Article Text

Statistics from Altmetric.com
Country overview and timelines of COVID-19 outbreak in Vietnam
Vietnam is a lower-income to middle-income country with a population of 97 million. In 2018, its gross domestic product per capita was US$2.566, and around US$150 per person were spent on healthcare. The healthcare system in Vietnam includes both public and private providers, with less than one doctor and two nurses per 1000 population. Public hospitals are divided into four levels: central, provincial, district and commune levels, and are responsible for providing healthcare for the majority of the residents in Vietnam.
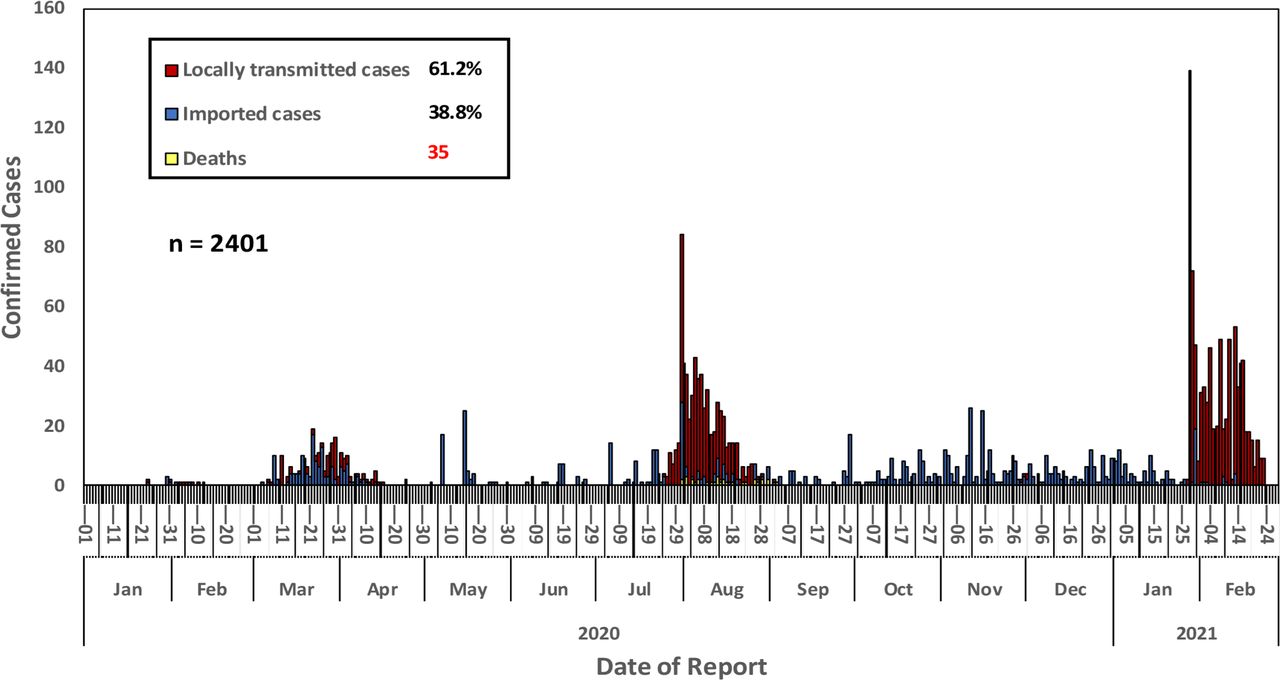
The country has a 1300 km border with China in the north, where SARS-CoV-2 first emerged.1 Therefore, Vietnam was at high risk of SARS-CoV-2 infection as the virus spread outside of China in early 2020. Yet, as of 23 February 2021, there have been only a total of 2401 reverse transcription (RT)-PCR-confirmed cases of SARS-CoV-2 infection with three major waves attributable to locally acquired infection (figure 1) and 35 deaths from the virus reported in Vietnam.2 The outbreak in the coastal city of Da Nang between July and August 2020 represented a major outbreak associated with community transmission.3 4 This was then followed by the detection of sporadic cases of community transmission in the last quarter of 2020. In the morning of 28 January 2021, after 55 days of no community transmission anywhere in the country, two cases of locally acquired infection were reported in two neighbouring provinces (Hai Duong and Quang Ninh). By the end of the same day, the number of infections climbed to 88, marking the beginning of the third wave of community transmission in Vietnam. Although as of 23 February 2021, a total 809 infections have been reported from the current outbreak, the epidemic curve is now falling (figure 1). Likewise, the number of provinces with ongoing community transmissions has decreased from 13 to 3 since 17 February 2021.2 5

Outbreaks of COVID-19 in Vietnam with three waves of community transmission (source: who.int/vietnam).
