
Impact and Strategies on Joint Surgery Centers without Lockdowns during the Peak of the COVID-19 Pandemic: A Multicenter Cross-Sectional Study


Abstract
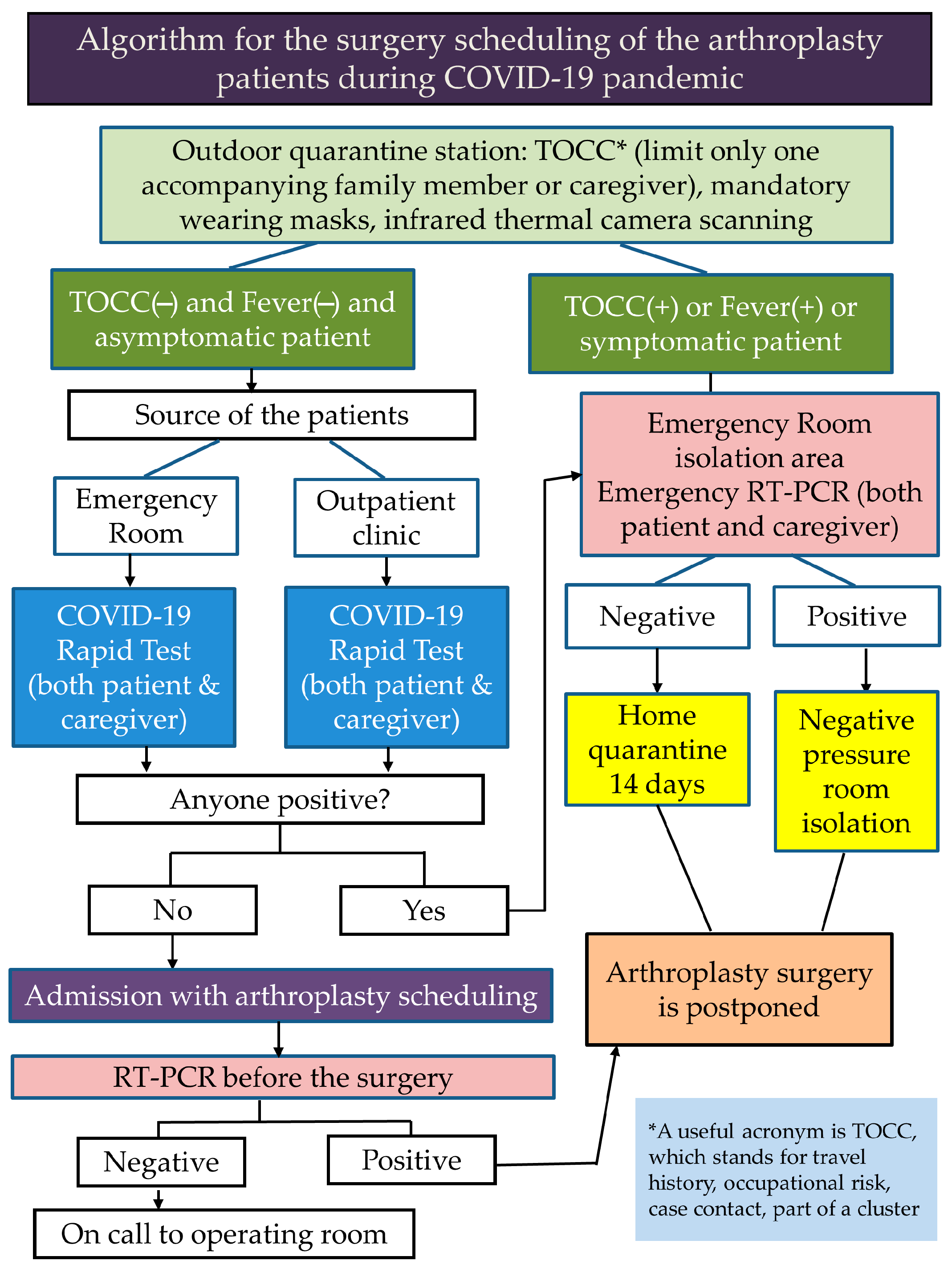
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition and Study Design
2.2. Statistical Analysis
3. Results
3.1. Overall Impact
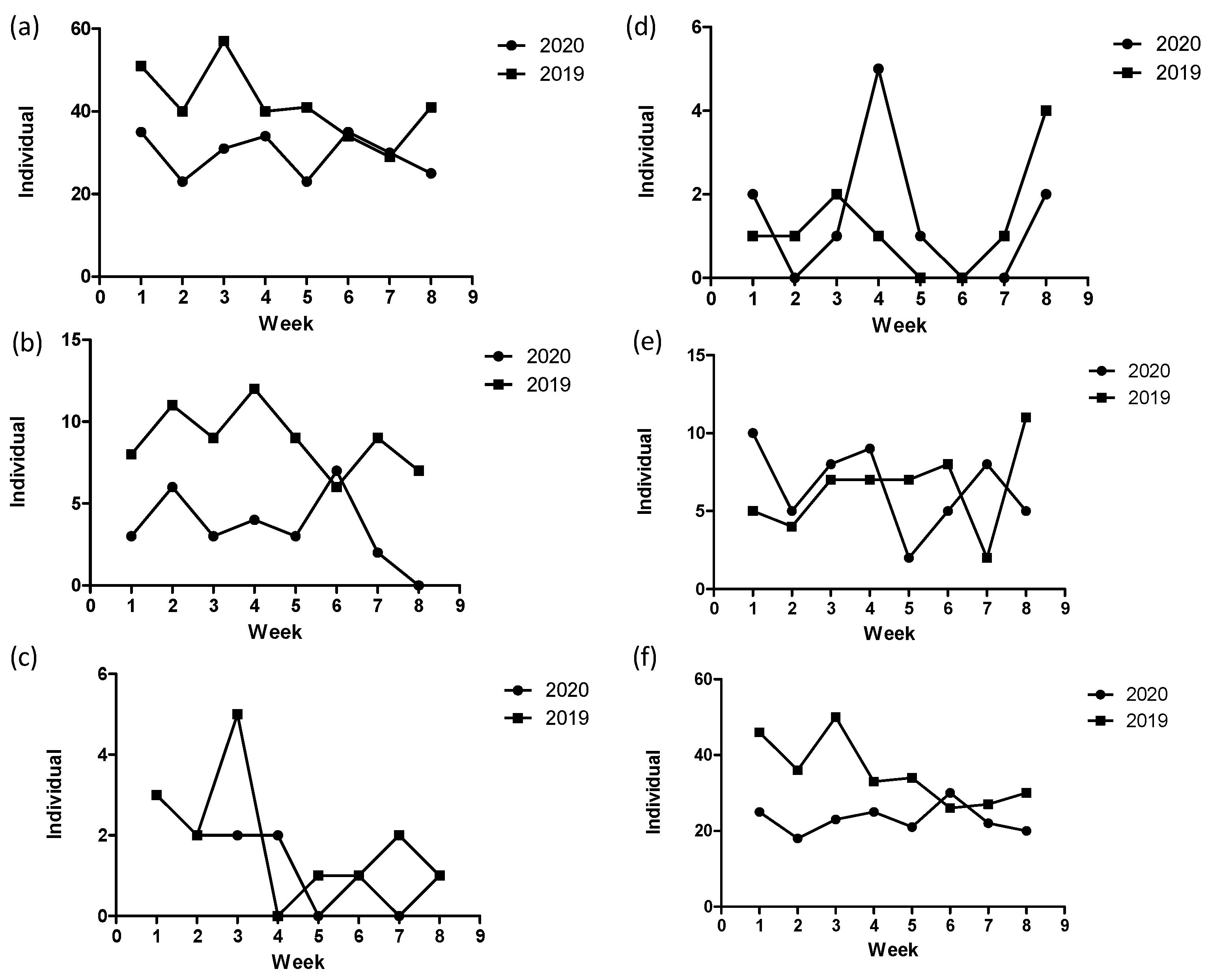
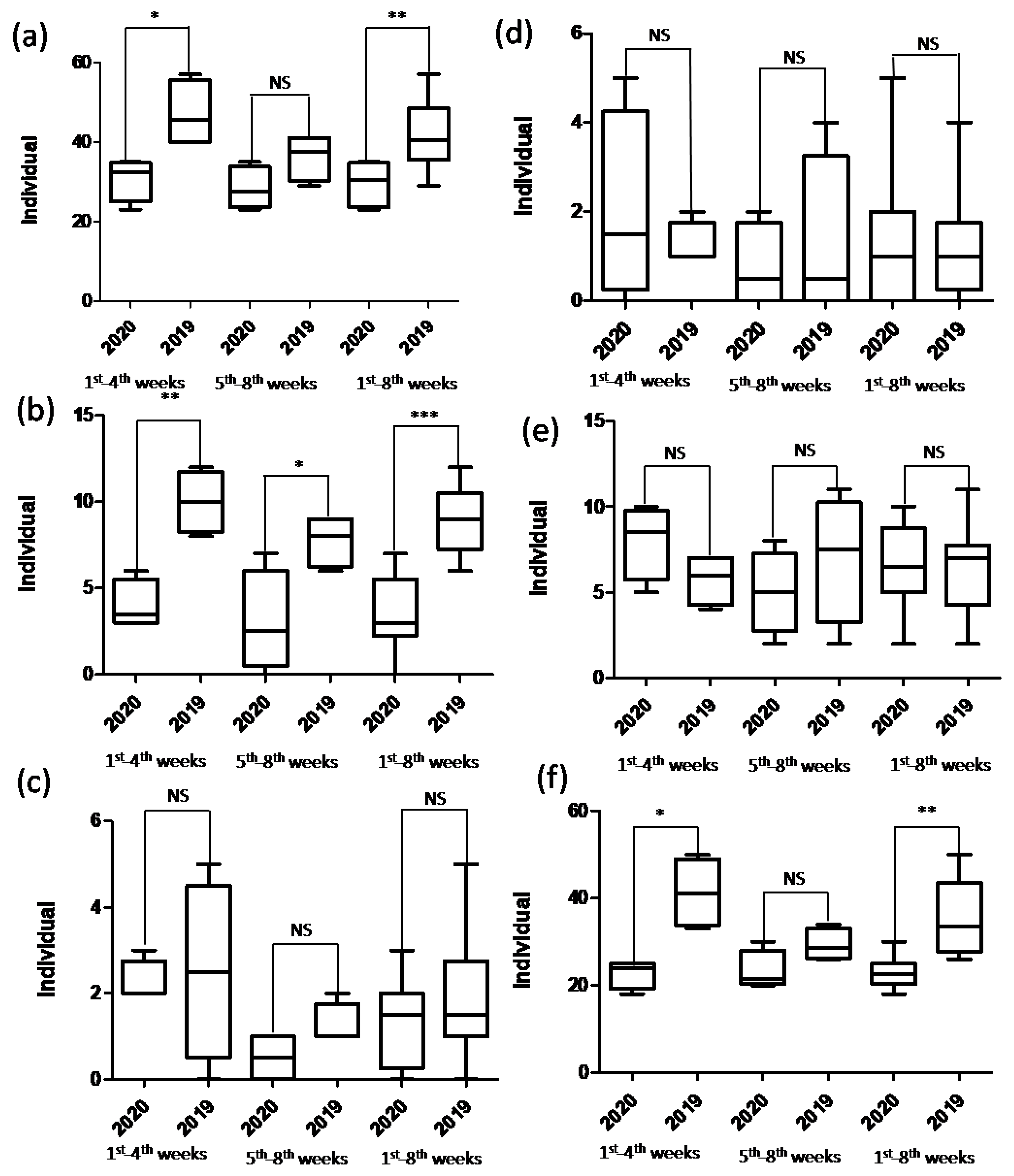
3.1.1. The Community Hospital
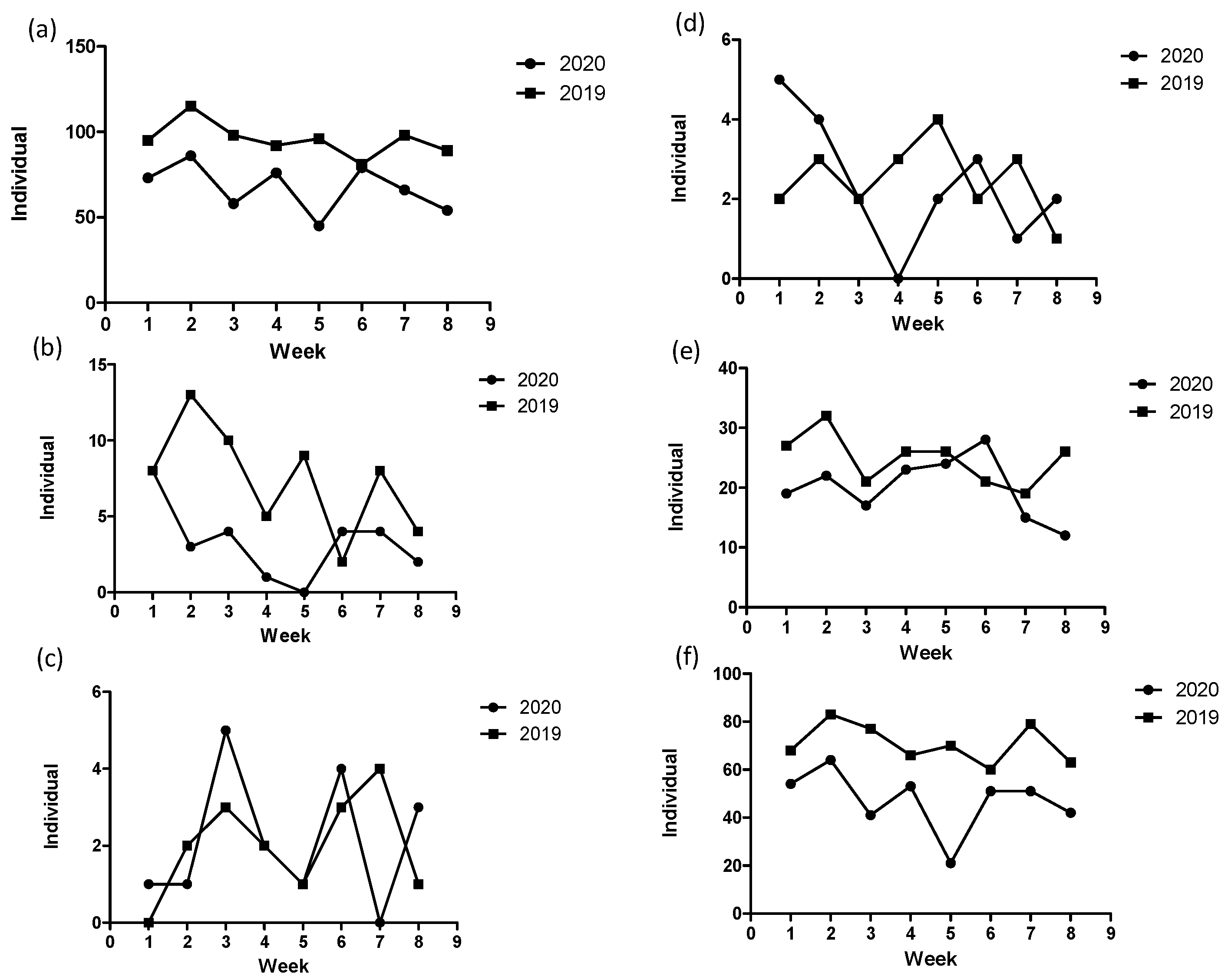
3.1.2. The University Hospital
3.2. TKA
3.2.1. The Community Hospital
3.2.2. The University Hospital
3.3. THA
3.3.1. The Community Hospital
3.3.2. The University Hospital
3.4. Hemiarthroplasty
3.4.1. The Community Hospital
3.4.2. The University Hospital
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biol. Med. 2020, 91, 157–160. [Google Scholar]
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. Available online: https://arcg.is/0fHmTX (accessed on 5 September 2021).
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef] [PubMed]
- Yen, M.-Y.; Schwartz, J.; Chen, S.-Y.; King, C.-C.; Yang, G.-Y.; Hsueh, P.-R. Interrupting COVID-19 transmission by implementing enhanced traffic control bundling: Implications for global prevention and control efforts. J. Microbiol. Immunol. Infect. 2020, 53, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Centers for Disease Control. CECC Confirms 4 More Imported COVID-19 Cases. Cases Arrive in Taiwan from Indonesia and the Philippines. Available online: https://www.cdc.gov.tw/En/Bulletin/Detail/0hKFLWF095r8WTnDDLgWfg?typeid=158 (accessed on 15 December 2020).
- Su, V.Y.-F.; Yen, Y.-F.; Yang, K.-Y.; Su, W.-J.; Chou, K.-T.; Chen, Y.-M.; Perng, D.-W. Masks and medical care: Two keys to Taiwan’s success in preventing COVID-19 spread. Travel. Med. Infect. Dis. 2020, 38, 101780. [Google Scholar]
- Hsu, C.-H.; Chen, C.-H.; Huang, H.-T.; Yang, C.-J.; Chen, Y.-H. To safely reopen after a lockdown, masks are crucial: Lessons from Taiwan. Public Health 2021, 190, 99–100. [Google Scholar] [CrossRef]
