
Neuropathology and Inflammatory Cell Characterization in 10 Autoptic COVID-19 Brains

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort and Clinical Information
2.2. Autopsy Procedures
2.3. Histological and Immunohistochemical Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
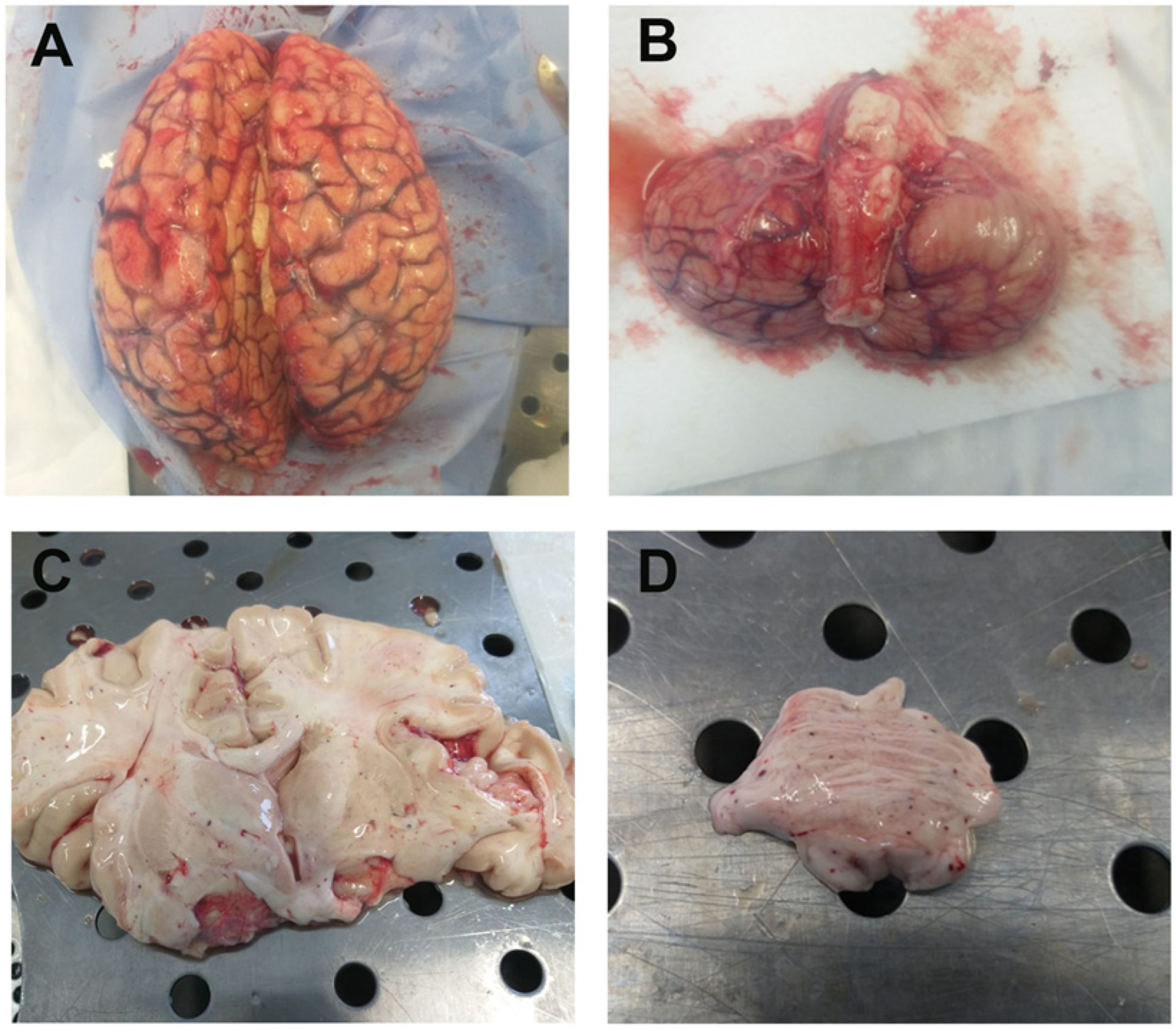
3.2. Autopsy Macroscopic Examination
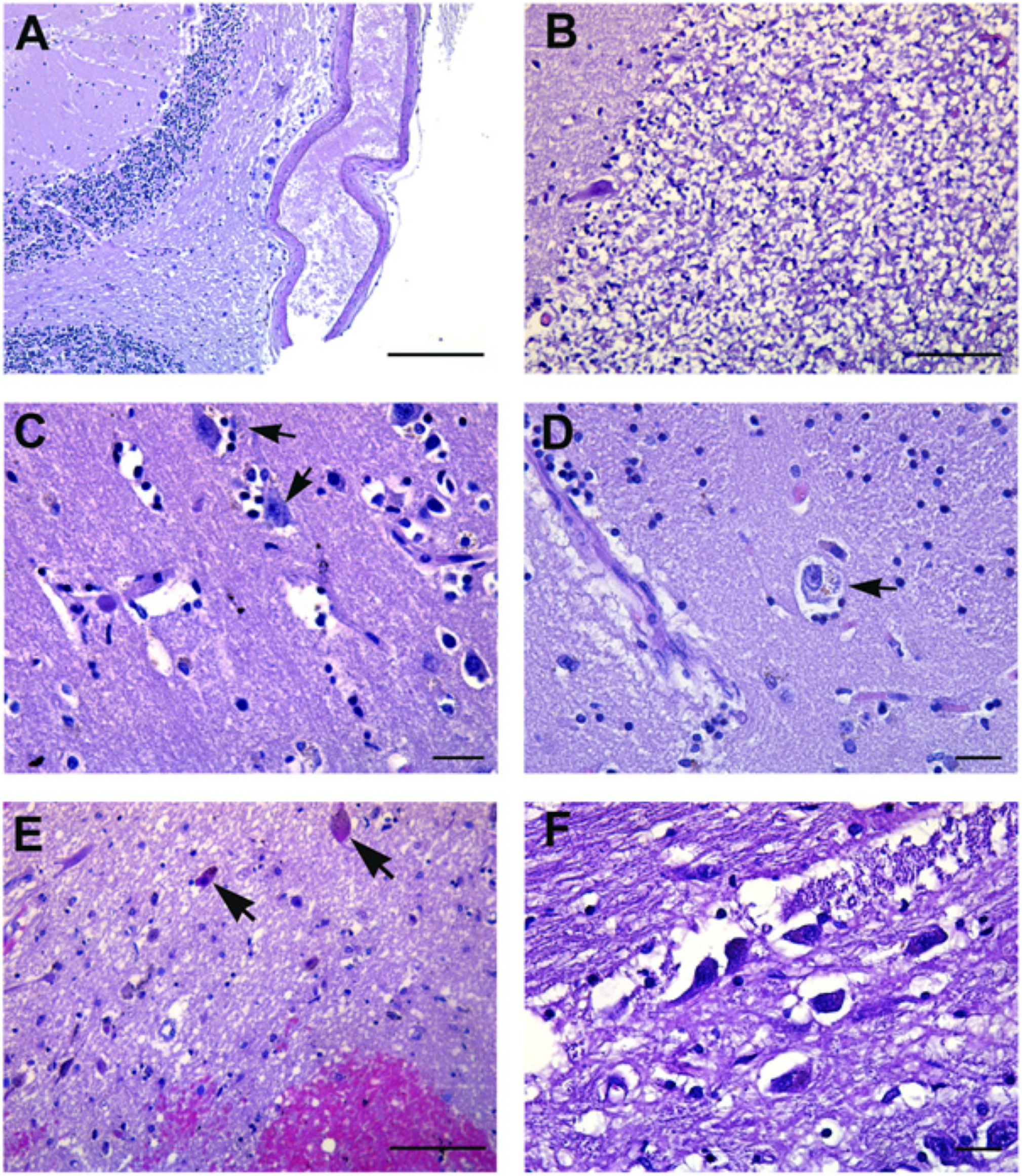
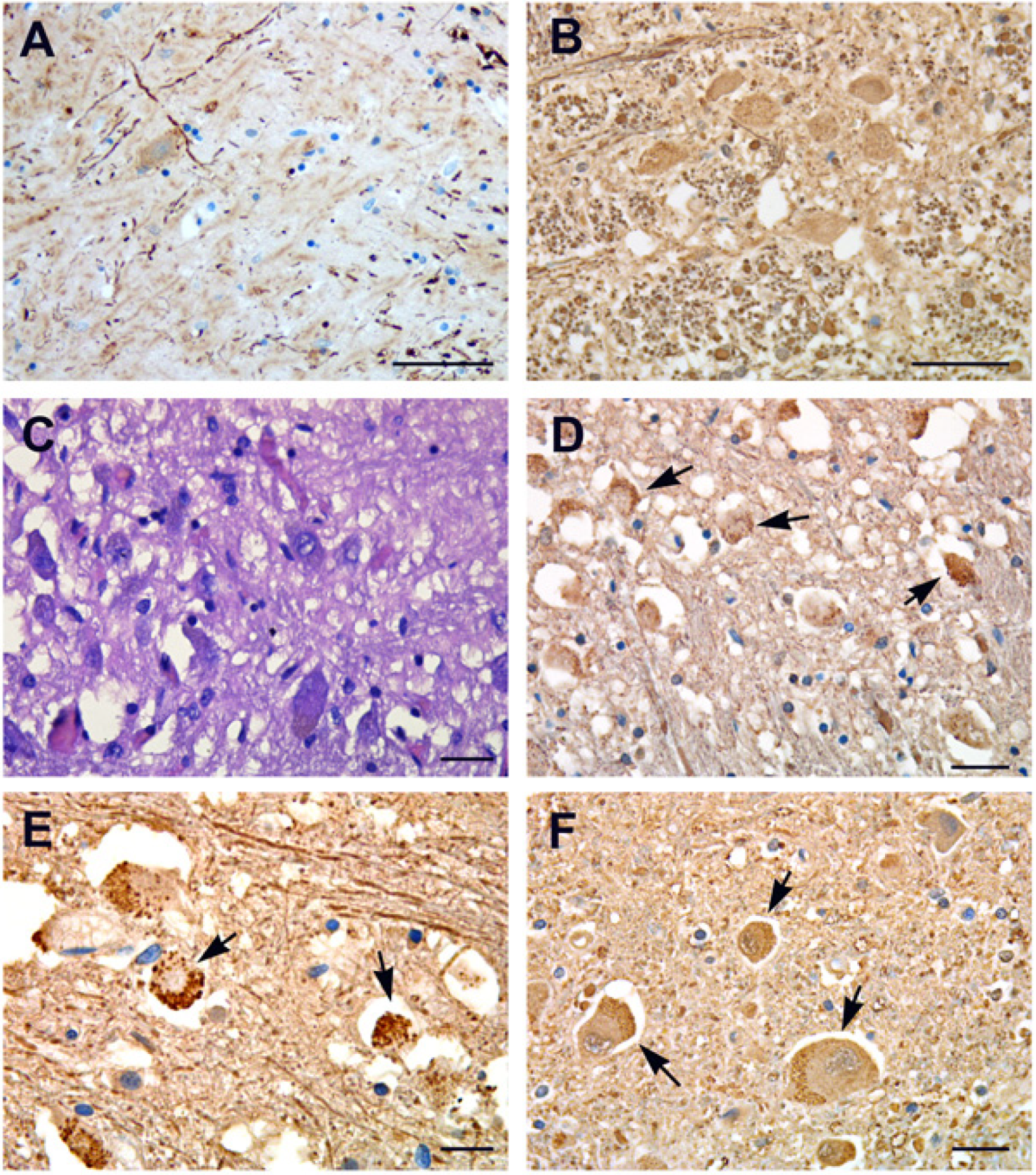
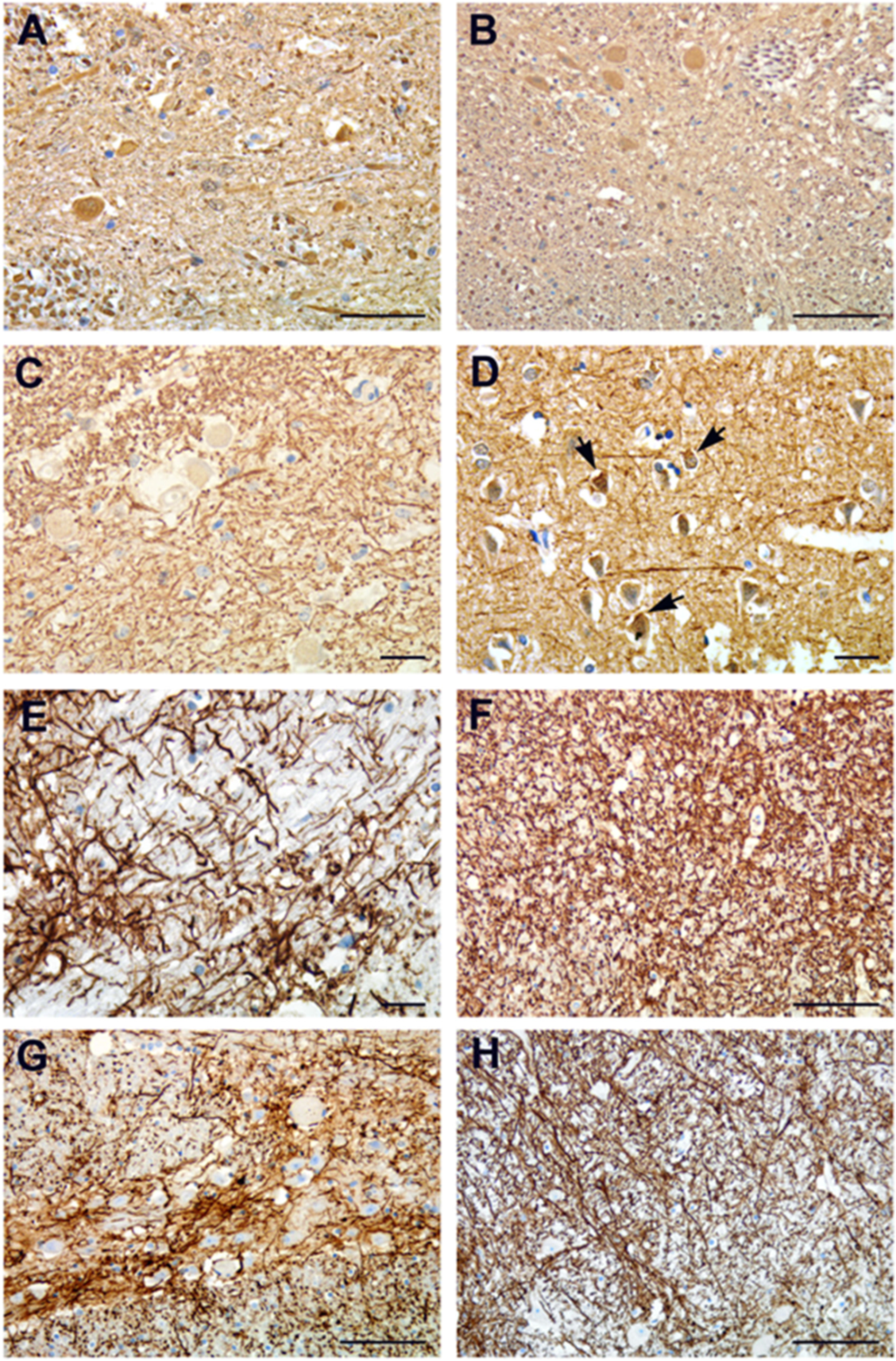
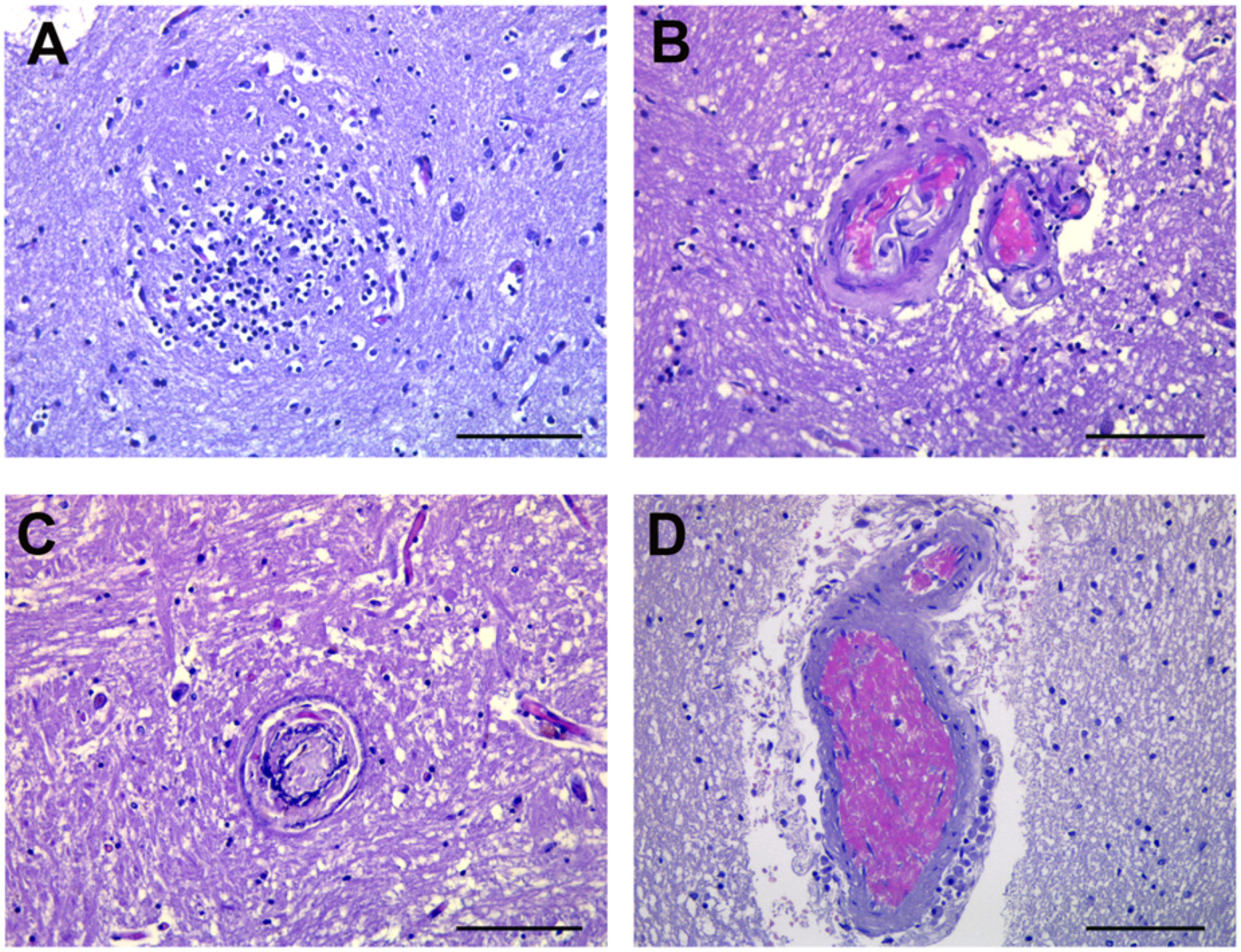
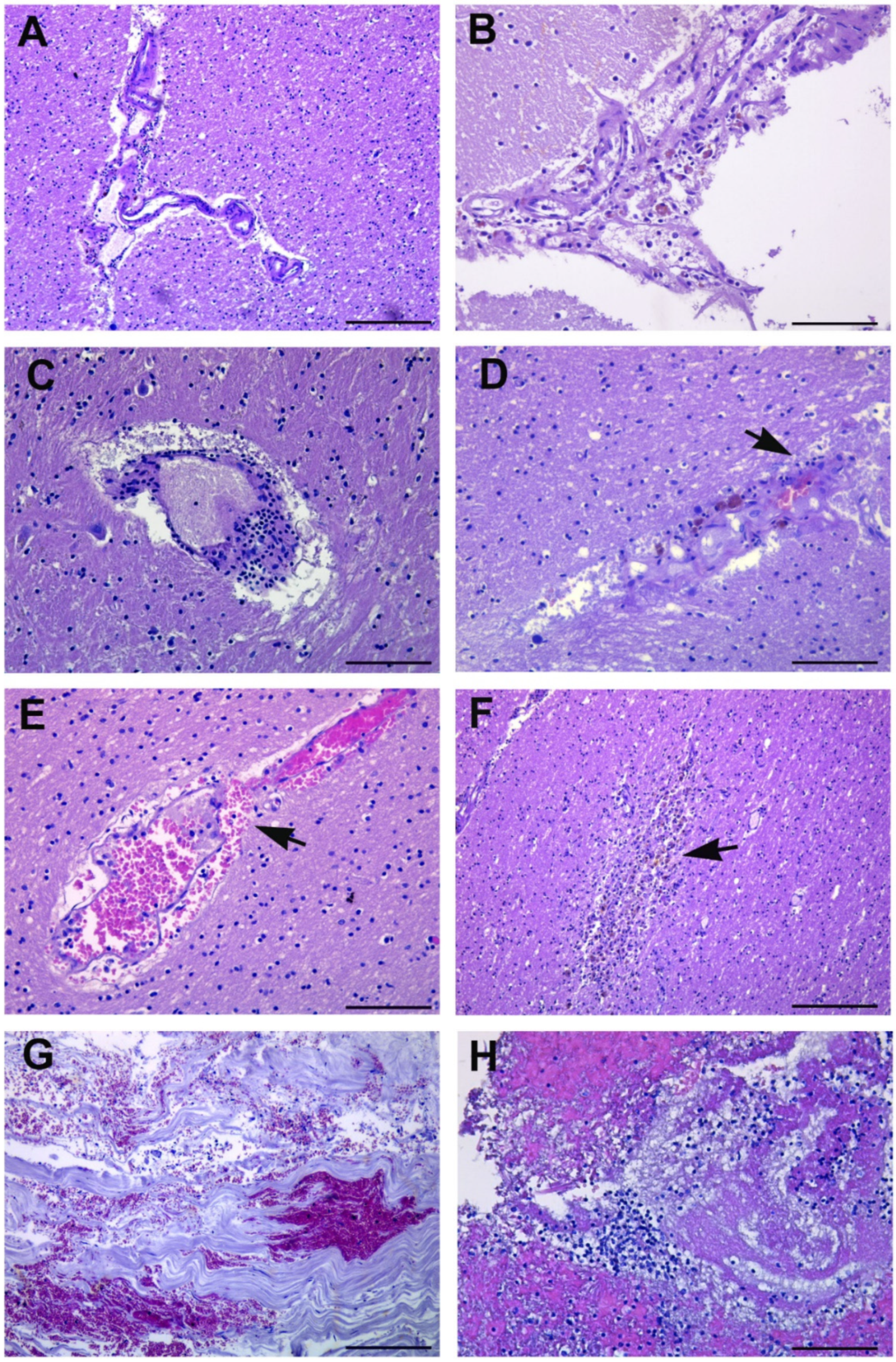
3.3. Microscopic Findings
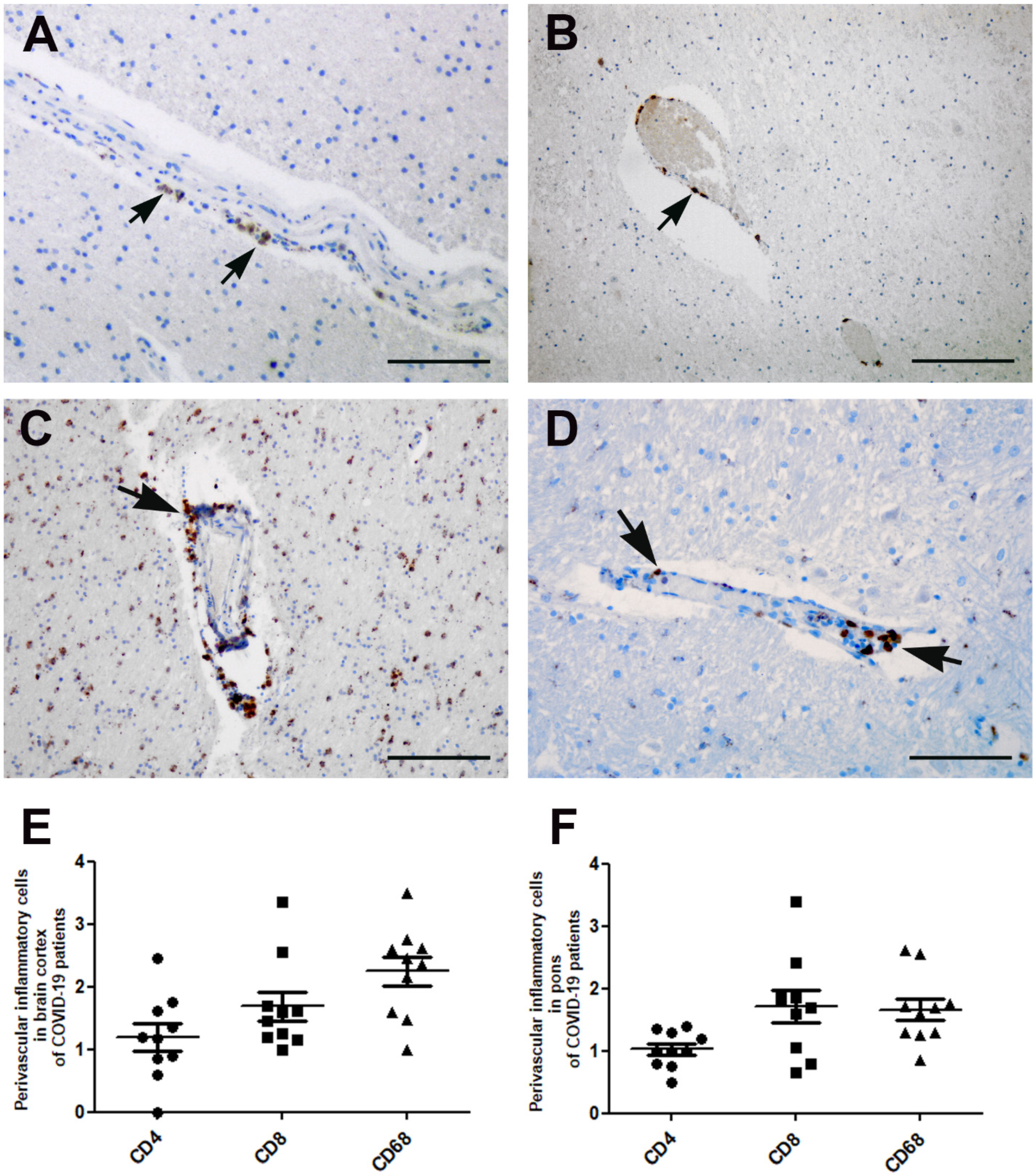
3.4. Perivascular Inflammation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Falasca, L.; Nardacci, R.; Colombo, D.; Lalle, E.; Di Caro, A.; Nicastri, E.; Antinori, A.; Petrosillo, N.; Marchioni, L.; Biava, G.; et al. Post-Mortem Findings in Italian Patients with COVID-19—A Descriptive Full Autopsy Study of cases with and without co-morbidities. J. Infect. Dis. 2020, 222, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the Nervous System. Cell 2020, 183, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Polonim, T.E.; Carlos, A.F.; Cairani, M.; Cutaia, C.; Medici, V.; Marelli, E.; Ferrari, D.; Galli, A.; Bognetti, P.; Davin, A.; et al. Prevalence and prognostic value of delirium as the initial presentation of COVID-19 in the elderly with dementia: An Italian retrospective study. EClinicalMedicine 2020, 26, 100490. [Google Scholar] [CrossRef] [PubMed]
