
Higher Dose Anticoagulation Cannot Prevent Disease Progression in COVID-19 Patients: A Systematic Review and Meta-Analysis
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Search Strategy, Selection Process, and Data Extraction
2.3. Subgroup Analyses
2.4. Risk of Bias and Evidence Level
2.5. Statistical Analysis
3. Results
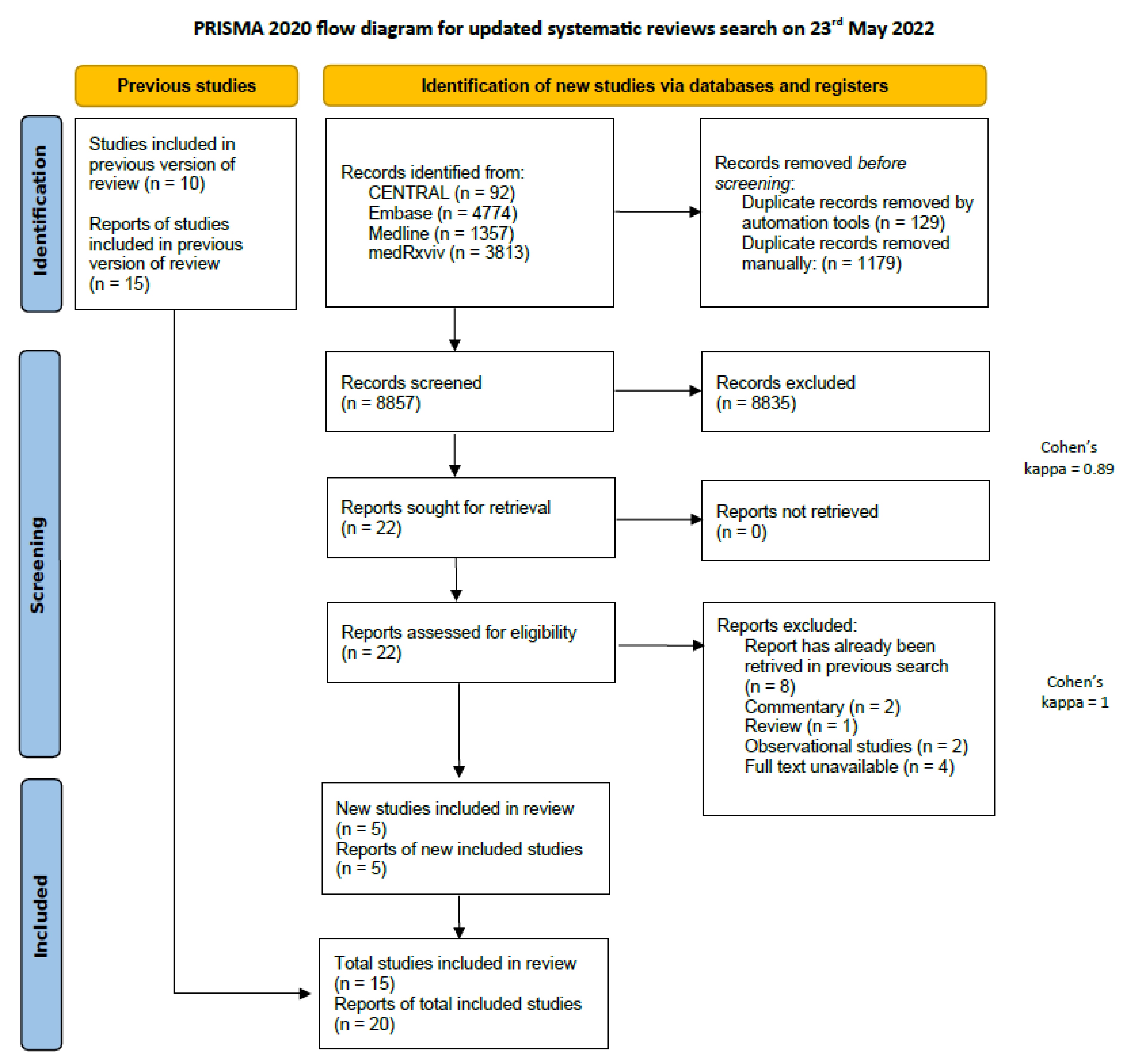
3.1. Systematic Search and Selection
3.2. Study Characteristics
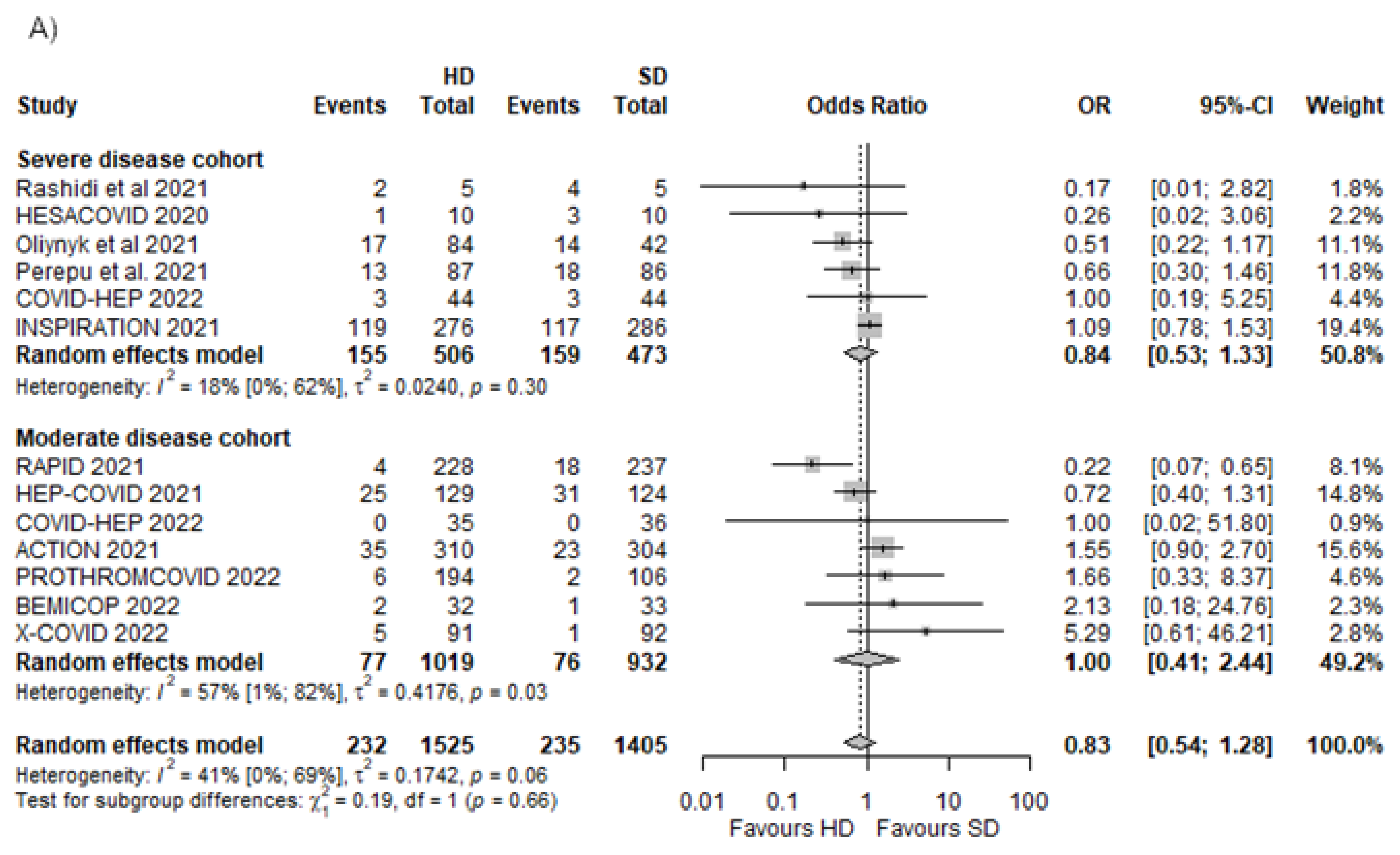
