
The Quality of Medical Care in the Conditions of the COVID-19 Pandemic, with Particular Emphasis on the Access to Primary Healthcare and the Effectiveness of Treatment in Poland


Abstract
:1. Introduction
- efficacy—the ability to produce the desired amount of the desired effect, i.e., success in achieving a specific goal;
- effectiveness—the degree to which the planned results, objectives or tasks are achieved as a result of an action, intervention or initiative aimed at achieving the desired effect, in ordinary, uncontrolled circumstances;
- efficiency—doing things in the most economical way. It is the ratio of performance to the inputs of any system [43].
2. Materials and Methods
2.1. Methodology
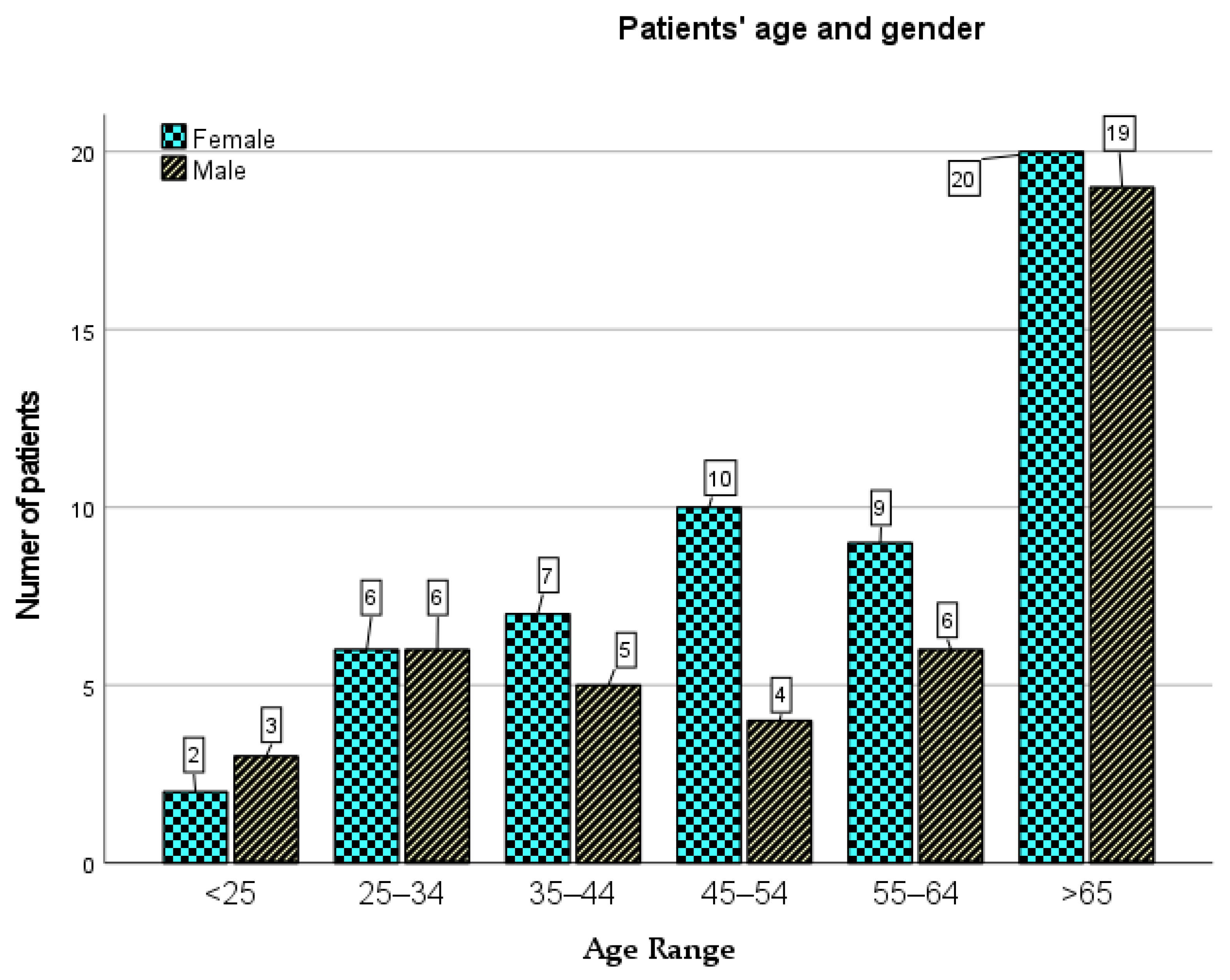
2.1.1. Population and Data Collection
2.1.2. Patient Satisfaction Questionnaire
2.1.3. Ethics
3. Results
3.1. Data Analysis
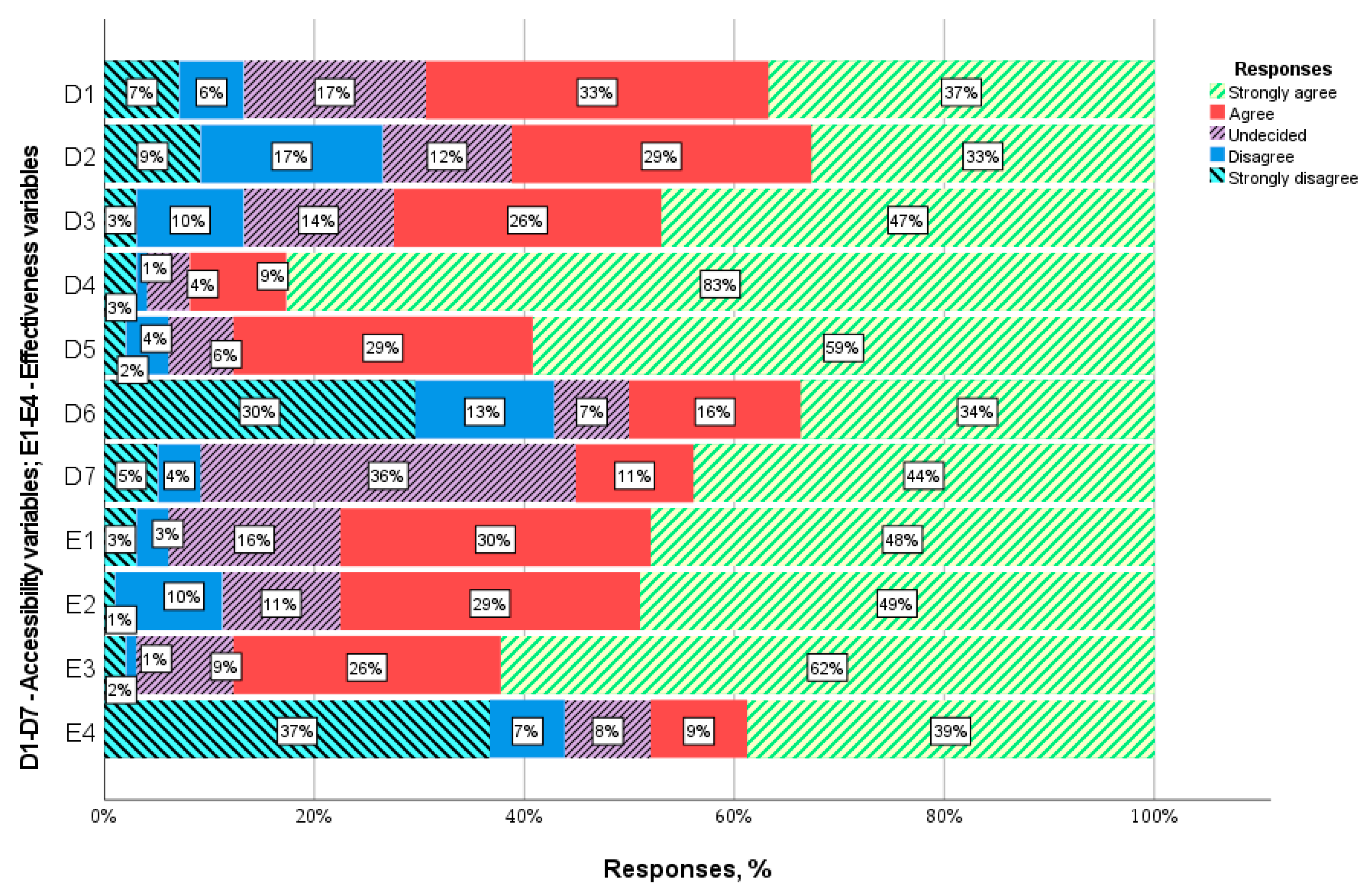
3.1.1. Accessibility
3.1.2. Effectiveness
3.2. Factor Analysis
3.2.1. Exploratory Factor Analysis
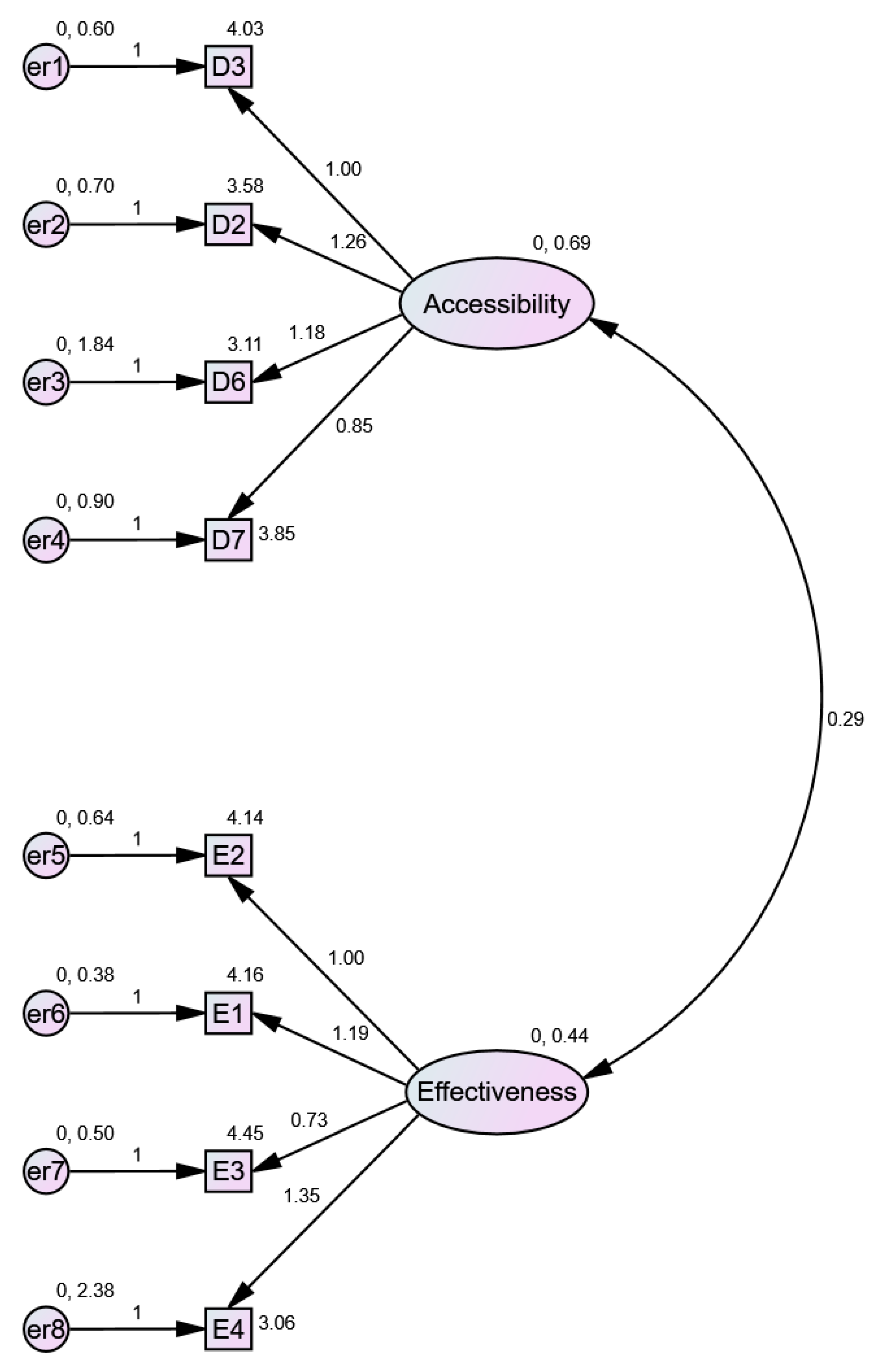
3.2.2. Confirmatory Factor Analysis
3.2.3. Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanecki, K.; Nitsch-Osuch, A.; Tyszko, P. Health-Related Quality of Life or Quality of Medical Service? Current challenges for family doctors. Fam. Med. Prim. Care Rev. 2016, 18, 382–386. [Google Scholar] [CrossRef] [Green Version]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.; Andersen, M.; Beisland, E.; Borge, C.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, J.P.; Kalmijn, S.; Lindeman, E.; Veldink, J.H.; de Visser, M.; Van der Graaff, M.M.; Wokke, J.H.J.; Van den Berg, L.H. Multidisciplinary ALS care improves quality of life in patients with ALS. Neurology 2005, 65, 1264–1267. [Google Scholar] [CrossRef]
- Glimelius, B.; Hoffman, K.; Sjödén, P.O.; Jacobsson, G.; Sellström, H.; Enander, L.K.; Linné, T.; Svensson, C. Chemotherapy improves survival and quality of life in advanced pancreatic and biliary cancer. Ann. Oncol. 1996, 7, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Crosby, R.D.; Kolotkin, R.L.; Williams, G.R. Defining clinically meaningful change in health-related quality of life. J. Clin. Epidemiol. 2003, 56, 395–407. [Google Scholar] [CrossRef]
- Constitution of the World Health Organization. Chron. World Health Organ; Constitution of the World Health Organization: Geneva, Switzerland, 1947; Volume 1. [Google Scholar]
- Raphael, D.; Renwick, R.; Brown, I.; Rootman, I. Quality of life indicators and health: Current status and emerging conceptions. Soc. Indic. Res. 1996, 39, 65–88. [Google Scholar] [CrossRef]
- Hollandsworth, J.G. Evaluating the impact of medical treatment on the quality of life: A 5-year update. Soc. Sci. Med. 1988, 26, 425–434. [Google Scholar] [CrossRef]
- Erikson, R. Description of inequality: The Swedish approach to welfare research. In The Quality of Life; Oxford University Press: Oxford, UK, 1993. [Google Scholar]
- Adler, N.E.; Boyce, W.T.; Chesney, M.A.; Folkman, S.; Syme, S.L. Socioeconomic Inequalities in Health: No Easy Solution. JAMA J. Am. Med. Assoc. 1993, 269, 3140–3145. [Google Scholar] [CrossRef]
