
Prevalence and Factors Associated with Psychological Problems of Healthcare Workforce in Vietnam: Findings from COVID-19 Hotspots in the National Second Wave

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling Methods
2.2. Measurements
2.2.1. PHQ-9
2.2.2. GAD-7
2.2.3. ISI
2.3. Variables
2.3.1. Main Outcome Variables
- ○
- Anxiety was defined as that in which an individual had a GAD-7 score of ≥10 [21].
- ○
- Depression was defined as that in which an individual had a PHQ-9 score of ≥10 [22].
- ○
- Clinical insomnia was defined as that in which an individual had an ISI score of ≥15 [23].
- ○
- Overall psychological problem was defined as that in which an individual had any symptom of moderate/severe anxiety, depression, or insomnia.
2.3.2. Socioeconomic and COVID-19 Control-Related Variables
2.4. Data Analysis
3. Results
3.1. Socioeconomic Characteristics and COVID-19 Control-Related Characteristics in Healthcare Workers
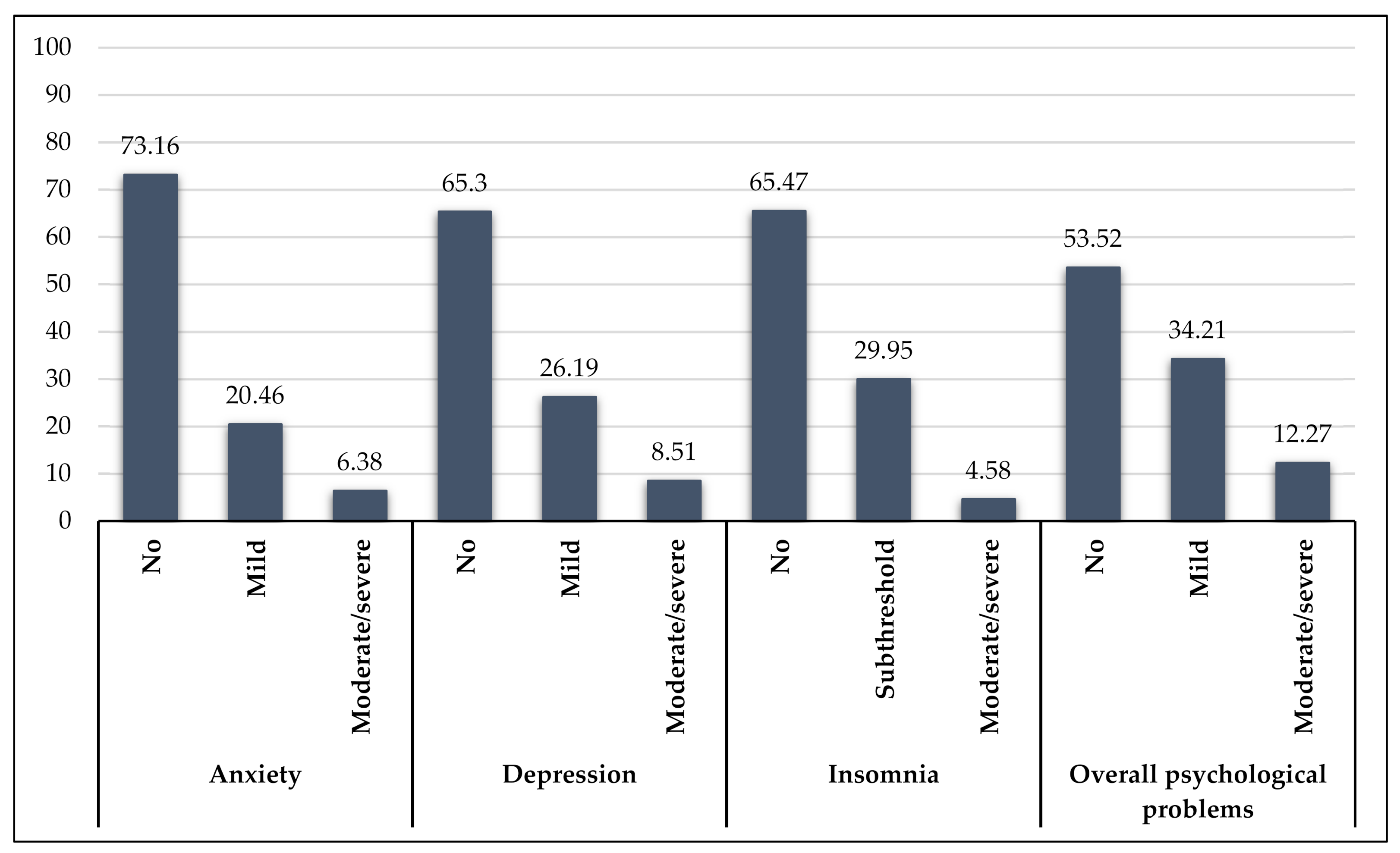
3.2. Prevalence of Psychological Problems in Healthcare Workers
3.3. Factors Associated with Psychological Problems
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. World Health Organization Coronavirus Disease 2019 (COVID-19) Situation Report; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. Coronavirus covid-19 has killed more people than SARS and MERS combined, despite lower case fatality rate. BMJ 2020, 368, m641. [Google Scholar] [CrossRef] [Green Version]
- The Lancet. COVID-19: Protecting health-care workers. Lancet 2020, 395, 922. [Google Scholar] [CrossRef]
- Catton, H. Global challenges in health and health care for nurses and midwives everywhere. Int. Nurs. Rev. 2020, 67, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallok, T. Emerging COVID-19 Success Story: Vietnam’s Commitment to Containment. Available online: https://ourworldindata.org/covid-exemplar-vietnam. (accessed on 27 July 2020).
