavez, J.F.; Ricci-Cabello, I.; Fraile-Navarro, D.; Fiol-deRoque, M.A.; Pastor-Moreno, G.; Castro, A.; Ruiz-Pérez, I.; Zamanillo Campos, R.; Gonçalves-Bradley, D.C. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 347–357. [Google Scholar] [CrossRef]
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Morawa, E.; Schug, C.; Geiser, F.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Hiebel, N.; Borho, A.; Erim, Y. Psychosocial burden and working conditions during the COVID-19 pandemic in Germany: The VOICE survey among 3678 health care workers in hospitals. J. Psychosom. Res. 2021, 144, 110415. [Google Scholar] [CrossRef]
- Boyraz, G.; Legros, D.N. Coronavirus Disease (COVID-19) and Traumatic Stress: Probable Risk Factors and Correlates of Post-traumatic Stress Disorder. J. Loss Trauma 2020, 25, 503–522. [Google Scholar] [CrossRef]
- Yuan, K.; Gong, Y.-M.; Liu, L.; Sun, Y.-K.; Tian, S.-S.; Wang, Y.-J.; Zhong, Y.; Zhang, A.-Y.; Su, S.-Z.; Liu, X.-X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: A meta-analysis and systematic review. Mol. Psychiatry 2021, 26, 4982–4998. [Google Scholar] [CrossRef]
- Bonanno, G.A. Loss, Trauma, and Human Resilience: Have We Underestimated the Human Capacity to Thrive After Ex-tremely Aversive Events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef]
- Hu, T.; Zhang, D.; Wang, J. A meta-analysis of the trait resilience and mental health. Pers. Individ. Differ. 2015, 76, 18–27. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar] [PubMed]
- Aburn, G.; Gott, M.; Hoare, K. What is resilience? An Integrative Review of the empirical literature. J. Adv. Nurs. 2016, 72, 980–1000. [Google Scholar] [CrossRef] [PubMed]
- Chmitorz, A.; Kunzler, A.; Helmreich, I.; Tüscher, O.; Kalisch, R.; Kubiak, T.; Wessa, M.; Lieb, K. Intervention studies to foster resilience—A systematic review and proposal for a resilience framework in future intervention studies. Clin. Psychol. Rev. 2018, 59, 78–100. [Google Scholar] [CrossRef] [PubMed]
- Hiebel, N.; Rabe, M.; Maus, K.; Peusquens, F.; Radbruch, L.; Geiser, F. Resilience in Adult Health Science Revisited—A Narrative Review Synthesis of Process-Oriented Approaches. Front. Psychol. 2021, 12, 659395. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Mealer, M.; Jones, J.; Newman, J.; McFann, K.K.; Rothbaum, B.; Moss, M. The presence of resilience is associated with a healthier psychological profile in intensive care unit (ICU) nurses: Results of a national survey. Int. J. Nurs. Stud. 2012, 49, 292–299. [Google Scholar] [CrossRef]
- Rushton, C.H.; Batcheller, J.; Schroeder, K.; Donohue, P. Burnout and Resilience among Nurses Practicing in High-Intensity Set-tings. Am. J. Crit. Care 2015, 24, 412–420. [Google Scholar] [CrossRef]
- E Cooke, G.P.; A Doust, J.; Steele, M.C. A survey of resilience, burnout, and tolerance of uncertainty in Australian general practice registrars. BMC Med. Educ. 2013, 13, 2. [Google Scholar] [CrossRef]
- Huang, L.; Wang, Y.; Liu, J.; Ye, P.; Chen, X.; Xu, H.; Qu, H.; Ning, G. Factors Influencing Anxiety of Health Care Workers in the Radiology Department with High Exposure Risk to COVID-19. Med. Sci. Monit. 2020, 26, e926008-1. [Google Scholar] [CrossRef]
