
Oral Antiseptics against SARS-CoV-2: A Literature Review

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Structure of SARS-CoV-2
3. Importance of the Transmission and Pathogenicity of SARS-CoV-2 in the Oral Cavity
4. Saliva as a Vector
5. Recommendation of the Use of Oral Antiseptics
6. Types of Oral Antiseptics against SARS-CoV-2
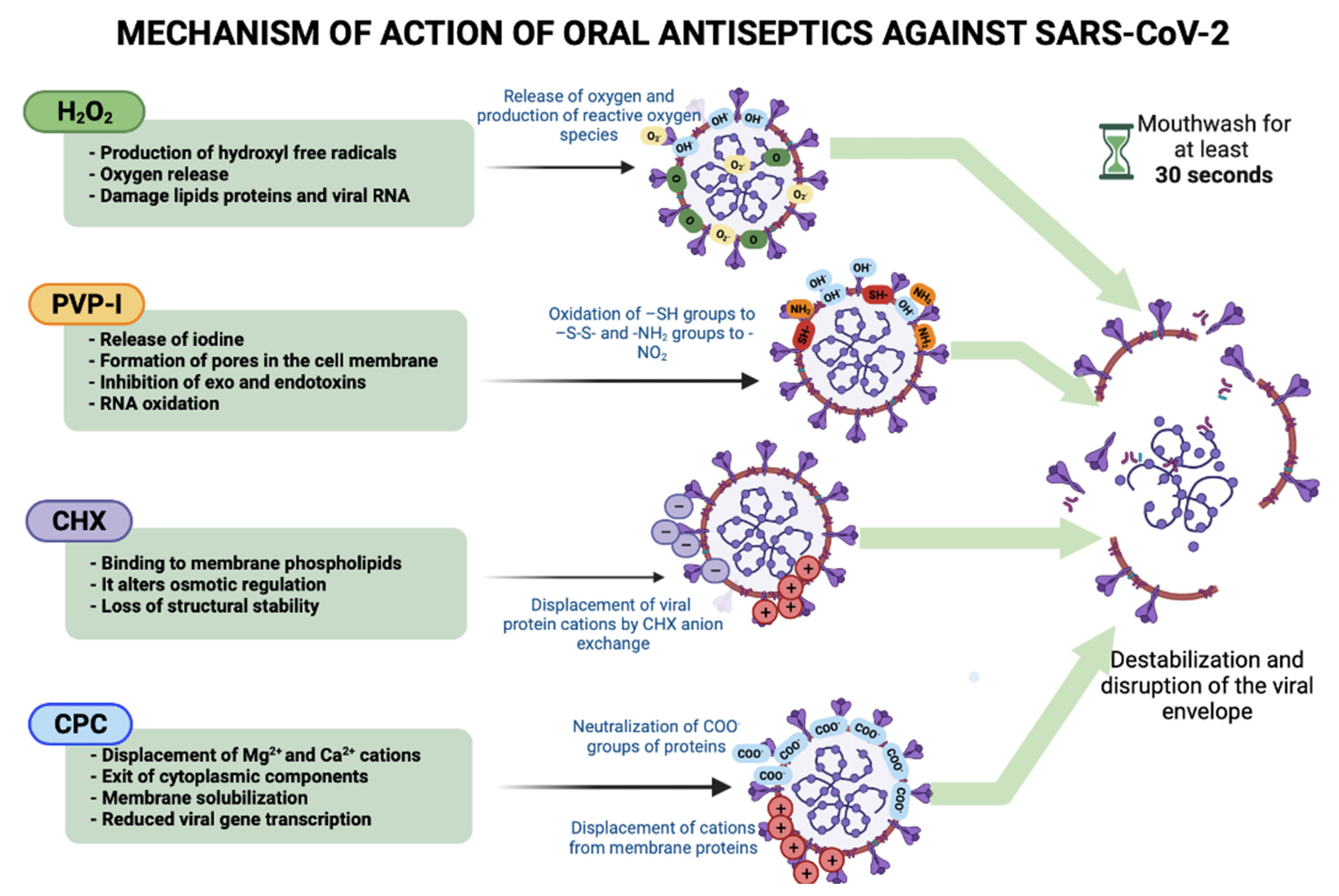
6.1. Hydrogen Peroxide (H2O2)
6.2. Chlorhexidine (CHX)
6.3. Povidone–Iodine (PVP-I)
6.4. Cetylpyridinium Chloride (CPC)
6.5. Bioflavonoids
6.6. Ethanol
6.7. Essential Oils
7. Real Virucidal Effect or Cytotoxic Effect of the Rinse?
8. Discussion
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://covid19.who.int (accessed on 23 June 2022).