- Ellul, M.A.; Benjamin, L.; Singh, B.; Lant, S.; Michael, B.D.; Easton, A.; Kneen, R.; Defres, S.; Sejvar, J.; Solomon, T. Neurological associations of COVID-19. Lancet Neurol. 2020, 19, 767–783. [Google Scholar] [CrossRef]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F., Jr.; Sabeti, P.; et al. Neuropathological Features of COVID-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef]
- Schurink, B.; Roos, E.; Radonic, T.; Barbe, E.; Bouman, C.S.C.; de Boer, H.H.; de Bree, G.J.; Bulle, E.B.; Aronica, E.M.; Florquin, S.; et al. Viral presence and immunopathology in patients with lethal COVID-19: A prospective autopsy cohort study. Lancet Microbe 2020, 1, e290–e299. [Google Scholar] [CrossRef]
- Kantonen, J.; Mahzabin, S.; Mäyränpää, M.I.; Tynninen, O.; Paetau, A.; Andersson, N.; Sajantila, A.; Vapalahti, O.; Carpén, O.; Kekäläinen, E.; et al. Neuropathologic features of four autopsied COVID-19 patients. Brain Pathol. 2020, 30, 1012–1016. [Google Scholar] [CrossRef]
- Mukerji, S.S.; Solomon, I.H. What can we learn from brain autopsies in COVID-19? Neurosci. Lett. 2021, 742, 135528. [Google Scholar] [CrossRef]