- Huffman, E.M.; Athanasiadis, D.I.; Anton, N.E.; Haskett, L.A.; Doster, D.L.; Stefanidis, D.; Lee, N.K. How resilient is your team? Exploring healthcare providers’ well-being during the COVID-19 pandemic. Am. J. Surg. 2020, 221, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Ren, Y.-H.; Gan, H.-J.; Chen, Y.; Huang, Y.-F.; You, X.-M. Factors associated with resilience among non-local medical workers sent to Wuhan, China during the COVID-19 outbreak. BMC Psychiatry 2020, 20, 417. [Google Scholar] [CrossRef] [PubMed]
- Barzilay, R.; Moore, T.M.; Greenberg, D.M.; DiDomenico, G.E.; Brown, L.A.; White, L.K.; Gur, R.C.; Gur, R.E. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl. Psychiatry 2020, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Ang, S.Y.; Uthaman, T.; Ayre, T.C.; Mordiffi, S.Z.; Ang, E.; Lopez, V. Association between demographics and resilience—A cross-sectional study among nurses in Singapore. Int. Nurs. Rev. 2018, 65, 459–466. [Google Scholar] [CrossRef]
- Gillespie, B.M.; Chaboyer, W.; Wallis, M. The influence of personal characteristics on the resilience of operating room nurses: A predictor study. Int. J. Nurs. Stud. 2009, 46, 968–976. [Google Scholar] [CrossRef]
- Yu, F.; Raphael, D.; Mackay, L.; Smith, M.; King, A. Personal and work-related factors associated with nurse resilience: A system-atic review. Int. J. Nurs. Stud. 2019, 93, 129–140. [Google Scholar] [CrossRef]
- McKinley, N.; Karayiannis, P.N.; Convie, L.; Clarke, M.; Kirk, S.J.; Campbell, W.J. Resilience in medical doctors: A systematic review. Postgrad. Med. J. 2019, 95, 140–147. [Google Scholar] [CrossRef]
- Chang, S.; Picco, L.; Abdin, E.; Yuan, Q.; Chong, S.A.; Subramaniam, M. Resilience and associative stigma among mental health professionals in a tertiary psychiatric hospital: A cross-sectional study in Singapore. BMJ Open 2019, 9, e033762. [Google Scholar] [CrossRef]
- Sull, A.; Harland, N.J.; Moore, A. Resilience of health-care workers in the UK; a cross-sectional survey. J. Occup. Med. Toxicol. 2015, 10, 20. [Google Scholar] [CrossRef]
- Fergus, S.; Zimmerman, M.A. ADOLESCENT RESILIENCE: A Framework for Understanding Healthy Development in the Face of Risk. Annu. Rev. Public Health 2005, 26, 399–419. [Google Scholar] [CrossRef]
- Schultze-Lutter, F.; Schimmelmann, B.G.; Schmidt, S.J. Resilience, risk, mental health and well-being: Associations and conceptual differences. Eur. Child Adolesc. Psychiatry 2016, 25, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Zhang, J.; Li, M.; Li, P.; Zhang, Y.; Zuo, X.; Miao, Y.; Xu, Y. Negative life events and mental health of Chinese medical students: The effect of resilience, personality and social support. Psychiatry Res. 2012, 196, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Arrogante, O.; Aparicio-Zaldivar, E. Burnout and health among critical care professionals: The mediational role of resilience. Intensiv. Crit. Care Nurs. 2017, 42, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Havnen, A.; Anyan, F.; Hjemdal, O.; Solem, S.; Gurigard Riksfjord, M.; Hagen, K. Resilience Moderates Negative Outcome from Stress during the COVID-19 Pandemic: A Moderated-Mediation Approach. Int. J. Environ. Res. Public Health 2020, 17, 6461. [Google Scholar] [CrossRef]