- Xu, C.; Wang, A.; Hoskin, E.R.; Cugini, C.; Markowitz, K.; Chang, T.L.; Fine, D.H. Differential effects of antiseptic mouth rinses on SARS-CoV-2 infectivity in vitro. Pathogens 2021, 10, 272. [Google Scholar] [CrossRef] [PubMed]
- Gottsauner, M.J.; Michaelides, I.; Schmidt, B.; Scholz, K.J.; Buchalla, W.; Widbiller, M.; Hitzenbichler, F.; Ettl, T.; Reichert, T.E.; Bohr, C. A prospective clinical pilot study on the effects of a hydrogen peroxide mouthrinse on the intraoral viral load of SARS-CoV-2. Clin. Oral Investig. 2020, 24, 3707–3713. [Google Scholar] [CrossRef] [PubMed]
- Departamento del Trabajo de los EE. UU., Administración de Seguridad y Salud Ocupacional. Guía sobre la Preparación de los Lugares de Trabajo para el virus, COVID-19. 2020. Available online: https://www.osha.gov/Publications/OSHA3992.pdf (accessed on 23 June 2022).
- Testori, T.; Wang, H.-L.; Basso, M.; Bordini, G.; Dian, A.; Vitelli, C.; Miletić, I.; Del Fabbro, M. COVID-19 and Oral Surgery: A narrative review of preoperative mouth rinses. Acta Stomatol. Croat. 2020, 54, 431–441. [Google Scholar] [CrossRef]
- Robertson, C.; Clarkson, J.E.; Aceves-Martins, M.; Ramsay, C.R.; Richards, D.; Colloc, T.; Group, C.W. A Review of Aerosol Generation Mitigation in International Dental Guidance. Int. Dent. J. 2021, 72, 203–210. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Considerations for the Provision of Essential Oral Health Services in the Context of COVID-19: Interim Guidance, 3 August 2020; World Health Organization: Geneva, Switzerland, 2020; pp. 1–5. [Google Scholar]
- Chin, A.W.; Chu, J.T.; Perera, M.R.; Hui, K.P.; Yen, H.-L.; Chan, M.C.; Peiris, M.; Poon, L.L. Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Jiang, C.M.; Duangthip, D.; Auychai, P.; Chiba, M.; Folayan, M.O.; Hamama, H.H.H.; Kamnoedboon, P.; Lyons, K.; Matangkasombut, O.; Mathu-Muju, K.R. Changes in oral health policies and guidelines during the COVID-19 pandemic. Front. Oral Health 2021, 2, 1–14. [Google Scholar] [CrossRef]
- Elmahgoub, F.; Coll, Y. Could certain mouthwashes reduce transmissibility of COVID-19? Evid.-Based Dent. 2021, 22, 82–83. [Google Scholar] [CrossRef]
- Deana, N.F.; Seiffert, A.; Aravena-Rivas, Y.; Alonso-Coello, P.; Muñoz-Millán, P.; Espinoza-Espinoza, G.; Pineda, P.; Zaror, C. Recommendations for Safe Dental Care: A Systematic Review of Clinical Practice Guidelines in the First Year of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10059. [Google Scholar] [CrossRef]
- Ortega, K.; Rech, B.; El Haje, G.; Gallo, C.; Pérez-Sayáns, M.; Braz-Silva, P. Do hydrogen peroxide mouthwashes have a virucidal effect? A systematic review. J. Hosp. Infect. 2020, 106, 657–662. [Google Scholar] [CrossRef]
- Zhu, F.; Zhong, Y.; Ji, H.; Ge, R.; Guo, L.; Song, H.; Wu, H.; Jiao, P.; Li, S.; Wang, C. ACE2 and TMPRSS2 in human saliva can adsorb to the oral mucosal epithelium. J. Anat. 2022, 240, 398–409. [Google Scholar] [CrossRef]
- Peng, J.; Sun, J.; Zhao, J.; Deng, X.; Guo, F.; Chen, L. Age and gender differences in ACE2 and TMPRSS2 expressions in oral epithelial cells. J. Transl. Med. 2021, 19, 1–11. [Google Scholar] [CrossRef]
- Salas Orozco, M.F.; Niño-Martínez, N.; Martínez-Castañón, G.-A.; Patiño Marín, N.; Sámano Valencia, C.; Dipp Velázquez, F.A.; Sosa Munguía, P.d.C.; Casillas Santana, M.A. Presence of SARS-CoV-2 and Its Entry Factors in Oral Tissues and Cells: A Systematic Review. Medicina 2021, 57, 523. [Google Scholar] [CrossRef] [PubMed]
