Article Text

Abstract
Introduction Coronovirus disease 2019 (COVID-19) misinformation has been reported globally and locally. This has the potential to influence public risk perception and reduce the acceptance of the COVID-19 vaccine. This study aims to determine the prevalence of COVID-19 misinformation and vaccine hesitancy in Buikwe district. The study will also pilot a social mobilisation intervention using community influencers and determine its effect on COVID-19 misinformation and vaccine hesitancy.
Methods and analysis The study will be conducted using a quasi-experimental study design, in which two villages will be assigned to the intervention arm and two villages assigned controls. A mixed-methods technique employing both quantitative and qualitative methods will be employed. Data will be collected from healthy men and women aged 18 years and older who reside in the selected villages. The study will be implemented in three phases. First, a baseline study of 12 in-depth interviews with key informants and 6 focus group discussions and a household survey among 632 participants will be done. Second, an intervention employing dialogue-based social mobilisation approach using 10-man community groups per village will be developed and implemented. These will be trained and facilitated to educate and sensitise their communities about COVID-19. Third, an end-line household survey done after 6-months of intervention implementation in the four villages to assess the effect of the intervention on COVID-19 misinformation and vaccine hesitancy. Post-intervention qualitative evaluation will be done after the endline quantitative assessment. Preliminary analysis of the endline quantitative analysis will inform any revisions of the discussion guides. Qualitative data collected will be analysed using thematic content analysis while quantitative data will be analysed using χ2 tests or logistic regression, by intention-to-treat analysis.
Ethics and dissemination The study was reviewed for ethics and approved by the Makerere University School of Health Sciences Research Ethics Committee, reference number MakSHSREC-2020-45 and the Uganda National Council of Science and Technology, reference number HS1140ES. Study finding shall be presented to the district and national COVID-19 task force and at scientific gatherings and published in a peer-reviewed journal.
Trial registration number PACTR202102846261362.
- COVID-19
- epidemiology
- protocols & guidelines
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This protocol reports sequential mixed qualitative and quantitative methods to assess the magnitude of a COVID-19 misinformation and vaccine hesitancy in the community.
The study has an intervention and comparison arm with a before-and-after assessment of the outcomes to address the counterfactual phenomenon.
The study will conduct post-intervention qualitative assessment to understand the mechanisms of effect of the intervention and explore what worked and why it worked.
The study employs a quasi-experimental study design with the attendant selection bias instead of a randomised clinical trial to generate empirical evidence about a public health intervention.
The study relies on self report which is amenable to social desirability bias to measure the outcome of COVID-19 misinformation and vaccination hesitancy.
Introduction
The unprecedented Coronavirus disease 2019 (COVID-19) pandemic has not only posed a health challenge but continues to affect most sectors worldwide. As of August 13th 2022, over 585,950,085 cases and 6,425,422 deaths have been reported globally, according to the World Health Organisation (WHO) COVID-19 dashboard. The COVID-19 pandemic has been marked by widespread misinformation globally.1 The WHO Director General stated in his address at the Munich Security Conference 2020 that the fight was not just about a pandemic but an infodemic as well. Misinformation is one form of information disorder besides disinformation and malinformation.2 Wardle and Derakhshan2 define misinformation as false information that is shared but is not necessarily intended to cause harm, while disinformation is false information that is deliberately created to harm a person, social group, organisation or country. On the other hand, malinformation is information based on reality and used to inflict harm on a person, organisation or country.2 This understanding is further supported by Chou et al3 who asserts that health misinformation is ‘a health-related claim of fact that is currently false due to lack of scientific evidence’.
The COVID-19 infodemic has greatly been promoted over mainstream social media which generally have limited censorship of posts on users’ timelines. Several conspiracies have emerged worldwide and among them includes its association with 5G technology, bioengineering from Wuhan, Bill Gates agenda on population control using vaccines, etc. In Uganda, a lot of health misinformation related to COVID-19 has been reported since the beginning of the present COVID-19 pandemic. An online survey reported that 30.2% of Ugandans consider COVID-19 to be ‘a disease of the whites’, and expect mortality to be highest among ‘white’ people from Europe and the USA.4 Misinformation affects public perception of risk and breeds mistrust which may undermine acceptance and adherence to preventive measures, including acceptance of the COVID-19 vaccine. As such, the WHO and other global and national actors have responded to the threat of misinformation by running campaigns that encourage fact-checking of health information.5 However, little has been done to address COVID-19 misinformation in Uganda or to understand and address how this could influence COVID-19 vaccine hesitancy.