- Donabedian, A. Twenty years of research on the quality of medical care: 1964–1984. Eval. Health Prof. 1985, 8, 243–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascoe, G.C. Patient satisfaction in primary health care: A literature review and analysis. Eval. Program Plann. 1983, 6, 185–210. [Google Scholar] [CrossRef]
- Van Campen, C.; Sixma, H.; Friele, R.D.; Kerssens, J.J.; Peters, L. Quality of Care and Patient Satisfaction: A Review of Measuring Instruments. Med. Care Res. Rev. 1995, 52, 109–133. [Google Scholar] [CrossRef] [PubMed]
- Strasser, S.; Aharony, L.; Greenberger, D. The Patient Satisfaction Process: Moving Toward a Comprehensive Model. Med. Care Res. Rev. 1993, 50, 219–248. [Google Scholar] [CrossRef] [PubMed]
- Revicki, D.A.; Osoba, D.; Fairclough, D.; Barofsky, I.; Berzon, R.; Leidy, N.K.; Rothman, M. Recommendations on health-related quality of life research to support labeling and promotional claims in the United States. Qual. Life Res. 2000, 9, 887–900. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.J.; Lin, I.M.; Fan, S.Y. Methodological issues in measuring health-related quality of life. Tzu Chi Med. J. 2013, 25, 8–12. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization. WHOQOL-Measuring Quality of Life; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Campbell, S.M.; Roland, M.O.; Buetow, S.A. Defining quality of care. Soc. Sci. Med. 2000, 51, 1611–1625. [Google Scholar] [CrossRef]
- Maxwell, R.J. Quality assessment in health. Br. Med. J. 1984, 288, 1470–1472. [Google Scholar] [CrossRef] [Green Version]
- Alonazi, W.B.; Thomas, S.A. Quality of Care and Quality of Life: Convergence or Divergence? Health Serv. Insights 2014, 7, 13283. [Google Scholar] [CrossRef]
- L’Esperance, V.; Sutton, M.; Schofield, P.; Round, T.; Malik, U.; White, P.; Ashworth, M. Impact of primary care funding on secondary care utilisation and patient outcomes: A retrospective cross-sectional study of English general practice. Br. J. Gen. Pract. 2017, 67, 792–799. [Google Scholar] [CrossRef] [Green Version]
- Chmiel, M. Quality Attributes of Primary Health Care Services. Sci. Pap. Silesian Univ. Technol. Organ. Manag. Ser. 2019, 2019, 7–16. [Google Scholar] [CrossRef]
- Korneta, P. Stakeholders and Performance Management Systems of Small and Medium-Sized Outpatient Clinics. Found. Manag. 2020, 12, 211–222. [Google Scholar] [CrossRef]
- Korneta, P.; Kludacz-Alessandri, M.; Walczak, R. The impact of COVID-19 on the performance of primary health care service providers in a capitation payment system: A case study from Poland. Int. J. Environ. Res. Public Health 2021, 18, 1407. [Google Scholar] [CrossRef]
- Jakubowski, D.; Sys, D.; Kajdy, A.; Lewandowska, R.; Kwiatkowska, E.; Cymbaluk-Płoska, A.; Rabijewski, M.; Torbé, A.; Kwiatkowski, S. Application of Telehealth in Prenatal Care during the COVID-19 Pandemic—A Cross-Sectional Survey of Polish Women. J. Clin. Med. 2021, 10, 2570. [Google Scholar] [CrossRef]