- Anyan, F.; Hjemdal, O. Adolescent stress and symptoms of anxiety and depression: Resilience explains and differentiates the relationships. J. Affect. Disord. 2016, 203, 213–220. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef]
- von Eisenhart Rothe, A.; Zenger, M.; Lacruz, M.E.; Emeny, R.; Baumert, J.; Haefner, S.; Ladwig, K.-H. Validation and development of a short-er version of the resilience scale RS-11: Results from the population-based KORA–age study. BMC Psychol. 2013, 1, 25. [Google Scholar] [CrossRef]
- Schmalbach, B.; Zenger, M.; Strauß, B.; Hinz, A.; Steffens-Guerra, I.; Decker, O.; Brähler, E. Validation and Psychometric Properties of the Resilience Scale-5 (RS-5) Results of a Representative Survey of the German General Population. Health Sci. J. 2016, 10, 1. [Google Scholar]
- Delacre, M.; Lakens, D.D.; Leys, C. Why Psychologists Should by Default Use Welch’s t-test Instead of Student’s t-test. Int. Rev. Soc. Psychol. 2017, 30, 92. [Google Scholar] [CrossRef]
- Delacre, M.; Leys, C.; Mora, Y.L.; Lakens, D. Taking Parametric Assumptions Seriously: Arguments for the Use of Welch’s F-test instead of the Classical F-test in One-Way ANOVA. Int. Rev. Soc. Psychol. 2019, 32, 13. [Google Scholar] [CrossRef]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling; University of Kansas: Lawrence, KS, USA, 2012. [Google Scholar]
- Garmezy, N.; Masten, A.S.; Tellegen, A. The Study of Stress and Competence in Children: A Building Block for Developmental Psychopathology. Child Dev. 1984, 55, 97. [Google Scholar] [CrossRef] [PubMed]
- Kukihara, H.; Yamawaki, N.; Uchiyama, K.; Arai, S.; Horikawa, E. Trauma, depression, and resilience of earth-quake/tsunami/nuclear disaster survivors of Hirono, Fukushima, Japan: Resilience of Japan disaster survivors. Psychiatry Clin. Neurosci. 2014, 68, 524–533. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Sinsky, C.; Trockel, M.; Tutty, M.; Nedelec, L.; Carlasare, L.E.; Shanafelt, T.D. Resilience and burnout among physicians and the general US working population. JAMA Netw. Open 2020, 3, e209385. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Westphal, M.; Mancini, A.D. Resilience to Loss and Potential Trauma. Annu. Rev. Clin. Psychol. 2011, 7, 511–535. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahov, D. What predicts psychological resilience after disaster? The role of de-mographics, resources, and life stress. J. Consult. Clin. Psychol. 2007, 75, 671–682. [Google Scholar] [CrossRef]
- Portzky, M.; Wagnild, G.; De Bacquer, D.; Audenaert, K. Psychometric evaluation of the Dutch Resilience Scale RS-nl on 3265 healthy participants: A confirmation of the association between age and resilience found with the Swedish version: Psycho-metric evaluation of RS-nl on healthy participants. Scand. J. Caring Sci. 2010, 24, 86–92. [Google Scholar] [CrossRef]