Vaccine hesitancy refers to ‘delay in acceptance or refusal of vaccines despite the availability of vaccination services’.6 It is a context-specific and vaccine-specific behavioural phenomenon that occurs when vaccine acceptance is lower than would be expected, given that vaccination services are available. Vaccine hesitancy occurs on a continuum between full vaccine acceptance and outright refusal of some or all vaccines.6 Hesitancy to the COVID-19 vaccine has been reported in different parts of the world. An American study shows that only 66% of adults would be somewhat or extremely likely to vaccinate themselves or their children with a COVID-19 vaccine if it was made available to them.7 Likewise, in Italy, 13.9% of university students expressed low intention to vaccinate with the COVID-19 vaccine.8
In Uganda, an online survey of 1067 respondents showed a 53.6% acceptance rate for the COVID-19 vaccine. Also, 46.7% of the respondents considered the COVID-19 vaccine to carry some risk to individuals.9 Among health profession students, COVID-19 vaccine acceptance was 37.3% with hesitancy at 30.7%. Although these studies may have had inherent limitations such as selection and information bias due to the online nature of data collection, the reported estimates are substantial. The predicted low COVID-19 vaccine acceptance rates and perception of risk will need to be addressed for successful deployment to achieve high coverage of a COVID-19 vaccine when it is made available in Uganda. Our study proposes to examine community-level hesitancy to the COVID-19 vaccine and prevalence of COVID-19 misinformation, an important driver of vaccine hesitancy.
Dialogue-based community interventions, especially those involving social mobilisation and the use of community influencers are effective in reducing vaccine hesitancy and increasing vaccine uptake.10 The Social Mobilisation Approach uses existing social capital to mobilise local resources to achieve community participation and local ownership of interventions.11 Social mobilisation facilitates change by engaging various partners and allies in interrelated and complementary efforts to raise awareness. The engagement of community influencers such as local and religious leaders has the potential for success as it is well aligned with natural community processes of seeking out community leaders and encouraging dialogue to inform and influence.10
With this intervention, we seek to reduce the prevalence of COVID-19 misinformation and vaccine hesitancy among adults in Buikwe District, Uganda. Adults are being targeted because they influence vaccine uptake among their children. Findings from the study will provide COVID-19 response teams and immunisation programme implementers in Uganda with information of the prevalence and spread of COVID-19 misinformation and how it may affect the acceptance of the COVID-19 vaccine. Results from piloting the intervention will also provide evidence of the effect of a social mobilisation intervention on COVID-19 misinformation and vaccine hesitancy in a low-resource setting.
Methods and materials
Conceptual framework
The Strategic Advisory Group of Experts on Immunisation has advanced a simple framework, commonly referred to as ‘3Cs’, for conceptualising the determinants of vaccine hesitancy. The ‘3Cs’ include (1) Confidence in the effectiveness and safety of vaccines and in the health systems that deliver them; (2) Complacency as a result of the low perceived risk of vaccine-preventable diseases and (3) Convenience—the extent to which ‘physical availability, affordability and willingness-to-pay, geographical accessibility, ability to understand and appeal of immunisation services affect uptake’.6
Additionally, Betsch et al12 in their work to develop a measure to assess psychological antecedents of vaccination argue for the inclusion of calculation (one’s engagement in extensive information searching) and collective responsibility (the willingness to protect others through herd immunity following one’s vaccination) as the fourth and fifth determinants of vaccine hesitancy and eventually vaccine uptake, respectively. See figure 1 for the conceptual framework adapted for this study. These determinants can be further reinforced by the presence of COVID-19 misinformation, which affects risk perception and creates mistrust in health systems.