- Major, P.; Stefura, T.; Wysocki, M.; Małczak, P.; Rzepa, A.; Proczko-Stepaniak, M.; Szeliga, J.; Pędziwiatr, M. Impact of SARS-CoV-2 pandemic on bariatric care in Poland: Results of national survey. BMC Surg. 2020, 20, 314. [Google Scholar] [CrossRef]
- Konieczny, M.; Cipora, E.; Sawicka, J.; Fal, A. Patient satisfaction with oncological care during the SARS-CoV-2 virus pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4122. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, J.; Biernat, K.; Kuciel, N.; Hap, K.; Sutkowska, E. The use of medical and non-medical services by the elderly during the SARS-CoV-2 pandemic differs between general and specialist practice: A one-center study in Poland. Healthcare 2021, 9, 8. [Google Scholar] [CrossRef]
- Wysocki, P.J.; Kwinta, Ł.; Potocki, P.; Konopka, K.; Streb, J.; Wojtukiewicz, M.Z.; Radecka, B.; Tomczak, P.; Jarząb, M.; Kawecki, A.; et al. Systemic treatment of patients with solid tumors during the COVID-19 (SARS-CoV-2) pandemic-comprehensive recommendations of the Polish Society of Clinical Oncology. Oncol. Clin. Pract. 2020, 16, 41–52. [Google Scholar] [CrossRef]
- Malicki, J.; Martenka, P.; Dyzmann-Sroka, A.; Paczkowska, K.; Leporowska, E.; Suchorska, W.; Lamperska, K.; Pieńkowski, P.; Chicheł, A.; Mocydlarz-Adamcewicz, M.; et al. Impact of COVID-19 on the performance of a radiation oncology department at a major comprehensive cancer centre in Poland during the first ten weeks of the epidemic. Rep. Pract. Oncol. Radiother. 2020, 25, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Maluchnik, M.; Podwójcic, K.; Więckowska, B. Decreasing access to cancer diagnosis and treatment during the COVID-19 pandemic in Poland. Acta Oncol. 2021, 60, 28–31. [Google Scholar] [CrossRef]
- Zduńczyk, A.J.; Jakubiak, A.; Łuczak, J. Raport Podstawowa Opieka Zdrowotna w Polsce-Diagnoza i Projekty Zmian; Instytut Medycyny Wsi im: Lublin, Poland, 2018. [Google Scholar]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of primary care to health systems and health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef]
- Bower, P.; Roland, M.; Campbell, J.; Mead, N. Setting standards based on patients’ views on access and continuity: Secondary analysis of data from the general practice assessment survey. Br. Med. J. 2003, 326, 258–260. [Google Scholar] [CrossRef] [Green Version]
- Campbell, S.M.; Hann, M.; Hacker, J.; Burns, C.; Oliver, D.; Thapar, A.; Mead, N.; Gelb Safran, D.; Roland, M.O. Identifying predictors of high quality care in English general practice: Observational study. Br. Med. J. 2001, 323, 784–787. [Google Scholar] [CrossRef] [Green Version]
- Cankurtaran, D.; Tezel, N.; Yildiz, S.Y.; Celik, G.; Unlu Akyuz, E. Evaluation of the effects of the COVID-19 pandemic on children with cerebral palsy, caregivers’ quality of life, and caregivers’ fear of COVID-19 with telemedicine. Ir. J. Med. Sci. 2021, 1–8. [Google Scholar] [CrossRef]
- Whitehead, M. The concepts and principles of equity and health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.M.; McCutcheon, A.; Aday, L.A.; Chiu, G.Y.; Bell, R. Exploring dimensions of access to medical care. Health Serv. Res. 1983, 18, 49–74. [Google Scholar] [PubMed]