- Lee, M.H.; Perl, D.P.; Nair, G.; Li, W.; Maric, D.; Murray, H.; Dodd, S.J.; Koretsky, A.P.; Watts, J.A.; Cheung, V.; et al. Microvascular Injury in the Brains of Patients with COVID-19. N. Engl. J. Med. 2021, 384, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Schwabenland, M.; Salié, H.; Tanevski, J.; Killmer, S.; Lago, M.S.; Schlaak, A.E.; Mayer, L.; Matschke, J.; Püschel, K.; Fitzek, A.; et al. Deep spatial profiling of human COVID-19 brains reveals neuroinflammation with distinct microanatomical microglia-T-cell interactions. Immunity 2021, 54, 1594–1610.e11. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in suspected COVID-19 cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Weyhern, C.H.; Kaufmann, I.; Neff, F.; Kremer, M. Early evidence of pronounced cerebral cortex involvement in fatal COVID-19 outcomes. Lancet 2020, 395, e109. [Google Scholar] [CrossRef]
- Deigendesch, N.; Sironi, L.; Kutza, M.; Wischnewski, S.; Fuchs, V.; Hench, J.; Frank, A.; Nienhold, R.; Mertz, K.D.; Cathomas, G.; et al. Correlates of critical illness-related encephalopathy predominate postmortem COVID-19 neuropathology. Acta Neuropathol. 2020, 140, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Al-Sarraj, S.; Troakes, C.; Hanley, B.; Osborn, M.; Richardson, M.P.; Hotopf, M.; Bullmore, E.; Everall, I.P. Invited Review: The spectrum of neuropathology in COVID-19. Neuropathol. Appl. Neurobiol. 2021, 47, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Ellison, D.; Love, S. Neuropathology: A Reference Text of CNS Pathology, 2nd ed.; Mosby: St. Louis, MO, USA, 2004. [Google Scholar]