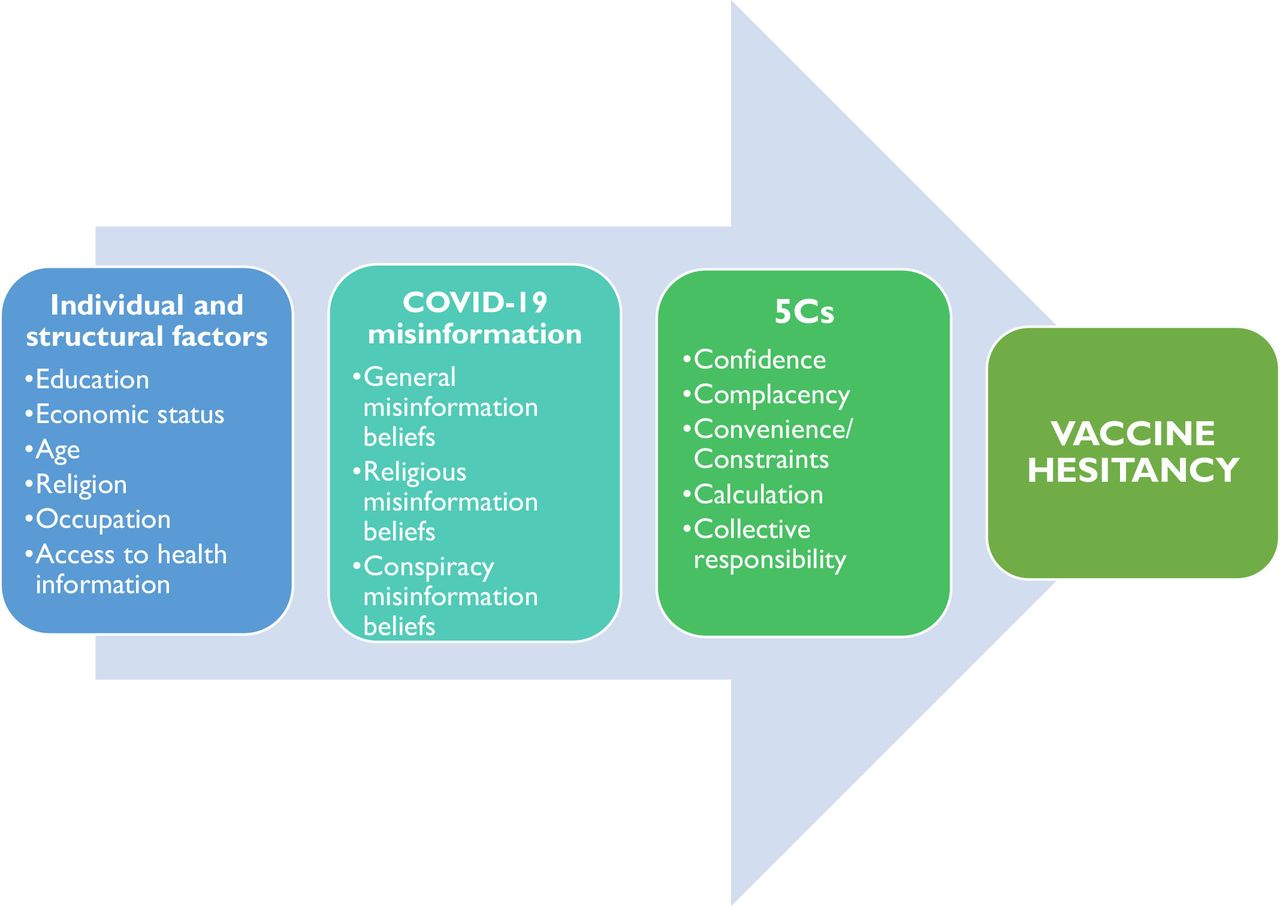
Conceptual framework showing factors that influence COVID-19 misinformation and their relationship with vaccine hesitancy.
Study objectives
Primary objectives
To determine the effect of community influencer groups on reducing:
The proportion of community members with COVID-19 misinformation.
The proportion of community members with hesitancy towards the COVID-19 vaccine.
Secondary objectives
To form, empower and initiate community influencer groups to address COVID-19 misinformation and hesitancy to the COVID-19 vaccine in Buikwe district.
To determine the effect of community influencer groups on confidence, complacency, constraints, calculations and collective responsibility of vaccination with regard to the COVID-19 vaccine.
Study design
The study will be quasi-experimental using a pre- and post-intervention evaluation design. It will be implemented in three phases. In phase 1, a baseline study will be conducted to understand: (1) the spread of COVID-19 misinformation, (2) the individual and social-cultural factors that perpetuate this misinformation and, (3) how the individual and social-cultural factors could affect acceptance of the COVID-19 vaccine. The second phase will involve the development and implementation of the intervention, and in the third phase, an end-line evaluation will be done after at least 6 months of intervention implementation.