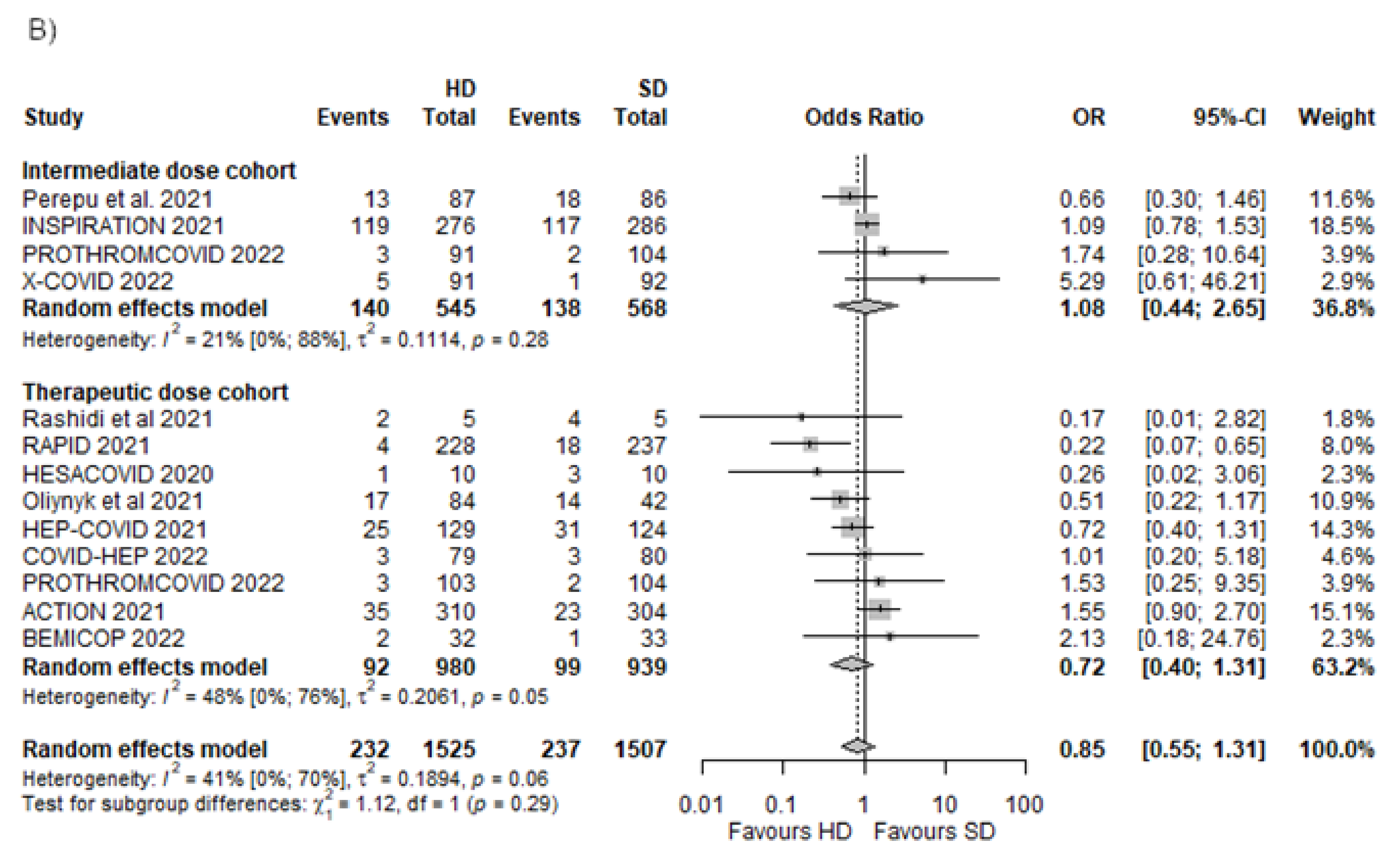
3.3. All-Cause Mortality
3.3.1. Different Dosing Regimens in Moderate and Severe Disease
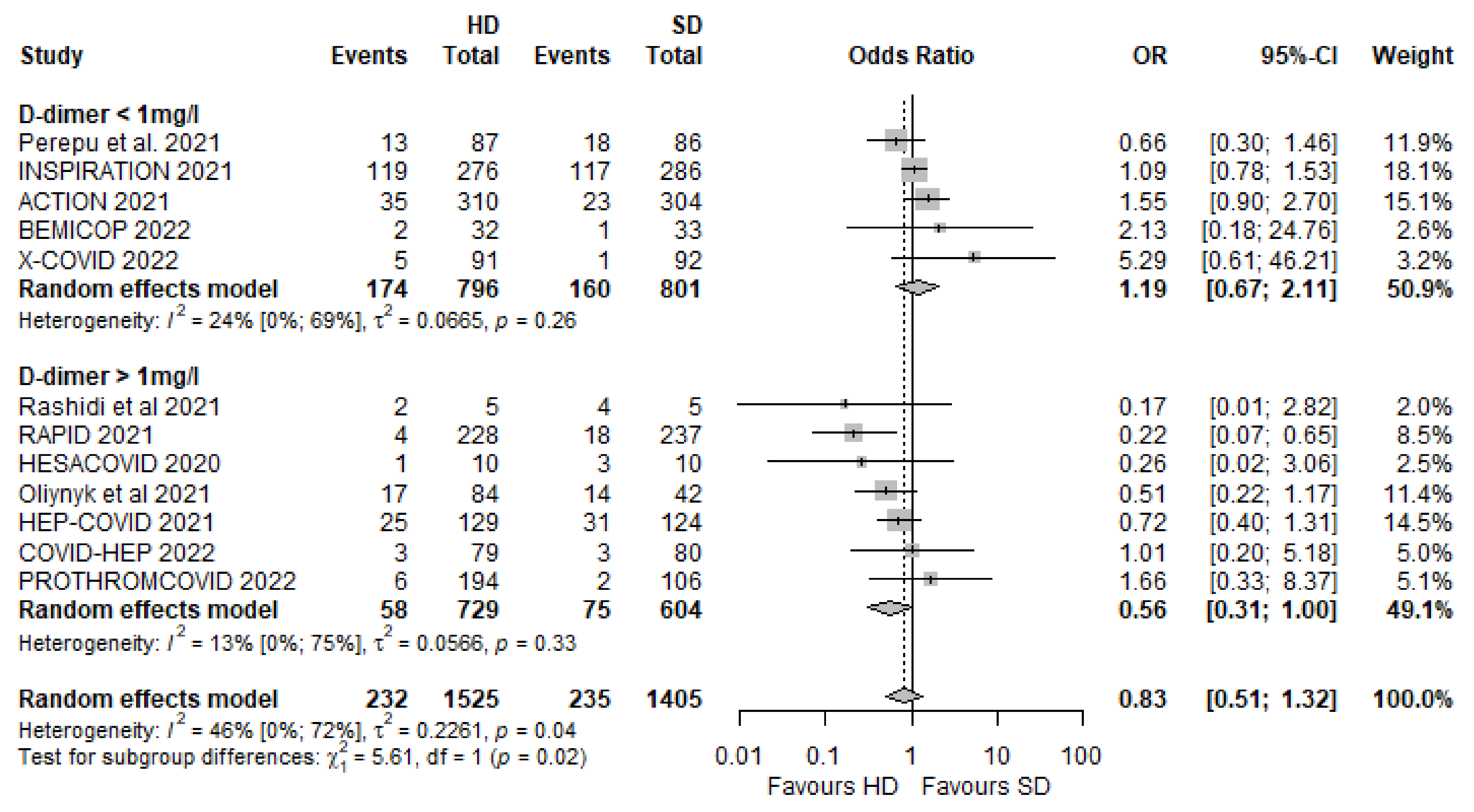
3.3.2. Different D-Dimer Levels in the Included Trials
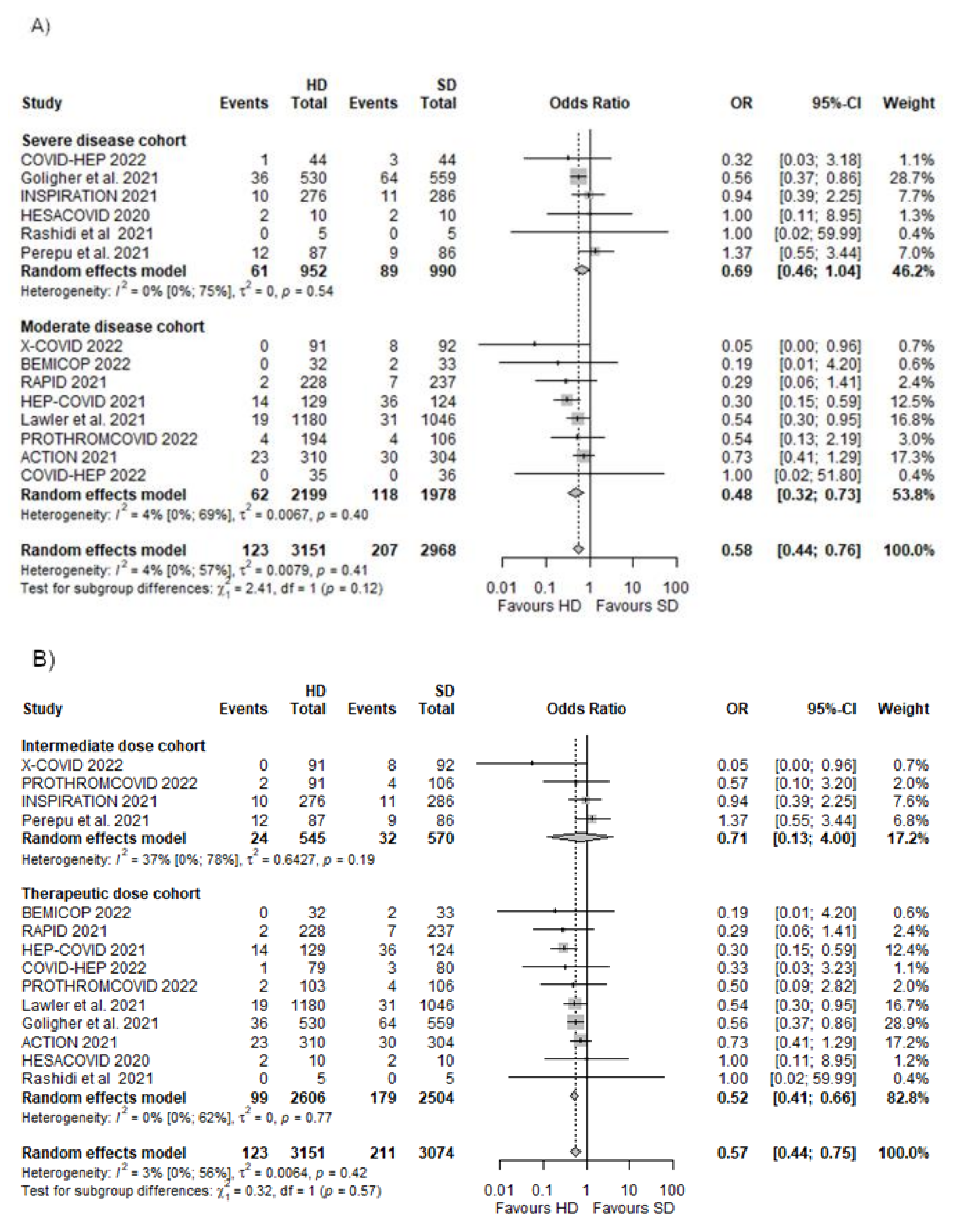
3.4. Any Thrombotic Events
Different Dosing Regimens in Moderate and Severe Disease
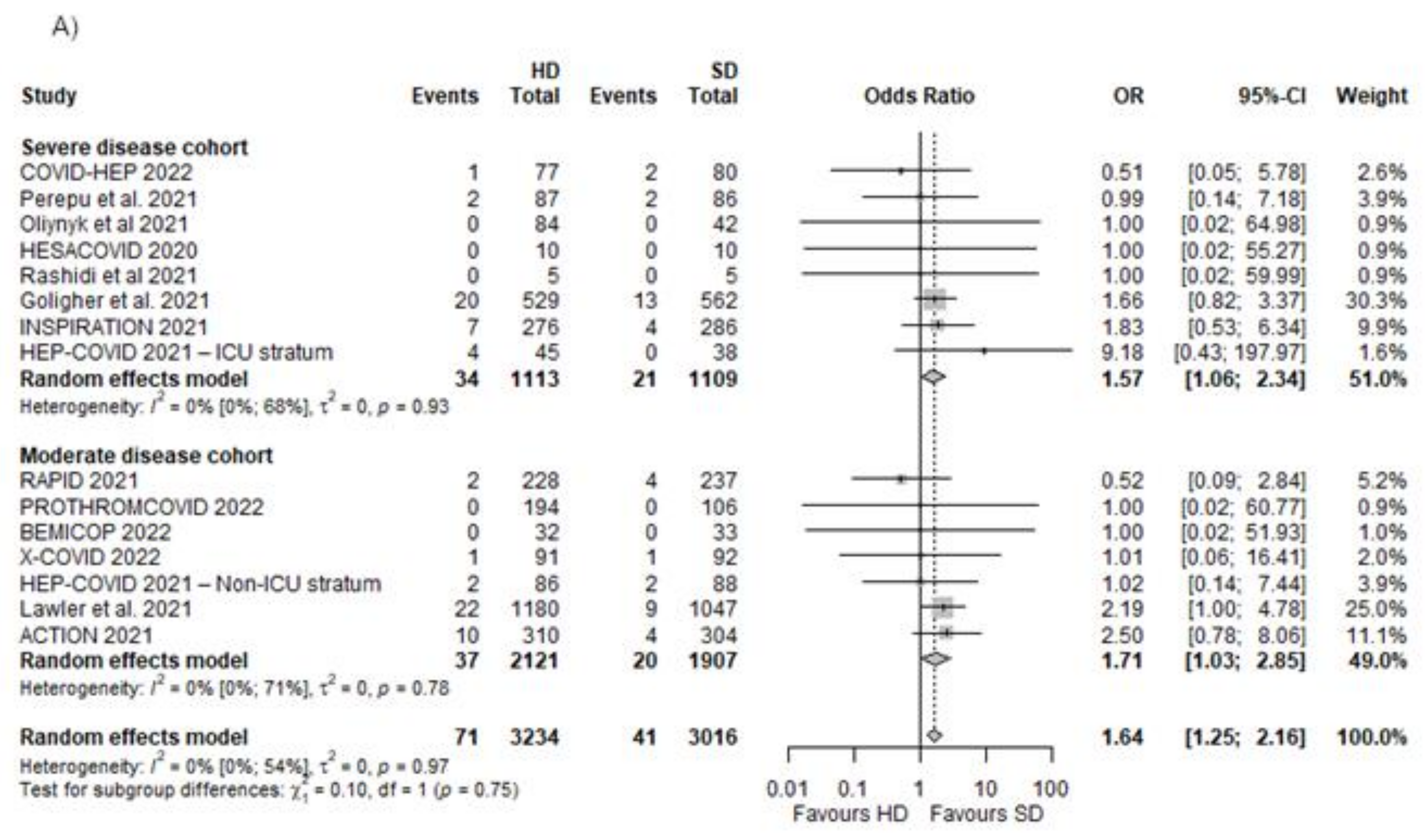
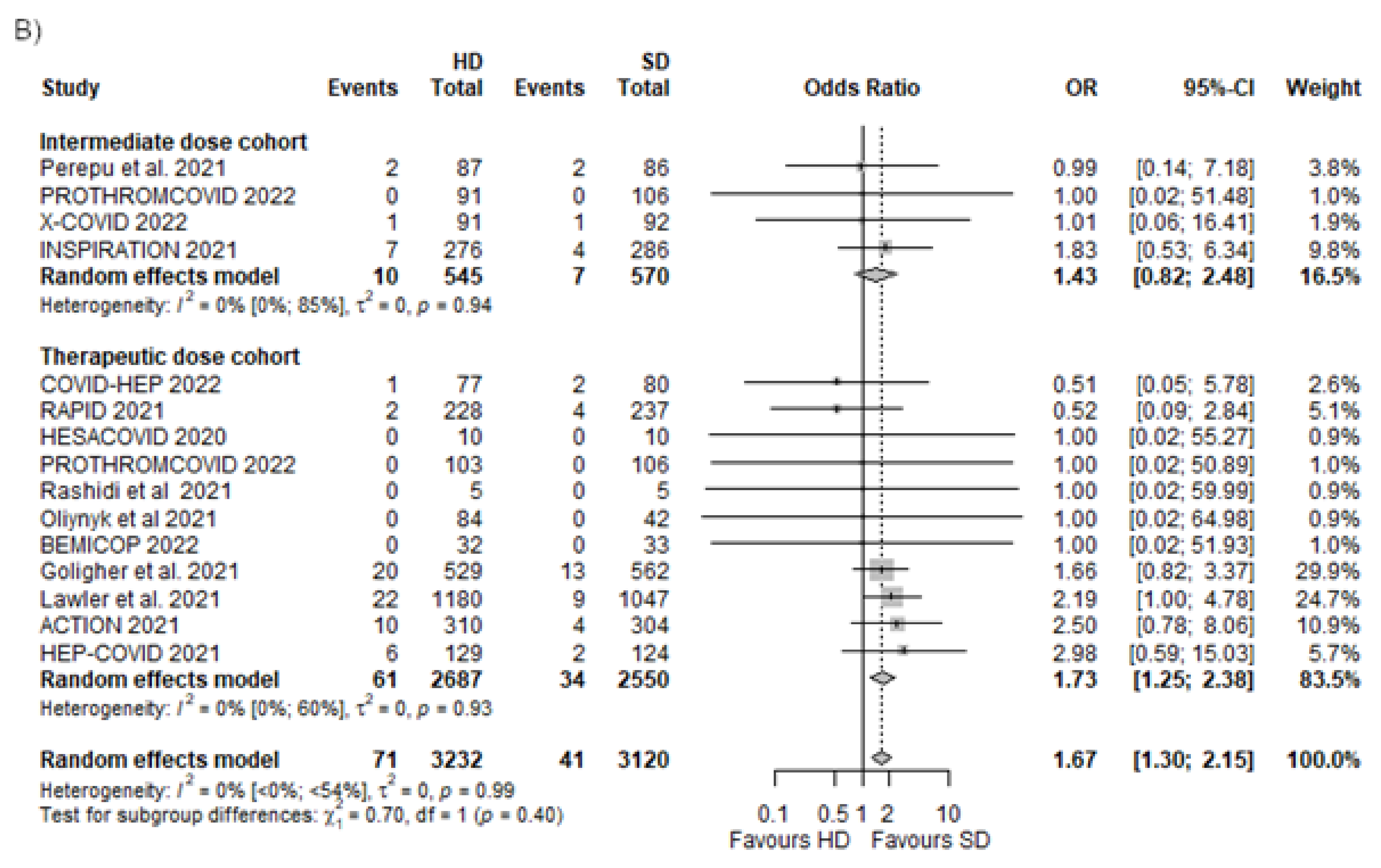
