
Efficacy of the mRNA-Based BNT162b2 COVID-19 Vaccine in Patients with Solid Malignancies Treated with Anti-Neoplastic Drugs

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Partipants
2.2. Assessment of Anti-SARS-CoV-2 Antibodies
2.3. Statistical Analysis
3. Results
3.1. Study Population
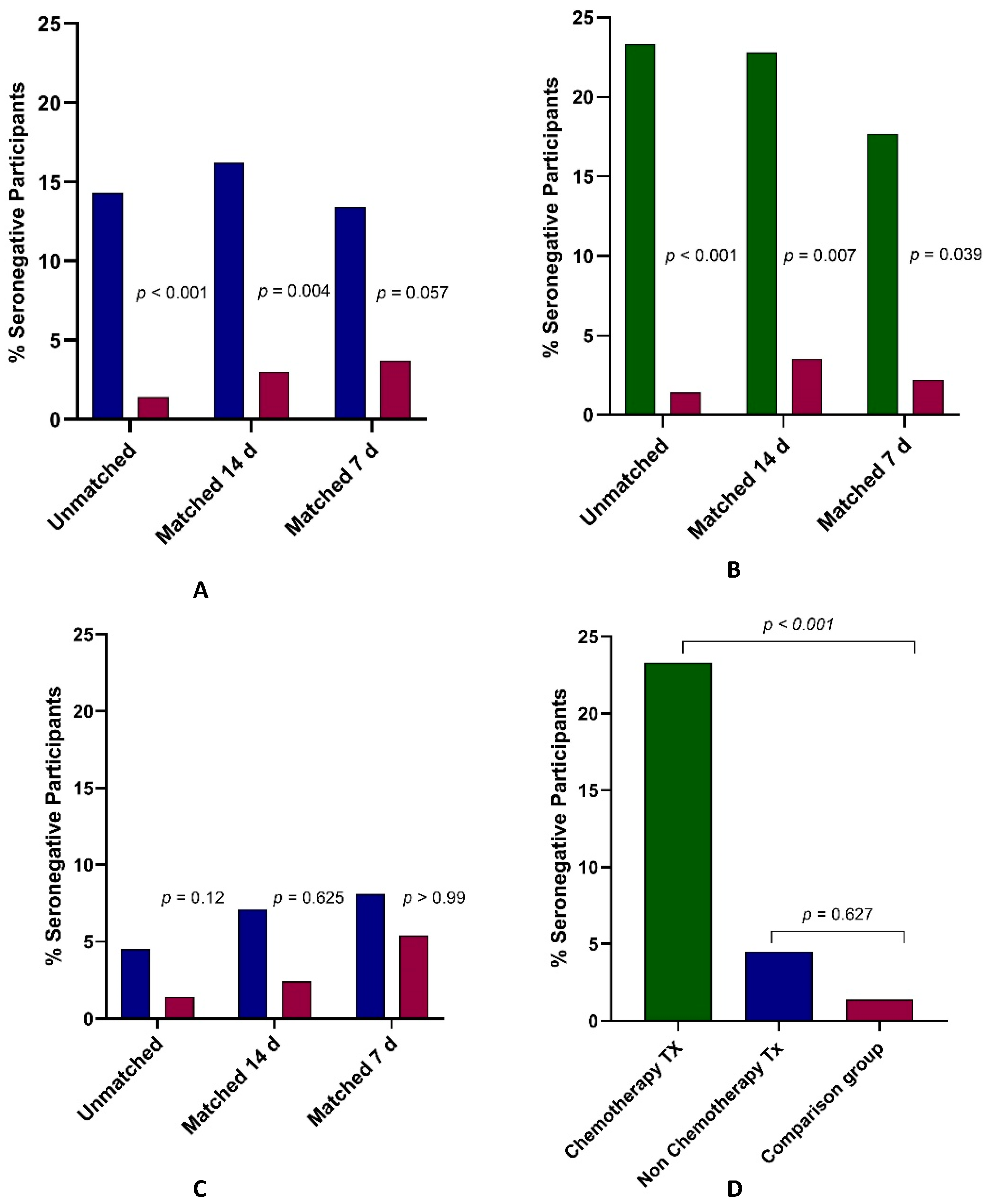
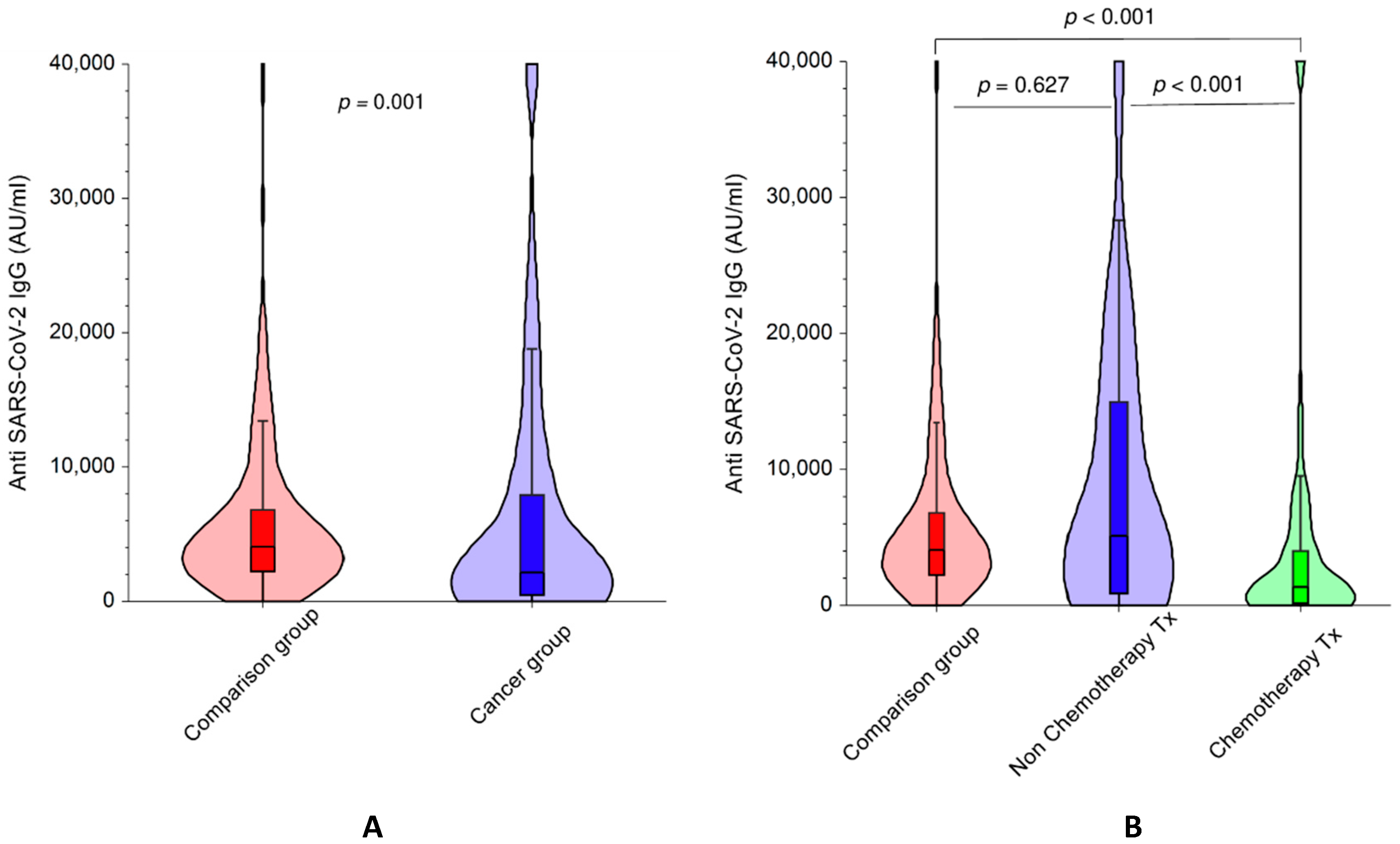
3.2. Response to BNT162b2 in Patients with Cancer versus Participants without A Cancer Diagnosis
3.3. Response to BNT162b2 in Cancer Patients Receiving Chemotherapy versus Participants without Cancer
3.4. Response to BNT162b2 in Cancer Patients Receiving Non-Chemotherapy Regimens versus Participants without Cancer
3.5. Response to BNT162b2 in Cancer Patients Receiving Chemotherapy versus Non-Chemotherapy Regimens
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coronavirus Resource Center. John Hopkins University & Medicine. Available online: https://coronavirus.jhu.edu/map.html (accessed on 26 March 2021).
- World Health Organization. WHO Director-General’s Opening Remarks at the Medica Briefing COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-11-march-2020 (accessed on 26 March 2021).