Study setting
The study will be done in Buikwe, a district in the Central part of Uganda (figure 2). Buikwe shares part of the border between Uganda and Tanzania to the South. Buikwe district is made up of one county with eight rural subcounties and four town councils, under which there are 470 village councils.13 The population of the district is estimated at 482 900 with 50.8% of these being female.14 About 45% of the population is aged 18 years and older, and out of all those aged 18 years and older, 21% are illiterate. Seventy-three per cent of all households in Buikwe are male-headed.15 Buikwe district was selected for this study because, like all border districts in the country, it has recorded a high number of COVID-19 cases. It is also one of four districts in the country with the highest number of locally transmitted cases of COVID-19.16

A map showing the study setting. Buikwe district is located in central Uganda along the shores of Lake Victoria.
The study will be done in four villages in the district. Two of the study villages will be randomly selected from a rural subcounty, while the other two will be from a town council, a periurban area. The intervention will be applied to one rural and one periurban village, while the other rural and periurban villages will serve as controls.
Eligibility criteria
Quantitative sample
All men and women without signs and symptoms of COVID-19 or a positive COVID-19 test nor in quarantine aged 18–65 years who normally reside in households in the selected villages, domestic servants who have slept for five nights a week or more in the households, and visitors who have slept in the household for at least the past 4 weeks will be eligible to participate in the study.
However, men and women from households that are under COVID-19 isolation or quarantine at the time of data collection will be excluded from the study if they do not have access to a phone for phone interviews to be conducted. This will be done to minimise the risk of spread of the infection to the data collectors.
Qualitative sample
A purposive sample of men and women similar to that for the quantitative household survey will be engaged in focus group discussions (FGDs) in the baseline study. Using village leaders, men and women without signs and symptoms of COVID-19 or a positive COVID-19 test nor in quarantine aged 18–65 years in the study villages will be identified and invited to participate in the study. The participants will be representative of the community members of the study villages. Key informants in Buikwe district including COVID-19 response team members; district immunisation programme implementers; religious and cultural leaders will also be engaged in in-depth interviews (IDIs).
Intervention arm
In the intervention villages, a dialogue-based social mobilisation intervention using community groups of social influencers will be implemented to address COVID-19 misinformation in the community. One community group of 10 members, 5 men and 5 women, will be formed per village. Each group will consist of influential community members such as village local council leaders, religious leaders of all major religious denominations including Christians, muslims, local beliefs, cultural leaders, village health team members and other opinion leaders.
Community influencers will be selected through participatory stakeholder engagements, involving community members, leaders, district immunisation programme team members and the district COVID-19 task force. Influencers will be selected from volunteers who will be tasked with championing the fight against COVID-19 misinformation in their communities. The identified community influencers will be educated about COVID-19 and trained to address misinformation and vaccine hesitancy in their communities.
Training will be conducted virtually using a blended learning approach. Instructor-led training will be done using live and pre-recorded sessions and relayed via a teleconferencing system as a way to promote adherence to prevailing COVID-19 prevention guidelines. Interactive methods such as group discussions, case studies, role-playing and quizzes will also be used. The training will provide the influencers with information on COVID-19 prevention measures, the available COVID-19 vaccines and address any misinformation identified in the baseline study. It will also cover effective communication, teamwork and leadership. Training will be done over 5 days and facilitated by two trainers separate from the project team. Additional training sessions will be organised routinely over the course of the project to address specific knowledge gaps identified.
The influencers will be expected to disseminate the information, education and communication (IEC) about COVID-19 in their communities using outdoor community radios where these are available and megaphones. They will also sensitise and educate their communities through public addresses at their routine permitted gatherings including religious services, weddings and funeral ceremonies. By working with the influencers and Ministry of Health officials, context-specific IEC material will be developed in the local language, piloted and refined. This IEC material will be shared with the community influencers to distribute to community members during their interactions.
Community influencers will be volunteers who will not be paid a salary. However, they will be provided with financial support and other facilitation to conduct their different activities. To minimise the risk of infection with COVID-19 during their activities, community influencers will be educated about the recommended infection prevention measures before commencing their activities and also regularly provided with face masks and hand sanitisers.
Control arm
Community influencer groups will not be formed in the two control villages. Sensitisation and education activities will continue as programmed by the Ministry of Health.