3.5. Major Bleedings
Different Dosing Regimens in Moderate and Severe Disease
3.6. Progression of Disease
3.6.1. Need for Invasive Mechanical Ventilation
3.6.2. Need for ICU Admission
3.6.3. Progression to ARDS
3.6.4. Death, Pulmonary Embolism, and Need for Invasive Mechanical Ventilation
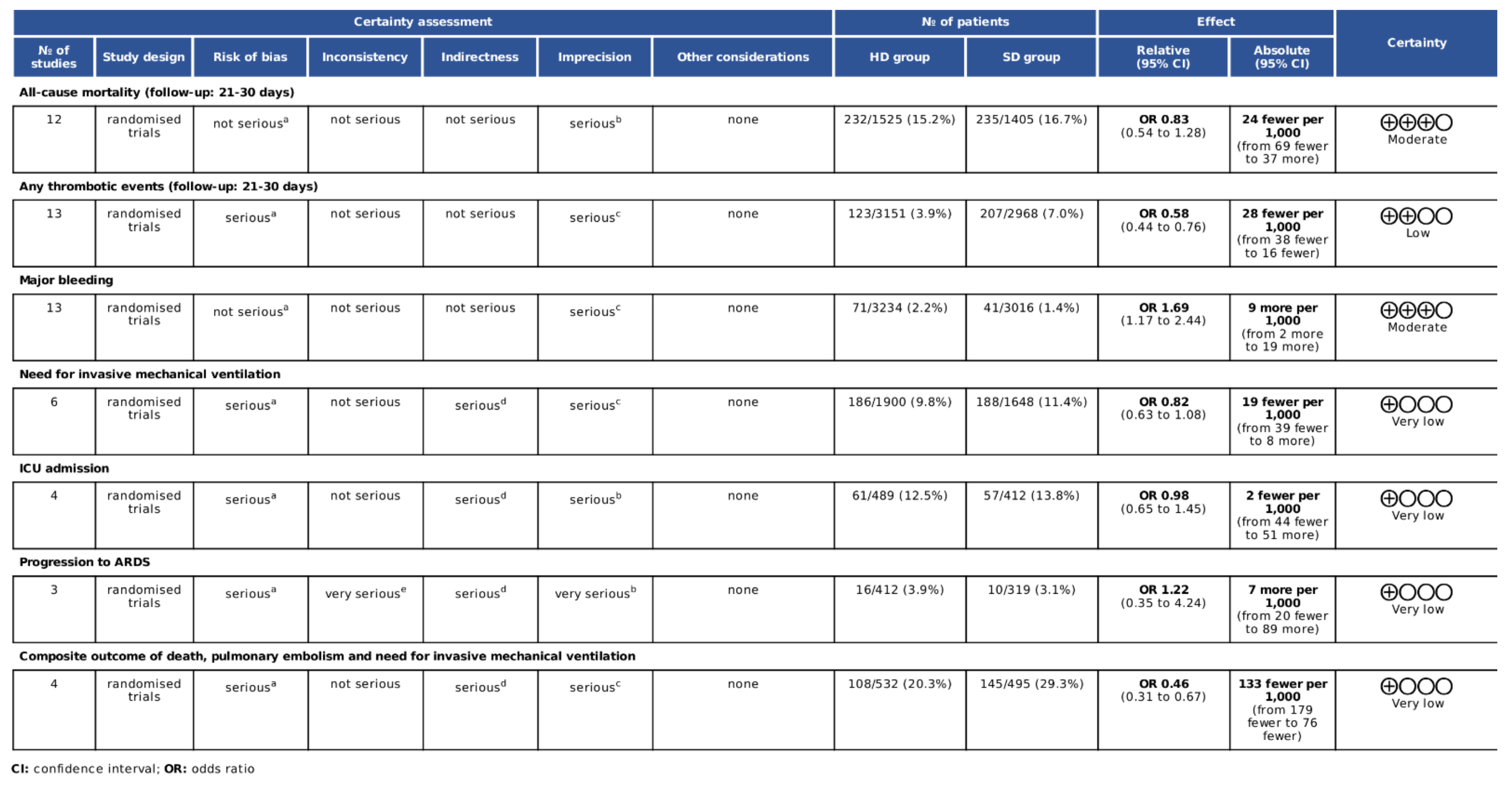
3.7. Assessment of Quality of Evidence
4. Discussion
4.1. Different Dosing Regimens and Disease Severity
4.2. Differences in the Degree of COVID-19-Associated Coagulopathy
4.3. Strengths and Limitations
5. Conclusions and Implications for Practice and Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Y.C.; Kuo, R.L.; Shih, S.R. COVID-19: The first documented coronavirus pandemic in history. Biomed. J. 2020, 43, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Worldometer. Worldometers.info. 2022. Available online: https://www.worldometers.info/coronavirus/ (accessed on 30 July 2022).