- Rodriguez-Llanes, J.M.; Vos, F.; Guha-Sapir, D. Measuring psychological resilience to disasters: Are evidence-based indicators an achievable goal? Environ. Health 2013, 12, 115. [Google Scholar] [CrossRef]
- Zolkoski, S.M.; Bullock, L.M. Resilience in children and youth: A review. Child. Youth Serv. Rev. 2012, 34, 2295–2303. [Google Scholar] [CrossRef]
- Ong, A.D.; Bergeman, C.S.; Boker, S.M. Resilience Comes of Age: Defining Features in Later Adulthood. J. Pers. 2009, 77, 1777–1804. [Google Scholar] [CrossRef]
- Phillips, S.P.; Auais, M.; Belanger, E.; Alvarado, B.; Zunzunegui, M.-V. Life-course social and economic circumstances, gender, and resilience in older adults: The longitudinal International Mobility in Aging Study (IMIAS). SSM-Popul. Health 2016, 2, 708–717. [Google Scholar] [CrossRef]
- Matos, P.S.; Neushotz, L.A.; Griffin, M.T.Q.; Fitzpatrick, J.J. An exploratory study of resilience and job satisfaction among psychiat-ric nurses working in inpatient units. Int. J. Mental Health Nurs. 2010, 19, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Taku, K. Relationships among perceived psychological growth, resilience and burnout in physicians. Pers. Individ. Differ. 2014, 59, 120–123. [Google Scholar] [CrossRef]
- Brown, R.; Wey, H.; Foland, K. The Relationship among Change Fatigue, Resilience, and Job Satisfaction of Hospital Staff Nurses. J. Nurs. Sch. 2018, 50, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Hudgins, T.A. Resilience, job satisfaction and anticipated turnover in nurse leaders. J. Nurs. Manag. 2015, 24, E62–E69. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef]
- Kleim, B.; Kalisch, R. Wer bleibt gesund? Zum Problem der Vorhersage von Resilienz. Der Nervenarzt 2018, 89, 754–758. [Google Scholar] [CrossRef]
- Cole, N.N.; Nonterah, C.W.; Utsey, S.O.; Hook, J.N.; Hubbard, R.R.; Opare-Henaku, A.; Fischer, N.L. Predictor and Moderator Effects of Ego Resilience and Mindfulness on the Relationship Between Academic Stress and Psychological Well-Being in a Sample of Ghanaian College Students. J. Black Psychol. 2014, 41, 340–357. [Google Scholar] [CrossRef]
- Collazzoni, A.; Stratta, P.; Pacitti, F.; Rossi, A.; Santarelli, V.; Bustini, M.; Talevi, D.; Socci, V.; Rossi, R. Resilience as a Mediator between Interpersonal Risk Factors and Hopelessness in Depression. Front. Psychiatry 2020, 11, 10. [Google Scholar] [CrossRef]
- Ye, Z.; Yang, X.; Zeng, C.; Wang, Y.; Shen, Z.; Li, X.; Lin, D. Resilience, Social Support, and Coping as Mediators between COVID-19-related Stressful Experiences and Acute Stress Disorder among College Students in China. Appl. Psychol. Health Well Being. 2020, 12, 1074–1094. [Google Scholar] [CrossRef]
- Schmuck, J.; Hiebel, N.; Rabe, M.; Schneider, J.; Erim, Y.; Morawa, E.; Jerg-Bretzke, L.; Beschoner, P.; Albus, C.; Hannemann, J.; et al. Sense of coherence, social support and religiosity as re-sources for medical personnel during the COVID-19 pandemic: A web-based survey among 4324 health care workers within the German Network University Medicine. PLoS ONE 2021, 16, e0255211. [Google Scholar] [CrossRef]
- Kunzler, A.M.; Helmreich, I.; Chmitorz, A.; König, J.; Binder, H.; Wessa, M.; Lieb, K. Psychological interventions to foster resilience in healthcare professionals. Cochrane Database Syst. Rev. 2020, 2020, CD012527. [Google Scholar] [CrossRef]