- Tuan, D. Prime Minister Agreed to Continue Implementing Directive 16 at Least Until 22/4 in Some Localities. Available online: http://baochinhphu.vn/Tin-noi-bat/Thu-tuong-nhat-tri-tiep-tuc-thuc-hien-Chi-thi-16-it-nhat-den-224-tai-mot-so-dia-phuong/393140.vgp (accessed on 1 August 2020).
- Vu, K.; Nguyen, P.; Pearson, J. After Aggressive Mass Testing, Vietnam Says It Contains Coronavirus Outbreak. Available online: https://www.reuters.com/article/us-health-coronavirus-vietnam-fight-insi/after-aggressive-mass-testing-vietnam-says-it-contains-coronavirus-outbreak-idUSKBN22B34H (accessed on 28 July 2020).
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerström test for nicotine dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Ministry of Health of Vietnam. Prime Minister: Calculate Closely before Deciding on Social Distance. Available online: https://moh.gov.vn/tin-noi-bat/-/asset_publisher/3Yst7YhbkA5j/content/thu-tuong-tinh-toan-chat-che-truoc-khi-quyet-inh-gian-cach-xa-hoi?inheritRedirect=false&redirect=https%3A%2F%2Fmoh.gov.vn%3A443%2Ftin-noi-bat%3Fp_p_id%3D101_INSTANCE_3Yst7YhbkA5j%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26p_p_col_id%3Drow-1-column-1%26p_p_col_count%3D1 (accessed on 2 August 2020).
- Ministry of Health of Vietnam. Tightening the Entire System, Putting Forces in Da Nang. Available online: https://moh.gov.vn/tin-noi-bat/-/asset_publisher/3Yst7YhbkA5j/content/siet-chat-toan-bo-he-thong-don-luc-dap-dich-o-a-nang?inheritRedirect=false&redirect=https%3A%2F%2Fmoh.gov.vn%3A443%2Ftin-noi-bat%3Fp_p_id%3D101_INSTANCE_3Yst7YhbkA5j%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26p_p_col_id%3Drow-1-column-1%26p_p_col_count%3D1 (accessed on 2 August 2020).