- Hawrysz, L.; Gierszewska, G.; Bitkowska, A. The research on patient satisfaction with remote healthcare prior to and during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5338. [Google Scholar] [CrossRef] [PubMed]
- Gordon, T.; Booysen, F.; Mbonigaba, J. Socio-economic inequalities in the multiple dimensions of access to healthcare: The case of South Africa. BMC Public Health 2020, 20, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haggerty, J.; Burge, F.; Lévesque, J.F.; Gass, D.; Pineault, R.; Beaulieu, M.D.; Santor, D. Operational definitions of attributes of primary health care: Consensus among Canadian experts. Ann. Fam. Med. 2007, 5, 336–344. [Google Scholar] [CrossRef]
- Drucker, P.F. The Effective Executive; Harper & Row: New York, NY, USA, 1967. [Google Scholar]
- Palmer, S.; Torgerson, D.J. Economics notes: Definitions of efficiency. BMJ Br. Med. J. 1999, 318, 1136. [Google Scholar] [CrossRef]
- Rezapour, R.; Tabrizi, J.S.; Farahbakhsh, M.; Saadati, M.; Abdolahi, H.M. Developing Iranian primary health care quality framework: A national study. BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Burches, E.; Burches, M. Efficacy, Effectiveness and Efficiency in the Health Care: The Need for an Agreement to Clarify its Meaning. Int. Arch. Public Health Community Med. 2020, 4, 35. [Google Scholar] [CrossRef]
- Głodziński, E. Efektywność Ekonomiczna—Dylematy Definiowania i Pomiaru Economic Efficiency—Dilemmas in Definition and Measurement; Zeszyty Naukowe. Organizacja i Zarządzanie/Politechnika Śląska. 2014; z. 73. pp. 155–167. Available online: https://yadda.icm.edu.pl/baztech/element/bwmeta1.element.baztech-9f73d895-2539-49fc-a3f4-5ccb3d7be1be (accessed on 15 June 2021).
- World Health Organization. Quality in Primary Health Care; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Agency for Healthcare Research and Quality. National Healthcare Quality and Disparities Reports; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2018.
- (CIHI) Canadian Institute for Health Information. Pan-Canadian Primary Health Care Indicator Update Report. 2012, p. 186. Available online: https://secure.cihi.ca/estore/productFamily.htm?locale=en&pf=PFC2000 (accessed on 15 June 2021).
- Australian Commission on Safety and Quality in Health Care. Practice-Level Indicators of Safety and Quality for Primary Health Care; Australian Commission on Safety and Quality in Health Care: Australia, 2012. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/practice-level-indicators-safety-and-quality-primary-health-care-synthesis-submission-consultation-paper-and-recommended-national-indicator-set (accessed on 15 June 2021).
- Langbecker, D.; Caffery, L.J.; Gillespie, N.; Smith, A.C. Using survey methods in telehealth research: A practical guide. J. Telemed. Telecare 2017, 23, 770–779. [Google Scholar] [CrossRef]
- Raczyńska, E. Efektywność w ochronie zdrowaia jako wyzwanie dla zarządzania. Przegląd Organ. 2020, 5, 27–34. [Google Scholar] [CrossRef]