- Didonna, A.; Opal, P. The role of neurofilament aggregation in neurodegeneration: Lessons from rare inherited neurological disorders. Mol. Neurodegener. 2019, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Sciacca, S.; Lynch, J.; Davagnanam, I.; Barker, R. Midcerebral cortex, Pons, and Medulla: Anatomy and Syndromes. Radiographics 2019, 39, 1110–1125. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.v.; Zhao, Z.; Al Rasheed, M.; et al. Pathophysiology of SARS-CoV-2: Targeting of endothelial cells renders a complex disease with thrombotic microangiopathy and aberrant immune response. The Mount Sinai COVID-19 autopsy experience. medRXix 2020. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° | Age/Sex | Comorbidities | Neurological History | Neurological Symptoms at Admission | Neurological Symptoms During Hospitalization | Oxygenation/Intensive Care | Post-Mortem Gross Findings | Hospital Stay (Days) |
|---|---|---|---|---|---|---|---|---|
| 1 | 90/F | IC; CKD;AF; partially-sighted | Lewy bodies dementia | Disoriented | Increasing somnolence | Oxygen nasal goggles | Left pneumonia; endocarditis; myocardial infarction | 33 |
| 2 | 85/M | COPD | Dementia | Somnolence | Loss of consciousness | Oxygen therapy with VMK 50% | Chronic ischemic cardiopathy; heart failure; left pneumonia | 16 |
