
COVID-19 Vaccination Status among Pregnant and Postpartum Women—A Cross-Sectional Study on More Than 1000 Individuals

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Recruitment
2.3. Design
2.4. Outcomes
2.5. Statistical Analysis
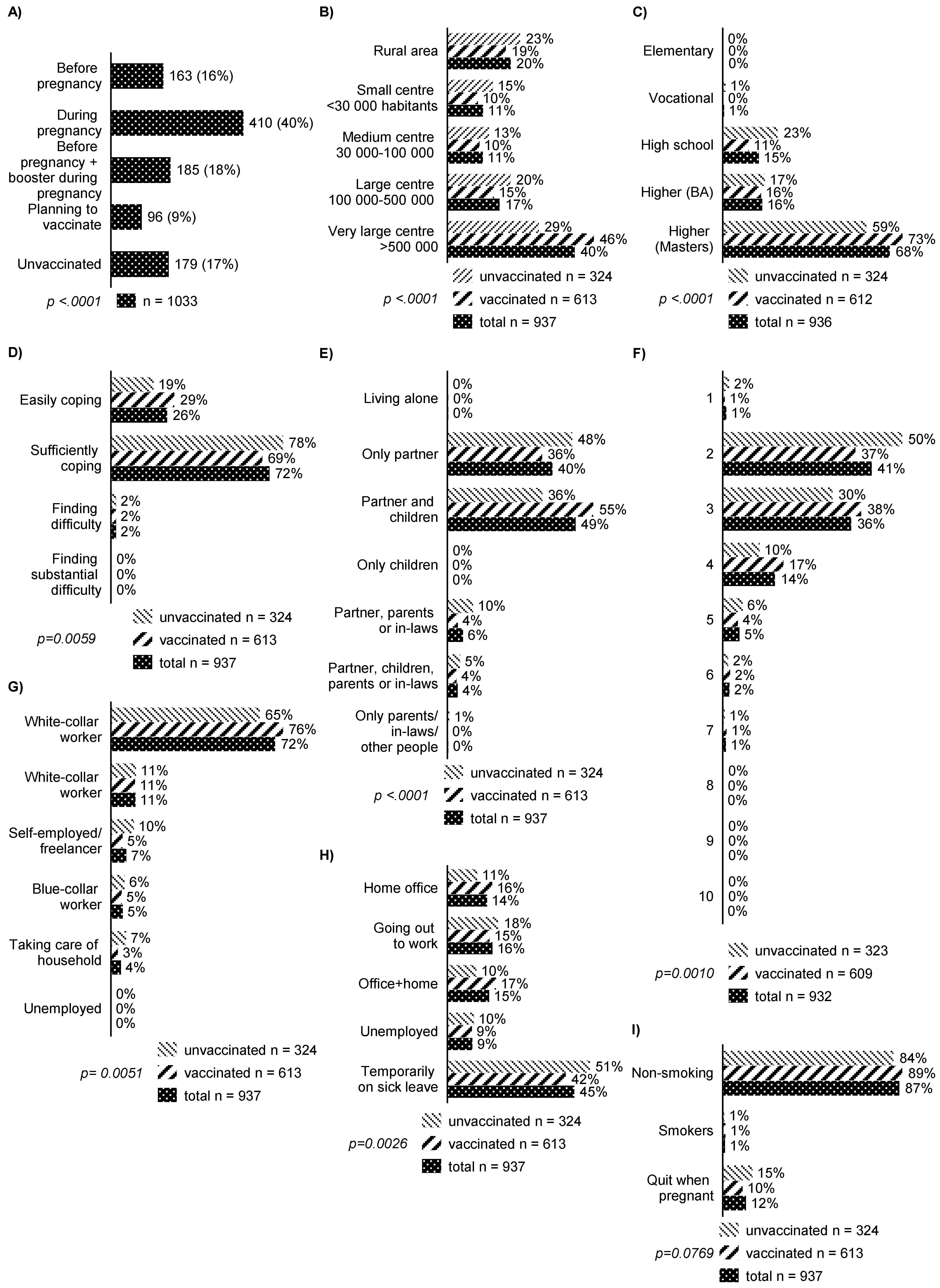
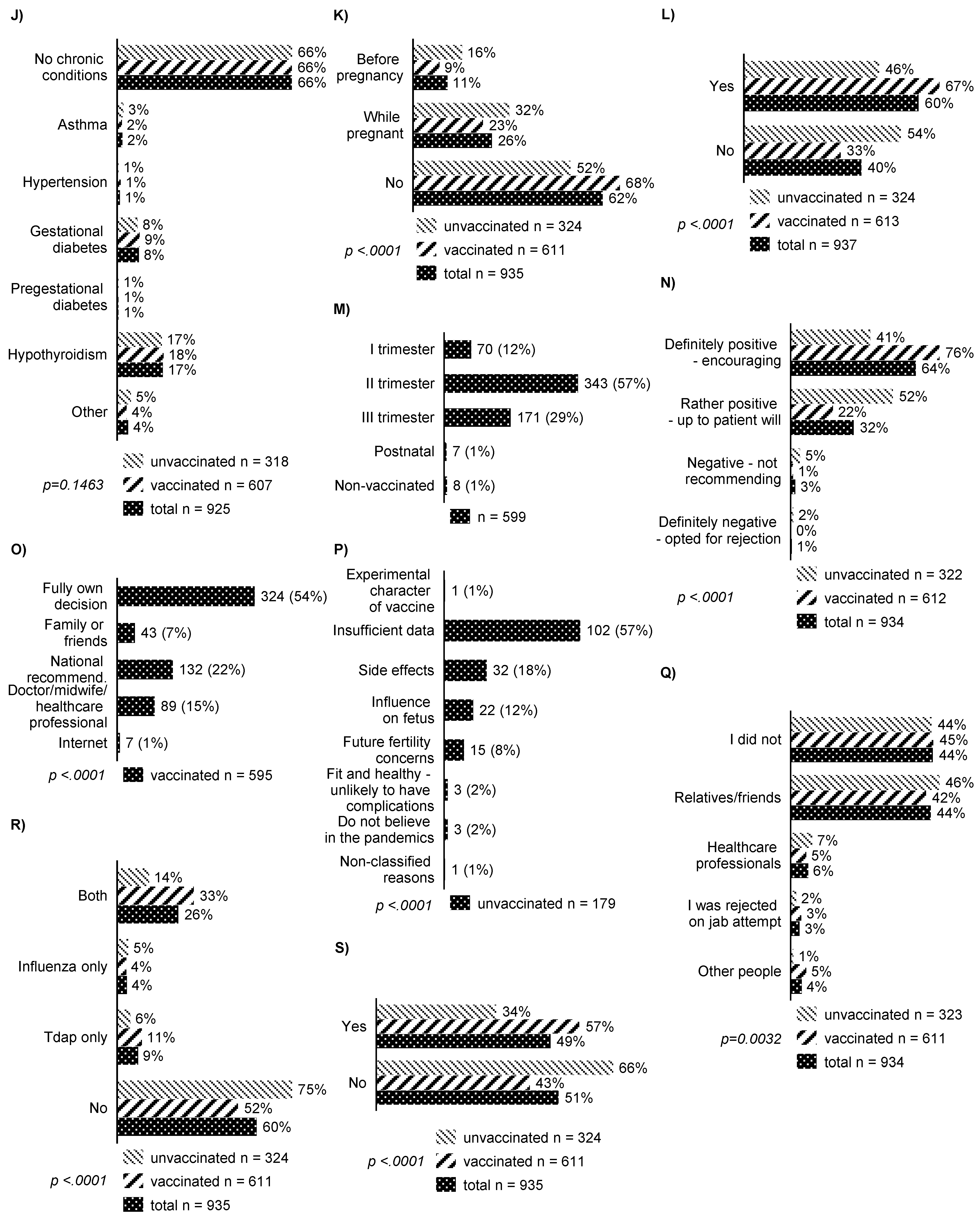
3. Results
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mullins, E.; Hudak, M.L.; Banerjee, J.; Getzlaff, T.; Townson, J.; Barnette, K.; Playle, R.; Bourne, T.; Lees, C.; PAN-COVID Investigators and the National Perinatal COVID-19 Registry Study Group. Pregnancy and neonatal outcomes of COVID-19: Coreporting of common outcomes from PAN-COVID and AAP-SONPM registries. Ultrasound Obstet. Gynecol. 2021, 57, 573. [Google Scholar] [CrossRef] [PubMed]
- Heydarifard, Z.; Zadheidar, S.; Yavarian, J.; Malekshahi, S.S.; Kalantari, S.; Mokhtari-Azad, T.; Shafiei-Jandaghi, N. Potential role of viral infections in miscarriage and insights into the underlying molecular mechanisms. Congenit. Anom. 2022, 62, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Oton-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on Spontaneous Abortion and Human Papillomavirus Infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef] [PubMed]