- Testa, M.A.; Simonson, D.C. Assessment of Quality-of-Life Outcomes. N. Engl. J. Med. 1996, 334, 835–840. [Google Scholar] [CrossRef]
- Gill, T.M.; Feinstein, A.R. A Critical Appraisal of the Quality of Quality-of-Life Measurements. JAMA J. Am. Med. Assoc. 1994, 272, 619–626. [Google Scholar] [CrossRef]
- Wilcox, L.D.; Brooks, R.M.; Beal, G.M.; Klonglan, G.E. Social Indicators and Societal Monitoring: An Annotated Bibliography; Jossey-Bass Inc. Publishers: San Francisco, CA, USA, 1972. [Google Scholar]
- Aday, L.A.; Andersen, R. A framework for the study of access to medical care. Health Serv. Res. 1974, 9, 208–220. [Google Scholar]
- Gene-Badia, J.; Ascaso, C.; Escaramis-Babiano, G.; Sampietro-Colom, L.; Catalan-Ramos, A.; Sans-Corrales, M.; Pujol-Ribera, E. Personalised care, access, quality and team coordination are the main dimensions of family medicine output. Fam. Pract. 2006, 24, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corscadden, L.; Levesque, J.-F.; Lewis, V.; Breton, M.; Sutherland, K.; Weenink, J.-W.; Haggerty, J.; Russell, G. Barriers to accessing primary health care: Comparing Australian experiences internationally. Aust. J. Prim. Health 2017, 23, 223. [Google Scholar] [CrossRef] [Green Version]
- Engels, Y. Developing a framework of, and quality indicators for, general practice management in Europe. Fam. Pract. 2005, 22, 215–222. [Google Scholar] [CrossRef]
- McIntyre, D.; Thiede, M.; Birch, S. Access as a policy-relevant concept in low- and middle-income countries. Health Econ. Policy Law 2009, 4, 179–193. [Google Scholar] [CrossRef]
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, K.; Yip, W.C.; Hsiao, W. The impact of quality on the demand for outpatient services in Cyprus. Health Econ. 2004, 13, 1167–1180. [Google Scholar] [CrossRef] [PubMed]
- Sans-Corrales, M. Family medicine attributes related to satisfaction, health and costs. Fam. Pract. 2006, 23, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, B.S.; Seidman, D.; Berger, N.; Cascetta, K.P.; Nezolosky, M.; Trlica, K.; Ryncarz, A.; Keeton, C.; Moshier, E.; Tiersten, A. Patient perception of telehealth services for breast and gynecologic oncology care during the COVID-19 pandemic: A single center survey-based study. J. Breast Cancer 2020, 23, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis; Pearson Education, Limited: London, UK, 2013. [Google Scholar]
- Sapsford, R. Survey Research; SAGE Publications: New York, NY, USA, 2006. [Google Scholar]
- Johnson, T.P. Handbook of Health Survey Methods; John Wiley & Sons, Incorporated: Hoboken, NJ, USA, 2014. [Google Scholar]
- Punch, K.F. Survey Research: The Basics; Sage Publications: New York, NY, USA, 2003. [Google Scholar]
- Davies, H.; Powell, A.; Rushmer, R. Healthcare Professionals’ Views on Clinician Engagement in Quality Improvement: A Literature Review. 2007. Available online: https://www.health.org.uk/publications/healthcare-professionals%E2%80%99-views-on-clinician-engagement-in-quality-improvement (accessed on 15 June 2021).