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Curigliano, G.; de Azambuja, E. Mortality in patients with cancer and coronavirus disease 2019: A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-based COVID-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.K.; Zhang, T.; Wang, A.Z.; Li, Z. COVID-19 vaccines for patients with cancer: Benefits likely outweigh risks. J. Hematol. Oncol. 2021, 14, 38. [Google Scholar] [CrossRef]
- Desai, A.; Gainor, J.F.; Hegde, A.; Schram, A.M.; Curigliano, G.; Pal, S.; Liu, S.V.; Halmos, B.; Groisberg, R.; Grande, E.; et al. COVID-19 vaccine guidance for patients with cancer participating in oncology clinical trials. Nat. Rev. Clin. Oncol. 2021, 18, 313–319. [Google Scholar] [CrossRef]
- National Cancer Institute. Coronavirus Vaccines and People with Cancer: A Q&A with Dr. Steven Pergam. Available online: https://www.cancer.gov/news-events/cancer-currents-blog/2021/people-with-cancer-coronavirus-vaccine (accessed on 29 March 2021).
- NCCN: Cancer and COVID-19 Vaccination. Recommendations of the NCCN COVID-19 Vaccination Advisory Committee Version 2.0. Available online: https://www.nccn.org/docs/default-source/covid-19/2021_covid-19_vaccination_guidance_v2-0.pdf?sfvrsn=b483da2b_2 (accessed on 10 March 2021).
- Centers for Disease Control and Prevention. Summary Document for Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/clinical-considerations.html (accessed on 16 April 2021).
- ASCO. COVID-19 Vaccines & Patients with Cancer. Available online: https://www.asco.org/asco-coronavirus-resources/covid-19-vaccines-patients-cancer (accessed on 16 April 2021).
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bornstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 Vaccine in Patients with Chronic Lymphocytic Leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Maneikis, K.; Šablauskas, K.; Ringelevičiūtė, U.; Vaitekėnaitė, V.; Čekauskienė, R.; Kryžauskaitė, L.; Naumovas, D.; Banys, V.; Pečeliūnas, V.; Beinortas, T.; et al. Immunogenicity of the BNT162b2 COVID-19 mRNA vaccine and early clinical outcomes in patients with haematological malignancies in Lithuania: A national prospective cohort study. Lancet Haematol. 2021, 8, e583–e592. [Google Scholar] [CrossRef]
- Agha, M.; Blake, M.; Chilleo, C.; Wells, A.; Haidar, G. Suboptimal response to COVID-19 mRNA vaccines in hematologic malignancies patients. medRxiv 2021. [Google Scholar] [CrossRef]
- Waissengrin, B.; Agbarya, A.; Safadi, E.; Padova, H.; Wolf, I. Short-term safety of the BNT162b2 mRNA COVID-19 vaccine in patients with cancer treated with immune checkpoint inhibitors. Lancet Oncol. 2021, 22, 581–583. [Google Scholar] [CrossRef]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; Del Moline Del Barrio, I.; Alaguthurai, T.; Domingo-Villa, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of seropositivity following BNT162b2 messenger RNA vaccination for SARS-CoV-2 in patients undergoing treatment for cancer. JAMA Oncol. 2021, 7, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Israel Ministry of Health. COVID-19 Vaccination Information. Available online: https://govextra.gov.il/ministry-of-health/covid19-vaccine/en-covid19-vaccination-information/ (accessed on 16 April 2021).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 vaccine in a nationwide mass vaccination setting. N. Eng. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Israel Association of Allergy and Clinical Immunology. Vaccination against COVID-19 Virus by Pfizer (BNT162b2) for Residents of the State of Israel. Available online: https://govextra.gov.il/media/29958/position-paper.pdf (accessed on 16 April 2021).