- Bidra, A.S.; Pelletier, J.S.; Westover, J.B.; Frank, S.; Brown, S.M.; Tessema, B. Rapid in-vitro inactivation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using povidone-iodine oral antiseptic rinse. J. Prosthodont. 2020, 29, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Serrano, J.; Roldán, S.; Sanz, M. Is the oral cavity relevant in SARS-CoV-2 pandemic? Clin. Oral Investig. 2020, 24, 2925–2930. [Google Scholar] [CrossRef] [PubMed]
- Carrouel, F.; Gonçalves, L.; Conte, M.; Campus, G.; Fisher, J.; Fraticelli, L.; Gadea-Deschamps, E.; Ottolenghi, L.; Bourgeois, D. Antiviral activity of reagents in mouth rinses against SARS-CoV-2. J. Dent. Res. 2021, 100, 124–132. [Google Scholar] [CrossRef]
- Bidra, A.S.; Pelletier, J.S.; Westover, J.B.; Frank, S.; Brown, S.M.; Tessema, B. Comparison of in vitro inactivation of SARS-CoV-2 with hydrogen peroxide and povidone-iodine oral antiseptic rinses. J. Prosthodont. 2020, 29, 599–603. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef]
- Meister, T.L.; Brüggemann, Y.; Todt, D.; Conzelmann, C.; Müller, J.A.; Groß, R.; Münch, J.; Krawczyk, A.; Steinmann, J.; Steinmann, J. Virucidal efficacy of different oral rinses against severe acute respiratory syndrome coronavirus 2. J. Infect. Dis. 2020, 222, 1289–1292. [Google Scholar] [CrossRef]
- Anderson, D.E.; Sivalingam, V.; Kang, A.E.Z.; Ananthanarayanan, A.; Arumugam, H.; Jenkins, T.M.; Hadjiat, Y.; Eggers, M. Povidone-iodine demonstrates rapid in vitro virucidal activity against SARS-CoV-2, the virus causing COVID-19 disease. Infect. Dis. Ther. 2020, 9, 669–675. [Google Scholar] [CrossRef]
- Jain, A.; Grover, V.; Singh, C.; Sharma, A.; Das, D.K.; Singh, P.; Thakur, K.G.; Ringe, R.P. Chlorhexidine: An effective anticovid mouth rinse. J. Indian Soc. Periodontol. 2021, 25, 86–88. [Google Scholar]
- Koch-Heier, J.; Hoffmann, H.; Schindler, M.; Lussi, A.; Planz, O. Inactivation of SARS-CoV-2 through Treatment with the Mouth Rinsing Solutions ViruProX® and BacterX® Pro. Microorganisms 2021, 9, 521. [Google Scholar] [CrossRef]
- Davies, K.; Buczkowski, H.; Welch, S.R.; Green, N.; Mawer, D.; Woodford, N.; Roberts, A.D.; Nixon, P.J.; Seymour, D.W.; Killip, M.J. Effective in vitro inactivation of SARS-CoV-2 by commercially available mouthwashes. J. Gen. Virol. 2021, 102, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Tiong, V.; Hassandarvish, P.; Bakar, S.A.; Mohamed, N.A.; Wan Sulaiman, W.S.; Baharom, N.; Abdul Samad, F.N.; Isahak, I. The effectiveness of various gargle formulations and salt water against SARS-CoV-2. Sci. Rep. 2021, 11, 20502. [Google Scholar] [CrossRef] [PubMed]
- Meyers, C.; Robison, R.; Milici, J.; Alam, S.; Quillen, D.; Goldenberg, D.; Kass, R. Lowering the transmission and spread of human coronavirus. J. Med. Virol. 2021, 93, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, J.S.; Tessema, B.; Frank, S.; Westover, J.B.; Brown, S.M.; Capriotti, J.A. Efficacy of povidone-iodine nasal and oral antiseptic preparations against severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2). Ear Nose Throat J. 2021, 100, 192S–196S. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Casanovas, H.J.; la Rosa, M.D.; Bello-Lemus, Y.; Rasperini, G.; Acosta-Hoyos, A.J. Virucidal Activity of Different Mouthwashes Using a Novel Biochemical Assay. Healthcare 2022, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.G.; Yoon, J.; Song, J.Y.; Yoon, S.