Study outcomes
Primary outcome variables
The proportion of community members with COVID-19 misinformation. Misinformation will be measured in three dimensions: general misinformation beliefs, conspiracy misinformation beliefs and religious misinformation beliefs.17 A scale adapted from Barua et al17 and refined using findings from the qualitative study will be used.
The proportion of community members with hesitancy towards the COVID-19 vaccine. COVID-19 vaccine hesitancy will be assessed using the question, ‘How accepting would you be of a COVID-19 vaccine for yourself if it was made available to you?’
Secondary outcome variables
The psychological antecedents of vaccination: confidence, complacency, constraints, calculations and collective responsibility. These will be measured using the 5C scale adopted from Betsch et al.12
Sample size
Quantitative sample size
The quantitative sample size was calculated using OpenEpi Sample size calculator V.3 for randomised trials using Fleiss’ formula.18 We aim to detect a 33% reduction in the prevalence of misinformation from 30.2% reported in an online survey done in Uganda2 to 20%. Statistical power was 80% at a 95% level of confidence. This gave a sample size of 287 participants in the control group and 287 in the intervention group. This was adjusted for 10% attrition to give 316 participants per study arm.
Qualitative sample size
IDIs will be conducted with 12 informants in the district. Six FGDs will also be done with purposively selected samples of 6–8 community members in each group. Three FGDs will be done with participants from rural settings and three with participants from periurban settings. The final number of KIIs and FGDs to be conducted will be informed by data saturation.
Participant timeline
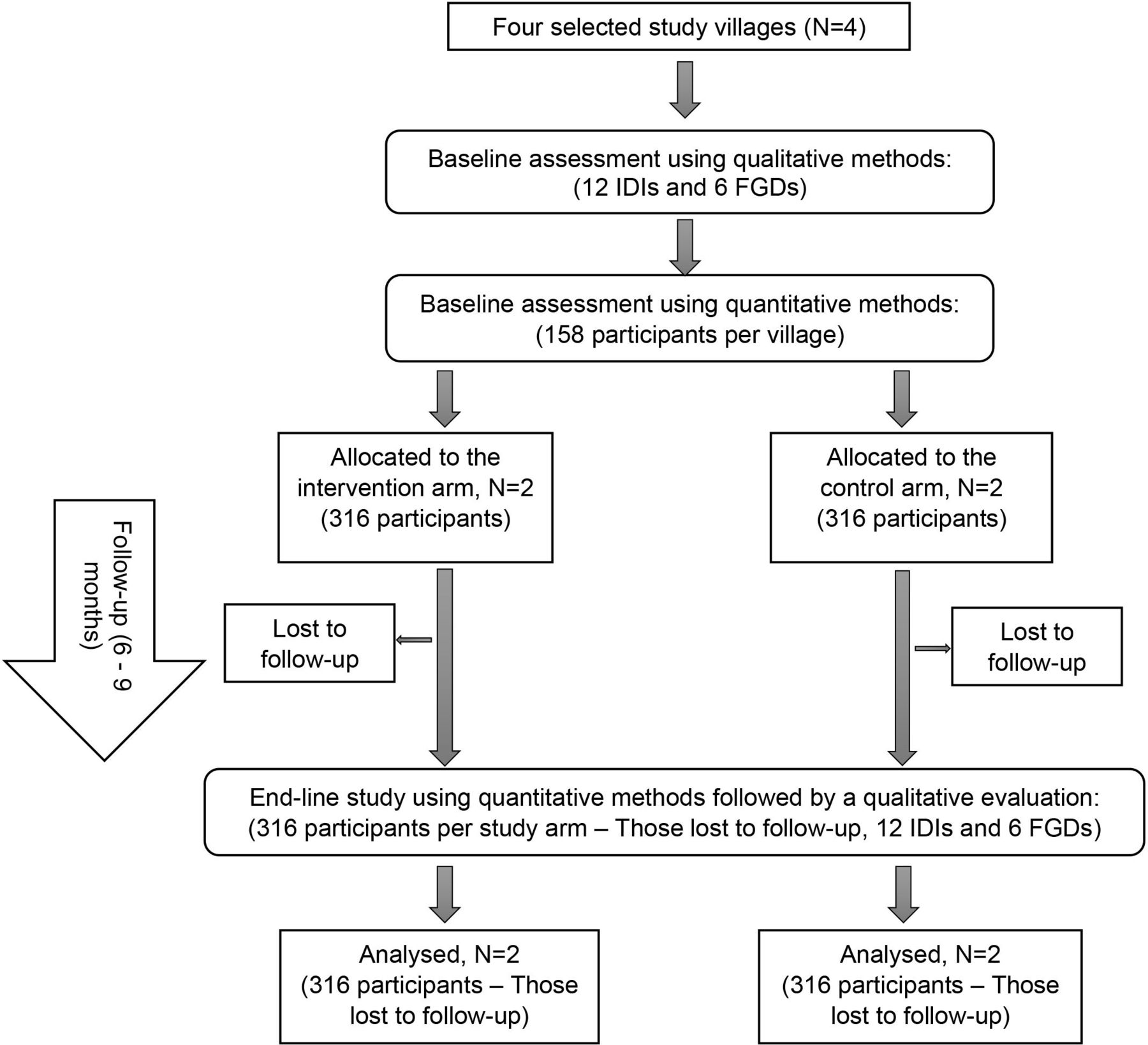
Two villages will be allocated to the intervention arm, one of which will be periurban and the other rural. The other two will be allocated to the control arm. For the baseline study, qualitative data will be collected in all four villages, followed by a quantitative household survey done among an equal number of participants in the control and intervention villages. The intervention will then be implemented in the two intervention villages. The two groups will be followed up for 6 months, after which another household survey will be done among the same participants as those included in the baseline survey. The flow of study participants is illustrated in figure 3.
{kind=link}
{kind=link}
{kind=link}
Participant flow chart. FGDs, focus group discussions; IDIs, in-depth interviews.
Participant recruitment
A list of households and telephone contact details of potential study participants will be obtained in each study village. Households to include in the study will be sampled systematically from this list. Quota sampling will be used to select one participant for interview per household, so as to achieve an equal number of male and female participants per village.
Data collection
Baseline study
