
Manuscript accepted on :02-03-2022
Published online on: 18-04-2022
Plagiarism Check: Yes
Reviewed by: Dr. Chandrabose Selvaraj
Second Review by: Dr. Luis del Carpio
Final Approval by: Dr. Kishore Kumar Jella
Prathibha KM , Soma Sri Harsha and Premkumar Sundararajan*
, Soma Sri Harsha and Premkumar Sundararajan*
Department of Physiology, Saveetha Medical College, Thandalam, Chennai - 602 105, India.
Corresponding Author E-mail: saralapremkumar@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2442
Abstract
Background: With 3.95 lakhs of active COVID-19 cases in India and Tamilnadu being the second-largest hub of COVID-19, the health and social impact on the public, especially the health care warriors would be considerable. Objective: To evaluate and compare the levels of knowledge, preventive behaviour and risk perception of South Indian Health Care Professional(HCP) Students regarding COVID-19.Methods: An institution-based cross-sectional questionnaire survey was conducted in a tertiary care centre and teaching hospital in May-June 2020 amongst 873 students pursuing various HCP courses. The questionnaire comprised four sections - demographic details, COVID–19 related knowledge, preventive behaviour and risk perception. Results: Females volunteered to complete the survey (n= 623; 71.4%) more than males (n= 250; 28.6%). Most participants had received awareness about COVID-19 (n=860; 98.5%) from many resources of information. While females (97.50 ± 8.94) had significantly higher scores on items for preventive behaviour than males (94.7±15.55; p=0.006), the scores were similar for knowledge and risk perception. There was a statistically significant difference in risk perception among various courses with students pursuing Pharmacy having higher risk perception. Items regarding the use of masks in general and hospital setups and availability of antivirals for COVID-19 received many incorrect responses. Conclusions: HCP students presented with high levels of COVID-19 related knowledge and preventive behaviour, but moderate risk perception. Continuing education programs and preventive behavioural training are the need of the hour to strengthen the knowledge and alleviate the anxiety of HCP students towards the pandemic.
Keywords
2019–nCoV; COVID-19; Health Care Professionals; Knowledge; Medical Students; Novel Coronavirus; Paramedical Students; Preventive Behaviour; Risk Perception
Download this article as:| Copy the following to cite this article: Prathibha K. M, Harsha S. S, Sundararajan P. Knowledge, Preventive Behaviour and Risk Perception about COVID-19 in Health Care Professional Students. Biomed Pharmacol J 2022;15(2). |
| Copy the following to cite this URL: Prathibha K. M, Harsha S. S, Sundararajan P. Knowledge, Preventive Behaviour and Risk Perception about COVID-19 in Health Care Professional Students. Biomed Pharmacol J 2022;15(2). Available from: https://bit.ly/3KW5qqY |
Introduction
In December 2019, a cluster of patients diagnosed with pneumonia of unknown origin was linked to a seafood market in Wuhan, China.1 What followed would be etched in history as one of the major pandemics that the human race battled in all walks of life. The novel Coronavirus (2019 nCoV) has spread globally with alarmingly high death tolls that have alerted a public health emergency.2 Human to human transmission through droplets and fomites, presence of asymptomatic carriers and cases with mild clinical presentation and lack of adequate infrastructure to provide isolation for all infected individuals and their close contacts, particularly in resource-limited countries have aggravated the spread and mortality.3 The plethora of comorbid conditions, absence of vaccines and lack of specific antiviral agents have also added to the risk. 4