-Y.; Lim, C.S.; Seong, H.; Noh, J.Y.; Cheong, H.J.; Kim, W.J. Clinical significance of a high SARS-CoV-2 viral load in the saliva. J. Korean Med. Sci. 2020, 35, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.M.; Parab, S.R.; Paranjape, M. Repurposing 0.5% povidone iodine solution in otorhinolaryngology practice in COVID 19 pandemic. Am. J. Otolaryngol. 2020, 41, 1–4. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Balan, P.; Ko, K.K.K.; Udawatte, N.S.; Lai, D.; Ng, D.H.L.; Venkatachalam, I.; Lim, K.S.; Ling, M.L.; Oon, L. Efficacy of commercial mouth-rinses on SARS-CoV-2 viral load in saliva: Randomized control trial in Singapore. Infection 2021, 49, 305–311. [Google Scholar] [CrossRef]
- Chaudhary, P.; Melkonyan, A.; Meethil, A.; Saraswat, S.; Hall, D.L.; Cottle, J.; Wenzel, M.; Ayouty, N.; Bense, S.; Casanova, F. Estimating salivary carriage of severe acute respiratory syndrome coronavirus 2 in nonsymptomatic people and efficacy of mouthrinse in reducing viral load: A randomized controlled trial. J. Am. Dent. Assoc. 2021, 152, 903–908. [Google Scholar] [CrossRef] [PubMed]
- De Paula Eduardo, F.; Corrêa, L.; Heller, D.; Daep, C.A.; Benitez, C.; Malheiros, Z.; Stewart, B.; Ryan, M.; Machado, C.M.; Hamerschlak, N. Salivary SARS-CoV-2 load reduction with mouthwash use: A randomized pilot clinical trial. Heliyon 2021, 7, e07346. [Google Scholar]
- Huang, Y.H.; Huang, J.T. Use of chlorhexidine to eradicate oropharyngeal SARS-CoV-2 in COVID-19 patients. J. Med. Virol. 2021, 93, 4370–4373. [Google Scholar] [CrossRef] [PubMed]
- Elzein, R.; Abdel-Sater, F.; Fakhreddine, S.; Abi Hanna, P.; Feghali, R.; Hamad, H.; Ayoub, F. In vivo evaluation of the virucidal efficacy of Chlorhexidine and Povidone-iodine mouthwashes against salivary SARS-CoV-2. A randomized-controlled clinical trial. J. Evid.-Based Dent. Pract. 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Bai, F.; Jonas, S.J.; Wirz, R.E. Cold atmospheric plasma for addressing the COVID-19 pandemic. Plasma Process. Polym. 2022, 1–13, e2200012. [Google Scholar] [CrossRef] [PubMed]
- Tadakamadla, J.; Boccalari, E.; Rathore, V.; Dolci, C.; Tartaglia, G.M.; Tadakamadla, S.K. In vitro studies evaluating the efficacy of mouth rinses on SARS-CoV-2: A systematic review. J. Infect. Public Health 2021, 14, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Sivaraman, K.; Radhakrishnan, R.; Balakrishnan, D.; Narayana, A. Can povidone iodine gargle/mouthrinse inactivate SARS-CoV-2 and decrease the risk of nosocomial and community transmission during the COVID-19 pandemic? An evidence-based update. Jpn. Dent. Sci. Rev. 2021, 57, 39–45. [Google Scholar] [CrossRef]
- Walsh, L.J. Safety issues relating to the use of hydrogen peroxide in dentistry. Aust. Dent. J. 2000, 45, 257–269. [Google Scholar] [CrossRef] [Green Version]
- Hossainian, N.; Slot, D.; Afennich, F.; Van der Weijden, G. The effects of hydrogen peroxide mouthwashes on the prevention of plaque and gingival inflammation: A systematic review. Int. J. Dent. Hyg. 2011, 9, 171–181. [Google Scholar] [CrossRef]
- Gilbert, P.; Moore, L.E. Cationic antiseptics: Diversity of action under a common epithet. J. Appl. Microbiol. 2005, 99, 703–715. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Nassani, M.Z.; Alaizari, N.; Kalakonda, B.; Al-Shamiri, H.M.; Alhajj, M.N.; Al-Soneidar, W.A.; Alahmary, A.W. Efficacy of aloe vera mouthwash versus chlorhexidine on plaque and gingivitis: A systematic review. Int. J. Dent. Hyg. 2020, 18, 44–51. [Google Scholar] [CrossRef]