- Caccia-Bava, M.C.; Guimaraes, V.C.K.; Guimaraes, T. Important factors for success in hospital BPR project phases. Int. J. Health Care Qual. Assur. 2013, 26, 729–745. [Google Scholar] [CrossRef]
- Hennington, A.; Janz, B.; Poston, R. I’m just burned out: Understanding information system compatibility with personal values and role-based stress in a nursing context. Comput. Hum. Behav. 2011, 27, 1238–1248. [Google Scholar] [CrossRef]
- De Ryck, E.; Willems, S. Erratum: Measures of quality, costs and equity in primary healthcare: Instruments developed to analyse and compare primary healthcare in 35 countries (Quality in Primary Care (2013) 21:2 (67–79)). Qual. Prim. Care 2013, 21, 205. [Google Scholar]
- Lai, H.; Gemming, L. Approaches to patient satisfaction measurement of the healthcare food services: A systematic review. Clin. Nutr. ESPEN 2021, 42, 61–72. [Google Scholar] [CrossRef]
- European Patients Forum. Patients’ Perceptions of Quality in Healthcare: Report of a survey conducted by EPF in 2016. Report in a Survey. 2017, p. 40. Available online: https://www.eu-patient.eu/globalassets/policy/quality-of-care/quality-survey-report.pdf (accessed on 15 June 2021).
- Bargawi, A.A.; Rea, D.M. Quality in Primary Health Care. Health Policy Plan. 2015, pp. 37–40. Available online: https://www.who.int/docs/default-source/primary-health-care-conference/quality.pdf (accessed on 15 June 2021).
- Shield, T.; Campbell, S.; Rogers, A.; Worrall, A.; Chew-Graham, C.; Gask, L. Quality indicators for primary care mental health services. Qual. Saf. Health Care 2003, 12, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Busse, R.; Klazinga, N.; Panteli, D.; Quentin, W. Improving Healthcare Quality in Europe; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics; Pearson Education: Upper Saddle River, NJ, USA, 2018; ISBN 9780134792859. [Google Scholar]
- Horn, J.L. Factors in Factor Analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Zhang, X.; Xiang, S. Learn About Reliability Analysis and Factor Analysis in SPSS With Online Shopping Data; SAGE Publications: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Williams, B.; Onsman, A.; Brown, T. Exploratory factor analysis: A five-step guide for novices. J. Emerg. Prim. Health Care 2010, 8, 225–236. [Google Scholar] [CrossRef] [Green Version]
- Kludacz-Alessandri, M.; Hawrysz, L.; Korneta, P.; Gierszewska, G.; Pomaranik, W.; Walczak, R. The impact of medical teleconsultations on general practitioner-patient communication during COVID- 19: A case study from Poland. PLoS ONE 2021, 16, e0254960. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, W.; Zhou, K.; Waddell, E.; Myers, T.; Dorsey, E.R. Improving Access to Care: Telemedicine across Medical Domains. In Annual Review of Public Health; Annual Reviews Inc.: Palo Alto, CA, USA, 2020; Volume 42, pp. 463–481. [Google Scholar]
- Grol, R.; Wensing, M. Patients Evaluate General/Family Practice: The EUROPEP Instrument; 2000. Available online: https://equip.woncaeurope.org/sites/equip/files/documents/publications/resources/grolwensing2000theeuropepinstrumentequipwonca.pdf (accessed on 15 June 2021).