- Lord, J.M. The effect of ageing of the immune system on vaccination responses. Hum. Vaccin. Immunother. 2013, 9, 1364–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, S.L.; Jedlicka, A.; Pekosz, A. The Xs and Y of immune responses to viral vaccines. Lancet Infect. Dis. 2010, 10, 338–349. [Google Scholar] [CrossRef]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef]
- Yazaki, S.; Yoshida, T.; Kojima, Y.; Yagishita, S.; Nakahama, H.; Okinaka, K.; Matsushita, H.; Shiotsuka, M.; Kobayashi, O.; Iwata, S.; et al. Difference in SARS-CoV-2 antibody status between patients with cancer and health care workers during the COVID-19 pandemic in Japan. JAMA Oncol. 2021, 7, 1141–1148. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e2. [Google Scholar] [CrossRef]
- Castrucci, M.R. Factors affecting immune responses to the influenza vaccine. Hum. Vaccin. Immunother. 2018, 14, 637–646. [Google Scholar] [CrossRef]
- Vollaard, A.; Schreuder, I.; Slok-Raijmakers, L.; Slok-Raijmakers, L.; Opstelten, W.; Rimmelzwaan, G.; Gelderblom, H. Influenza vaccination in adult patients with solid tumours treated with chemotherapy. Eur. J. Cancer 2017, 76, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Dini, G.; Toletone, A.; Barberis, I.; Debarbieri, N.; Massa, E.; Paganino, C.; Bersi, F.; Montecucco, A.; Alicino, C.; Durando, P. Persistence of protective anti-HBs antibody levels and anamnestic response to HBV booster vaccination: A cross-sectional study among healthcare students 20 years following the universal immunization campaign in Italy. Hum. Vaccin. Immunother. 2017, 13, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Greub, G.; Zysset, F.; Genton, B.; Spertini, R.; Frei, P.C. Absence of anti-hepatitis B surface antibody after vaccination does not necessarily mean absence of immune response. Med. Microbiol. Immunol. 2001, 189, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transplant. 2021, 21, 2719–2726. [Google Scholar] [CrossRef] [PubMed]
- Lo Sasso, B.; Giglio, R.V.; Vidali, M.; Scazzone, C.; Bivona, G.; Gambino, C.M.; Ciaccio, A.M.; Agnello, L.; Ciaccio, M. Evaluation of Anti-SARS-CoV-2 S-RBD IgG Antibodies after COVID-19 mRNA BNT162b2 vaccine. Diagnostics 2021, 11, 1135. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Gal Levin, E.; Rubin, C.; Indenbaum, V.; et al. COVID-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir. Med. 2021, 9, 712–720. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.P.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T cell immunity in convalescent individuals with asymptomatic or mild COVID-19. Cell 2020, 183, 158–168.e14. [Google Scholar] [CrossRef]
- Shroff, R.T.; Chalasani, P.; Wei, R.; Pennington, D.; Quirk, G.; Schoenle, M.V.; Uhrlaub, J.L.; Ripperger, T.J.; Jergović, M.; Dalgai, S.; et al. Immune responses to COVID-19 mRNA vaccines in patients with solid tumors on active, immunosuppressive cancer therapy. medRxiv 2021. [Google Scholar] [CrossRef]
- Wilson, R.A.M.; Evans, T.R.J.; Fraser, A.R.; Nibbs, R.J.B. Immune checkpoint inhibitors: New strategies to checkmate cancer. Clin. Exp. Immunol. 2018, 191, 133–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Cancer Participants | Non-Cancer Participants | Statistical Test | p * |
|---|---|---|---|---|
| Number (n) | 140 | 215 | ||
| Age, mean (SD) [years] | 65.3 (1.4) | 62.5 (13) | t | 0.05 |
| Male [%] | 76 (54%) | 80 (37.2%) | χ2 | 0.002 |
| Time from second vaccine to test, median (IQR) [days] | 35 (23.5–45) | 51 (43–62) | Mann-Whitney | <0.001 |
| Type of Cancer, n (%) | ||||
| Gastrointestinal | 48 (34.2%) | |||
| Breast | 30 (21.4%) | |||
| Lung | 27 (19.3%) | |||
| Urinary | 13 (9.3%) | |||
| Gynecological | 9 (6.4%) | |||
| Other types | 13 (9.3%) | |||
| Treatment, n (%) | ||||
| Chemotherapy | 73 (52%) | |||