- Ministry of Health of Vietnam. The Prime Minister Instructed: Speed Up the Tracking of the Source of COVID-19 Infection. Available online: https://moh.gov.vn/hoat-dong-cua-lanh-dao-bo/-/asset_publisher/TW6LTp1ZtwaN/content/thu-tuong-chi-ao-tang-toc-truy-vet-nguon-lay-covid-19?inheritRedirect=false&redirect=https%3A%2F%2Fmoh.gov.vn%3A443%2Fhoat-dong-cua-lanh-dao-bo%3Fp_p_id%3D101_INSTANCE_TW6LTp1ZtwaN%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26p_p_col_id%3Drow-0-column-2%26p_p_col_count%3D2 (accessed on 2 August 2020).
- Anh, L.; Duong, T. COVID-19 Prevention of Community Infection: Many Measures Are Applied for the First Time. Available online: https://tuoitre.vn/phong-chong-covid-19-lay-nhiem-cong-dong-nhieu-bien-phap-lan-dau-ap-dung-20200727000320695.htm (accessed on 2 August 2020).
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef] [Green Version]
- Chong, M.Y.; Wang, W.C.; Hsieh, W.C.; Lee, C.Y.; Chiu, N.M.; Yeh, W.C.; Huang, T.-L.; Wen, J.K.; Chen, C.L. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br. J. Psychiatry 2004, 185, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maunder, R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: Lessons learned. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2004, 359, 1117–1125. [Google Scholar] [CrossRef] [Green Version]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.B.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term Psychological and Occupational Effects of Providing Hospital Healthcare during SARS Outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef]
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.; Sham, P.C.; Chua, S.E.; Wong, J.G. Immediate and Sustained Psychological Impact of an Emerging Infectious Disease Outbreak on Health Care Workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Que, J.; Shi, L.; Deng, J.; Liu, J.; Zhang, L.; Wu, S.; Gong, Y.; Huang, W.; Yuan, K.; Yan, W.; et al. Psychological impact of the COVID-19 pandemic on healthcare workers: A cross-sectional study in China. Gen. Psychiatry 2020, 33, e100259. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.-A.; Que, J.-Y.; Huang, X.-L.; Liu, L.; Ran, M.-S.; Gong, Y.-M.; Yuan, K.; Yan, W.; Sun, Y.-K.; et al. Prevalence of and Risk Factors Associated with Mental Health Symptoms Among the General Population in China During the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Pandemic in Mainland China. Available online: https://en.wikipedia.org/wiki/COVID-19_pandemic_in_mainland_China (accessed on 1 October 2020).
- Covid-19 Pandemic in Vietnam. Available online: https://en.wikipedia.org/wiki/COVID-19_pandemic_in_Vietnam (accessed on 30 September 2020).
- Maunder, R.G.; Lancee, W.J.; Rourke, S.; Hunter, J.J.; Goldbloom, D.; Balderson, K.; Petryshen, P.; Steinberg, R.; Wasylenki, D.; Koh, D.; et al. Factors Associated with the Psychological Impact of Severe Acute Respiratory Syndrome on Nurses and Other Hospital Workers in Toronto. Psychosom. Med. 2004, 66, 938–942. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. Available online: https://www.who.int/news/item/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 5 October 2020).