- Smith, C.H.; Armstrong, D. Comparison of criteria derived by government and patients for evaluating general practitioner services. Br. Med. J. 1989, 299, 494–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekeland, A.G.; Bowes, A.; Flottorp, S. Effectiveness of telemedicine: A systematic review of reviews. Int. J. Med. Inform. 2010, 79, 736–771. [Google Scholar] [CrossRef] [Green Version]
- Champagne-Langabeer, T.; Langabeer, J.R.; Roberts, K.E.; Gross, J.S.; Gleisberg, G.R.; Gonzalez, M.G.; Persse, D. Telehealth Impact on Primary Care Related Ambulance Transports. Prehospital Emerg. Care 2019, 23, 712–717. [Google Scholar] [CrossRef] [PubMed]
- de Catapan, S.C.; Calvo, M.C.M. Teleconsultation: An Integrative Review of the Doctor-Patient Interaction Mediated by Technology. Rev. Bras. Educ. Med. 2020, 44. [Google Scholar] [CrossRef]
- Newbould, J.; Abel, G.; Ball, S.; Corbett, J.; Elliott, M.; Exley, J.; Martin, A.; Saunders, C.; Wilson, E.; Winpenny, E.; et al. Evaluation of telephone first approach to demand management in English general practice: Observational study. BMJ 2017, 358, 4197. [Google Scholar] [CrossRef] [Green Version]
- Moth, G.; Huibers, L.; Christensen, M.B.; Vedsted, P. Drug prescription by telephone consultation in Danish out-of-hours primary care: A population-based study of frequency and associations with clinical severity and diagnosis. BMC Fam. Pract. 2014, 15, 142. [Google Scholar] [CrossRef] [Green Version]
- Dawson, A.Z.; Walker, R.J.; Campbell, J.A.; Davidson, T.M.; Egede, L.E. Telehealth and indigenous populations around the world: A systematic review on current modalities for physical and mental health. mHealth 2020, 6, 30. [Google Scholar] [CrossRef]
- Morris, J.; Campbell-Richards, D.; Wherton, J.; Sudra, R.; Vijayaraghavan, S.; Greenhalgh, T.; Collard, A.; Byrne, E.; O’Shea, T. Webcam consultations for diabetes: Findings from four years of experience in Newham. Pract. Diabetes 2017, 34, 45–50. [Google Scholar] [CrossRef]
- Haig-Ferguson, A.; Loades, M.; Whittle, C.; Read, R.; Higson-Sweeney, N.; Beasant, L.; Starbuck, J.; Crawley, E. “It’s not one size fits all”; the use of videoconferencing for delivering therapy in a Specialist Paediatric Chronic Fatigue Service. Internet Interv. 2019, 15, 43–51. [Google Scholar] [CrossRef]
- Chwistek, M. “are You Wearing Your White Coat?”: Telemedicine in the Time of Pandemic. JAMA J. Am. Med. Assoc. 2020, 324, 149–150. [Google Scholar] [CrossRef]
- Sutherland, A.E.; Stickland, J.; Wee, B. Can video consultations replace face-to-face interviews? Palliative medicine and the COVID-19 pandemic: Rapid review. BMJ Support Palliat. Care 2020, 26, 26. [Google Scholar] [CrossRef]
- Wade, V.A.; Karnon, J.; Elshaug, A.G.; Hiller, J.E. A systematic review of economic analyses of telehealth services using real time video communication. BMC Health Serv. Res. 2010, 10, 233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imlach, F.; McKinlay, E.; Middleton, L.; Kennedy, J.; Pledger, M.; Russell, L.; Churchward, M.; Cumming, J.; McBride-Henry, K. Telehealth consultations in general practice during a pandemic lockdown: Survey and interviews on patient experiences and preferences. BMC Fam. Pract. 2020, 21, 269. [Google Scholar] [CrossRef]
- Thornton, J. COVID-19: How coronavirus will change the face of general practice forever. BMJ 2020, 368, m1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raczkiewicz, D.; Kister, A.; Rzemek, C.; Tarkowski, K.; Dybciak, P.; Owoc, A.; Bojar, I. Telemedicine in the opinion of primary health care physicians. Eur. J. Med. Technol. 2018, 2, 43. [Google Scholar]
- Ackerman, M.J.; Filart, R.; Burgess, L.P.; Lee, I.; Poropatich, R.K. Developing next-generation telehealth tools and technologies: Patients, systems, and data perspectives. In Telemedicine and e-Health; NCBI: Bethesda, MD, USA, 2010; Volume 16, pp. 93–95. [Google Scholar]
- Zanaboni, P.; Wootton, R. Adoption of telemedicine: From pilot stage to routine delivery. BMC Med. Inform. Decis. Mak. 2012, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Gomes Rodrigues, D.L.; Belber, G.S.; de Queiroz Padilha, F.V.; Spinel, L.F.; Moreira, F.R.; Maeyama, M.A.; Marques Pinho, A.P.N.; Júnior, Á.A. Impact of teleconsultation on patients with type 2 diabetes in the Brazilian public health system: Protocol for a randomized controlled trial (TELEconsulta diabetes trial). JMIR Res. Protoc. 2021, 10, e23679. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date and Type of the Survey | Total | |||
|---|---|---|---|---|
| February 2021 CATI | March 2021 Paper-Based Survey | |||
| Number of Responses | ||||
| Facility | Warsaw 1 | 0 | 21 | 21 |
| Warsaw 2 | 19 | 0 | 19 | |
| Warsaw 3 | 22 | 19 | 41 | |