- Rieckert, A.; Schuit, E.; Bleijenberg, N.; Cate, D.T.; De Lange, W.; Ginkel, J.M.D.M.-V.; Mathijssen, E.; Smit, L.C.; Stalpers, D.; Schoonhoven, L.; et al. How can we build and maintain the resilience of our health care professionals during COVID-19? Recommendations based on a scoping review. BMJ Open 2021, 11, e043718. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.-H.; Tseng, P.-C.; Lin, C.-Y.; Lin, K.-H.; Chen, Y.-Y. Burnout in the intensive care unit professionals: A systematic review. Medicine 2016, 95, e5629. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n | % | RS-5 a (M ± SD) | Univariate Test Statistics b | Effect Size c | p | Multivariate Test Statistics | Effect Size d | p | |
|---|---|---|---|---|---|---|---|---|---|
| Gender | t(625) = 0.82 | 0.05 | 0.413 | F(11,017) = 0.35 | 0.000 | 0.553 | |||
| Male | 296 | 28.6 | 29.04 ± 4.28 | ||||||
| Female | 738 | 71.4 | 28.78 ± 4.95 | ||||||
| Age group | F(4397) = 6.58 | 0.02 | <0.001 | F(41,017) = 3.32 | 0.013 | 0.010 | |||
| 18–30 | 192 | 18.6 | 27.88 ± 5.16 | ||||||
| 31–40 | 227 | 22.0 | 28.41 ± 4.90 | ||||||
| 41–50 | 191 | 18.5 | 28.57 ± 4.79 | ||||||
| 51–60 | 333 | 32.2 | 29.52 ± 4.41 | ||||||
| >60 | 91 | 8.8 | 30.22 ± 4.15 | ||||||
| Children | t(966) = 3.83 | 0.24 | <0.001 | F(11,017) = 4.28 | 0.004 | 0.039 | |||
| Yes | 558 | 54.0 | 29.38 ± 4.50 | ||||||
| No | 476 | 46.0 | 28.24 ± 5.00 | ||||||
| Living situation | t(377) = −1.23 | 0.09 | 0.221 | F(11,017) = 0.11 | 0.000 | 0.739 | |||
| Living alone | 240 | 23.2 | 28.52 ± 4.97 | ||||||
| Not living alone | 794 | 76.8 | 28.96 ± 4.70 | ||||||
| Occupation | F(4379) = 2.05 | 0.01 | 0.086 | F(41,017) = 1.48 | 0.006 | 0.206 | |||
| Physician | 257 | 24.9 | 29.20 ± 4.30 | ||||||
| Nurse | 330 | 31.9 | 28.54 ± 5.07 | ||||||
| MTA | 90 | 8.7 | 27.88 ± 6.08 | ||||||
| PPE | 154 | 14.9 | 29.43 ± 3.81 | ||||||
| Else | 203 | 19.6 | 28.94 ± 4.76 | ||||||
| Job Experience | F(3180) = 0.98 | 0.00 | 0.403 | F(31,017) = 0.27 | 0.001 | 0.850 | |||
| <3 years | 136 | 13.2 | 28.46 ± 4.24 | ||||||
| 3–6 years | 129 | 12.5 | 28.49 ± 4.93 | ||||||
| >6 years | 713 | 69.0 | 29.02 ± 4.82 | ||||||
| unknown | 56 | 5.4 | 28.57 ± 4.88 | ||||||
| Fulltime employment | t(707) = −0.27 | 0.02 | 0.788 | F(11,017) = 0.78 | 0.001 | 0.378 | |||
| Full time | 701 | 67.8 | 28.83 ± 4.90 | ||||||
| Part time | 333 | 32.2 | 28.91 ± 4.49 | ||||||
| Contact with SARS-CoV-2 | t(879) = −0.73 | 0.05 | 0.463 | F(11,017) = 1.35 | 0.001 | 0.246 | |||
| yes | 627 | 60.6 | 28.94 ± 4.80 | ||||||
| no | 407 | 39.4 | 28.72 ± 4.71 |
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| 1. Gender a | ||||||||
| 2. Age b | −0.11 *** | |||||||
| 3. Resilience (RS-5) | 28.86 | 4.77 | −0.02 | 0.15 *** | ||||
| 4. Depression (PHQ-2) | 1.54 | 1.37 | 0.06 * | −0.17 *** | −0.36 *** | |||
| 5. Anxiety (GAD-2) | 1.41 | 1.43 | 0.07 * | −0.09 ** | −0.34 *** | 0.63 *** | ||
| 6. Subj. Stress Burden | 2.13 | 0.96 | 0.07 * | 0.00 | −0.20 *** | 0.41 *** | 0.43 *** |
| Model | R2 | ∆ R2 | B | SE | ß | t | p | ||