The baseline study will be done in all four villages. Data for the baseline study will be collected using a sequential exploratory design where qualitative methods will be done first to inform the refinement of quantitative data collection tools.
Qualitative methods
The qualitative methods will be used to understand misinformation about COVID-19 and how it is likely to impact the acceptance of the COVID-19 vaccine. IDIs will be conducted with key informants in the district while FGDs will be held with purposively selected samples of community members. IDIs will be conducted at the key informants’ places of work or in designated spaces in the community using the IDI topic guide (online supplemental file 1). FGDs will be conducted in the community while maintaining a distance of two metres among all participants using the FGD topic guide (online supplemental file 2). These will be done separately for male and female participants.
Supplemental material
Supplemental material
Data will be collected by trained research assistants with a background in Social Sciences and trained in the study procedures and research ethics. These will use pretested FGD and IDI topic guides and, depending on the participants’ preferences, will administer the interviews and moderate the FGDs either in English or Luganda, the language predominantly spoken in the district. To minimise the risk of infection with COVID-19, key informant interviews will be conducted on phone for participants with mobile phones. All IDIs and FGDs will be audio recorded.
Quantitative methods
A quantitative household survey will be done, informed by findings from the qualitative study. Face-to-face interviews expose the research team and study participants to a risk of infection with COVID-19. To minimise this risk, interviews will be conducted by phone interview as much as possible. For households where no member has a phone, research assistants will travel to the households and conduct the interviews while observing the 2 m physical distance and other COVID-19 preventive measures.
All data will be collected electronically using KoboToolbox19 installed on tablets by trained research assistants with a bachelor’s degree in social sciences or public health who will be supervised by the principal investigators. A questionnaire developed by the researchers will be used to collect the data. A copy of this structured questionnaire has been provided at online supplemental file 3. The questionnaire will be refined using findings from the qualitative interviews, translated in Luganda, and pretested in a village in Buikwe district not included in the study.
Supplemental material
The questionnaire will collect data on the study outcomes: COVID-19 misinformation and hesitancy towards a potential COVID-19 vaccine, as well as participant individual and household characteristics. These will include age, gender, tribe, religion, education, marital status, occupation, economic status, position in the household and information sources used. Data will also be collected on the participants’ adult vaccination status, hesitancy towards childhood vaccines and their adherence to COVID-19 preventive measures in place.
