
Trends in COVID-19 Inpatient Cases and Hospital Capacities during the Emergence of the Omicron Variant in the United States

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Variables
2.2. Data Analyses
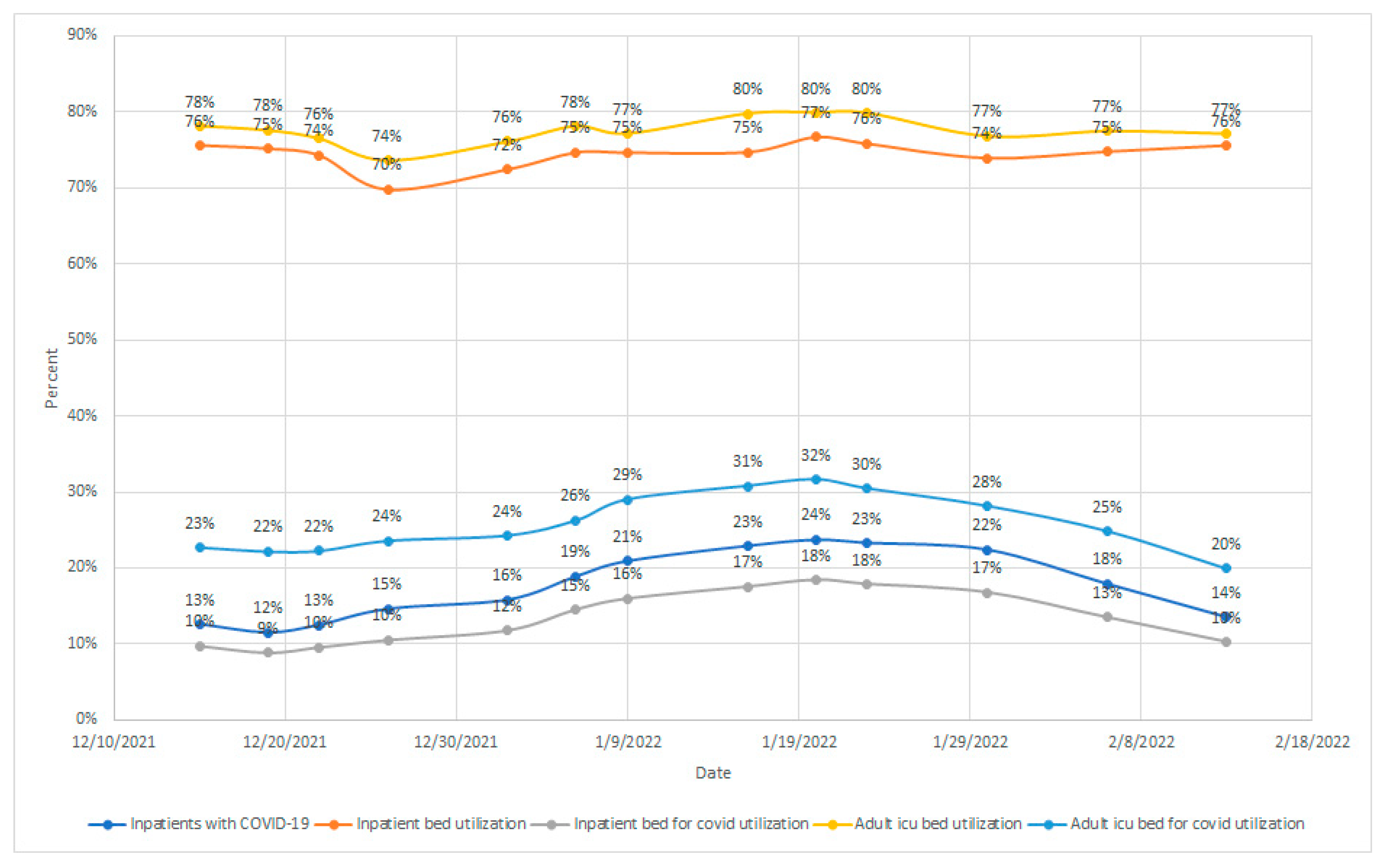
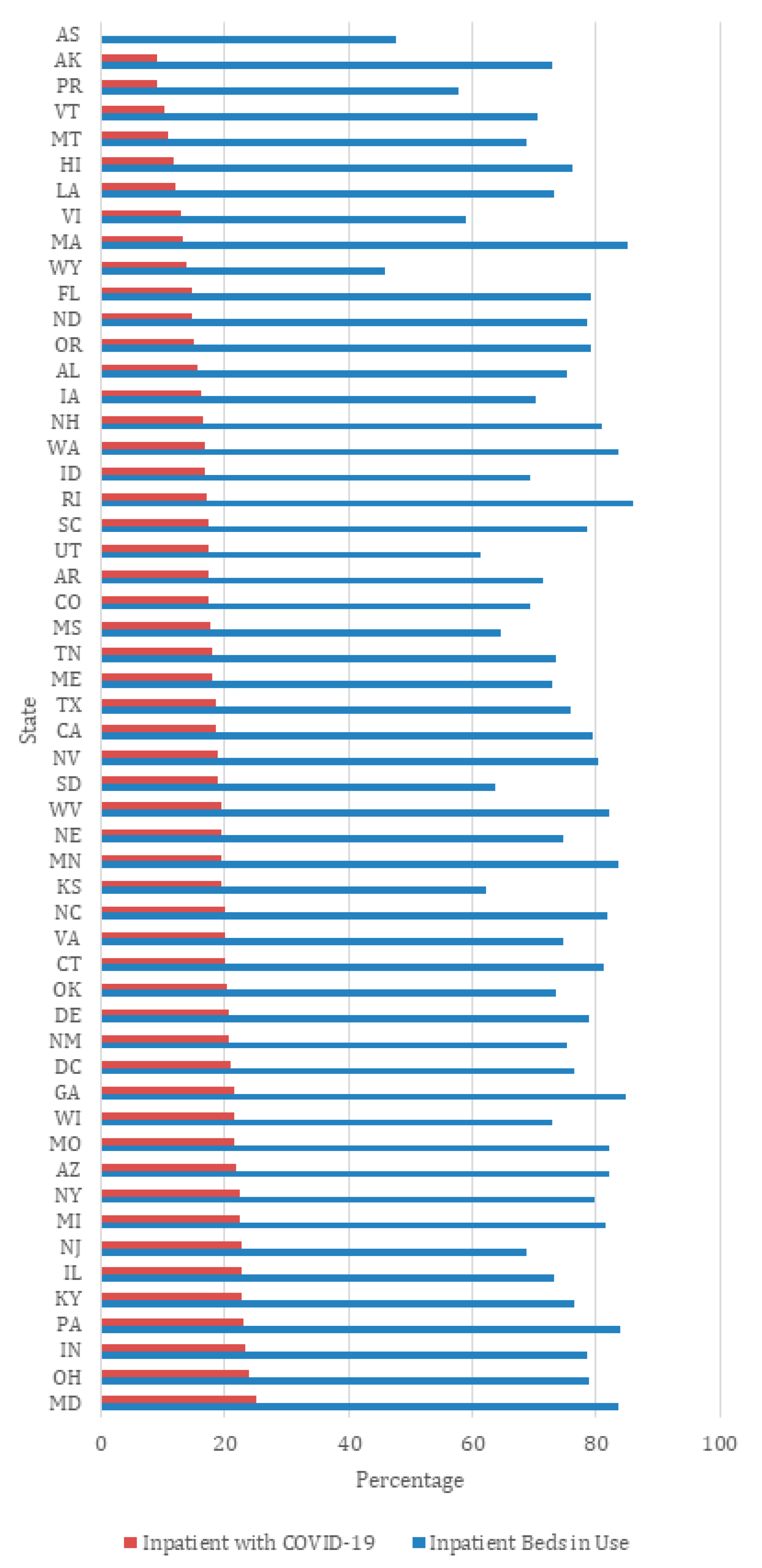
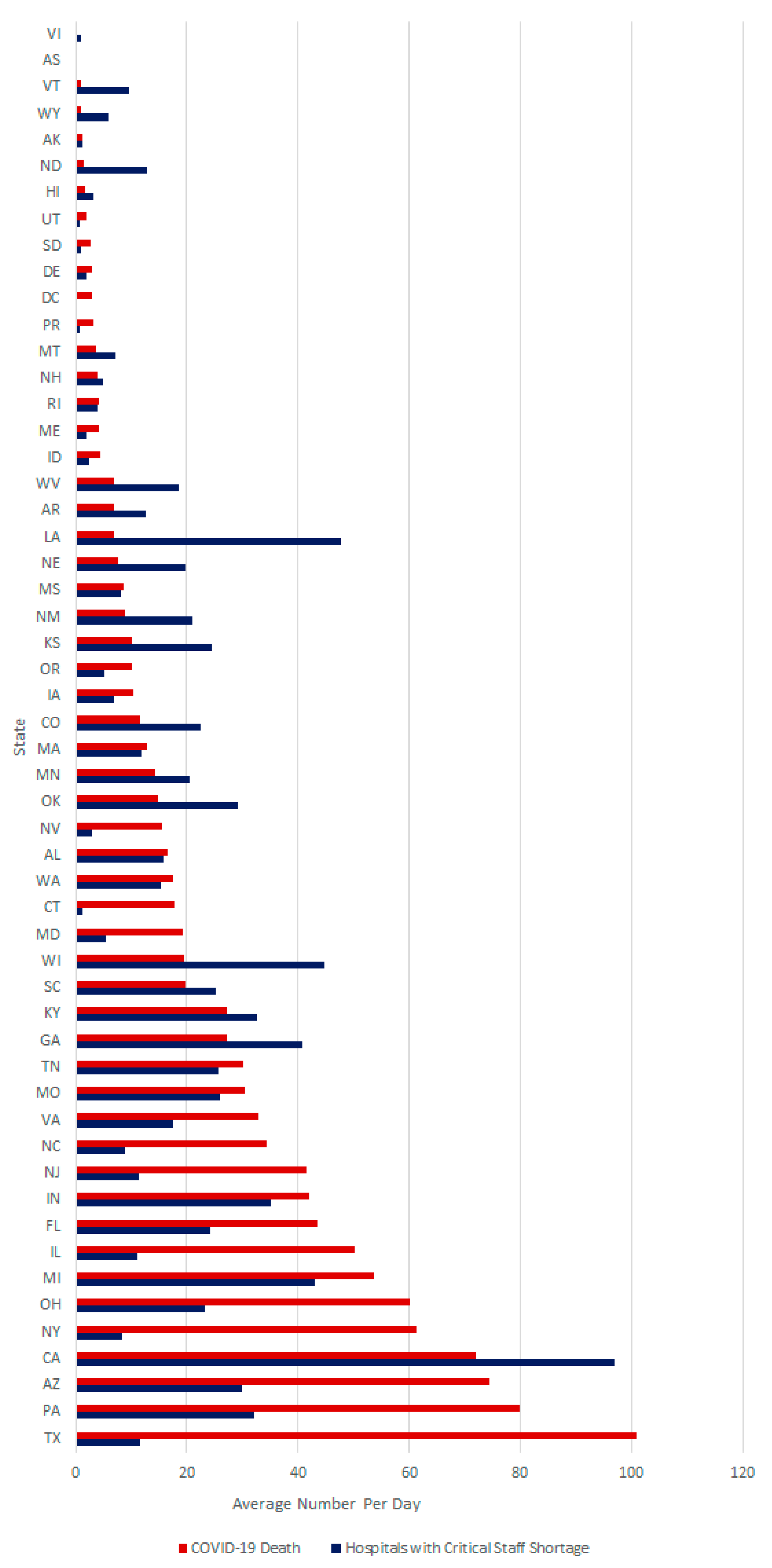
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, M.; Adil, S.F.; Alkhathlan, H.Z.; Tahir, M.N.; Saif, S.; Khan, M.; Khan, S.T. COVID-19: A Global Challenge with Old History, Epidemiology and Progress so Far. Molecules 2021, 26, 39. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D.; Okeagu, C.N.; Pham, A.D.; Silva, R.A.; Hurley, J.J.; Arron, B.L.; Sarfraz, N.; Lee, H.N.; Ghali, G.E.; Gamble, J.W.; et al. Economic Impact of COVID-19 Pandemic on Healthcare Facilities and Systems: International Perspectives. Best Pract. Res. Clin. Anaesthesiol. 2021, 35, 293–306. [Google Scholar] [CrossRef] [PubMed]
- McCabe, R.; Schmit, N.; Christen, P.; D’Aeth, J.C.; Løchen, A.; Rizmie, D.; Nayagam, S.; Miraldo, M.; Aylin, P.; Bottle, A.; et al. Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC Med. 2020, 18, 329. [Google Scholar] [CrossRef] [PubMed]