| 3 | 70/F | Type II DM; hypertensive cardiopathy. | Bipolar disorder; pontine lesion | Somnolence | Balance deficit/cognitive impairment/nonresponsive to verbal stimuli. | Oxygen therapy with VMK 60% | Bilateral interstitial pneumonia; pleural and pericardial effusion; hypovolemic shock | 72 |
| 4 | 60/M | Hypertension | None | None | None | cPAP/O2 therapy with VMK alternate; tracheostomy | Bilateral interstitial pneumonia; cardiogenic shock | 33 |
| 5 | 57/M | Hypertension; DM;COPD | None | None | None | VMK; orotracheal intubation; tracheostomy | Bilateral interstitial pneumonia; acute pneumonia; heart failure; | 14 + 27 |
| 6 | 68/M | Hypertension; cardiopathy; metabolic syndrome; autoimmune hypotiroidism; psoriatic arthritis | None | None | None | NIV; orotracheal intubation; ECMO | Bilateral interstitial pneumonia; acute pneumonia. | 41 |
| 7 | 66/M | None | None | Somnolence Disoriented | diffuse brain deficiency/seizures/Coma | NIV; orotracheal intubation | DIC; hemorrhage of right atrium, endocardium, coronary sinus area | 11 |
| 8 | 63/M | Hypertension; cerebral ischemic vasculopathy | Transient ischemic attack | Anosmia | Coma | Oxygen therapy with VMK 40%; orotracheal intubation | Interstitial pneumonia, DAD | 5 |
| 9 | 38/M | Obesity (BMI 43) | None | None | None | Ventimask orotracheal intubation; VMK | Myocarditis; interstitial pneumonia, broncopneumonia | 36 |