- Theorell, T. Evaluating life events and chronic stressors in relation to health: Stressors and health in clinical work. In The Psychosomatic Assessment; Karger Publishers: Basel, Switzerland, 2012; pp. 58–71. [Google Scholar]
- Zhang, W.-R.; Wang, K.; Yin, L.; Zhao, W.-F.; Xue, Q.; Peng, M.; Min, B.-Q.; Tian, Q.; Leng, H.-X.; Du, J.-L.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Khanal, P.; Devkota, N.; Dahal, M.; Paudel, K.; Joshi, D. Mental health impacts among health workers during COVID-19 in a low resource setting: A cross-sectional survey from Nepal. Glob. Health 2020, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated with Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Singer, C. Health effects of social isolation and loneliness. J. Aging Life Care 2018, 28, 4–8. [Google Scholar]
- Pietrabissa, G.; Simpson, S.G. Psychological Consequences of Social Isolation During COVID-19 Outbreak. Front. Psychol. 2020, 11, 2201. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Rautio, N.; Filatova, S.; Lehtiniemi, H.; Miettunen, J. Living environment and its relationship to depressive mood: A systematic review. Int. J. Soc. Psychiatry 2018, 64, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Xue, D.; Liu, Y.; Chen, H.; Qiu, Y. The relationship between urbanization and depression in China: The mediating role of neighborhood social capital. Int. J. Equity Health 2018, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Physician (n = 144) | Nurses (n = 326) | Technicians (n = 141) | Total (n = 611) |
|---|---|---|---|---|
| Count (% of Total) | Count (% of Total) | Count (% of Total) | Count (% of Total) | |
| Gender | ||||
| Male | 83 (57.64) | 23 (7.06) | 52 (36.88) | 158 (25.86) |
| Female | 61 (42.36) | 303 (92.94) | 89 (63.12) | 453 (74.14) |
| Marital status | ||||
| Married | 93 (64.58) | 245 (75.15) | 99 (70.21) | 437 (71.52) |
| Single | 50 (34.72) | 78 (23.93) | 39 (27.66) | 167 (27.33) |
| Widowed | 0 (0.00) | 1 (0.31) | 1 (0.71) | 2 (0.33) |
| Divorced | 1 (0.69) | 2 (0.61) | 2 (1.42) | 5 (0.82) |
| Number of people living with (people) | ||||
| 1–3 people | 37 (25.69) | 66 (20.25) | 32 (22.70) | 135 (22.09) |
| 4–5 people | 74 (51.39) | 166 (50.92) | 73 (51.77) | 313 (51.23) |
| >5 people | 33 (22.92) | 94 (28.83) | 36 (25.53) | 163 (26.68) |
| Living area | ||||
| Village | 41 (28.47) | 143 (43.87) | 58 (41.13) | 242 (39.61) |
| Town | 39 (27.08) | 58 (17.79) | 42 (29.79) | 139 (22.75) |
| City | 64 (44.44) | 125 (38.34) | 41 (29.08) | 230 (37.64) |
| Distance between home and main or regular place of work (meter) | ||||
| <1000 m | 32 (22.22) | 57 (17.48) | 27 (19.15) | 116 (18.99) |
| 1000–5000 m | 43 (29.86) | 102 (31.29) | 52 (36.88) | 197 (32.24) |
| 5000–10,000 m | 32 (22.22) | 64 (19.63) | 31 (21.99) | 127 (20.79) |
| 5000–10,000 m | 37 (25.69) | 103 (31.60) | 31 (21.99) | 171 (27.99) |
| Education | ||||