- Levin, Z.; Choyke, K.; Georgiou, A.; Sen, S.; Karaca-Mandic, P. Trends in Pediatric Hospitalizations for Coronavirus Disease 2019. JAMA Pediatrics 2021, 175, 415–417. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact of the COVID-19 Pandemic on Hospital Admissions in the United States. Health Aff. 2020, 39, 2010–2017. [Google Scholar] [CrossRef]
- Auener, S.; Kroon, D.; Wackers, E.; Dulmen, S.V.; Jeurissen, P. COVID-19: A Window of Opportunity for Positive Healthcare Reforms. Int. J. Health Policy Manag. 2020, 9, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Bridgman, A.; Merkley, E.; Loewen, P.J.; Owen, T.; Ruths, D.; Teichmann, L.; Zhilin, O. The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media. Harv. Kennedy Sch. Misinf. Rev. 2020, 1, 1–18. [Google Scholar] [CrossRef]
- Kokudo, N.; Sugiyama, H. Hospital capacity during the COVID-19 pandemic. Glob. Health Med. 2021, 3, 56–59. [Google Scholar] [CrossRef] [PubMed]
- HealthData.gov. COVID-19 Reported Patient Impact and Hospital Capacity by State Timeseries. U.S. Department of Health & Human Services. 2022. Available online: https://healthdata.gov/Hospital/COVID-19-Reported-Patient-Impact-and-Hospital-Capa/g62h-syeh (accessed on 18 April 2022).
- Iuliano, A.D.; Brunkard, J.M.; Boehmer, T.K.; Peterson, E.; Adjei, S.; Binder, A.M.; Cobb, S.; Graff, P.; Hidalgo, P.; Panaggio, M.J.; et al. Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared with Previous SARS-CoV-2 High Transmission Periods—United States, December 2020–January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 146–152. [Google Scholar] [CrossRef] [PubMed]
- World Population Review. United States by Density 2022. 2022. Available online: https://worldpopulationreview.com/state-rankings/state-densities (accessed on 18 April 2022).
- World Population Review. Median Age by State 2022. 2022. Available online: https://worldpopulationreview.com/state-rankings/median-age-by-state (accessed on 18 April 2022).
- Healio. Omicron’s Burden on Health System Apparent in New Data. 2022. Available online: https://www.healio.com/news/infectious-disease/20220125/omicrons-burden-on-health-system-apparent-in-new-data (accessed on 18 April 2022).