- Lee, I.-K.; Wang, C.-C.; Lin, M.-C.; Kung, C.-T.; Lan, K.-C.; Lee, C.-T. Effective strategies to prevent coronavirus disease-2019 (COVID-19) outbreak in hospital. J. Hosp. Infect. 2020, 105, 102–103. [Google Scholar] [CrossRef] [Green Version]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Gaido, L.; et al. Reduced rate of hospital admissions for ACS during Covid-19 outbreak in Northern Italy. N. Eng. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef]
- Athey, A.G.; Cao, L.; Okazaki, K.; Zagra, L.; Castelli, C.C.; Kendoff, D.O.; Kerr, J.M.; Yates, A.J.; Stambough, J.B.; Sierra, R.J. Survey of AAHKS International Members on the Impact of COVID-19 on hip and knee arthroplasty practices. J. Arthroplast. 2020, 35, S89–S94. [Google Scholar] [CrossRef]
- Bedard, N.A.; Elkins, J.M.; Brown, T.S. Effect of COVID-19 on hip and knee arthroplasty surgical volume in the United States. J. Arthroplast. 2020, 35, S45–S48. [Google Scholar] [CrossRef]
- Brown, T.S.; Bedard, N.A.; Rojas, E.O.; Anthony, C.A.; Schwarzkopf, R.; Barnes, C.L.; Stambough, J.B.; Mears, S.C.; Edwards, P.K.; Nandi, S.; et al. The effect of the COVID-19 pandemic on electively scheduled hip and knee arthroplasty patients in the United States. J. Arthroplast. 2020, 35, S49–S55. [Google Scholar] [CrossRef]
- Park, C.; Sugand, K.; Nathwani, D.; Bhattacharya, R.; Sarraf, K.M. Impact of the COVID-19 pandemic on orthopedic trauma workload in a London level 1 trauma center: The “golden month”. Acta Orthop. 2020, 91, 556–561. [Google Scholar] [CrossRef]
- Phillips, M.R.; Chang, Y.; Zura, R.D.; Mehta, S.; Giannoudis, P.V.; Nolte, P.A.; Bhandari, M. Impact of COVID-19 on orthopaedic care: A call for nonoperative management. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20934276. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.S.H.; Cheung, K.M.C. Impact of COVID-19 on orthopaedic and trauma service: An epidemiological study. J. Bone Jt. Surg. 2020, 102, e80. [Google Scholar] [CrossRef] [PubMed]
- Ranuccio, F.; Tarducci, L.; Familiari, F.; Mastroianni, V.; Giuzio, E. Disruptive effect of COVID-19 on orthopaedic daily practice: A cross-sectional survey. J. Bone Jt. Surg. 2020, 102, e77. [Google Scholar] [CrossRef]