- Galang, R.R.; Chang, K.; Strid, P.; Snead, M.C.; Woodworth, K.R.; House, L.D.; Perez, M.; Barfield, W.D.; Meaney-Delman, D.; Jamieson, D.J.; et al. Severe Coronavirus Infections in Pregnancy: A Systematic Review. Obstet. Gynecol. 2020, 136, 262–272. [Google Scholar] [CrossRef]
- Kiefer, M.K.; Mehl, R.; Costantine, M.M.; Johnson, A.; Cohen, J.; Summerfield, T.L.; Landon, M.B.; Rood, K.M.; Venkatesh, K.K. Characteristics and perceptions associated with COVID-19 vaccination hesitancy among pregnant and postpartum individuals: A cross-sectional study. BJOG: Int. J. Obstet. Gynaecol. 2022, 129, 1342–1351. [Google Scholar] [CrossRef]
- Kalafat, E.; Magee, L.A.; von Dadelszen, P.; Heath, P.; Khalil, A. COVID-19 booster doses in pregnancy and global vaccine equity. Lancet 2022, 399, 907–908. [Google Scholar] [CrossRef]
- Etti, M.; Calvert, A.; Galiza, E.; Lim, S.; Khalil, A.; Le Doare, K.; Heath, P.T. Maternal vaccination: A review of current evidence and recommendations. Am. J. Obstet. Gynecol. 2022, 226, 459–474. [Google Scholar] [CrossRef]
- Skirrow, H.; Barnett, S.; Bell, S.; Riaposova, L.; Mounier-Jack, S.; Kampmann, B.; Holder, B. Women’s views on accepting COVID-19 vaccination during and after pregnancy, and for their babies: A multi-methods study in the UK. BMC Pregnancy Childbirth 2022, 22, 1–15. [Google Scholar] [CrossRef]
- CDC. Centers for Disease Control and Prevention. Information about COVID-19 Vaccines for People Who Are Pregnant or Breastfeeding. Internet. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html (accessed on 6 March 2022).
- Joint Committee on Vaccination and Immunisation: Advice on Priority Groups for COVID-19 Vaccination, 30 December 2020—GOV.UK. Available online: https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and-immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020 (accessed on 6 March 2022).
- Stanowisko PTGiP Dotyczące Szczepień Kobiet Ciężarnych Przeciwko COVID-19|ptgin.pl. Available online: https://www.ptgin.pl/aktualnosc/stanowisko-ptgip-dotyczace-szczepien-kobiet-ciezarnych-przeciwko-covid19 (accessed on 6 March 2022).