With 33.4 crores cases globally (of which 3.79 crores of cases are in India) and Tamilnadu being the fourth-largest hub of COVID-19, the health and social impact on the public, especially the health care warriors would be considerable. 5 (Fig.1& 2)
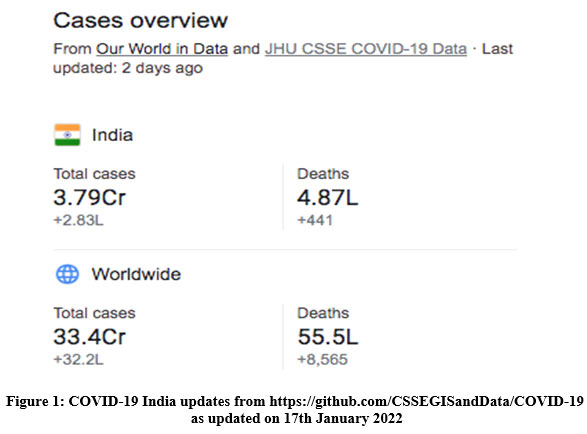 |
Figure 1: COVID-19 India updates from https://github.com /CSSEGIS and Data/ COVID-19 as updated on 17th January 2022. |
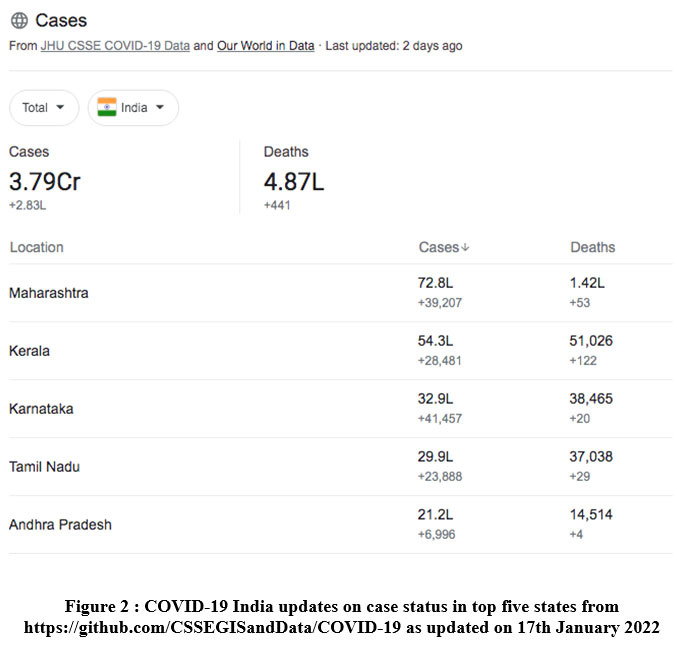 |
Figure 2 : COVID-19 India updates on case status in top five states from https://github.com/ CSSEGISandData/COVID-19 as updated on 17th January 2022. |
Several studies from the past during SARS and MERS epidemics reported the role of health care workers and medical students in the trying times.7 The spread of the COVID-19 virus entrusted all medical professionals, both on a personal and professional scale to demonstrate their knowledge and commitment to society to curb the spread and promote the wellbeing of the community. A report by the end of April 2020 revealed hundreds of health care workers testing positive for COVID-19 and the numbers have only exponentially increased since then. 8
A survey was conducted during the Severe Acute Respiratory Syndrome (SARS) epidemic in 2006 in teaching hospitals of two universities in Hongkong.9 The anxiety level caused by SARS in medical students at the teaching hospital was higher than in non-medical students in the same university and lowest in students of the other university situated 20 km away from the affected hospital. 7 Existing literature on the knowledge or behaviour of HCP students was scanty pointing towards the need for understanding the current scenario. A study on Iranian medical students reported adequate knowledge but moderate self-protective behaviour and poor risk perception.10 In India, a questionnaire-based survey on the awareness, knowledge, and infection control practices related to COVID-19 was conducted in the health care workers of Mumbai Metropolitan Region which pointed towards the dire need for regular educational interventions and training programs on infection in the healthcare setting.11
With the progressively increasing number of cases and deaths coupled with the widespread presence of Health Care Professional (HCP) students of the teaching hospital of our University in large numbers across the nation, the objective of the present study was to evaluate the levels of awareness, attitude and risk perception towards the pandemic.
Methodology
An institution-based cross-sectional study was conducted among the students (n=873) pursuing undergraduate Health Care Professional courses (MBBS along with Interns (CRRI), BDS, BOT (Occupational therapy), BPT (Physiotherapy), Allied Health Sciences, Nursing, Pharmacy, M.Sc. Health sciences) in a tertiary health care cum teaching hospital of Saveetha Institute of Medical and Technical Sciences, Chennai. Participation in the survey was entirely voluntary. The study proposal was taken up to the IRB for approval through emails and permission was obtained.