- Liebensteiner, M.C.; Khosravi, I.; Hirschmann, M.T.; Heuberer, P.R.; Thaler, M. Massive cutback in orthopaedic healthcare ser-vices due to the COVID-19 pandemic: An online survey of almost 1400 orthopaedic surgeons in Austria, Germany and Switzerland. Knee Surg. Sport Traumatol. Arthrosc. 2020, 28, 1705–1711. [Google Scholar] [CrossRef] [PubMed]
- Thaler, M.; Khosravi, I.; Hirschmann, M.T.; Kort, N.P.; Zagra, L.; Epinette, J.A.; Liebensteiner, M.C. Disruption of joint arthroplasty services in Europe during the COVID-19 pandemic: An online survey within the European Hip Society (EHS) and the European Knee Associates (EKA). Knee Surg. Sport Traumatol. Arthrosc. 2020, 28, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Vermeşan, D.; Todor, A.; Andrei, D.; Niculescu, M.; Tudorache, E.; Haragus, H. Effect of COVID-19 Pandemic on Orthopedic Surgery in Three Centers from Romania. Int. J. Environ. Res. Public Health 2021, 18, 2196. [Google Scholar] [CrossRef]
- Magro, F.; Perazzo, P.; Bottinelli, E.; Possenti, F.; Banfi, G. Managing a Tertiary Orthopedic Hospital during the COVID-19 Epidemic, Main Challenges and Solutions Adopted. Int. J. Environ. Res. Public Health 2020, 17, 4818. [Google Scholar] [CrossRef]
- Tarantino, U.; Cariati, I.; Tancredi, V.; Casamassima, D.; Piccirilli, E.; Iundusi, R.; Gasbarra, E. State of Fragility Fractures Management during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7732. [Google Scholar] [CrossRef]
- Aprato, A.; Guindani, N.; Massè, A.; Castelli, C.C.; Cipolla, A.; Antognazza, D.; Benazzo, F.; Bove, F.; Casiraghi, A.; Catani, F.; et al. Clinical Activities, Contaminations of Surgeons and Cooperation with Health Authorities in 14 Orthopedic Departments in North Italy during the Most Acute Phase of Covid-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5340. [Google Scholar] [CrossRef]
- Elran-Barak, R.; Mozeikov, M. One Month into the Reinforcement of Social Distancing due to the COVID-19 Outbreak: Subjective Health, Health Behaviors, and Loneliness among People with Chronic Medical Conditions. Int. J. Environ. Res. Public Health 2020, 17, 5403. [Google Scholar] [CrossRef]