Despite the ongoing challenges, Vietnam is one of the few countries worldwide that have successfully controlled SARS-CoV-2. Here, we discuss the measures taken that have led to the control of SARS-CoV-2 in Vietnam.
Rapid and coordinated public health response
Before the SARS-CoV-2 pandemic, Vietnam had experienced outbreaks of several emerging infectious diseases. They have included the severe acute respiratory syndrome (SARS) caused by SARS-CoV-1 in 2003, bird influenza caused by influenza A virus subtype H5N1 in 2004 and the 2009 H1N1 pandemic. Notably, back in 2003, Vietnam was recognised by the WHO as the first country to successfully contain SARS-CoV-1. Additionally, endemic infections such as dengue and hand, foot and mouth disease have continuously posed significant challenges on the healthcare system in Vietnam on a yearly basis. Lessons learnt from these outbreaks and endemic infections were thus critical in informing Vietnam’s rapid and coordinated response to SARS-CoV-2.6
On 16 January 2020, the Vietnam Ministry of Health (MOH) issued the first national guidelines on COVID-19 diagnostics and management. The guidelines also covered guidance on contact tracing and 14-day isolation of individuals in contact with a PCR-confirmed case. Furthermore, on 20 January 2020, the MOH issued the national strategic plan for COVID-19 response with the overarching aims of early detection, rapid containment and effective case management. On 30 January 2020, the government assembled the National Steering Committee for COVID-19. The Committee is responsible for the highest level of COVID-19 response and coordination in Vietnam. On the same day, the MOH established the National Rapid Response Team, with members drawn from referral hospitals across the country. The team is responsible for providing expert support to primary COVID-19 centres and hospitals across Vietnam.
Centralised patient management
Unlike strategies applied in other countries, where only confirmed cases with severe illness are admitted to health facilities for clinical management, any PCR-confirmed cases in Vietnam have been admitted to one of the designated COVID-19 treatment centres/hospitals deployed across the country since early 2020, regardless of clinical symptoms. Severe cases are subjected to panel discussion via teleconference with participants from the national COVID-19 response team, thus enabling the best clinical management.
Early school closures and robust border controls
School closure was initially scheduled for the Lunar New Year holiday between the end of January and early February 2020. However, in response to the introduction of SARS-CoV-2 into Vietnam on 23 January 20207 and the escalation of community transmission during of the first wave, school and university closures were extended until early May 2020 when the nationwide outbreak was brought under control.
Vietnam also took early actions to enhance border control measures from as early as January 2020, when the country first heard about the emergence of a cluster of pneumonia of unknown origin in Wuhan, China (table 1). Additionally, body temperature screening at airports and border gates was applied for passengers arriving in Vietnam from Wuhan where the epidemic first started. This was then extended to arrivals from the whole China and other countries where community transmission was ongoing.
Timelines of early border control measures in 2020 leading to the success of COVID-19 control in Vietnam
An international travel ban was first applied to Wuhan, China, on 23 January 2020. As the pandemic escalated in the region and beyond, Vietnam closed its borders and banned international flights to and from China, followed by other countries (including Taiwan, Korea, Italy, the UK and the USA). Finally, Vietnam closed all main and auxiliary border gates on 1 April 2020 (table 1).
Mask policies and 5K message
Wearing a face mask in public was recommended by the government in January 2020 and was then made mandatory on 16 March 2020. On 31 August 2020, the MOH launched a 5K (in Vietnamese) message to help people get used to a new normal state under the COVID-19 pandemic while protecting themselves from the infection. 5K stands for ‘Khẩu trang’ (face masks), ‘Khử khuẩn’ (disinfection), ‘Khoảng cách’ (distance), ‘Không tụ tập’ (no gathering) and ‘Khai báo y tế’ (health declaration). By launching the 5K campaign, the government encouraged people to (1) wear masks in public, quarantine centres and medical facilities; (2) regularly wash hands with soap or sanitisers plus surface cleaning by disinfectants; (3) keep distance from each other, (4) avoid mass gathering and (5) make health declaration.