|---|---|---|---|---|---|---|---|---|---|
| Depression Symptoms (PHQ-2) | 1 | (constant) | 2.915 | 0.308 | 9.47 | <0.001 | |||
| Burden | 0.249 | 0.249 | 0.497 | 0.046 | 0.349 | 10.90 | <0.001 | ||
| Resilience | −0.084 | 0.009 | −0.294 | −9.39 | <0.001 | ||||
| 2 | (constant) | 1.533 | 0.039 | 39.63 | <0.001 | ||||
| Burden | 0.501 | 0.046 | 0.351 | 10.83 | <0.001 | ||||
| Resilience | 0.250 | 0.001 | −0.083 | 0.009 | −0.288 | −9.26 | <0.001 | ||
| Burden × Resilience | −0.010 | 0.009 | −0.033 | −1.06 | 0.291 | ||||
| Anxiety Symptoms (GAD-2) | 1 | (constant) | 2.446 | 0.346 | 7.08 | <0.001 | |||
| Burden | 0.250 | 0.250 | 0.568 | 0.048 | 0.380 | 11.89 | <0.001 | ||
| Resilience | −0.078 | 0.010 | −0.260 | −7.63 | <0.001 | ||||
| 2 | (constant) | 1.386 | 0.040 | 34.32 | <0.001 | ||||
| Burden | 0.575 | 0.048 | 0.384 | 11.95 | <0.001 | ||||
| Resilience | 0.255 | 0.005 | −0.074 | 0.010 | −0.246 | −7.50 | <0.001 | ||
| Burden × Resilience | −0.021 | 0.010 | −0.070 | −2.25 | 0.025 | ||||
| Level of Moderator Variable | B | SE | t | p |
|---|---|---|---|---|
| Low resilience | 0.68 | 0.07 | 9.53 | <0.001 |
| Average resilience | 0.58 | 0.05 | 11.94 | <0.001 |
| High resilience | 0.47 | 0.06 | 7.83 | <0.001 |
| Effect | Depression Symptoms (PHQ-2) | Anxiety Symptoms (GAD-2) | ||||||
|---|---|---|---|---|---|---|---|---|
| B (SE) | ß | p-Value | Bias-Corrected Bootstrap 95% CI | B (SE) | ß | p-Value | Bias-Corrected Bootstrap 95% CI | |
| a | −0.98 (0.15) | −0.20 | <.001 | −0.98 (0.15) | −0.20 | <0.001 | ||
| b | −0.08 (0.01) | −0.29 | <0.001 | −0.08 (0.01) | −0.26 | <0.001 | ||
| c | 0.58 (0.04) | 0.41 | <0.001 | 0.64 (0.04) | 0.43 | <0.001 | ||
| c’ | 0.50 (0.04) | 0.35 | <0.001 | 0.57 (0.04) | 0.38 | <0.001 | ||
| a × b | 0.08 (0.02) | 0.06 | <0.001 | [0.05,0.12] | 0.08 (0.02) | 0.05 | <0.001 | [0.05,0.11] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmuck, J.; Hiebel, N.; Kriegsmann-Rabe, M.; Schneider, J.; Matthias, J.-K.; Erim, Y.; Morawa, E.; Jerg-Bretzke, L.; Beschoner, P.; Albus, C.; et al. Individual Stress Burden and Mental Health in Health Care Workers during the COVID-19 Pandemic: Moderating and Mediating Effects of Resilience. Int. J. Environ. Res. Public Health 2022, 19, 6545. https://doi.org/10.3390/ijerph19116545
Schmuck J, Hiebel N, Kriegsmann-Rabe M, Schneider J, Matthias J-K, Erim Y, Morawa E, Jerg-Bretzke L, Beschoner P, Albus C, et al. Individual Stress Burden and Mental Health in Health Care Workers during the COVID-19 Pandemic: Moderating and Mediating Effects of Resilience. International Journal of Environmental Research and Public Health. 2022; 19(11):6545. https://doi.org/10.3390/ijerph19116545
Chicago/Turabian StyleSchmuck, Jonas, Nina Hiebel, Milena Kriegsmann-Rabe, Juliane Schneider, Julia-Katharina Matthias, Yesim Erim, Eva Morawa, Lucia Jerg-Bretzke, Petra Beschoner, Christian Albus, and et al. 2022. "Individual Stress Burden and Mental Health in Health Care Workers during the COVID-19 Pandemic: Moderating and Mediating Effects of Resilience" International Journal of Environmental Research and Public Health 19, no. 11: 6545. https://doi.org/10.3390/ijerph19116545