- Ruzzini, L.; De Salvatore, S.; Lamberti, D.; Maglione, P.; Piergentili, I.; Crea, F.; Ossella, C.; Costici, P.F. COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department. Int. J. Environ. Res. Public Health 2021, 18, 6573. [Google Scholar] [CrossRef] [PubMed]
- Verdoni, F.; Ricci, M.; Di Grigoli, C.; Rossi, N.; Lombardo, M.D.M.; Curci, D.; Accetta, R.; Viganò, M.; Peretti, G.M.; Mangiavini, L. Effect of the COVID-19 Outbreak on Pediatric Patients’ Admissions to the Emergency Department in an Italian Orthopedic Trauma Hub. Children 2021, 8, 645. [Google Scholar] [CrossRef] [PubMed]
- Trisolino, G.; Toniolo, R.M.; Marengo, L.; Dibello, D.; Guida, P.; Panuccio, E.; Evangelista, A.; Stallone, S.; Sansò, M.L.; Amati, C.; et al. Resilience Against COVID-19: How Italy Faced the Pandemic in Pediatric Orthopedics and Traumatology. Children 2021, 8, 530. [Google Scholar] [CrossRef]
- Brayda-Bruno, M.; Giorgino, R.; Gallazzi, E.; Morelli, I.; Manfroni, F.; Briguglio, M.; Accetta, R.; Mangiavini, L.; Peretti, G.M. How SARS-CoV-2 Pandemic Changed Traumatology and Hospital Setting: An Analysis of 498 Fractured Patients. J. Clin. Med. 2021, 10, 2585. [Google Scholar] [CrossRef]
- Agrawal, S.; Makuch, S.; Dróżdż, M.; Strzelec, B.; Sobieszczańska, M.; Mazur, G. The Impact of the COVID-19 Emergency on Life Activities and Delivery of Healthcare Services in the Elderly Population. J. Clin. Med. 2021, 10, 4089. [Google Scholar] [CrossRef] [PubMed]
- Pokryszko-Dragan, A.; Chojdak-Łukasiewicz, J.; Gruszka, E.; Pawłowski, M.; Pawłowski, T.; Rudkowska-Mytych, A.; Rymaszewska, J.; Budrewicz, S. Burden of COVID-19 Pandemic Perceived by Polish Patients with Multiple Sclerosis. J. Clin. Med. 2021, 10, 4215. [Google Scholar] [CrossRef] [PubMed]
- Polizzi, C.; Burgio, S.; Lavanco, G.; Alesi, M. Parental Distress and Perception of Children’s Executive Functioning after the First COVID-19 Lockdown in Italy. J. Clin. Med. 2021, 10, 4170. [Google Scholar] [CrossRef]
- Frade, F.; Jacobsohn, L.; Gómez-Salgado, J.; Martins, R.; Allande-Cussó, R.; Ruiz-Frutos, C.; Frade, J. Impact on the Mental and Physical Health of the Portuguese Population during the COVID-19 Confinement. J. Clin. Med. 2021, 10, 4464. [Google Scholar] [CrossRef] [PubMed]