The present study was a web-based questionnaire survey conducted from 31st May to 7th June 2020. The required sample size was calculated to be 666. However, on sharing the survey link through various online portals to the constituent colleges, the authors received 935 responses. During data analysis, 62 responses (incorrect and duplicate entries) were deleted, leaving the sample size to be 873 (adequate and more than the required number).
The survey was conducted using a structured and validated online questionnaire in the English language used in a health care setting in Iran.10 The questionnaire comprised four sections – demographic details, assessment of COVID-19 related knowledge, self–reported preventive behaviours and risk perceptions among the HCP students. For demographic details, the study participants were asked to provide information on their age, gender, level of education, COVID-19 related education and the source from where they obtained COVID related awareness. With regard to COVID-19 related knowledge, there were fifteen items in the questionnaire investigating the basic science and aetiology of COVID-19, symptoms and incubation period, transmission, diagnosis, treatment, referral, prevention measures for the public and medical professionals, in particular. About nine items in the questionnaire investigated the self–reported preventive behaviours like the use of public places in daily life, hand washing, surface disinfection and social distancing. Each item in the knowledge and behaviour section was given a value of one if correct and zero if incorrect, amounting to a total score of 15 for knowledge and 9 for behaviour. The total score was converted into a percentile for knowledge and behaviour related sections. The scores more than or equal to 75 per cent were designated as high performance and below 75 per cent as low performance.
The questionnaire had two items to assess risk perception among participants. Responses were provided using a 4-point Likert-type scale, from 1 = not at all to 4 = absolutely yes and the total score ranged from 2 to 8. Scores between 2 to 3 were designated as low and 6 to 8 were designated as high-risk perception.
Data analysis was done using the SPSS version 23. None of the major outcomes followed a normal distribution and was analyzed using nonparametric tests. The frequencies and percentages were computed for categorical variables and the means and standard deviations were tabulated.
Results
The mean age of the study participants (n = 873) was 19.42 ± 1.48 years. A larger number of females volunteered to complete the survey (n= 623; 71.4%) when compared to males (n= 250; 28.6%). Table 1 shows the gender distribution and course of study, the percentage of participants who had COVID-19 related education and the source of information among the study participants. HCP students from the College of Allied Health Sciences (33.1%) volunteered the maximum to complete the survey, followed by students of Medicine (23.8%) and Physiotherapy (16.7%). Most of the participants received awareness on the COVID-19 pandemic (n=860; 98.5%) from more than one source of education with newspaper and social media (37.7%) being the single most used resource. (Table 1).
Table 1: Demographic Profile and COVID 19 related knowledge and source of the study participants.
| Characteristics | Frequency (n=873) | Percent (%) |
| Gender | ||
| Male | 250 | 28.6 |
| Female | 623 | 71.4 |
| Course of study | ||
| MBBS | 208 | 23.8 |
| BDS | 20 | 2.3 |
| BPT (Physiotherapy) | 146 | 16.7 |
| BOT (Occupational therapy) | 84 | 9.6 |
| Allied Health Sciences | 289 | 33.1 |
| Pharmacy | 24 | 2.7 |
| Nursing | 89 | 10.2 |
| M.Sc. Health Sciences | 13 | 1.5 |
| Received awareness/education about COVID-19 | ||
| Yes | 860 | 98.5 |
| No | 13 | 1.5 |
| If yes, source of education | ||
| WHO, CDC, UpToDate | 36 | 4.2 |
| National guidelines | 14 | 1.6 |
| Newspaper/ Social Media | 324 | 37.7 |
| All of the above | 486 | 56.5 |
Among the participants who reported that they received awareness/ education about COVID-19, there was a statistically significant difference in scores for preventive behaviour and risk perception about the source of education resorted to COVID 19 related information. Using the Dunn-Bonferroni Post-hoc test, it was found that the preventive behaviour scores were statistically lower for those who received awareness through WHO, CDC, UpToDate than those who received awareness through all the sources (p=0.011). Also, the risk perception scores were statistically lower for those who received awareness through newspaper and social media than those who received awareness through all the sources (p=0.001).