Third-degree contact tracing
An innovative and unique strategy to SARS-CoV-2 control in Vietnam has been a meticulous contact-tracing approach, which is referred as third-degree contact tracing (figure 2). According to this approach, a confirmed case is defined as F0, while close contacts of F0 are called F1, and F2s are those in close contact with an F1. Once an F1 is tested positive, F2s become F1 and therefore contacts of F2s (F3s) become F2, and so on.

Illustration showing the third-degree contact tracing applied as part of COVID-19 control measures in Vietnam since the beginning of the pandemic (adapted from Pollack et al 4 with permission).
When a confirmed case (F0) is identified, local health officers conduct an epidemiological investigation by asking the F0 to recall his/her recent close contacts (F1) and travel history since his/her last contact with a confirmed case (if known) or over the last 14 days. Detailed travel history and contacts of F0 are then made publically available on the government COVID-19 website (ncov.moh.gov.vn), local magazines and national TV channels so that people can identify whether they have an epidemiological link with a confirmed case. Supporting this meticulous contact tracing approach is the use of locally developed mobile apps, such as Bluezone (rolled out on 18 April 2020). Bluezone is a Bluetooth-based app, which helps users identify whether they were in close contact with a confirmed case. Individuals with an epidemiological link with F0 are thus encouraged to present to or contact the nearest local hospital for advice on isolation and testing. Once F1s are identified, the same approach is used to determine their contacts or F2, and so on.
Mass quarantine and targeted lockdown
In addition to the administration of F0 to COVID-19 treating hospitals for clinical follow-up, F1s are also subjected to a minimum of 14-day isolation at one of the state-run quarantine facilities deployed across Vietnam since early March. Meanwhile, F2s are requested to self-isolate at home for a maximum of 14 days. The same 14-day quarantine at state-run facilities has also been applied to all travellers arriving in Vietnam since early March 2020. As of 21 February 2021, more than 1.3 million people have been quarantined at one of the designated isolation centres across Vietnam.5 As the pandemic progressed and scientific evidence about the transmission potential of asymptomatic infection arose,8 Vietnam’s extensive contact tracing, mass quarantine and wearing a face mask in public proved to be innovative and critical to suppress the community transmission of SARS-CoV-2 in the country.
Alongside the isolation of confirmed cases, their contacts and travellers to Vietnam, Vietnam has also implemented mass quarantine of suspected transmission hotspots (eg, a city, a town or a community). Table 2 lists all major lockdowns implemented by the Vietnamese government as of February 2021. The first community lockdown was applied on 13 February 2020 to Son Loi commune in Vinh Phuc, Northern Vietnam. At that time, there was a cluster of six local infections linked with eight Vietnamese employees returning from Wuhan.9 The lockdown was lifted on 3 March, marking the first in-country success of targeted lockdown.
Major lockdowns implemented by the Vietnamese government as of February 2021
On 1 April 2020, when community transmission was escalating and the total reported cases in Vietnam exceeded 200, the prime minister enacted a 2-week nationwide lockdown. Accordingly, non-essential businesses and public transport were shut down, while only essential travel between cities/provinces was allowed. Gatherings of more than two people in public were prohibited. People were asked not to leave their house unless there was a need for essential activities (eg, buying food or seeking medical care). The lockdown was extended to 30 April for high-risk areas (including Ho Chi Minh city and Ha Noi).
Most recently, on 28 January 2021, Chi Linh, a city of 220 000 households in Hai Duong province in northern Vietnam, was immediately placed under quarantine after the report of 83 new cases of locally acquired infection of unknown origin. Since then, the lockdown has been extended to other towns and villages. On 16 February, Hai Duong province, the epicentre of the ongoing nationwide outbreak, was placed under full lockdown due to the escalation of the in-province outbreak.