- Del Río-Carbajo, L.; Vidal-Cortés, P. Tipos de antisépticos, presentaciones y normas de uso. Med. Intensiva 2019, 43, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Haydari, M.; Bardakci, A.G.; Koldsland, O.C.; Aass, A.M.; Sandvik, L.; Preus, H.R. Comparing the effect of 0.06%-, 0.12% and 0.2% Chlorhexidine on plaque, bleeding and side effects in an experimental gingivitis model: A parallel group, double masked randomized clinical trial. BMC Oral Health 2017, 17, 118. [Google Scholar] [CrossRef] [PubMed]
- Kamolnarumeth, K.; Thussananutiyakul, J.; Lertchwalitanon, P.; Rungtanakiat, P.; Mathurasai, W.; Sooampon, S.; Arunyanak, S.P. Effect of mixed chlorhexidine and hydrogen peroxide mouthrinses on developing plaque and stain in gingivitis patients: A randomized clinical trial. Clin. Oral Investig. 2021, 25, 1697–1704. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Miyake, M.; Hazama, A.; Omori, K. Povidone-iodine-induced cell death in cultured human epithelial HeLa cells and rat oral mucosal tissue. Drug Chem. Toxicol. 2014, 37, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, S.; Saha, A.; Jamir, L.; Kakkar, R. Protection at Portal of Entry (PPE) with Povidone Iodine for COVID-19. Int. J. Med. Public Health 2020, 10, 166–168. [Google Scholar] [CrossRef]
- Hooper, S.J.; Lewis, M.A.O.; Wilson, M.J.; Williams, D.W. Antimicrobial activity of Citrox® bioflavonoid preparations against oral microorganisms. Br. Dent. J. 2011, 210, 1–5. [Google Scholar] [CrossRef] [Green Version]
- González-Mas, M.C.; Rambla, J.L.; López-Gresa, M.P.; Blázquez, M.A.; Granell, A. Volatile compounds in citrus essential oils: A comprehensive review. Front. Plant Sci. 2019, 10, 1–18. [Google Scholar] [CrossRef]
- Sun, J. D-Limonene: Safety and clinical applications. Altern. Med. Rev. 2007, 12, 259. [Google Scholar]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Koarai, A.; Sugiura, H.; Yanagisawa, S.; Ichikawa, T.; Minakata, Y.; Matsunaga, K.; Hirano, T.; Akamatsu, K.; Ichinose, M. Oxidative stress enhances toll-like receptor 3 response to double-stranded RNA in airway epithelial cells. Am. J. Respir Cell Mol. Biol. 2010, 42, 651–660. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.A.; Del Prete, A.; Lazzarino, A.I.; Capaldi, R.; Grumetto, L. Might hydrogen peroxide reduce the hospitalization rate and complications of SARS-CoV-2 infection? Infect. Control Hosp. Epidemiol. 2020, 41, 1360–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komine, A.; Yamaguchi, E.; Okamoto, N.; Yamamoto, K. Virucidal activity of oral care products against SARS-CoV-2 in vitro. J. Oral Maxillofac. Surg. Med. Pathol. 2021, 33, 475–477. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Active Ingredients | Effect | Year | References |
|---|---|---|---|
| Povidone–iodine (PVP-I); hydrogen peroxide (H2O2) | After 15 and 30 s of contact, PVP-I at 0.5%, 1.25%, and 1.5% completely inactivated SARS-CoV-2. The solutions of H2O2 at 1.5% and 3.0% showed minimal virucidal activity. | 2020 | [19] |
| Hydrogen peroxide (H2O2); chlorhexidine digluconate; a solution with benzalkonium chloride, dequalinium chloride; 1.0% PVP-I solution; a mouthwash with ethanol and essential oils; a solution with octenidine dihydrochloride; polyaminopropylbiguanide solution. | All the active ingredients inactivated different strains of SARS-CoV-2. Particularly, the solution with benzalkonium chloride, dequalinium chloride, PVP-I solution, and mouthwash with ethanol and essential oils significantly reduced viral infectivity to undetectable levels. | 2020 | [21] |