Table 2: Differences in Knowledge, Preventive behaviours and Risk Perception by Gender and Source of education for COVID-19 related information.
| Variables | Characteristics | N (%) | Knowledge (Possible range: 0-100) | P-value | Preventive Behaviours (Possible range: 0-100) | P-value | Risk Perception (Possible range: 2-8) | P-value |
| Mean (SD) | Mean (SD) | Mean (SD) | ||||||
| Gender | Male | 250 (28.6) | 79.16 (9.81) | 0.177 | 94.72 (15.55) | 0.006** | 4 (2) | 0.571 |
| Female | 623 (71.4) | 79.96 (9.49) | 97.50 (8.94) | 4 (2) | ||||
| Source of education/awareness # | WHO, CDC, UpToDate | 36 (4.2) | 80.30 (9.35) | 0.391 | 91.11 (23.64) | 0.035* | 4 (2) | 0.015* |
| National guidelines | 14 (1.6) | 77.27 (9.26) | 97.14 (7.26) | 4 (1) | ||||
| Newspapers/ Social Media | 324 (37.7) | 79.24 (9.73) | 96.30 (11.72) | 3 (2) | ||||
| All of the above | 486 (56.5) | 80.21 (9.37) | 97.61 (8.95) | 4 (2) |
# Includes only those who reported that they received awareness/ education about COVID-19 (860/873)
Note: Tests used – Mann-Whitney U and Kruskall-Wallis test
*Significant at 0.05 level, ** Significant at 0.01 level
Table 2 shows the differences observed in knowledge about COVID-19, preventive behaviour and risk perception between sexes, courses of study and sources of COVID-19 related awareness tested for significance using Mann-Whitney U and Kruskall-Wallis test. It was observed that males and females had similar scores pertaining to knowledge and risk perception, while females (97.50 ± 8.94) had significantly higher scores on items for preventive behaviour than males (94.7±15.55; p=0.006).
Among the 15 questions pertaining to knowledge on COVID 19, the mean score of all the participants was 79.74 ± 9.58. There was a higher number of wrong responses to questions no 12, 13 and 14. (Table 3) With regard to self-protective behaviour, the mean score of all the participants was 96.7 ± 11.3. (Table 4).
Table 3: Percentage of correct responses for items evaluating Knowledge regarding COVID-19.
| S. No | Items | Number (N= 873) | Percentage |
| 1. | COVID-19 is a respiratory infection caused by a new species of the coronavirus family. | 845 | 96.8 |
| 2. | The first case of COVID-19 was diagnosed in Wuhan, China. | 865 | 99.1 |
| 3. | The origin of COVID-19 is not clear but it seems that it has been transmitted to humans by seafoods, snakes or bats. | 702 | 80.4 |
| 4. | Common symptoms of COVID-19 are fever, cough and shortness of breath but nausea and diarrhoea were reported rarely. | 852 | 97.6 |
| 5. | The incubation period of COVID-19 is up to 14 days with a mean of 5 days. | 817 | 93.6 |
| 6. | COVID-19 can be diagnosed by PCR test on samples collected from nasopharyngeal and oropharyngeal discharge or sputum and bronchial washing. | 819 | 93.8 |
| 7. | COVID-19 is transmitted through respiratory droplets such as cough and sneeze. | 860 | 98.5 |
| 8. | COVID-19 is transmitted through close contacts with an infected case (especially in the family, crowded places and health centres). | 867 | 99.3 |
| 9. | COVID-19 disease can be prevented through handwashing and personal hygiene. | 865 | 99.1 |
| 10. | A medical mask is useful to prevent the spread of respiratory droplets during coughing. | 856 | 98.1 |
| 11. | COVID-19 disease can be prevented through no close contacts such as handshakes or kissing, not attending meetings and frequent hand disinfection. | 852 | 97.6 |
| 12. | All people in the society should wear masks. | 58 | 6.6 |
| 13. | Only during intubation, suction, bronchoscopy and cardiopulmonary resuscitation do you have to wear an N95 mask. | 576 | 66.0 |
| 14. | COVID-19 disease can be treated by usual antiviral drugs. | 460 | 52.7 |
| 15. | If symptoms of COVID-19 appear within 14 days from direct contact with a suspected case, the person should inquire at a nearby public health centre. | 855 | 97.9 |
Table 4: Percentage of correct responses for items evaluating preventive behaviour regarding COVID – 19.