- Jenner, W.J.; Gorog, D.A. Incidence of thrombotic complications in COVID-19: On behalf of ICODE: The International COVID-19 Thrombosis Biomarkers Colloquium. J. Thromb. Thrombolysis 2021, 52, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Al-Ani, F.; Chehade, S.; Lazo-Langner, A. Thrombosis risk associated with COVID-19 infection. A scoping review. Thromb. Res. 2020, 192, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Avila, J.; Long, B.; Holladay, D.; Gottlieb, M. Thrombotic complications of COVID-19. Am. J. Emerg. Med. 2021, 39, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Borczuk, A.C. Pulmonary pathology of COVID-19: A review of autopsy studies. Curr. Opin. Pulm. Med. 2021, 27, 184–192. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Li, Y.; Deng, Y.; Ye, L.; Sun, H.; Du, S.; Huang, H.; Zeng, F.; Chen, X.; Deng, G. Clinical Significance of Plasma D-Dimer in COVID-19 Mortality. Front. Med. 2021, 8, 638097. [Google Scholar] [CrossRef]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. 2020, 26, 107602962093814. [Google Scholar] [CrossRef]
- Spyropoulos, A.; Levy, J.; Ageno, W.; Connors, J.; Hunt, B.; Iba, T.; Levi, M.; Samama, C.; Thachil, J.; Giannis, D.; et al. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1859–1865. [Google Scholar] [CrossRef]
- Buijsers, B.; Yanginlar, C.; Maciej-Hulme, M.L.; de Mast, Q.; van der Vlag, J. Beneficial non-anticoagulant mechanisms underlying heparin treatment of COVID-19 patients. eBioMedicine 2020, 59, 102969. [Google Scholar] [CrossRef]
- Meizlish, M.L.; Goshua, G.; Liu, Y.; Fine, R.; Amin, K.; Chang, E.; DeFilippo, N.; Keating, C.; Liu, Y.; Mankbadi, M.; et al. Intermediate-dose anticoagulation, aspirin, and in-hospital mortality in COVID-19: A propensity score-matched analysis. Am. J. Hematol. 2021, 96, 471–479. [Google Scholar] [CrossRef]
- Patell, R.; Chiasakul, T.; Bauer, E.; Zwicker, J.I. Pharmacologic Thromboprophylaxis and Thrombosis in Hospitalized Patients with COVID-19: A Pooled Analysis. Thromb. Haemost. 2021, 121, 76–85. [Google Scholar] [CrossRef]
- Patel, N.G.; Bhasin, A.; Feinglass, J.M.; Angarone, M.P.; Cohen, E.R.; Barsuk, J.H. Mortality, critical illness, and mechanical ventilation among hospitalized patients with COVID-19 on therapeutic anticoagulants. Thromb. Update 2021, 2, 100027. [Google Scholar] [CrossRef]
- Kuno, T.; So, M.; Takahashi, M.; Egorova, N.N. Prophylactic versus therapeutic anticoagulation for survival of patients with COVID-19 on steroid. J. Thromb. Thrombolysis 2022, 53, 352–358. [Google Scholar] [CrossRef]
- Hoogenboom, W.; Lu, J.; Musheyev, B.; Borg, L.; Janowicz, R.; Pamlayne, S.; Hou, W.; Duong, T. Prophylactic versus therapeutic dose anticoagulation effects on survival among critically ill patients with COVID-19. PLoS ONE 2022, 17, e0262811. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bonaccio, M.; Cauda, R.; Guaraldi, G.; Menicanti, L.; Mennuni, M.; et al. Heparin in COVID-19 Patients Is Associated with Reduced In-Hospital Mortality: The Multicenter Italian CORIST Study. Thromb. Haemost. 2021, 121, 1054–1065. [Google Scholar] [CrossRef]
- Lynn, L.; Reyes, J.A.; Hawkins, K.; Panda, A.; Linville, L.; Aldhahri, W.; Kango, G.; Shah, S.; Ayanian, S.; Teufel, K. The effect of anticoagulation on clinical outcomes in novel Coronavirus (COVID-19) pneumonia in a U.S. cohort. Thromb. Res. 2021, 197, 65–68. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs. Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-risk Hospitalized Patients with COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612. [Google Scholar] [CrossRef]
- The ATTACC; ACTIV-4a; REMAP-CAP Investigators. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef]
- Sholzberg, M.; Tang, G.H.; Rahhal, H.; AlHamzah, M.; Kreuziger, L.B.; Áinle, F.N.; Alomran, F.; Alayed, K.; Alsheef, M.; AlSumait, F.; et al. Effectiveness of therapeutic heparin versus prophylactic heparin on death, mechanical ventilation, or intensive care unit admission in moderately ill patients with covid-19 admitted to hospital: RAPID randomised clinical trial. BMJ 2021, 375, n2400. [Google Scholar] [CrossRef]
- Lopes, R.D.; de Barros ESilva, P.; Furtado, R.; Macedo, A.; Bronhara, B.; Damiani, L.P.; Barbosa, L.M.; de Aveiro Morata, J.; Ramacciotti, E.; de Aquino Martins, P.; et al. Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): An open-label, multicentre, randomised, controlled trial. Lancet 2021, 397, 2253–2263. [Google Scholar] [CrossRef]
- Morici, N.; Podda, G.; Birocchi, S.; Bonacchini, L.; Merli, M.; Trezzi, M.; Massaini, G.; Agostinis, M.; Carioti, G.; Saverio Serino, F.; et al. Enoxaparin for thromboprophylaxis in hospitalized COVID-19 patients: The X-COVID-19 Randomized Trial. Eur. J. Clin. Investig. 2022, 52, e13735. [Google Scholar] [CrossRef]
- Marcos-Jubilar, M.; Carmona-Torre, F.; Vidal, R.; Ruiz-Artacho, P.; Filella, D.; Carbonell, C.; Jiménez-Yuste, V.; Schwartz, J.; Llamas, P.; Alegre, F.; et al. Therapeutic versus Prophylactic Bemiparin in Hospitalized Patients with Nonsevere COVID-19 Pneumonia (BEMICOP Study): An Open-Label, Multicenter, Randomized, Controlled Trial. Thromb. Haemost. 2022, 122, 295–299. [Google Scholar] [CrossRef]
- Muñoz-Rivas, N.; Aibar, J.; Gabara-Xancó, C.; Trueba-Vicente, Á.; Urbelz-Pérez, A.; Gómez-Del, V.; Demelo-Rodriguez, P.; Rivera-Gallego, A.; Bosch-Nicolau, P.; Perez-Pinar, M.; et al. Optimal Thromboprophylaxis Strategies in Non-Critically Ill Patients with COVID-19 Pneumonia. The PROTHROMCOVID Randomized Controlled Trial. medRxiv 2022. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.3; John Wiley and Sons, Ltd.: Chichester, UK, 2022. [Google Scholar]
- Kovács, E.H.; Turan, C.; Lee, B.Y.; Ocskay, K.; Tánczos, K.; Molnár, Z. Investigation of the Effects and Safety of Different Anticoagulant Doses Applied for Thrombosis Prophylaxis on Clinical Outcomes in COVID-19 PROSPERO: International Prospective Register of Systematic Reviews. 2021. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021284808 (accessed on 23 May 2022).