| Lower secondary/upper secondary | 0 (0.00) | 18 (5.52) | 1 (0.71) | 19 (3.11) |
| College | 2 (1.39) | 181 (55.52) | 90 (63.83) | 273 (44.68) |
| University | 79 (54.86) | 123 (37.73) | 43 (30.50) | 245 (40.10) |
| Postgraduation | 63 (43.75) | 4 (1.23) | 7 (4.96) | 74 (12.11) |
| Professional experience (years) | ||||
| <1 year | 6 (4.17) | 9 (2.76) | 6 (4.26) | 21 (3.44) |
| 1–2 year(s) | 25 (17.36) | 37 (11.35) | 17 (12.06) | 79 (12.93) |
| 3–5 years | 37 (25.69) | 65 (19.94) | 36 (25.53) | 138 (22.59) |
| 5–10 years | 35 (24.31) | 112 (34.36) | 45 (31.91) | 192 (31.42) |
| >10 years | 41 (28.47) | 103 (31.60) | 37 (26.24) | 181 (29.62) |
| Current situation | ||||
| Being in quarantine zone doing nothing | 26 (18.06) | 32 (9.82) | 9 (6.38) | 67 (10.97) |
| Being in quarantine to care for the COVID-19 infected patient | 28 (19.44) | 55 (16.87) | 8 (5.67) | 91 (14.89) |
| Being in quarantine at home | 29 (20.14) | 33 (10.12) | 7 (4.96) | 69 (11.29) |
| Having ended the duration in quarantine and normally work | 17 (11.81) | 36 (11.04) | 24 (17.02) | 77 (12.60) |
| Normal working | 44 (30.56) | 170 (52.15) | 93 (65.96) | 307 (50.25) |
| Duration participating in COVID-19 control (weeks) | ||||
| <1 week | 30 (20.83) | 53 (16.26) | 27 (19.15) | 110 (18.00) |
| 1–2 week(s) | 45 (31.25) | 127 (38.96) | 50 (35.46) | 222 (36.33) |
| 2–4 weeks | 54 (37.50) | 112 (34.36) | 43 (30.50) | 209 (34.21) |
| 4–8 weeks | 6 (4.17) | 15 (4.60) | 11 (7.80) | 32 (5.24) |
| >8 weeks | 9 (6.25) | 19 (5.83) | 10 (7.09) | 38 (6.22) |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Age (years) | 34.49 (9.63) | 31.63 (7.45) | 32.41 (8.63) | 32.49 (8.35) |
| Anxiety | Depression | Insomnia | Overall Psychological Problems | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No n (%) | Mild n (%) | Moderate/ Severe n (%) | No, n (%) | Mild n (%) | Moderate/ Severe n (%) | No n (%) | Subthreshold n (%) | Moderate/ Severe n (%) | No n (%) | Mild n (%) | Moderate/ Severe n (%) | |
| Physician, n (% of total) | 107 (74.31) | 21 (14.58) | 16 (11.11) | 97 (67.36) | 30 (20.83) | 17 (11.81) | 95 (65.97) | 42 (29.17) | 7 (4.86) | 78 (54.17) | 45 (31.25) | 21 (14.58) |
| Nurse, n (% of total) | 235 (72.09) | 70 (21.47) | 21 (6.44) | 200 (61.35) | 103 (31.60) | 23 (7.06) | 208 (63.80) | 99 (30.37) | 19 (5.82) | 164 (50.31) | 121 (37.12) | 41 (12.58) |
| Technician, n (% of total) | 105 (74.47) | 34 (24.11) | 2 (1.42) | 102 (72.34) | 27 (19.15) | 12 (8.51) | 97 (68.79) | 42 (29.79) | 2 (1.42) | 85 (60.28) | 43 (30.50) | 13 (9.22) |
| Variable | Anxiety | Depression | Insomnia | Overall Psychological Problems |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age | 0.99 (0.95–1.03) | 0.98 (0.95–1.02) | 0.93 (0.86–0.99) * | 0.98 (0.95–1.01) |
| Gender | ||||
| Male | REF | REF | REF | REF |
| Female | 1.01 (0.48–2.13) | 1.05 (0.55–2.02) | 1.64 (0.61–4.38) | 1.46 (0.80–2.64) |
| Marital status | ||||
| Single | REF | REF | REF | REF |