| 10 | 44/M | Sudden Death | None | None | None | No therapy | Myocarditis, pulmonary edema, demyelination of the pons and the medulla oblungata | Sudden death |
| Patient Number | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Cerebral meninges alterations | Hyperhemic Leptomeninges Sub-dural hematoma | Hyperhemic Leptomeninges | Hyperhemic Leptomeninges | Hyperhemic Leptomeninges | Hyperhemic Leptomeninges | Hyperhemic Leptomeninges Sub-dural hematoma | Hyperhemic Leptomeninges | Hyperhemic Leptomeninges | Hyperhemic Leptomeninges | |
| Cerebellum | Right lobe hemorragia | Right lobe hemorragia | ||||||||
| Hemorrhagic petechias | Right frontal lobe and basal nuclei | Pontine region | Basal nuclei | Basal nuclei | ||||||
| Other Changes | Hydrocephalus ex vacuo Multiple choroid plexus cysts | Hydrocephalus ex vacuo | Cerebral hemorrhage of right thalamic and pontine region | Cerebral edema | Cerebral infarction with hemorrhagic lesion of right occipito-parietal lobes with mesencephalic hemorrhage | |||||
| PATIENT | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| CEREBRAL CORTEX | Perivascular Inflammation | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ |
| Meningeal Hemorrhage | ++ | ++ | ++ | + | + | ++ | ++ | ++ | - | - | |
| Parenchymal Hemorrhage | ++ | + | ++ | ++ | ++ | ++ | ++ | - | - | ++ | |