| S. No | Items | Number (N= 873) | Percentage |
| 1 | I cancelled or postponed meetings with friends, eating-out and sports events | 847 | 97.0 |
| 2. | I reduced the use of public transportation | 861 | 98.6 |
| 3. | I went shopping less frequently | 857 | 98.2 |
| 4. | I reduced the use of closed spaces, such as library, theatres and cinema. | 863 | 98.9 |
| 5. | I avoided coughing around people as much as possible. | 866 | 99.2 |
| 6. | I avoided places where a large number of people are gathered. | 867 | 99.3 |
| 7. | I increased the frequency of cleaning and disinfecting items that can be easily touched with hands (i.e. door handles and surfaces). | 837 | 95.9 |
| 8. | I washed my hands more often than usual. | 855 | 97.9 |
| 9. | I discussed COVID-19 prevention with my family and friends. | 860 | 98.5 |
Risk perception about higher chances of being infected with COVID-19 was higher amongst the paramedical HCP students in comparison to the medical and dental students. As seen in Table 5, using Kruskal Wallis Test, it was found that there was a statistically significant difference in risk perception among HCP students of various courses. Using the Dunn-Bonferroni Post-hoc test, it was found that the risk perception scores of students of Pharmacy were significantly lower than those of other HCP students.
Table 5: Differences in Knowledge, Preventive behaviours and risk perception by Course of study of HCP students.
| Course of Study | N (%) | Knowledge (Possible range: 0-100) | P-value | Preventive Behaviours (Possible range: 0-100) | P-value | Risk Perception (Possible range: 2-8) | P-value |
| Mean (SD) | Mean (SD) | Mean (SD) | |||||
| MBBS | 208 (23.8) | 80.68 (8.63) | 0.556 | 97.31 (10.24) | 0.766 | 4 (2) | 0.000** |
| BDS | 20 (2.3) | 83.18 (6.10) | 96.00 (10.46) | 4 (2) | |||
| BPT (Physio therapy) | 146 (16.7) | 80.01 (9.76) | 96.71 (9.97) | 3 (2) | |||
| BOT (Occupational therapy) | 84 (9.6) | 79.55 (10.45) | 98.10 (6.67) | 4 (2) | |||
| Allied Health Sciences | 289 (33.1) | 79.36 (9.98) | 95.78 (13.85) | 4 (2) | |||
| Pharmacy | 24 (2.7) | 77.65 (10.38) | 98.33 (8.16) | 3 (1) | |||
| Nursing | 89 (10.2) | 78.24 (9.36) | 96.63 (10.97) | 4 (2) | |||
| M.Sc. Health Sciences | 13 (1.5) | 79.72 (10.60) | 96.92 (11.09) | 4 (2) |
Discussion
Emerging and reemerging pathogens are challenges for global public health. (12) Novel coronavirus like infections have always been likely to emerge periodically in humans across the globe. (13) The magnitude of the current COVID-19 pandemic highlights the importance of effective public health strategies to be practised, both by the public and health care professional workers. (14) It is imperative to ensure the awareness of health care workers and HCP students not only to provide efficient patient care but also to ensure the safety of self, families and the community. (15) Therefore, the present study was conducted as an attempt to understand the awareness levels, knowledge, behaviour and risk perception of the existing pandemic scenario of HCP students.