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; Davila, J.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021, 5, 872–888. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. 2021, 27, 107602962110109. [Google Scholar] [CrossRef]
- Zhao, R.; Su, Z.; Komissarov, A.A.; Liu, S.L.; Yi, G.; Idell, S.; Matthay, M.A.; Ji, H.L. Associations of D-Dimer on Admission and Clinical Features of COVID-19 Patients: A Systematic Review, Meta-Analysis and Meta-Regression. Front. Immunol. 2021, 12, 691249. [Google Scholar] [CrossRef]
- Velasco-Rodríguez, D.; Alonso-Dominguez, J.M.; Vidal Laso, R.; Lainez-González, D.; García-Raso, A.; Martín-Herrero, S.; Herrero, A.; Martínez Alfonzo, I.; Serrano-López, J.; Jiménez-Barral, E.; et al. Development and validation of a predictive model of in-hospital mortality in COVID-19 patients. PLoS ONE 2021, 16, e0247676. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- GRADEpro Guideline Development Tool; McMaster University: Hamilton, ON, Canada; Evidence Prime: Hamilton, ON, Canada, 2022; Available online: https://www.gradepro.org/ (accessed on 19 June 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 1 May 2022).
- Schwarzer, G. Meta: General Package for Meta-Analysis. 2022. Available online: https://github.com/guido-s/meta/https:// (accessed on 12 May 2022).
- Cuijpers, P.; Furukawa, T.; Ebert, D.D. Dmetar: Companion R Package for the Guide Doing Meta-Analysis in R. 2022. Available online: https://dmetar.protectlab.org (accessed on 12 May 2022).
- Mantel, N.; Haenszel, W. Statistical Aspects of the Analysis of Data from Retrospective Studies of Disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [CrossRef]
- Robins, J.; Greenland, S.; Breslow, N.E. A General Estimator for the Variance of the Mantel-Haenszel Odds Ratio. Am. J. Epidemiol. 1986, 124, 719–723. [Google Scholar] [CrossRef]
- Thompson, S.G.; Turner, R.M.; Warn, D.E. Multilevel models for meta-analysis, and their application to absolute risk differences. Stat. Methods Med. Res. 2001, 10, 375–392. [Google Scholar] [CrossRef]
- Knapp, G.; Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 2003, 22, 2693–2710. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef]
- Harris, C.M.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis, 2nd ed.; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- Sweeting, M.; Sutton, A.J.; Lambert, P. What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data. Stat. Med. 2004, 23, 1351–1375. [Google Scholar] [CrossRef]
- Paule, R.C.; Mandel, J. Consensus Values and Weighting Factors. J. Res. Natl. Bur. Stand. 1982, 87, 377. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Toshi, F.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide, 1st ed.; Chapman & Hall: Boca Raton, FL, USA, 2021; Available online: https://link.springer.com/book/10.1007/978-3-319-21416-0 (accessed on 1 May 2022).
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Viechtbauer, W.; Cheung, M.W.L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Lemos, A.; do Espírito Santo, D.A.; Salvetti, M.C.; Gilio, R.N.; Agra, L.B.; Pazin-Filho, A.; Miranda, C.H. Therapeutic versus prophylactic anticoagulation for severe COVID-19: A randomized phase II clinical trial (HESACOVID). Thromb. Res. 2020, 196, 359–366. [Google Scholar] [CrossRef]
- The REMAP-CA; ACTIV-4a; ATTACC Investigators. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Perepu, U.S.; Chambers, I.; Wahab, A.; Ten Eyck, P.; Wu, C.; Dayal, S.; Sutamtewagul, G.; Bailey, S.R.; Rosenstein, L.J.; Lentz, S.R. Standard prophylactic versus intermediate dose enoxaparin in adults with severe COVID-19: A multi-center, open-label, randomized controlled trial. J. Thromb. Haemost. 2021, 19, 2225–2234. [Google Scholar] [CrossRef] [PubMed]
- Blondon, M.; Cereghetti, S.; Pugin, J.; Marti, C.; Darbellay Farhoumand, P.; Reny, J.L.; Calmy, A.; Combescure, C.; Mazzolai, L.; Pantet, O.; et al. Therapeutic anticoagulation to prevent thrombosis, coagulopathy, and mortality in severe COVID-19: The Swiss COVID-HEP randomized clinical trial. Res. Pract. Thromb. Haemost. 2022, 6, e12712. [Google Scholar] [CrossRef]
- Oliynyk, O.; Barg, W.; Slifirczyk, A.; Oliynyk, Y.; Dubrov, S.; Gurianov, V.; Rorat, M. Comparison of the Effect of Unfractionated Heparin and Enoxaparin Sodium at Different Doses on the Course of COVID-19-Associated Coagulopathy. Life 2021, 11, 1032. [Google Scholar] [CrossRef]
- INSPIRATION Investigators; Sadeghipour, P.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Beigmohammadi, M.T.; Farrokhpour, M.; Sezavar, S.H.; Payandemehr, P.; Dabbagh, A.; et al. Effect of Intermediate-Dose vs. Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality among Patients with COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620. [Google Scholar] [CrossRef]
- Rashidi, F.; Barco, S.; Rezaeifar, P.; Sadeghipour, P.; Ghodrati, S.; Bakhshandeh, H.; Mousavi-Aghdas, S.A.; Sadeghi, A.; Sharifi, A.; Valizadeh, H.; et al. Tissue plasminogen activator for the treatment of adults with critical COVID-19: A pilot randomized clinical trial. Thromb. Res. 2021, 216, 125–128. [Google Scholar] [CrossRef]
- Connors, J.M.; Brooks, M.M.; Sciurba, F.C.; Krishnan, J.A.; Bledsoe, J.R.; Kindzelski, A.; Baucom, A.L.; Kirwan, B.A.; Eng, H.; Martin, D.; et al. Effect of Antithrombotic Therapy on Clinical Outcomes in Outpatients with Clinically Stable Symptomatic COVID-19: The ACTIV-4B Randomized Clinical Trial. JAMA 2021, 326, 1703. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 3i72, n71. [Google Scholar] [CrossRef]
- López Castro, J. Approach to post-COVID-19 syndrome (PC19S): How long to maintain corticotherapy and heparin after discharge from intensive care? Rev. Esp. Geriatría Gerontol. 2021, 56, 380. [Google Scholar] [CrossRef]