| Married | 2.65 (1.02–6.90) * | 1.04 (0.55–1.97) | 0.80 (0.35–1.80) | 1.32 (0.75–2.35) |
| Widowed | - | - | - | - |
| Divorced | 8.1 (0.76–86.23) | - | - | 2.21 (0.23–20.89) |
| Number of people living with (people) | ||||
| 1–3 people | REF | REF | REF | REF |
| 4–5 people | 1.18 (0.48–2.88) | 2.01 (0.86–4.69) | 1.65 (0.54–5.06) | 1.88 (0.91–3.88) |
| >5 people | 1.58 (0.61–4.09) | 1.72 (0.67–4.39) | 1.91 (0.58–6.36) | 2.16 (0.99–4.69) |
| Living area | ||||
| Village | REF | REF | REF | REF |
| Town | 1.18 (0.55–2.52) | 0.97 (0.49–1.94) | 1.22 (0.51–2.93) | 0.93 (0.52–1.68) |
| City | 0.51 (0.22–1.15) | 0.52 (0.26–1.04) | 0.47 (0.18–1.26) | 0.47 (0.26–0.85) * |
| Distance between home and main or regular place of work (meter) | ||||
| <1000 m | REF | REF | REF | REF |
| 1000–5000 m | 1.07 (0.47–2.39) | 1.14 (0.53–2.46) | 0.88 (0.35–2.21) | 1.26 (0.63–2.49) |
| 5000–10,000 m | 0.17 (0.04–0.79) * | 0.64 (0.25–1.66) | 0.22 (0.04–1.04) | 0.62 (0.27–1.46) |
| 5000–10,000 m | 0.59 (0.23–1.50) | 0.72 (0.31–1.69) | 0.49 (0.17–1.45) | 1.08 (0.53–2.20) |
| Education | ||||
| Lower Secondary/Upper Secondary | REF | REF | REF | REF |
| College | 1.35 (0.17–10.64) | 1.73 (0.22–13.57) | - | 1.29 (0.29–5.82) |
| University | 0.93 (0.11–7.54) | 1.51 (0.19–11.96) | - | 1.09 (0.24–5.00) |
| Postgraduation | 1.88 (0.22–16.29) | 2.18 (0.26–18.60) | - | 1.18 (0.23–5.96) |
| Professional experience (years) | ||||
| <1 year | REF | REF | REF | REF |
| 1–2 year(s) | 0.38 (0.06–2.41) | 0.48 (0.13–1.78) | - | 0.69 (0.19–2.43) |
| 3–5 years | 0.74 (0.15–3.65) | 0.30 (0.08–1.07) | - | 0.48 (0.14–1.63) |
| 5–10 years | 0.75 (0.16–3.54) | 0.55 (0.17–1.78) | - | 0.76 (0.24–2.41) |
| >10 years | 0.56 (0.11–2.73) | 0.22 (0.06–0.80) * | - | 0.44 (0.13–1.46) |
| Current situation | ||||
| Being in quarantine zone doing nothing | REF | REF | REF | REF |
| Being in quarantine to care for the COVID-19 infected patient | 1.36 (0.43–4.26) | 1.03 (0.31–3.41) | 3.57 (0.74–17.08) | 2.01 (0.73–5.48) |
| Being in quarantine at home | 1.40 (0.42–4.65) | 1.63 (0.50–5.25) | 2.00 (0.35–11.30) | 1.93 (0.67–5.55) |
| Having ended the duration in quarantine and normally work | 0.68 (0.17–2.64) | 1.85 (0.60–5.72) | 2.75 (0.54–14.09) | 2.26 (0.82–6.26) |
| Normal working | 0.59 (0.21–1.71) | 0.96 (0.35–2.63) | 0.76 (0.15–3.73) | 1.06 (0.42–2.67) |
| Duration participating in COVID-19 control (weeks) | ||||
| <1 week | REF | REF | REF | REF |
| 1–2 week(s) | 0.99 (0.41–2.39) | 1.16 (0.53–2.52) | 1.07 (0.42–2.70) | 1.15 (0.59–2.27) |
| 2–4 weeks | 0.85 (0.34–2.11) | 0.89 (0.39–2.01) | 0.36 (0.11–1.16) | 0.89 (0.44–1.80) |
| 4–8 weeks | 0.85 (0.17–4.22) | 0.32 (0.04–2.62) | - | 0.71 (0.19–2.64) |
| >8 weeks | - | 0.27 (0.03–2.18) | 0.40 (0.05–3.34) | 0.38 (0.08–1.76) |
| Working directly in contact with COVID-19 patients frequently | ||||
| No | REF | REF | REF | REF |