- Lucki, M.; Wareńczak, A.; Chlebuś, E.; Daroszewski, P.; Lisiński, P. The ICF Classification as a Simple Tool to Aid in the Assessment of Healthcare Services in a Non-COVID-19 Hospital during the COVID-19 Pandemic. Healthcare 2021, 9, 398. [Google Scholar] [CrossRef]
- Polan, C.; Burggraf, M.; Kauther, M.D.; Meyer, H.-L.; Rademacher, F.; Braitsch, H.; Jöckel, K.-H.; Hardes, J.; Streitbürger, A.; Dudda, M. Development of Case Numbers during the COVID-19 Pandemic in a Center of Maximum-Care for Traumatology and Orthopedic Oncology. Healthcare 2021, 9, 3. [Google Scholar] [CrossRef]
- Placella, G.; Salvato, D.; Delmastro, E.; Bettinelli, G.; Salini, V. CoViD-19 and ortho and trauma surgery: The Italian experience. Injury 2020, 51, 1403–1405. [Google Scholar] [CrossRef] [PubMed]
- Ciatti, C.; Maniscalco, P.; Quattrini, F.; Gattoni, S.; Magro, A.; Capelli, P.; Banchini, F.; Fiazza, C.; Pavone, V.; Pagliarello, C.P.; et al. The epidemiology of proximal femur fractures during COVID-19 emergency in Italy: A multicentric study. Acta Biomed. 2021, 92, e2021398. [Google Scholar] [PubMed]
- Simon, S.; Frank, B.J.H.; Aichmair, A.; Manolopoulos, P.P.; Dominkus, M.; Schernhammer, E.S.; Hofstaetter, J.G. Impact of the 1st and 2nd Wave of the COVID-19 Pandemic on Primary or Revision Total Hip and Knee Arthroplasty—A Cross-Sectional Single Center Study. J. Clin. Med. 2021, 10, 1260. [Google Scholar] [CrossRef]
- Czubak-Wrzosek, M.; Czubak, J.; Grzelecki, D.; Tyrakowski, M. The Effect of the COVID-19 Pandemic on Total Hip and Knee Arthroplasty Surgical Volume in 2020 in Poland. Int. J. Environ. Res. Public Health 2021, 18, 8830. [Google Scholar] [CrossRef]
- Kazubski, K.; Tomczyk, Ł.; Kopczyński, B.; Morasiewicz, P. The Epidemiology of Hip and Knee Primary and Revision Arthroplasties during the COVID-19 Pandemic. Healthcare 2021, 9, 519. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, M.; Orlandini, L.; Meroni, V.; D’Errico, M.; Fontana, A.; Viganò, M.; Mangiavini, L.; D’Anchise, R.; Parente, F.; Pozzoni, R.; et al. Remote Management of Patients after Total Joint Arthroplasty via a Web-Based Registry during the COVID-19 Pandemic. Healthcare 2021, 9, 1296. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W. Enhanced Recovery after Surgery (ERAS) for Hip and Knee Replacement—Why and How It Should Be Implemented Following the COVID-19 Pandemic. Medicina 2021, 57, 81. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, P.D.; Villa, F.; Gallazzi, E.; Debernardi, A.; Schirò, G.R.; Crisà, F.M.; Talamonti, G.; D’Aliberti, G. The management of emergency spinal surgery during the COVID-19 pandemic in Italy. Bone Jt. J. 2020, 102-B, 671–676. [Google Scholar] [CrossRef]
- Nuñez, J.H.; Sallent, A.; Lakhani, K.; Guerra-Farfan, E.; Vidal, N.; Ekhtiari, S.; Minguell, J. Impact of the COVID-19 pandemic on an emergency traumatology service: Experience at a tertiary Trauma Centre in Spain. Injury 2020, 51, 1414–1418. [Google Scholar] [CrossRef]
- Schwartz, J.; King, C.-C.; Yen, M.-Y. Protecting healthcare workers during the coronavirus disease 2019 (COVID-19) outbreak: Lessons from Taiwan’s severe acute respiratory syndrome response. Clin. Infect. Dis. 2020, 71, 858–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Georgeo, M.R.; De Georgeo, J.M.; Egan, T.M.; Klee, K.P.; Schwemm, M.S.; Bye-Kollbaum, H.; Kinser, A.J. Containing SARS-CoV-2 in hospitals facing finite PPE, limited testing, and physical space variability: Navigating resource constrained enhanced traffic control bundling. J. Microbiol. Immunol. Infect. 2021, 54, 4–11. [Google Scholar] [CrossRef]
- Yen, M.-Y.; Schwartz, J.; King, C.-C.; Lee, C.-M.; Hsueh, P.-R. Society of Taiwan Long-term Care Infection Prevention and Control. Recommendations for protecting against and mitigating the COVID-19 pandemic in long-term care facilities. J. Microbiol. Immunol. Infect. 2020, 53, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic transmission, the Achilles’ heel of current strategies to control Covid-19. N. Eng. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N. Eng. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.-L.; Huang, P.-J.; Huang, H.-T.; Chen, C.-H.; Lee, T.-C.; Hsu, C.-H. Impact of the COVID-19 pandemic and its related psychological effect on orthopedic surgeries conducted in different types of hospitals in Taiwan. J. Orthop. Surg. 2021, 29, 1–8. [Google Scholar] [CrossRef]