Innovative testing strategies
One of the key factors determining the success of Vietnam’s approach to extensive contact tracing, isolation and targeted lockdown has been the ability of the country to rapidly increase its diagnostic capacity and the innovative way of conducting mass RT-PCR screening. Soon after the diagnosis of the first cases of SARS-CoV-2 in Vietnam in January 2020, the government pushed forward the development of local diagnostic kits for SARS-CoV-2. On 5 March, the first locally produced COVID-19 RT-PCR test kit developed by Military Medical University was commercialised by Viet A Corporation. The kit has now been widely used as a screening assay at the majority of COVID-19 diagnostic labs in Vietnam, while WHO recommended RT-PCR protocols serve as confirmatory assays.10 Additionally, centres qualified for SARS-CoV-2 RT-PCR testing increased from two sites in early 2020 to 91 across the country by 23 November 2020. The country’s current capacity is around 100 000 PCR tests per day. As of 21 February 2021, nearly two million PCR tests have been conducted in Vietnam.5
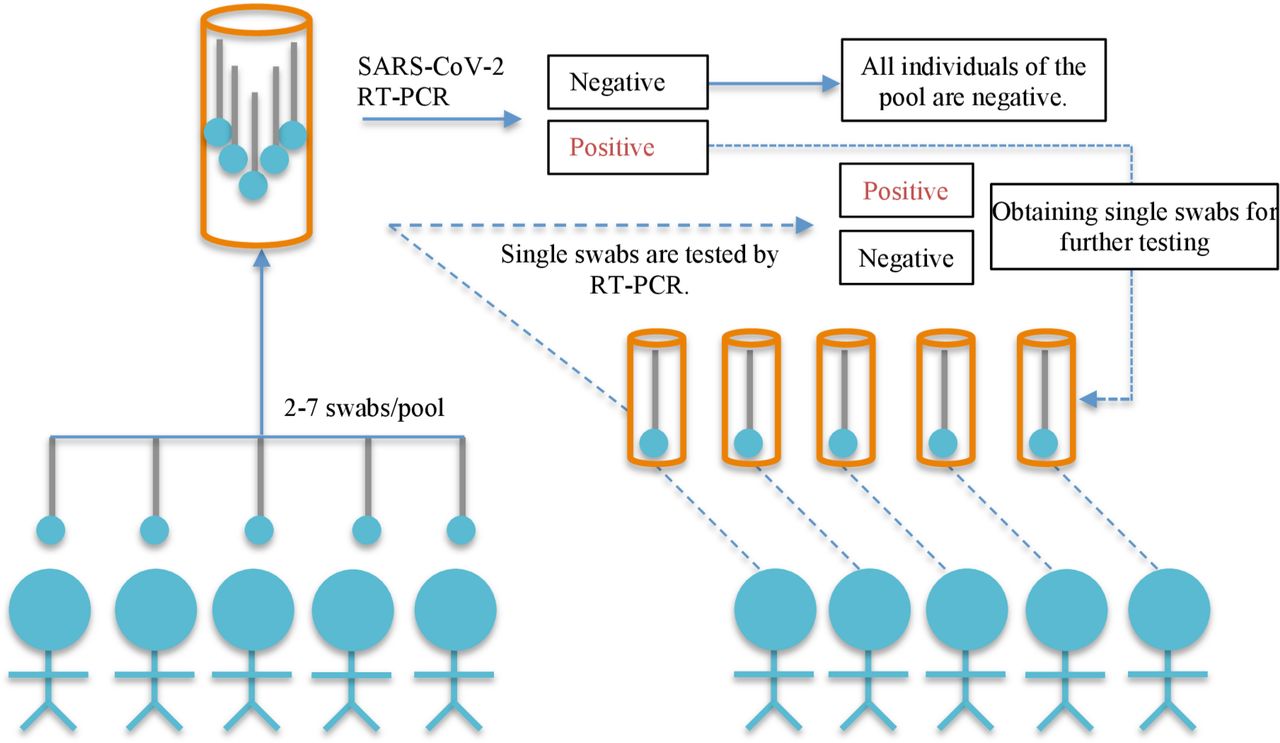
The availability of in-country capacity has allowed Vietnam to integrate mass PCR screening into its national COVID-19 control programme. For example, during the Da Nang outbreak in July–August, mass screening coupled with an innovative sample pooling strategy11 was applied. Accordingly, swabs from two to seven individuals living in areas under lockdown were placed in one tube at collection for mass screening (figure 3). In this way, a total of 22 people without any history of contact with a confirmed case were identified after testing nearly 100 000 individuals by RT-PCR between 8 and 21 August 2020.This approach contributed to the success of COVID-19 control during the second wave. Most recently, this novel sample pooling strategy has been deployed for mass screening of SARS-CoV-2 as part of the national response to the ongoing outbreak.5
{kind=link}
{kind=link}
{kind=link}
Illustration of the sample pooling strategy that was successfully applied for mass screening of SARS-CoV-2 during the second wave of COVID-19 in Vietnam, July–August 2020.11 Nasal–pharyngeal throat swabs from two to seven individuals were combined in a single 15 mL collection tube containing 3 mL of viral transport medium for subsequent reverse transcription (RT)-PCR screening for SARS-CoV-2. If SARS-CoV-2 testing of the pool returned positive, single nasal–pharyngeal throat swabs from each individual of the corresponding group were then collected and retested separately for SARS-CoV-2 by RT-PCR.