| Vascular Hyaline Wall and Mineral deposits | ++ | ++ | ++ (focal) | ++ | ++ (focal) | ++ | ++ | - | ++ | - | |
| Neuron Damage | ++ | ++ | ++ | ++ | ++ | - | ++ | ++ | ++ | - | |
| Neuronophagia | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | - | |
| Infarction | - | ++ | - | - | - | ++ | ++ | ++ (focal ischemic change) | ++ (hemorragic) | - | |
| Other Changes | Lewy bodies Arach-id cysts Ferrugi-us neurons | Pituitary fibrosclerosis | Basal ganglia and thalamus hemorragic necrosis | Acute inflammation neutrophil dominance | Dense meshwork of glial fibers | Pseudolaminar necrosis | |||||
| CEREBELLUM | Perivascular Inflammation | Colliquative degeneration | ++ | ++ | ++ | ++ | Colliquative degeneration | ++ | + | ++ | ++ |
| Parenchymal Hemorrhage | Colliquative degeneration | - | ++ | - | - | Colliquative degeneration | ++ | - | ++ | - | |
| Loss Purkinjie Cells | Colliquative degeneration | ++ | ++ | ++ | ++ | Colliquative degeneration | ++ | - | ++ (Pyknosis, red neurons) | ++ (focal) | |
| Loss Granular Layer Neurons | Colliquative degeneration | - | ++ | ++ | ++ | Colliquative degeneration | ++ | - | ++ | - | |
| PONS | Perivascular Inflammation | ++ | - | ++ | ++ | ++ | ++ | ++ | + | + | + |
| Meningeal Hemorrhage | - | - | - | - | - | ++ | - | - | - | ||
| Parenchymal Hemorrhage | ++ | - | ++ | - | ++ | ++ | ++ | ++ (focal) | + (perivascular) | ++ (focal) | |
| Vascular Changes Hyaline Wall | ++ | - | ++ | - | - | ++ | ++ | + | - | - | |