- Lei, S.; Jiang, F.; Su, W.; Chen, C.; Chen, J.; Mei, W.; Zhan, L.-Y.; Jia, Y.; Zhang, L.; Liu, D.; et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalmedicine 2020, 21, 100331. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2020 | 2019 | 2020 | 2019 | 2020 | 2019 | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1–4 Weeks | p-Value | 5–8 Weeks | p-Value | 1–8 Weeks | p-Value | ||||
| All types of surgery | |||||||||
| Age | 59.5 ± 18.0 | 62.1 ± 17.2 | 0.200 | 56.9 ± 18.6 | 61.5 ± 18.4 | 0.048 * | 58.3 ± 18.3 | 61.8 ± 17.7 | 0.019 * |
| Sex (F/M) | 118/70 | 79/44 | 0.794 | 73/40 | 97/48 | 0.700 | 152/84 | 215/118 | 0.969 |
| Total knee arthroplasty | |||||||||
| Age | 70.1 ± 7.1 | 72.5 ± 6.8 | 0.245 | 70.3 ± 6.2 | 74.0 ± 5.9 | 0.080 | 70.2 ± 6.6 | 73.1 ± 6.4 | 0.044 * |
| Sex (F/M) | 13/3 | 32/8 | 0.915 | 9/3 | 26/5 | 0.503 | 22/6 | 58/13 | 0.723 |
| Total hip arthroplasty | |||||||||
| Age | 61.9 ± 14.3 | 62.3 ± 7.9 | 0.938 | 56.5 ± 3.5 | 53.8 ± 12.0 | 0.778 | 60.9 ± 13.0 | 59.5 ± 9.9 | 0.751 |
| Sex (F/M) | 6/3 | 4/6 | 0.245 | 2/0 | 4/1 | 0.495 | 8/3 | 8/7 | 0.315 |
| Hemiarthroplasty | |||||||||
| Age | 79.6 ± 8.6 | 77.0 ± 11.1 | 0.640 | 72.3 ± 12.4 | 78.2 ± 5.3 | 0.347 | 77.6 ± 9.7 | 77.6 ± 8.2 | 0.993 |
| Sex (F/M) | 5/3 | 4/1 | 0.506 | 2/1 | 1/4 | 0.187 | 7/4 | 5/5 | 0.528 |
| Emergency surgery | |||||||||
| Age | 60.1 ± 17.5 | 56.7 ± 23.0 | 0.540 | 54.5 ± 22.5 | 57.6 ± 19.0 | 0.597 | 57.9 ± 19.6 | 57.2 ± 20.6 | 0.863 |
| Sex (F/M) | 17/15 | 15/8 | 0.370 | 13/7 | 16/12 | 0.583 | 30/22 | 31/20 | 0.750 |
| Elective surgery | |||||||||
| Age | 59.2 ± 18.1 | 62.8 ± 16.2 | 0.107 | 57.5 ± 17.7 | 62.5 ± 18.2 | 0.047 * | 58.3 ± 17.9 | 62.7 ± 17.0 | 0.009 ** |
| Sex (F/M) | 62/29 | 103/62 | 0.361 | 60/33 | 81/39 | 0.470 | 122/62 | 184/98 | 0.814 |
| 2020 | 2019 | 2020 | 2019 | 2020 | 2019 | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1–4 Weeks | p-Value | 5–8 Weeks | p-Value | 1–8 Weeks | p-Value | ||||
| All types of surgery | |||||||||