- Stock, S.J.; Carruthers, J.; Calvert, C.; Denny, C.; Donaghy, J.; Goulding, A.; Hopcroft, L.E.M.; Hopkins, L.; McLaughlin, T.; Pan, J.; et al. SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland. Nat. Med. 2022, 28, 504–512. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1. [Google Scholar] [CrossRef]
- Vaccine Pregnancy Registry|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/vsafepregnancyregistry.html (accessed on 6 March 2022).
- Key Information on COVID-19 in Pregnancy|NPEU. Available online: https://www.npeu.ox.ac.uk/news/2171-covid-19-in-pregnancy-2 (accessed on 11 March 2022).
- Hosokawa, Y.; Okawa, S.; Hori, A.; Morisaki, N.; Takahashi, Y.; Fujiwara, T.; Nakayama, S.F.; Hamada, H.; Satoh, T.; Tabuchi, T. The prevalence of COVID-19 vaccination and vaccine hesitancy in pregnant women: An internet-based cross-sectional study in Japan. J. Epidemiol. 2022, 32, 188–194. [Google Scholar] [CrossRef]
- Nowacka, U.; Kozlowski, S.; Januszewski, M.; Sierdzinski, J.; Jakimiuk, A.; Issat, T. COVID-19 Pandemic-Related Anxiety in Pregnant Women. Int. J. Environ. Res. Public Health 2021, 18, 7221. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Kelley, K.; Clark, B.; Brown, V.; Sitzia, J. Good practice in the conduct and reporting of survey research. Int. J. Qual. Health Care 2003, 15, 261–266. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Sutton, D.; D’Alton, M.; Zhang, Y.; Kahe, K.; Cepin, A.; Goffman, D.; Staniczenko, A.; Yates, H.; Burgansky, A.; Coletta, J.; et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am. J. Obstet. Gynecol. MFM 2021, 3, 100403. [Google Scholar] [CrossRef]
- Esen, B.K.; Can, G.; Pirdal, B.Z.; Aydin, S.N.; Ozdil, A.; Balkan, I.I.; Budak, B.; Keskindemirci, Y.; Karaali, R.; Saltoglu, N. COVID-19 Vaccine Hesitancy in Healthcare Personnel: A University Hospital Experience. Vaccines 2021, 9, 1343. [Google Scholar] [CrossRef]
- Kilich, E.; Dada, S.; Francis, M.R.; Tazare, J.; Chico, R.M.; Paterson, P.; Larson, H.J. Factors that influence vaccination decision-making among pregnant women: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0234827. [Google Scholar] [CrossRef]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus disease 2019 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef]
- Situation Ukraine Refugee Situation. Available online: https://data2.unhcr.org/en/situations/ukraine (accessed on 23 March 2022).
- Coronavirus (COVID-19) Vaccinations—Our World in Data. Available online: https://ourworldindata.org/covid-vaccinations?country=UKR (accessed on 23 March 2022).
- Saitoh, A.; Takaku, M.; Saitoh, A. High rates of vaccine hesitancy among pregnant women during the coronavirus disease 2019 (COVID-19) pandemic in Japan. Hum. Vaccines Immunother. 2022, 18, 1–7. [Google Scholar] [CrossRef]
- DesJardin, M.; Raff, E.; Baranco, N.; Mastrogiannis, D. Cross-Sectional Survey of High-Risk Pregnant Women’s Opinions on COVID-19 Vaccination. Women’s Health Rep. 2022, 3, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, K.; Messer, A.; Alvarado, S.; Gaudette, M.; Tran, C.; Bandoli, G. COVID-19 vaccine hesitancy and acceptance among pregnant people contacting a teratogen information service. J. Genet. Couns. 2022. [Google Scholar] [CrossRef] [PubMed]
- Poland: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/region/euro/country/pl (accessed on 21 March 2022).