The present study showed similar scores in knowledge and risk perception related segments between males and females and significantly higher scores for preventive behaviour amongst the females. Also, it was observed that female students volunteered more than males to respond to the survey. Similar results were observed in a study on Iranian medical students, where they reported higher scores risk perception and correlated it to a higher awareness of the importance of the pandemic amongst females. (10)
Amongst all the HCP courses, students of Allied health sciences courses responded to the survey in large numbers, followed by Medicine and Physiotherapy. The active participation of the Allied Health Sciences students could be attributed to their larger numbers in the University and their earlier involvement in patient care during the course of study. It was encouraging to note that almost all the participants resorted to some resource for awareness. All sources of information like WHO, CDC, UpToDate, National guidelines, newspaper and social media were used by all study participants for COVID 19 related knowledge. However, it was observed that newspapers were the most used resource of information independently, thereby indicating that the HCP students must be encouraged to seek information from more evidence-based and reliable resources.
The present study showed similar scores in knowledge and preventive behaviour related segments between the students of all courses. The knowledge scores of the present study were similar to the study on Iranian medical students but higher than a few MERS related studies conducted during earlier epidemics. (7,16) In a survey conducted amongst the healthcare workers of South Korea, a poor level of knowledge of the modes of transmission of MERS coronavirus was observed. (16)
Item numbers 12, 13 and 14 had a lower percentage of correct responses which could be attributed to both deficiency of knowledge and the true/false type nature of the question, where the respondents could have carelessly ticked the first option. It was shocking to note that many had answered “No” to the question “if all people in the society should wear masks”. Further, people were unsure about the use of N95 masks (Item no.13) in the clinical setting during certain procedures. In a study conducted by Pranav D Modi et al, the nursing students exhibited the maximum score on the use of masks, respirators and related devices. The medical students also scored higher than the students of the present study. (11) Adequate training on the use of masks in general in the community, in special scenarios at the hospital set up must be provided in the form of video lectures and reading materials to all students.
Most of the HCP students were of the false belief that COVID-19 disease could be treated by the usual antiviral drugs (Item no.14). Awareness regarding the various antivirals under trial, vaccine trials, the scope of antimalarial agents like hydroxychloroquine (HCQ) and dexamethasone must be shared with students of the University.
The average score of preventive behaviour was higher than similar studies conducted in Iran and Saudi Arabia. (7,10) The overall risk perception scores were low amongst all students indicating their awareness and lack of undue fear in the given circumstances. But, the risk perception scores of students of Pharmacy were significantly higher than those of other HCP students. While interpreting the results along with a biostatistician, it was doubted if the statistical significance should be attributed to the large sample size and not the variable as such, because the actual scores varied only negligibly amongst groups. However, it was decided that measures to reduce risk perception, stress and anxiety amongst all students in the form of awareness lectures as webinars and messages through social media platforms would be organized. (9,17) Autoinfection is not only a risk for the health worker but also for their families and communities in which they live. (18) The above-mentioned results highlighted the need for more preventive behavioural training among the students to counteract the threats imposed by COVID-19 infection.
Limitations and Recommendations
The response rate to the survey was lower when compared to the existing number of students in the University. However, the current sample size which was more than the calculated one contributed to some statistically significant results which in reality did not translate to actual significant differences. Also, more number of questions in the risk perception segment could have contributed to a better understanding of the dimension per se. The present study could be preliminary research. Yet, the results could be used by the University to plan and execute training for HCP students of all courses. The pandemic is likely to cause great anxiety to the students, both at work and at home due to lockdown. Provision of clear guidelines and stress management awareness to all students to handle the anxiety and ambiguity during such outbreaks is essential. (9,19)
Conclusion
The novel coronavirus has led to a public health emergency of international concern representing a test of the global capacity and preparedness to detect, prevent and manage the threat and its associated complications. The HCP students of the present study presented with a high level of COVID-19 related knowledge and self-protective behaviour, but a moderate risk perception. Continuing education programs and preventive behavioural training are the need of the hour to strengthen the knowledge and alleviate the anxiety of HCP students towards the pandemic in the interest of self and global public health.
Acknowledgement
None
Conflicting Interests
There is no conflict of interest.