| Age | 49.2 ± 21.3 | 53.0 ± 20.5 | 0.017 * | 50.8 ± 20.6 | 52.2 ± 20.3 | 0.382 | 49.9 ± 21.0 | 52.6 ± 20.4 | 0.018 * |
| Sex (F/M) | 152/141 | 229/170 | 0.245 | 127/117 | 164/200 | 0.091 | 279/258 | 393/370 | 0.695 |
| Total knee arthroplasty | |||||||||
| Age | 70.1 ± 6.2 | 70.2 ± 8.8 | 0.968 | 73.4 ± 7.6 | 72.4 ± 7.4 | 0.734 | 71.4 ± 6.8 | 71.1 ± 8.3 | 0.872 |
| Sex (F/M) | 13/3 | 28/8 | 0.777 | 7/3 | 16/7 | 0.980 | 20/6 | 44/15 | 0.817 |
| Total hip arthroplasty | |||||||||
| Age | 60.6 ± 20.3 | 53.3 ± 15.6 | 0.448 | 68.1 ± 9.6 | 61.2 ± 19.2 | 0.373 | 64.1 ± 16.2 | 57.8 ± 17.6 | 0.288 |
| Sex (F/M) | 7/2 | 3/4 | 0.152 | 7/1 | 5/4 | 0.149 | 14/3 | 8/8 | 0.049 * |
| Hemiarthroplasty | |||||||||
| Age | 77.3 ± 6.5 | 80.5 ± 11.6 | 0.457 | 77.4 ± 9.7 | 76.8 ± 9.0 | 0.898 | 77.8 ± 7.9 | 78.7 ± 10.3 | 0.786 |
| Sex (F/M) | 7/3 | 5/5 | 0.361 | 5/3 | 8/2 | 0.410 | 13/6 | 13/7 | 0.821 |
| Emergency surgery | |||||||||
| Age | 48.5 ± 23.3 | 55.6 ± 21.6 | 0.034 * | 48.6 ± 21.2 | 49.4 ± 23.8 | 0.811 | 48.5 ± 22.2 | 52.7 ± 22.8 | 0.084 |
| Sex (F/M) | 41/40 | 57/48 | 0.602 | 32/47 | 36/56 | 0.855 | 73/87 | 93/104 | 0.638 |
| Elective surgery | |||||||||
| Age | 49.4 ± 20.6 | 52.1 ± 20.0 | 0.146 | 51.8 ± 20.3 | 53.2 ± 18.9 | 0.470 | 50.5 ± 20.5 | 52.6 ± 19.5 | 0.104 |
| Sex (F/M) | 111/101 | 172/122 | 0.17 | 95/70 | 128/144 | 0.033 | 206/171 | 300/266 | 0.621 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-H.; Hsu, N.-C. Impact and Strategies on Joint Surgery Centers without Lockdowns during the Peak of the COVID-19 Pandemic: A Multicenter Cross-Sectional Study. J. Clin. Med. 2021, 10, 5392. https://doi.org/10.3390/jcm10225392
Hsu C-H, Hsu N-C. Impact and Strategies on Joint Surgery Centers without Lockdowns during the Peak of the COVID-19 Pandemic: A Multicenter Cross-Sectional Study. Journal of Clinical Medicine. 2021; 10(22):5392. https://doi.org/10.3390/jcm10225392
Chicago/Turabian StyleHsu, Chia-Hao, and Nin-Chieh Hsu. 2021. "Impact and Strategies on Joint Surgery Centers without Lockdowns during the Peak of the COVID-19 Pandemic: A Multicenter Cross-Sectional Study" Journal of Clinical Medicine 10, no. 22: 5392. https://doi.org/10.3390/jcm10225392