| Yes | 1.85 (0.89–3.85) | 1.57 (0.81–3.05) | 2.65 (1.19–5.91) * | 1.93 (1.10–3.35) * |
| Level of preparation before participating in COVID-19 control | ||||
| None | REF | REF | REF | REF |
| Average | 0.57 (0.21–1.59) | 0.76 (0.28–2.09) | 0.78 (0.22–2.73) | 0.79 (0.33–1.89) |
| Adequate | 0.20 (0.06–0.67) ** | 0.35 (0.12–1.07) | 0.20 (0.04–0.94) * | 0.34 (0.13–0.89) * |
| Level of equipment in current workplace conditions | ||||
| None | REF | REF | REF | REF |
| Average | 0.73 (0.16–3.33) | 0.23 (0.08–0.64) ** | 1.18 (0.15–9.29) | 0.35 (0.12–0.97) * |
| Adequate | 0.31 (0.06–1.53) | 0.10 (0.03–0.31) *** | 0.39 (0.04–3.41) | 0.17 (0.06–0.50) ** |
| Affected by workplace conditions | ||||
| No | REF | REF | REF | REF |
| Yes | 4.18 (1.72–10.13) ** | 1.83 (0.98–3.41) | 6.26 (1.87–20.95) ** | 2.28 (1.32–3.95) ** |
| Affected a lot by the community | ||||
| No | REF | REF | REF | REF |
| Yes | 11.60 (4.07–33.06) *** | 2.62 (1.43–4.79) ** | 16.72 (3.93–71.11) *** | 3.50 (2.06–5.96) *** |
| Feeling stressed about current works | ||||
| No | REF | REF | REF | REF |
| Yes | 6.83 (3.08–15.14) *** | 6.85 (3.44–13.62) *** | - | 8.84 (4.81–16.23) *** |
| Feeling anxious about current works | ||||
| No | REF | REF | REF | REF |
| Yes | 4.98 (2.47–10.06) *** | 6.37 (3.36–12.07) *** | 13.33 (4.56–38.96) *** | 5.66 (3.35–9.57) *** |
| Feeling sad about current works | ||||
| No | REF | REF | REF | REF |
| Yes | 5.62 (2.89–10.96) *** | 7.62 (4.18–13.89) *** | 10.87 (4.67–25.33) *** | 7.03 (4.21–11.74) *** |
| Variable | Anxiety | Depression | Insomnia | Overall Psychological Problems |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age | 1.06 (0.98–1.13) | 0.93 (0.85–1.02) | ||
| Gender | ||||
| Male | REF | REF | ||
| Female | 1.89 (0.79–4.47) | |||
| Heathcare workforce | ||||
| Physician | REF | REF | REF | |
| Nurse | 0.40 (0.18–0.90) * | 0.38 (0.18–0.80) * | 3.69 (1.14–11.93) * | |
| Technician | 0.08 (0.02–0.44) ** | |||
| Marital status | ||||
| Single | REF | REF | ||
| Married | 2.76 (0.95–8.03) | |||
| Widowed | ||||
| Divorced | 13.82 (0.97–196.30) | |||
| Number of people living with (people) | ||||
| 1–3 people | REF | REF | ||
| 4–5 people | 2.11 (1.07–4.14) * | 1.45 (0.83–2.54) | ||
| >5 people | ||||
| Living area | ||||
| Village | REF | REF | ||
| Town | ||||
| City | 0.46 (0.19–1.10) | 0.45 (0.24–0.86) * | ||
| Distance between home and main or regular place of work (meter) | ||||
| <1000 m | REF | REF | REF | REF |
| 1000–5000 m | 2.16 (0.99–4.71) | 1.95 (0.99–3.85) | 2.77 (1.05–7.29) * | 1.93 (1.08–3.45) * |
| 5000–10,000 m | 0.33 (0.07–1.54) | |||
| 5000–10,000 m | ||||
| Education | ||||
| Lower Secondary/Upper Secondary | REF | REF | REF | |
| College | 0.58 (0.26–1.32) | |||
| University | 7.88 (1.37–45.30) * | |||
| Postgraduation | ||||
| Professional experience (years) | ||||
| <1 year | REF | REF | REF | |
| 1–2 year(s) | 3.69 (0.96–14.24) | |||
| 3–5 years | 0.47 (0.20–1.13) | 0.54 (0.27–1.08) | ||