| PVP-I 10% w/v solution; PVP-I 7.5% w/v solution; PVP-I 1.0% w/v solution and PVP-I 0.45% w/v solution. | All the PVP-I solutions inactivated SARS-CoV-2 by 99.99% at 30 s of exposure. | 2020 | [22] |
| PVP-I oral antiseptic solutions at concentrations of 0.5%, 1.0%, and 1.5%; ethanol at 70%. | The three concentrations of povidone–iodine completely inactivated SARS-CoV-2 in the first 15 s of contact. Ethanol at 70% inactivated the virus at 30 s of exposure. | 2020 | [16] |
| Chlorhexidine digluconate, 0.2% | Within 30 s of exposure, it inactivated 99.99% of SARS-CoV-2 and was even more effective than povidone–iodine. | 2021 | [23] |
| H2O2 solution; (alcohol and essential oils); povidone–iodine and chlorhexidine gluconate. | A 5% v/v dilution of H2O2 or povidone-iodine completely inhibited SARS-CoV-2 infectivity; a 50% v/v dilution of chlorhexidine gluconate or (alcohol and essential oils) was necessary to inhibit the capacity of SARS-CoV-2 infection. | 2021 | [2] |
| Oral antiseptic solution with 0.05% cetylpyridinium chloride (CPC) and 1.5% H2O2; oral antiseptic solution with 0.1% chlorhexidine, 0.05% CPC and 0.005% sodium fluoride. | CPC or a combination of chlorhexidine with CPC is more effective than chlorhexidine or H2O2 alone. Rinses with these active ingredients could reduce the viral load in the oral cavity and the transmission of SARS-CoV-2 during dental procedures. | 2021 | [24] |
| A solution with 1.4% dipotassium oxalate, without ethanol; mouthwash with eucalyptol, thymol, menthol, sodium fluoride, and zinc fluoride. | These active ingredients, as well as other mouthwashes containing 0.01–0.02% hypochlorous acid or 0.58% povidone–iodine, successfully inactivated SARS-CoV-2. | 2021 | [25] |
| 0.12% chlorhexidine digluconate solution; antiseptic oral solution with 0.075% CPC and 0.05% NaF; 0.05% thymol solution; mouthwash with 0.1% hexetidine with 9% ethanol; saline water (0.34 M sodium chloride). | Rinses with CPC and hexetidine demonstrated a potent virucidal effect. Chlorhexidine digluconate showed a slightly lesser effect, whereas thymol or saline water had no significant effect in reducing the SARS-CoV-2 viral load. | 2021 | [26] |
| Sodium bicarbonate (NaHCO3; 1% baby shampoo in PBS (phosphate-buffered saline) nasal rinse solution; 1.5% H2O2 solution; oral antiseptic solution with 1.5% H2O2 and 0.1% menthol 0.1%; 0.07% CPC solution; mouthwash solutions with 0.092% eucalyptol, 0.042% menthol, 0.06% methyl salicylate, and 0.064% thymol; 5% PVP-I solution. | 1% baby shampoo nasal rinse solution and mouthwash solutions with eucalyptol, menthol, methyl salicylate, and thymol inactivated 99.9% of the human coronavirus. Rinses with 1.5% and 3.0% H2O2 decreased the viral load of human coronaviruses between 90% and 99%. PVP-I exhibited a virucidal effect on human coronaviruses, but NaHCO3 had no effect on coronavirus viral load. | 2021 | [27] |
| Oral and nasal antiseptic solutions with 1% or 5% PVP-I. | All concentrations of PVP-I showed a virucidal effect against SARS-CoV-2. | 2021 | [28] |
| Solution with D-limonene (0.2%) and CPC (0.05%). | It showed an approximately 99.99% reduction in virucidal activity against SARS-CoV-2. | 2022 | [29] |
| Active Ingredients | Effect | Year | References |
|---|---|---|---|
| 1% H2O2 solution. | Mouthwash with 1% H2O2 did not produce a significant reduction in intraoral viral load in patients positive for SARS-CoV-2 after 30 min of application. | 2020 | [3] |