Funding Sources
There is no funding sources.
References
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020 Feb 20;382(8):727–33.
CrossRef - Habibzadeh P, Stoneman EK. The novel coronavirus: A bird’s eye view [Internet]. Vol. 11, International Journal of Occupational and Environmental Medicine. 2020 [cited 2020 Jun 25]. p. 65–71.
CrossRef - Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-NCOV infection from an asymptomatic contact in Germany [Internet]. Vol. 382, New England Journal of Medicine. Massachussetts Medical Society; 2020 [cited 2020 Jun 25]. p. 970–1.
CrossRef - Centers for Disease Control and Prevention. How to Protect Yourself & Others | CDC [Internet]. Coronavirus Disease 2019 (COVID-19). 2019 [cited 2020 Jun 25]. p. para. 4.
- Ministry of Health and Family Welfare. COVID-19 India [Internet]. Government of India. 2020 [cited 2020 Jun 25].
- http://covidindiaupdates.in/
- Elamin F, Nour MO, Babilghith AO, Natto HA, Al-Amin FO, Alawneh SM. Knowledge, attitude and practices of healthcare providers towards MERS-CoV infection at Makkah hospitals
- Radhakrishnan V, Sen S, Naresh S. Data | How many doctors and nurses have tested positive for coronavirus in India ? The Hindu [Internet]. 2020 [cited 2020 Jun 25];4.
- Wong TW, Gao Y, Tam WWS. Anxiety among university students during the SARS epidemic in Hong Kong. Stress Heal. 2007 Feb;23(1):31–5.
CrossRef - Taghrir MH, Borazjani R, Shiraly R. COVID-19 and iranian medical students; A survey on their related-knowledge, preventive behaviours and risk perception. Arch Iran Med [Internet]. 2020 [cited 2020 Jun 25];23(4):249–54.
CrossRef - Modi PD, Nair G, Uppe A, Modi J, Tuppekar B, Gharpure AS, et al. COVID-19 Awareness Among Healthcare Students and Professionals in Mumbai Metropolitan Region: A Questionnaire-Based Survey. Cureus [Internet]. 2020 Apr 2 [cited 2020 Jun 25];12(4).
CrossRef - Gao GF. From “A”IV to “Z”IKV: Attacks from Emerging and Re-emerging Pathogens. Vol. 172, Cell. Cell Press; 2018. p. 1157–9.
CrossRef - Cui J, Li F, Shi ZL. Origin and evolution of pathogenic coronaviruses [Internet]. Vol. 17, Nature Reviews Microbiology. Nature Publishing Group; 2019 [cited 2020 Jun 25]. p. 181–92.
CrossRef - Yin Y, Wunderink RG. MERS, SARS and other coronaviruses as causes of pneumonia. Vol. 23, Respirology. Blackwell Publishing; 2018. p. 130–7.
CrossRef - Chang D, Xu H, Rebaza A, Sharma L, Dela Cruz CS. Protecting health-care workers from subclinical coronavirus infection [Internet]. Vol. 8, The Lancet Respiratory Medicine. 2020 [cited 2020 Jun 25]. p. e13.
CrossRef - Alsahafi AJ, Cheng AC. Knowledge, attitudes and behaviours of healthcare workers in the kingdom of Saudi Arabia to MERS coronavirus and other emerging infectious diseases. Int J Environ Res Public Health [Internet]. 2016 [cited 2020 Jun 25];13(12).
CrossRef - Poon E, Liu KS, Cheong DL, Lee CK, Yam LYC, Tang WN. Impact of severe acute respiratory syndrome on anxiety levels of frontline health care workers. Hong Kong Med J [Internet]. 2004 [cited 2020 Jun 25];10(5):325–30.
- McCloskey B, Heymann DL. SARS to novel coronavirus – Old lessons and new lessons. Epidemiol Infect. 2020;1–4.
CrossRef - Shapiro SL, Shapiro DE, Schwartz GER. Stress management in medical education: A review of the literature. Acad Med [Internet]. 2000 [cited 2020 Jun 25];75(7):748–59.
CrossRef