- Riley, L.E. mRNA COVID-19 Vaccines in Pregnant Women. N. Engl. J. Med. 2021, 384, 2342–2343. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (N = 1033) | COVID-19 Vaccinated (N = 613) | COVID-19 Unvaccinated (N = 324) | Planning to Vaccinate to COVID-19 (N = 96) | |
|---|---|---|---|---|
| % | 100% | 59.3% | 31.4% | 9.3% |
| Maternal age, mean (SD) | 30.5 (4.1) | 31.2 (3.9) | 29.4 (4.2) | 30.4 (4.1) |
| Mean gestational age (SD) | 27.1 (9.1) | 29.2 (8.4) | 24.4 (9.1) | 27.7 (11.1) |
| Mean gestational age at delivery (SD) | 38.9 (2.4) | 38.9 (2.6) | 38.7 (2.2) | 39.0 (1.4) |
| Number of pregnancies mean (SD) | 1.68 (0.9) | 1.7 (0.9) | 1.63 (0.9) | 1.71 (0.9) |
| Mean parity (SD) | 0.89 (1.2) | 0.94 (0.9) | 1.73 (1.8) | 1.09 (0.9) |
| Effect | OR | 95% CI | Standard Error | p-Value |
|---|---|---|---|---|
| Parity 0 vs. ≥1 | 1.74 | 1.43–2.12 | 0.0995 | <0.0001 |
| Place of residence (medium center vs. small + rural area) | 1.15 | 0.7–1.88 | 0.2517 | 0.5852 |
| Place of residence (large and very large center vs. small + rural area) | 1.51 | 1.09–2.1 | 0.1673 | 0.0137 |
| Education (masters + bachelor’s vs. elementary + vocational + high school) | 2.26 | 1.53–3.34 | 0.1988 | <0.0001 |
| History of COVID-19 infection | 1.92 | 1.43–2.59 | 0.1527 | <0.0001 |
| Vaccination offered by a doctor/midwife | 1.54 | 1.11–2.12 | 0.1657 | 0.0097 |
| Positive attitude of a doctor/midwife towards vaccination | 2.74 | 1.2–6.29 | 0.4234 | 0.0172 |
| Information from a doctor/midwife about a high risk of COVID-19 complications | 2.15 | 1.55–2.98 | 0.1672 | <0.0001 |
| Effect | OR | 95% CI | Standard Error | p-Value |
|---|---|---|---|---|
| Having children 3 and more vs. 0 | 4.8 | 2.0–11.6 | 0.4522 | 0.0006 |
| Having children 3 vs. 1 | 2.15 | 0.89–5.2 | 0.4502 | 0.0896 |
| Having children 3 vs. 2 | 1.78 | 0.69–4.59 | 0.4825 | 0.2318 |
| Education (elementary + vocational + high school vs. master’s + bachelor’s) | 2.29 | 1.55–3.39 | 0.1990 | <0.0001 |
| Lack of COVID-19 infection in the past | 1.89 | 1.4–2.55 | 0.1533 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowacka, U.; Malarkiewicz, P.; Sierdzinski, J.; Januszaniec, A.; Kozłowski, S.; Issat, T. COVID-19 Vaccination Status among Pregnant and Postpartum Women—A Cross-Sectional Study on More Than 1000 Individuals. Vaccines 2022, 10, 1179. https://doi.org/10.3390/vaccines10081179
Nowacka U, Malarkiewicz P, Sierdzinski J, Januszaniec A, Kozłowski S, Issat T. COVID-19 Vaccination Status among Pregnant and Postpartum Women—A Cross-Sectional Study on More Than 1000 Individuals. Vaccines. 2022; 10(8):1179. https://doi.org/10.3390/vaccines10081179
Chicago/Turabian StyleNowacka, Urszula, Paulina Malarkiewicz, Janusz Sierdzinski, Aleksandra Januszaniec, Szymon Kozłowski, and Tadeusz Issat. 2022. "COVID-19 Vaccination Status among Pregnant and Postpartum Women—A Cross-Sectional Study on More Than 1000 Individuals" Vaccines 10, no. 8: 1179. https://doi.org/10.3390/vaccines10081179