- Birocchi, S.; Manzoni, M.; Podda, G.M.; Casazza, G.; Cattaneo, M. High rates of pulmonary artery occlusions in COVID-19. A meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13433. [Google Scholar] [CrossRef] [PubMed]
- Hulshof, A.M.; Brüggemann, R.; Mulder, M.; van de Berg, T.W.; Sels, J.; Olie, R.H.; Spaetgens, B.; Streng, A.S.; Verhezen, P.; van der Horst, I.; et al. Serial EXTEM, FIBTEM, and tPA Rotational Thromboelastometry Observations in the Maastricht Intensive Care COVID Cohort—Persistence of Hypercoagulability and Hypofibrinolysis Despite Anticoagulation. Front. Cardiovasc. Med. 2021, 8, 654174. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.K.; Prabhakaran, K.; Latifi, R.; Smiley, A.; Klein, J.; Lombardo, G.; Rhee, P. Serial rotational thromboelastography (ROTEM) in mechanically ventilated patients with COVID-19 demonstrates hypercoagulopathy despite therapeutic heparinization. Trauma Surg Acute Care Open 2022, 7, e000603. [Google Scholar] [CrossRef] [PubMed]
- Nougier, C.; Benoit, R.; Simon, M.; Desmurs-Clavel, H.; Marcotte, G.; Argaud, L.; David, J.S.; Bonnet, A.; Negrier, C.; Dargaud, Y. Hypofibrinolytic state and high thrombin generation may play a major role in SARS-COV2 associated thrombosis. J. Thromb. Haemost. 2020, 18, 2215–2219. [Google Scholar] [CrossRef]
- Görlinger, K.; Almutawah, H.; Almutawaa, F.; Alwabari, M.; Alsultan, Z.; Almajed, J.; Alwabari, M.; Alsultan, M.; Shahwar, D.; Yassen, K.A. The role of rotational thromboelastometry during the COVID-19 pandemic: A narrative review. Korean J. Anesthesiol. 2021, 74, 91–102. [Google Scholar] [CrossRef]
- Heinz, C.; Miesbach, W.; Herrmann, E.; Sonntagbauer, M.; Raimann, F.J.; Zacharowski, K.; Weber, C.F.; Adam, E.H. Greater Fibrinolysis Resistance but No Greater Platelet Aggregation in Critically Ill COVID-19 Patients. Anesthesiology 2021, 134, 457–467. [Google Scholar] [CrossRef]
- Izuzquiza-Avanzini, I.; Gutiérrez-López, R.; Lorenzo López-Reboiro, M.; Martínez-Vivero, C.; López-Castro, J. COVID-19 and Thrombosis: Pathophysiological Mechanisms and Therapeutic Update. In Anticoagulation—Current Perspectives; Qi, X., Guo, X., Eds.; IntechOpen: London, UK, 2022; Volume 95. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Nevesny, F.; Rotzinger, D.C.; Sauter, A.W.; Loebelenz, L.I.; Schmuelling, L.; Alkadhi, H.; Ebner, L.; Christe, A.; Platon, A.; Poletti, P.A.; et al. Acute Pulmonary Embolism in Patients with COVID-19 at CT Angiography and Relationship to d -Dimer Levels. Radiology 2020, 296, E189–E191. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Olivé, I.; Sintes, H.; Radua, J.; Abad Capa, J.; Rosell, A. D-dimer in patients infected with COVID-19 and suspected pulmonary embolism. Respir. Med. 2020, 169, 106023. [Google Scholar] [CrossRef]
- Whyte, M.B.; Kelly, P.A.; Gonzalez, E.; Arya, R.; Roberts, L.N. Pulmonary embolism in hospitalised patients with COVID-19. Thromb. Res. 2020, 195, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Tassiopoulos, A.K.; Mofakham, S.; Rubano, J.A.; Labropoulos, N.; Bannazadeh, M.; Drakos, P.; Volteas, P.; Cleri, N.A.; Alkadaa, L.N.; Asencio, A.A.; et al. D-Dimer-Driven Anticoagulation Reduces Mortality in Intubated COVID-19 Patients: A Cohort Study with a Propensity-Matched Analysis. Front. Med. 2021, 8, 631335. [Google Scholar] [CrossRef] [PubMed]
- Duo, H.; Li, Y.; Sun, Y.; Wei, L.; Wang, Z.; Fang, F.; Zhong, Y.; Huang, J.; Luo, L.; Peng, Z.; et al. Effect of Therapeutic versus Prophylactic Anticoagulation Therapy on Clinical Outcomes in COVID-19 Patients: A Systematic Review with an Updated Meta-Analysis. Thromb. J. 2022, 20, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Flumignan, R.L.; Civile, V.T.; Tinôco, J.; Pascoal, P.I.; Areias, L.L.; Matar, C.F.; Tendal, B.; Trevisani, V.F.; Atallah, Á.N.; Nakano, L.C. Anticoagulants for people hospitalised with COVID-19. Cochrane Database Syst. Rev. 2022, 2022, CD013739. [Google Scholar] [CrossRef]
- Jorda, A.; Siller-Matula, J.M.; Zeitlinger, M.; Jilma, B.; Gelbenegger, G. Anticoagulant Treatment Regimens in Patients with COVID-19: A Meta-Analysis. Clin. Pharmacol. Ther. 2022, 111, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Kow, C.S.; Ramachandram, D.S.; Hasan, S.S. The effect of higher-intensity dosing of anticoagulation on the clinical outcomes in hospitalized patients with COVID-19: A meta-analysis of randomized controlled trials. J. Infect. Chemother. 2022, 28, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paz, L.; Galli, M.; Capodanno, D.; Franchi, F.; Rollini, F.; Bikdeli, B.; Mehran, R.; Montalescot, G.; Gibson, C.M.; Lopes, R.D.; et al. Safety and efficacy of different prophylactic anticoagulation dosing regimens in critically and non-critically ill patients with COVID-19: A systematic review and meta-analysis of randomized controlled trials. Eur. Heart J.-Cardiovasc. Pharmacother. 2021. [Google Scholar] [CrossRef]
- Reis, S.; Popp, M.; Schmid, B.; Stegemann, M.; Metzendorf, M.I.; Kranke, P.; Meybohm, P.; Weibel, S. Safety and Efficacy of Intermediate- and Therapeutic-Dose Anticoagulation for Hospitalised Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 11, 57. [Google Scholar] [CrossRef]
- Wills, N.K.; Nair, N.; Patel, K.; Sikder, O.; Adriaanse, M.; Eikelboom, J.; Wasserman, S. Efficacy and Safety of Intensified versus Standard Prophylactic Anticoagulation Therapy in Patients with COVID-19: A Systematic Review and Meta-Analysis. Infect. Dis. 2022, 9. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; Kahn, S.R.; et al. American Society of Hematology living guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19: May 2021 update on the use of intermediate-intensity anticoagulation in critically ill patients. Blood Adv. 2021, 5, 3951–3959. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. The Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 30 July 2022).