| Non-chemotherapy | 67 (48%) | |||
| Immunotherapy | 43 (30.7%) | |||
| Treatment type, n (%) | ||||
| Metastatic | 109 (77.8%) | |||
| Adjuvant | 23 (16.4%) | |||
| Neoadjuvant | 8 (5.7%) |
| Group | Analysis | Parameter | Cancer Participants | Non-Cancer Participants | Statistical Test | p |
|---|---|---|---|---|---|---|
| All Participants | Unmatched | Number (n) | 140 | 215 | ||
| Seronegative, n (%) | 20 (14.3) | 3 (1.4) | Fisher | <0.001 | ||
| IgG [AU], median (IQR) | 2231 (445–8023) | 4100 (2231–6774) | Mann-Whitney | 0.001 | ||
| Matched * 14 d | Number (n) | 99 | 99 | |||
| Seronegative, n (%) | 16 (16.2) | 3 (3) | McNemar | 0.004 | ||
| IgG [AU], median (IQR) | 1771 (284–7292) | 2993 (1775–6002) | Wilcoxon | 0.52 | ||
| Matched * 7 d | Number (n) | 82 | 82 | |||
| Seronegative, n (%) | 11 (13.4) | 3 (3.7) | McNemar | 0.057 | ||
| IgG [AU], median (IQR) | 1918 (414–7176) | 3677 (1842–6777) | Wilcoxon | 0.176 | ||
| Chemo Treated vs. Non-Cancer | Unmatched | Number (n) | 73 | 215 | ||
| Seronegative, n (%) | 17 (23.3) | 3 (1.4) | Fisher | <0.001 | ||
| IgG [AU], median (IQR) | 1361 (162–4030) | 4100 (2231–6774) | Mann-Whitney | <0.001 | ||
| Matched * 14 d | Number (n) | 57 | 57 | |||
| Seronegative, n (%) | 13 (22.8) | 2 (3.5) | McNemar | 0.007 | ||
| IgG [AU], median (IQR) | 821 (162–4177) | 3559 (1691–5957) | Wilcoxon | 0.035 | ||
| Matched * 7 d | Number (n) | 45 | 45 | |||
| Seronegative, n (%) | 8 (17.7) | 1 (2.2) | McNemar | 0.039 | ||
| IgG [AU], median (IQR) | 864 (256–4178) | 3329 (1691–7491) | Wilcoxon | 0.013 | ||
| Unmatched | Number (n) | 67 | 215 | |||
| Seronegative, n (%) | 3 (4.5) | 3 (1.4) | Fisher | 0.12 | ||
| IgG [AU], median (IQR) | 5088 (890–14925) | 4100 (2231–6774) | Mann-Whitney | 0.627 | ||
| Number (n) | 42 | 42 | ||||
| Seronegative, n (%) | 3 (7.1) | 1 (2.4) | McNemar | 0.625 | ||
| IgG [AU], median (IQR) | 3168 (573–10465) | 2977 (1920–6860) | Wilcoxon | 0.163 | ||
| Matched * 7 d | Number (n) | 37 | 37 | |||
| Seronegative, n (%) | 3 (8.1) | 2 (5.4) | McNemar | >0.99 | ||
| IgG [AU], median (IQR) | 3619 (851–10315) | 4792 (2117–6926) | Wilcoxon | 0.57 | ||
| Immuno Treated vs. Non-Cancer | Unmatched | Number (n) | 43 | 215 | ||
| Seronegative, n (%) | 3 (7) | 3 (1.4) | Fisher | 0.06 | ||
| IgG [AU], median (IQR) | 2714 (611–15564) | 4100 (2231–6774) | Mann-Whitney | 0.6 | ||
| Matched * 14 d | Number (n) | 26 | 26 | |||
| Seronegative, n (%) | 3 (11.5) | 1 (3.8) | McNemar | 0.625 | ||
| IgG [AU], median (IQR) | 2136 (443–8126) | 3066 (2014–7772) | Wilcoxon | 0.97 | ||
| Matched * 7 d | Number (n) | 21 | 21 | |||
| Seronegative, n (%) | 3 (14.3) | 2 (9.5) | McNemar | >0.99 | ||
| IgG [AU], median (IQR) | 1771 (434–7535) | 4066 (2081–6574) | Wilcoxon | 0.715 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbarya, A.; Sarel, I.; Ziv-Baran, T.; Agranat, S.; Schwartz, O.; Shai, A.; Nordheimer, S.; Fenig, S.; Shechtman, Y.; Kozlener, E.; et al. Efficacy of the mRNA-Based BNT162b2 COVID-19 Vaccine in Patients with Solid Malignancies Treated with Anti-Neoplastic Drugs. Cancers 2021, 13, 4191. https://doi.org/10.3390/cancers13164191
Agbarya A, Sarel I, Ziv-Baran T, Agranat S, Schwartz O, Shai A, Nordheimer S, Fenig S, Shechtman Y, Kozlener E, et al. Efficacy of the mRNA-Based BNT162b2 COVID-19 Vaccine in Patients with Solid Malignancies Treated with Anti-Neoplastic Drugs. Cancers. 2021; 13(16):4191. https://doi.org/10.3390/cancers13164191
Chicago/Turabian StyleAgbarya, Abed, Ina Sarel, Tomer Ziv-Baran, Sivan Agranat, Orna Schwartz, Ayelet Shai, Sharon Nordheimer, Shlomit Fenig, Yelena Shechtman, Ella Kozlener, and et al. 2021. "Efficacy of the mRNA-Based BNT162b2 COVID-19 Vaccine in Patients with Solid Malignancies Treated with Anti-Neoplastic Drugs" Cancers 13, no. 16: 4191. https://doi.org/10.3390/cancers13164191