| Radom | 24 | 0 | 24 | |
| Total | 65 | 40 | 105 | |
| Variable Name | Question | |
|---|---|---|
| Accessibility | D1 | I can get medical help when I need it, even in case of emergency |
| D2 | I can easily make a telehealth consultation with a General Practitioner (GP) of my choice | |
| D3 | I can easily make an appointment with a GP at the healthcare facility | |
| D4 | The healthcare facility’s working hours are convenient | |
| D5 | Telehealth consultations take place at an agreed time | |
| D6 | I can easily contact the healthcare facility via phone / Internet | |
| D7 | I can easily ask questions after the telehealth consultation | |
| Effectiveness | E1 | The treatment helped me improve my health |
| E2 | The health problem with which I turned to the GP was solved | |
| E3 | The treatment plan proposed by the GP meets my expectations | |
| E4 | The health problem with which I turned to the doctor did not require additional medical consultations with other specialists | |
| Variable | Mean | Skewness | Kurtosis | |||||
|---|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Std. Deviation | Variance | Statistic | Std. Error | Statistic | Std. Error | |
| D1 | 3.8571 | 0.12049 | 1.19276 | 1.423 | −0.983 | 0.244 | 0.202 | 0.483 |
| D2 | 3.5816 | 0.13601 | 1.34642 | 1.813 | −0.565 | 0.244 | −0.966 | 0.483 |
| D3 | 4.0306 | 0.11554 | 1.14382 | 1.308 | −0.989 | 0.244 | −0.023 | 0.483 |
| D4 | 4.6735 | 0.08676 | 0.85886 | 0.738 | −3.098 | 0.244 | 9.634 | 0.483 |
| D5 | 4.3878 | 0.09359 | 0.92650 | 0.858 | −1.807 | 0.244 | 3.223 | 0.483 |
| D6 | 3.1122 | 0.17032 | 1.68610 | 2.843 | −0.127 | 0.244 | −1.703 | 0.483 |
| D7 | 3.8469 | 0.11992 | 1.18715 | 1.409 | −0.603 | 0.244 | −0.505 | 0.483 |
| Variable | Mean | Skewness | Kurtosis | |||||
|---|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Std. Deviation | Variance | Statistic | Std. Error | Statistic | Std. Error | |
| E1 | 4.1633 | 0.10225 | 1.01223 | 1.025 | −1.249 | 0.244 | 1.276 | 0.483 |
| E2 | 4.1429 | 0.10560 | 1.04536 | 1.093 | −1.066 | 0.244 | 0.148 | 0.483 |
| E3 | 4.4490 | 0.08718 | 0.86301 | 0.745 | −1.902 | 0.244 | 4.127 | 0.483 |
| E4 | 3.0612 | 0.18106 | 1.79240 | 3.213 | −0.072 | 0.244 | −1.817 | 0.483 |
| Variable | Component | |
|---|---|---|
| Accessibility | Effectiveness | |
| D3 | 0.804 | |
| D6 | 0.795 | |
| D2 | 0.777 | |
| D7 | 0.686 | |
| E2 | 0.837 | |
| E1 | 0.795 | |
| E3 | 0.645 | |
| E4 | 0.638 | |
| Component | Initial Eigenvalues | Extraction Sums of Squared Loadings | Rotation Sums of Squared Loadings | ||||
|---|---|---|---|---|---|---|---|
| Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % | Total | |
| 1 | 3.185 | 39.809 | 39.809 | 3.185 | 39.809 | 39.809 | 2.711 |
| 2 | 1.374 | 17.178 | 56.987 | 1.374 | 17.178 | 56.987 | 2.551 |
| 3 | 0.841 | 10.512 | 67.499 | ||||
| 4 | 0.725 | 9.069 | 76.568 | ||||
| 5 | 0.564 | 7.055 | 83.623 | ||||
| 6 | 0.527 | 6.594 | 90.216 | ||||
| 7 | 0.474 | 5.921 | 96.137 | ||||
| 8 | 0.309 | 3.863 | 100.000 | ||||
| Correlations | ||||
|---|---|---|---|---|
| D_Accessibility | E_Effectiveness | AVE | ||
| D_Accessibility | Pearson Correlation | 1 | 0.390 ** | 0.461 |
| Sig. (2-tailed) | 0.000 | |||
| N | 98 | 98 | ||
| E_Effectiveness | Pearson Correlation | 0.390 ** | 1 | 0.401 |
| Sig. (2-tailed) | 0.000 | |||
| N | 98 | 98 | ||
| ANOVA a | ||||||
|---|---|---|---|---|---|---|
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 14.762 | 1 | 14.762 | 17.233 | 0.000 b |
| Residual | 82.238 | 96 | 0.857 | |||
| Total | 97.000 | 97 | ||||
| Model Summary b | ||||
|---|---|---|---|---|
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | 0.390 a | 0.152 | 0.143 | 0.92554997 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kludacz-Alessandri, M.; Walczak, R.; Hawrysz, L.; Korneta, P. The Quality of Medical Care in the Conditions of the COVID-19 Pandemic, with Particular Emphasis on the Access to Primary Healthcare and the Effectiveness of Treatment in Poland. J. Clin. Med. 2021, 10, 3502. https://doi.org/10.3390/jcm10163502
Kludacz-Alessandri M, Walczak R, Hawrysz L, Korneta P. The Quality of Medical Care in the Conditions of the COVID-19 Pandemic, with Particular Emphasis on the Access to Primary Healthcare and the Effectiveness of Treatment in Poland. Journal of Clinical Medicine. 2021; 10(16):3502. https://doi.org/10.3390/jcm10163502
Chicago/Turabian StyleKludacz-Alessandri, Magdalena, Renata Walczak, Liliana Hawrysz, and Piotr Korneta. 2021. "The Quality of Medical Care in the Conditions of the COVID-19 Pandemic, with Particular Emphasis on the Access to Primary Healthcare and the Effectiveness of Treatment in Poland" Journal of Clinical Medicine 10, no. 16: 3502. https://doi.org/10.3390/jcm10163502