- Barnes, G.; Burnett, A.; Allen, A.; Ansell, J.; Blumenstein, M.; Clark, N.; Crowther, M.; Dager, W.; Deitelzweig, S.; Ellsworth, S.; et al. Thromboembolic prevention and anticoagulant therapy during the COVID-19 pandemic: Updated clinical guidance from the anticoagulation forum. J. Thromb. Thrombolysis 2022, 54, 197–210. [Google Scholar] [CrossRef]
- Moores, L.; Tritschler, T.; Brosnahan, S.; Carrier, M.; Collen, J.; Doerschug, K.; Holley, A.; Jimenez, D.; Le Gal, G.; Rali, P.; et al. Prevention, Diagnosis, and Treatment of VTE in Patients With Coronavirus Disease 2019. Chest 2020, 158, 1143–1163. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Enrollment Period | Country | Sample Size | Patients Admitted to | Intervention Arms | Follow-Up Period (days) |
|---|---|---|---|---|---|---|---|
| HESACOVID 2020 [50] | Open-label, single center RCT | From April 2020 to July 2020 | Brazil | 20 | 100% ICU | Therapeutic: enoxaparin 1 mg/kg twice daily or UFH adjusted to aPTT 1.5–2 Standard: enoxaparin 40 mg once daily or UFH 5000 three times a day a | 28 |
| Goligher et al., 2021 [51] | Open-label, adaptive, multiplatform RCT | From 21 April 2020 to 19 December 2020 | United States, Canada, the United Kingdom, Brazil, Mexico, Nepal | 1103 | 100% ICU | Therapeutic: enoxaparin 1.5 mg/kg once daily, UFH titrated to have 1.5–2.5 aPTT, dalteparin 200 UI once daily Tinzaparin 175 UI/kg once daily Standard: enoxaparin 40 mg once daily, dalteparine 5000 UI once, tinzaparine 4500 UI, fondaparinux 2.5 mg, UFH 5000 UI/ 8–12 h b | 21 |
| Lawler et al., 2021 [20] | Open-label, adaptive, multiplatform RCT | From 21 April 2020 to 22 January 2021 | United States, Canada, the United Kingdom, Brazil, Mexico, Nepal | 2219 | 100% ward | Therapeutic: enoxaparin 1.5 mg/kg once daily, UFH titrated to have 1.5–2.5 aPTT, dalteparin 200 UI once daily OR 100 UI twice daily tinzaparin 175 UI/kg once daily Standard: enoxaparin 40 mg once daily, dalteparine 5000 UI once, tinzaparine 4500 UI, fondaparinux 2.5 mg UFH 5000 UI/ 8–12 h b | 21 |
| Perepu et al., 2021 [52] | Open-label, multicenter RCT | From 26 April 2020 to 6 January 2021 | USA | 173 | 38% ward 62% ICU | Intermediate: enoxaparin 1 mg/kg SC daily Standard: enoxaparin 40 mg daily b | 30 |
| X-COVID 2021 [23] | Open-label, multicentre RCT | From 30 April 2020 to 25 April 2021 | Italy | 183 | 100% ward | Intermediate: enoxaparin 40 mg twice daily Standard: enoxaparin 40 mg once daily | 30 |
| COVID-HEP 2022 [53] | Open-label, multicentre RCT | From April 2020 to June 2021 | Switzerland | 159 | 45% ward 26% intermediate care 28% ICU | Therapeutic: enoxaparin 1 mg/kg twice daily or UFH with anti-Xa titration Standard: enoxaparin 40 mg once daily or UFH 5000 IU twice daily at ward enoxaparin 40 mg twice daily or UFH 5000 three times daily c | 30 |
| HEP-COVID 2020 [19] | Single-blinded, multicentre RCT | From 8 May 2020 to 14 May 2021 | USA | 253 | 67% ward 32% ICU | Therapeutic: enoxaparin 1 mg/kg twice daily Standard dose: enoxaparin 30 or 40 mg once or twice daily d | 30 |
| RAPID 2021 [21] | Open-label, adaptive, multicentre RCT | from 29 May 2020 to 12 April 2021 | Brazil, Canada, Ireland, Saudi Arabia, United Arab Emirates, United States of America | 465 | 100% ward | Therapeutic: enoxaparin 1.5 mg/kg once daily, dalteparin 200 UI/kg once daily, tinzaparin 175 IU/kg once daily, or UFH titrated according to aPPT Standard: 40 mg enoxaparin once daily, dalteparin 5000 UI daily, tinzaparin 4500 UI daily, UFH 5000 UI two or three times a day b | 28 |
| ACTION 2021 [22] | Open-label, pragmatic, multicentre RCT | From 24 June 2020 to 26 February 2021 | Brazil | 615 | 93% ward 6% ICU | Therapeutic: Rivaroxaban 20 mg once daily, enoxaparin 1 mg/kg twice daily, UFH titrated until anti-Xa 0.3–0.7 Standard: local prophylatic guidelines | 30 |
| Oliynyk et al., 2021 [54] | Open-label RCT | From July 2020 to 1 March 2021 | Ucraine | 126 | 100% ICU | Therapeutic: group 1: enoxaparin of 100 antiXa IU/kg twice daily group 2: UFH titrated to aPTT 40–70 s Standard: enoxaparin of 50 antiXa IU/kg once daily | 28 |
| INSPIRATION 2021 [55] | Open-label, multicenter RCT | From 29 July 2020 to 19 November 2020 | Iran | 562 | 100% ICU | Intermediate: enoxaparin 1 mg/kg daily Standard: enoxaparin 40 mg daily | 30 |
| Rashidi et al., 2021 [56] | Open-label, pilot RCT | From September 2020 to April 2021 | Iran | 10 | 100% ICU | Therapeutic dose: UFH 5000 IU every 8 h Standard: UFH titrated until aPTT 5–70 | 30 |
| BEMICOP 2022 [24] | Open-label, multicenter, RCT | From October 2020 to May 2021 | Spain | 65 | 100% ward | Therapeutic: bemiparin 115 UI/kg daily Standard: bemiparin 3500 UI daily | 30 |
| PROTHROMCOVID 2022 [25] | Open-label, multicenter RCT | From 1 February 2021 to 30 September 2021 | Spain | 300 | 100% ward | Therapeutic: tinzaparin 175 UI/kg Intermediate: tinzaparin 100 UI/kg Standard: tinzaparin 4500 UI daily | 30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovács, E.H.; Tánczos, K.; Szabó, L.; Turan, C.; Dembrovszky, F.; Ocskay, K.; Lee, B.-Y.; Hegyi, P.; Molnár, Z. Higher Dose Anticoagulation Cannot Prevent Disease Progression in COVID-19 Patients: A Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 2194. https://doi.org/10.3390/biomedicines10092194
Kovács EH, Tánczos K, Szabó L, Turan C, Dembrovszky F, Ocskay K, Lee B-Y, Hegyi P, Molnár Z. Higher Dose Anticoagulation Cannot Prevent Disease Progression in COVID-19 Patients: A Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(9):2194. https://doi.org/10.3390/biomedicines10092194
Chicago/Turabian StyleKovács, Emőke Henrietta, Krisztián Tánczos, László Szabó, Caner Turan, Fanni Dembrovszky, Klementina Ocskay, Bo-Young Lee, Péter Hegyi, and Zsolt Molnár. 2022. "Higher Dose Anticoagulation Cannot Prevent Disease Progression in COVID-19 Patients: A Systematic Review and Meta-Analysis" Biomedicines 10, no. 9: 2194. https://doi.org/10.3390/biomedicines10092194