| Neuron Damage | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | |
| Neuron Damage (NF aggregation *) | ++ | - | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | |
| Neuronophagia | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ (glial nodules) | ++ | - | |
| Derangement of neuropil and axonal swelling | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | ++ | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo, D.; Falasca, L.; Marchioni, L.; Tammaro, A.; Adebanjo, G.A.R.; Ippolito, G.; Zumla, A.; Piacentini, M.; Nardacci, R.; Del Nonno, F. Neuropathology and Inflammatory Cell Characterization in 10 Autoptic COVID-19 Brains. Cells 2021, 10, 2262. https://doi.org/10.3390/cells10092262
Colombo D, Falasca L, Marchioni L, Tammaro A, Adebanjo GAR, Ippolito G, Zumla A, Piacentini M, Nardacci R, Del Nonno F. Neuropathology and Inflammatory Cell Characterization in 10 Autoptic COVID-19 Brains. Cells. 2021; 10(9):2262. https://doi.org/10.3390/cells10092262
Chicago/Turabian StyleColombo, Daniele, Laura Falasca, Luisa Marchioni, Antonella Tammaro, Ganiyat Adenike Ralitsa Adebanjo, Giuseppe Ippolito, Alimuddin Zumla, Mauro Piacentini, Roberta Nardacci, and Franca Del Nonno. 2021. "Neuropathology and Inflammatory Cell Characterization in 10 Autoptic COVID-19 Brains" Cells 10, no. 9: 2262. https://doi.org/10.3390/cells10092262