| 5–10 years | ||||
| >10 years | 0.24 (0.07–0.84) * | |||
| Current situation | ||||
| Being in quarantine zone doing nothing | REF | REF | REF | REF |
| Being in quarantine to care for the COVID-19 infected patient | ||||
| Being in quarantine at home | 2.11 (0.74–5.94) | 2.20 (0.87–5.57) | 2.28 (1.01–5.16) * | |
| Having ended the duration in quarantine and normally work | 2.14 (0.68–6.70) | |||
| Normal working | ||||
| Duration participating in COVID-19 control (weeks) | ||||
| <1 week | REF | REF | ||
| 1–2 week(s) | ||||
| 2–4 weeks | 0.28 (0.09–0.89) * | |||
| 4–8 weeks | ||||
| >8 weeks | 0.31 (0.06–1.56) | |||
| Working directly in contact with COVID-19 patients frequently | ||||
| No | REF | REF | ||
| Yes | 3.39 (1.17–9.86) * | 1.77 (0.93–3.37) | ||
| Level of preparation before participating in COVID-19 control | ||||
| None | REF | REF | REF | |
| Average | 2.25 (0.78–6.48) | 1.58 (0.86–2.92) | ||
| Adequate | 0.51 (0.20–1.27) | |||
| Level of equipment in current workplace conditions | ||||
| None | REF | REF | ||
| Average | 0.19 (0.05–0.69) * | 0.45 (0.14–1.45) | ||
| Adequate | 0.12 (0.03–0.47) ** | |||
| Affected by workplace conditions | ||||
| No | REF | |||
| Yes | ||||
| Affected a lot by the community | ||||
| No | REF | REF | REF | |
| Yes | 5.39 (1.70–17.11) ** | 4.26 (0.91–19.95) | ||
| Feeling stressed about current works | ||||
| No | REF | REF | REF | |
| Yes | 2.66 (0.98–7.25) | 2.47 (0.99–6.17) | 4.84 (2.40–9.75) *** | |
| Feeling anxious about current works | ||||
| No | REF | REF | ||
| Yes | 2.52 (1.07–5.92) * | |||
| Feeling sad about current works | ||||
| No | REF | REF | REF | REF |
| Yes | 1.91 (0.80–4.58) | 3.71 (1.72–7.98) ** | 2.28 (0.86–6.00) | 3.24 (1.76–6.00) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuan, N.Q.; Phuong, N.D.; Co, D.X.; Son, D.N.; Chinh, L.Q.; Dung, N.H.; Thach, P.T.; Thai, N.Q.; Thu, T.A.; Tuan, N.A.; et al. Prevalence and Factors Associated with Psychological Problems of Healthcare Workforce in Vietnam: Findings from COVID-19 Hotspots in the National Second Wave. Healthcare 2021, 9, 718. https://doi.org/10.3390/healthcare9060718
Tuan NQ, Phuong ND, Co DX, Son DN, Chinh LQ, Dung NH, Thach PT, Thai NQ, Thu TA, Tuan NA, et al. Prevalence and Factors Associated with Psychological Problems of Healthcare Workforce in Vietnam: Findings from COVID-19 Hotspots in the National Second Wave. Healthcare. 2021; 9(6):718. https://doi.org/10.3390/healthcare9060718
Chicago/Turabian StyleTuan, Nguyen Quang, Nguyen Doan Phuong, Dao Xuan Co, Do Ngoc Son, Luong Quoc Chinh, Nguyen Huu Dung, Pham The Thach, Nguyen Quoc Thai, Truong Anh Thu, Nguyen Anh Tuan, and et al. 2021. "Prevalence and Factors Associated with Psychological Problems of Healthcare Workforce in Vietnam: Findings from COVID-19 Hotspots in the National Second Wave" Healthcare 9, no. 6: 718. https://doi.org/10.3390/healthcare9060718