- Klein, M.G.; Cheng, C.J.; Lii, E.; Mao, K.; Mesbahi, H.; Zhu, T.; Muckstadt, J.A.; Hupert, N. COVID-19 Models for Hospital Surge Capacity Planning: A Systematic Review. Disaster Med. Public Health Prep. 2020, 16, 390–397. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, M.; Mennell, B.; Christensen, A.; Mohajeri, A.; Azabache, H.; Moffat, R. Trends in COVID-19 Inpatient Cases and Hospital Capacities during the Emergence of the Omicron Variant in the United States. COVID 2022, 2, 1207-1213. https://doi.org/10.3390/covid2090087
Hung M, Mennell B, Christensen A, Mohajeri A, Azabache H, Moffat R. Trends in COVID-19 Inpatient Cases and Hospital Capacities during the Emergence of the Omicron Variant in the United States. COVID. 2022; 2(9):1207-1213. https://doi.org/10.3390/covid2090087
Chicago/Turabian StyleHung, Man, Benjamin Mennell, Angela Christensen, Amir Mohajeri, Helen Azabache, and Ryan Moffat. 2022. "Trends in COVID-19 Inpatient Cases and Hospital Capacities during the Emergence of the Omicron Variant in the United States" COVID 2, no. 9: 1207-1213. https://doi.org/10.3390/covid2090087