Innovative communications
Keys to the success of SARS-CoV-2 control in Vietnam have been the transparent communications of the Vietnamese government and the compliance of the population with control measures. Since the beginning of the pandemic, the government has used a wide range of innovative communication strategies to keep the public informed with information about the disease, the transmission mechanisms and the in-country preventive responses. Social media, national television, local magazines, national hotline (19009095), mobile short message service (SMS) texts and the official COVID-19 website of the MOH (ncov.moh.gov.vn) were all used as communication tools.
Since the beginning of the pandemic, MOH sent regular updates on COVID-19 preventive responses and the national situation via SMS texts and messaging apps such as Zalo. On 9 January, the first COVID-19 news was posted on the government COVID-19 website (ncov.moh.gov.vn). Since then, this website has served as the most reliable and up-to-date source of information on the COVID-19 situation in Vietnam.
In February, a popular Vietnamese song was given new lyrics, ‘Ghen Co Vy’ (Jealous Coronavirus) to raise public awareness of the disease and to promote good hygiene habits against COVID-19.12 In collaboration with the Central Committee of the Vietnam Fatherland Front, the Vietnam Digital Media Association and the United Nations Children’s Fund, the MOH launched the #Onhavanvui (#StayHomeIsFun) campaign on TikTok.13 In addition to using this approach as a communication channel about COVID-19, the government also aimed to create a virtual playground for the community to stay connected while under the lockdown. Accordingly, TikTok users are encouraged to share their daily activities at home such as cooking (#onhanoitro), exercising (#onhakhoemanh), studying (#onhahocbai) with the community. Remarkably, as of January 2021, the hashtag #Onhavanvui of the MOH on TikTok has attracted nearly 11 billion views, while Ghen Co Vy has received some 70 million views.
Creative approaches initiated by the community to support vulnerable people
Caring for others, especially during a difficult time, has always been part of the Vietnamese culture. As such, during the COVID-19 crisis, Vietnamese people came up with various innovative initiatives to support each other. For example, during the national lockdown in April, entrepreneur Hoang Tuan Anh invented a rice automated teller machine (ATM). The aim was to help vulnerable people with daily meals. These semiautomatic machines dispensed rice for free from a container through a plastic tube with an amount of 1.5 kg each time. It was first introduced in Ho Chi Minh City and was then expanded to other cities, including Ha Noi and Da Nang. Building on the success of rice ATM, mask and food ATM initiatives were subsequently invented.
Conclusions
Early preparedness and proactive coordinated responses encompassing early border closure, physical distancing, face masks, targeted lockdown, contact tracing, isolation and pooled testing coupled with innovative communication and the engagement of the whole society have been keys to the success of SARS-CoV-2 control in Vietnam.
Ethics statements
Acknowledgments
The authors thank WHO Vietnam Country Office and Chevy Lazenby from Gates Venture for providing us with high-resolution figures (1 and 2) for reproduction in the present work.
Footnotes
Twitter @Le_Van_Tan
Contributors Conceptual design: NVVC, GT, DDA and LVT; writing the first draft: LVT; review, editing and approval of the manuscript: all authors.
Funding LVT, GT and RG are supported by the Wellcome Trust of Great Britain (204904/Z/16/Z (LVT) and106680/B/14/Z (GT and RG)).
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.