| 0.12% chlorhexidine gluconate solution. | 0.12% chlorhexidine solution considerably decreased the viral load of SARS-CoV-2 in the saliva of patients during early stages of COVID-19 infection. | 2020 | [30] |
| 0.5% PVP-I solution. | The solution applied intranasally and orally was well tolerated in a group of patients and health workers. Pre-trial studies suggest that the use of 0.5% PVP-I could help in reducing the spread of SARS-CoV-2, especially during clinical examination procedures such as endoscopy. | 2020 | [31] |
| 0.5% w/v PVP-I solution; 0.2% w/v chlorhexidine gluconate solution; 0.075% CPC solution. | PVP-I and CPC mouthwashes decreased the SARS-CoV-2 viral load in patient saliva samples up to 6 h after use. | 2021 | [32] |
| 1% H2O2 solution; 0.12% chlorhexidine gluconate solution; 0.5% PVP-I solution; saline solution. | The four solutions decreased the viral load of SARS-CoV-2 in saliva samples from asymptomatic, pre-symptomatic, symptomatic, and post-symptomatic individuals. In those individuals with an initial viral load of fewer than 104 copies/mL of saliva, there was a 100% reduction in viral load at 15 and 45 min after application. | 2021 | [33] |
| Mouthwash with 0.075% CPC + 0.28% zinc lactate; mouthwash with 1.5% H2O2; mouthwash with 0.12% chlorhexidine gluconate. | Mouthwashes with CPC + zinc lactate and chlorhexidine gluconate significantly decreased the viral load of SARS-CoV-2 in the saliva of patients up to 60 min after application, whereas H2O2 only decreased viral load 30 min after use. | 2021 | [34] |
| 0.12% chlorhexidine gluconate. | The use of chlorhexidine gluconate as a mouthwash applied for 30 s twice a day for 4 days was effective in eliminating the viral load of SARS-CoV-2 in 62.1% of a group of 121 patients positive for infection. Additionally, 173 patients positive for SARS-CoV-2 and treated with chlorhexidine gluconate mouthwash and nasal spray twice daily for 4 days resulted in clearance of the SARS-CoV-2 viral load in 86% of patients. | 2021 | [35] |
| 0.2% chlorhexidine gluconate; 1% PVP-I. | The application of oral solutions with chlorhexidine and PVP-I for 30 s was effective in significantly reducing the viral load of SARS-CoV-2 in the saliva of 61 patients positive for infection. | 2021 | [36] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero Bernal, C.G.; Reyes Uribe, E.; Salazar Flores, J.; Varela Hernández, J.J.; Gómez-Sandoval, J.R.; Martínez Salazar, S.Y.; Gutiérrez Maldonado, A.F.; Aguilar Martínez, J.; Lomelí Martínez, S.M. Oral Antiseptics against SARS-CoV-2: A Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 8768. https://doi.org/10.3390/ijerph19148768
Guerrero Bernal CG, Reyes Uribe E, Salazar Flores J, Varela Hernández JJ, Gómez-Sandoval JR, Martínez Salazar SY, Gutiérrez Maldonado AF, Aguilar Martínez J, Lomelí Martínez SM. Oral Antiseptics against SARS-CoV-2: A Literature Review. International Journal of Environmental Research and Public Health. 2022; 19(14):8768. https://doi.org/10.3390/ijerph19148768
Chicago/Turabian StyleGuerrero Bernal, Cristian Gabriel, Emmanuel Reyes Uribe, Joel Salazar Flores, Juan José Varela Hernández, Juan Ramón Gómez-Sandoval, Silvia Yolanda Martínez Salazar, Adrián Fernando Gutiérrez Maldonado, Jacobo Aguilar Martínez, and Sarah Monserrat Lomelí Martínez. 2022. "Oral Antiseptics against SARS-CoV-2: A Literature Review" International Journal of Environmental Research and Public Health 19, no. 14: 8768. https://doi.org/10.3390/ijerph19148768