End-line study
An end-line study will be done after 6 months of intervention implementation in the four villages to assess the effect of the intervention on the study outcomes. Only the quantitative household survey will be done in the end-line survey. This will be done in the same households and on the same participants as those included in the baseline study. The same questionnaire and data collection procedures will be used in the end-line study as in the baseline study. All precautions stipulated by the National Guidelines for Conduct of Research during Coronavirus Disease 2019 Pandemic20 will be observed during data collection. Qualitative interviews including FGDs and IDIs with some of the social influencers and the beneficiaries of the intervention will be conducted. The interviews will examine the complexities of how the intervention was received, what worked and what did not and how it can be improved. Exploration of relevant emerging issues as the COVID-19 pandemic and COVID-19 vaccination drive has changed over time will be done. At least 12 IDIs and 6 FGDs with community influencers, representatives of the beneficiary community members, healthcare workers and district officials will be conducted after the endline quantitative assessment. However, the actual number will be guided by achievement of topical saturation. Preliminary analysis of the endline quantitative data will be done to inform the final discussion guides for this qualitative evaluation.
Planned start date of the study: April 2021.
Planned end of study: November 2022.
Data management
Qualitative data management
Recorded IDIsand FGDs will be directly translated from Luganda to English (if not conducted in English) and transcribed by the research team. Transcripts will be exchanged between the data collectors and transcribers to check for accuracy against the audio recording and written notes. All transcripts and recordings will be stored on password-protected
Quantitative data management
Data collected using the electronic questionnaire will be synched to a common server at the end of each field day, and it will be checked by the principal investigators for any errors and inconsistencies. It will then be imported into STATA V.14 (StataCorp) for cleaning. Source documents and files will not be destroyed or altered without specific written permission from the principal investigators. Only the principal investigators and authorised personnel will have access to the questionnaires and supporting documents that will be kept on password-protected computers and backed up on Google Drive to prevent total data loss.
Data analysis plan
Qualitative data analysis
Transcripts will be exported into NVivo qualitative data analysis software for analysis. These will be read thoroughly to gain understanding of the context of each interview. Thematic content analysis will then be used to process all responses along with the identification of relevant concepts and ideas found in the transcripts linked to the topics of inquiry. Relevant ideas will be coded and then categorised under specific themes. Pre-existing themes will be included as well as emergent themes.
Quantitative data analysis
Data will be analysed using STATA V.14 (StataCorp). Summary statistics of normally distributed continuous variables will be presented as means with SDs, while those of non-normally distributed continuous variables will be presented as medians with IQRs. Percentages will be used for the categorical variables. Continuous variables with right-skewed distributions will be log-transformed. Categorical characteristics will be compared between groups using χ2 tests or logistic regression, while characteristics of normally distributed continuous variables will be compared using t-tests, and non-normal continuous variables using Wilcoxon tests. Difference-in-difference analysis between the intervention and control villages will also be done. A two-sided statistical test will be used for all analyses with a 95% CI. Intention-to-treat analysis will be done.
Adverse event reporting and harms
Any harms occurring to either households or individuals participating in the study either related to the study or not will be monitored, recorded, reported and addressed accordingly, depending on nature.
Ethical considerations
Research ethics approval
Ethics approval for the study was obtained from the Makerere University School of Health Sciences Research and Ethics Committee (MakSHS REC), reference number MakSHSREC-2020-45 and the Uganda National Council of Science and Technology, reference number HS1140ES. Administrative clearance was sought from Buikwe district administration before project commencement.
Informed consent
Informed consent will be sought from all study participants before interview by the research assistants after they explain the study procedures to the participants, including all possible risks and benefits. Participants interviewed by phone will provide audioconsent, while those interviewed face to face or involved in the FGDs will provide written informed consent to be interviewed and to be audiotaped.
Confidentiality
To ensure confidentiality, all study files will be stored on password-protected computers with access limited to authorised personnel only. Although names will be on the consent forms, these will not be linked to any gathered data, and no participant identifiers will be retained. Participant phone numbers will only be used for research purposes, and will not be linked to any data collected.
Dissemination plans
Study findings will be disseminated to the Buikwe district health team, community members and Ministry of Health officials in a dissemination workshop at the district if there are no COVID-19 restrictions on public gatherings at the time of the dissemination. Otherwise, a virtual dissemination event will be organised. Online dissemination events will also be held involving other researchers to communicate findings and devise ways to take up recommendations from the study. Findings will also be published in a peer-reviewed open-access journal to communicate findings to the international research community.
Patient and public involvement
No patient will be involved. However, the public will participate in the intervention arm through the selection of the social influencers. These social influencers include influential community members such as village local council leaders, religious leaders of all major religious denominations including Christians, Muslims, local beliefs, cultural leaders, village health team members and other opinion leaders. They will be selected through participatory stakeholder engagements with community members, members of the public, leaders, district immunisation programme team members and the district COVID-19 task force.
The social influencers will participate in the cocreation of the dialogue-based social mobilisation interventions and their delivery to address COVID-19 misinformation and vaccine hesitancy. Results from this study will be disseminated to communities where the study was conducted through community engagement, and talks at the community gathering such as church gatherings. Also, the findings will be disseminated through mass media including radio talk shows and print media.
Discussion
This study seeks to address COVID-19 misinformation and potential COVID-19 vaccine hesitancy among adults in a rural part of Uganda using a dialogue-based social mobilisation intervention. In light of the COVID-19 pandemic and restrictions on social interactions, the study uses virtual data collection methods, as much as possible to minimises the risk of infection for both the project team and study participants, allowing research to proceed amidst the COVID-19 pandemic. To avoid selection bias, for households without access to a mobile phone, provisions will be made for research assistants to travel to the households and conduct the interviews while observing all COVID-19 preventive measures.
However, because of COVID-19, some households may be under quarantine or isolation at the time of data collection and may have to be excluded from the study. This creates potential for bias in the selection of participants and may limit the generalisability of study findings. Nonetheless, findings from this study will generate evidence about the effectiveness of a social mobilisation approach on COVID-19 misinformation and vaccine hesitancy in a rural part of Uganda, amidst the COVID-19 pandemic. Furthermore, the study will provide useful information about the feasibility of virtual data collection in a resource-limited setting.
Informed by the baseline assessment in the study, strategies that have been reported to be effective in addressing vaccine hesitancy will be adapted. One study has highlighted the role of healthcare workers as critical vehicles to address vaccine hesitancy.21 Thus, our interventions will explore building the capacity and awareness of the healthcare workers to address the COVID-19 misinformation and vaccine hesitancy among the community. We shall aim to improve their communication skills and ability to fact-check and keep up to date with the latest evidence. They will be encouraged to assess continuously knowledge gaps, needs and concerns of potential vaccination beneficiaries, and to share and discuss information the disease risk and severity, the COVID-19 vaccine’s effectiveness and safety; and to provide the practical information about how to access vaccines.
Additional studies have identified minority groups to be at higher risk of vaccine hesitancy and lower vaccine uptake than the rest of the population.22 Therefore, our interventions will endeavour to address the explanatory barriers that may include factors such as pre-existing mistrust of formal services, lack of information about the vaccine’s safety, misinformation, inaccessible communications, and lack of access logistical issues. Borrowing from the findings from the baseline assessment, the interventions will adapt aspects of inclusive communications through trusted communicators and increasing visibility of minority ethnic groups in the media and use of healthcare networks. Additional studies have affirmed that interventions are more effective the targeted beneficiaries are involved with the topic using text-only mitigation.23
Ethics statements
Patient consent for publication
Acknowledgments
The authors are grateful to Dr Alfred Driwale and Dr Immaculate Ampaire of the Uganda National Expanded Program on Immunisation (UNEPI), Uganda Ministry of Health, the District Health Office in Buikwe district and Makerere University for the guidance and technical support to this initiative.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @fredkitutu
Contributors JNS and FEK conceived the idea, applied for funding and conceptualised the study and are responsible for drafting the manuscript and incorporating feedback. RK, RO and JK read the early versions manuscript and refined the research plan and helped to refine the study design and edited the manuscript. All authors provided editorial assistance with the manuscript preparation, read and approved the final manuscript.
Funding This research is funded by the Social and Behavioral Interventions for Vaccination Acceptance Small Grants Program, Sabin Vaccine Institute, Washington DC, USA, Letter of Agreement number 050112-00 titled, ‘Using community influencer groups to address COVID-19 misinformation and vaccine hesitancy in Buikwe, Uganda’.
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Makerere University is the primary employer of the investigators and as such provided salary support to them.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.