
A Review of the Prevalence of Thromboembolic Complications among Pregnant Women Infected with COVID-19
 , , , and
, , , and
Abstract
:1. Introduction
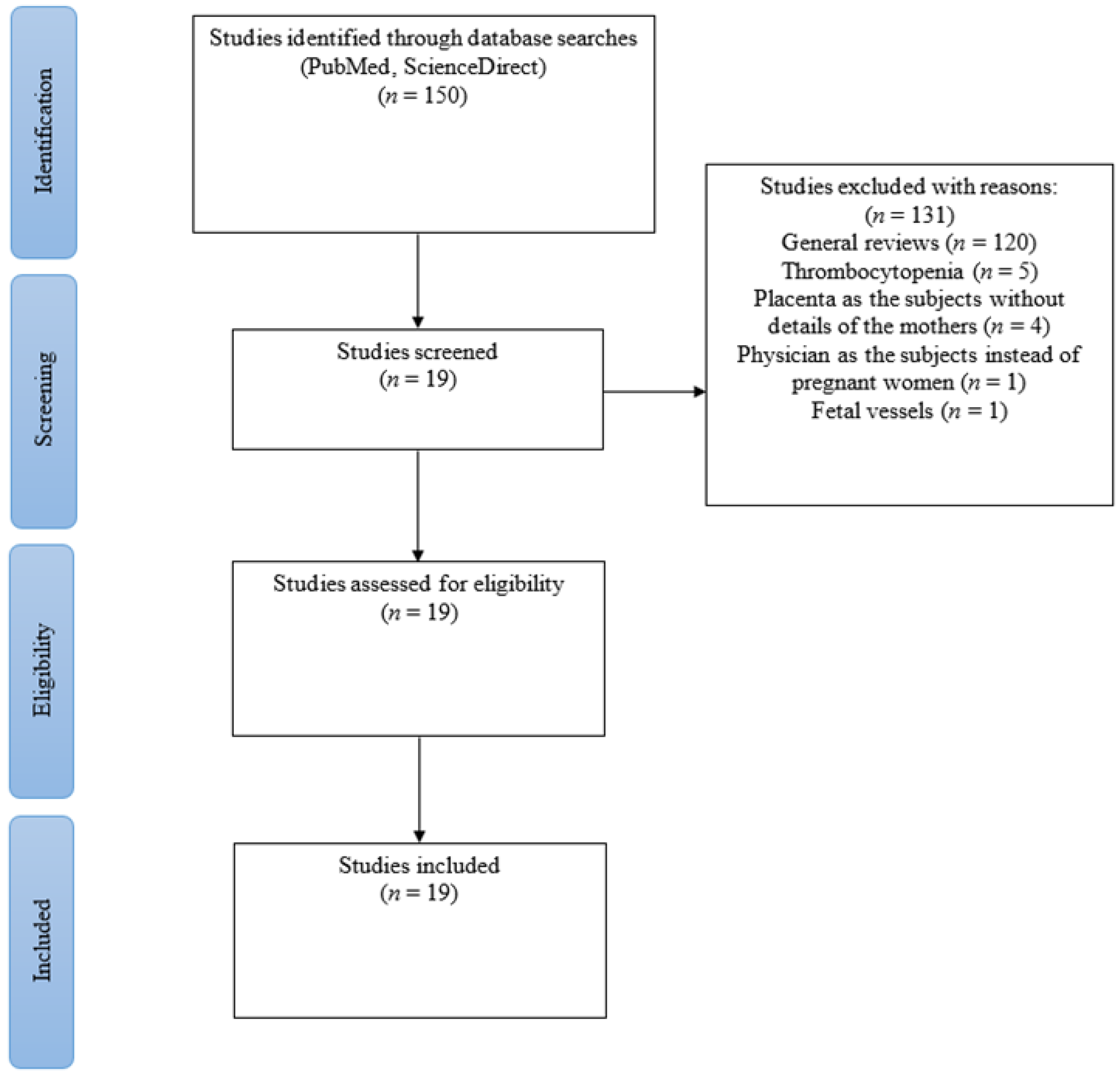
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Daru, J.; White, K.; Hunt, B.J. COVID-19, thrombosis and pregnancy. Thromb Update 2021, 5, 100077. [Google Scholar] [CrossRef]
- He, M.; Skaria, P.; Kreutz, K.; Chen, L.; Hagemann, I.S.; Carter, E.B.; Mysorekar, I.U.; Nelson, D.M.; Pfeifer, J.; Dehner, L.P. Histopathology of Third Trimester Placenta from SARS-CoV-2-Positive Women. Fetal Pediatr. Pathol. 2020, 41, 403–412. [Google Scholar] [CrossRef]
- Bain, E.; Wilson, A.; Tooher, R.; Gates, S.; Davis, L.J.; Middleton, P. Prophylaxis for venous thromboembolic disease in pregnancy and the early postnatal period. Cochrane Database Syst. Rev. 2014, 2, Cd001689. [Google Scholar] [CrossRef]
- Gabrieli, D.; Cahen-Peretz, A.; Shimonovitz, T.; Marks-Garber, K.; Amsalem, H.; Kalish, Y.; Lavy, Y.; Walfisch, A. Thromboembolic events in pregnant and puerperal women after COVID-19 lockdowns: A retrospective cohort study. Int. J. Gynaecol. Obs. 2021, 155, 95–100. [Google Scholar] [CrossRef]
- James, A.H. Pregnancy-associated thrombosis. Hematology 2009, 2009, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; Sivapalaratnam, S. Disseminated intravascular coagulation: An update on pathogenesis and diagnosis. Expert Rev. Hematol. 2018, 11, 663–672. [Google Scholar] [CrossRef]
- Morgen, E.K.; Fitzgerald, B.; Keating, S. Intervillous Thrombosis. In Pathology of the Placenta: A Practical Guide; Khong, T.Y., Mooney, E.E., Nikkels, P.G.J., Morgan, T.K., Gordijn, S.J., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 67–76. [Google Scholar] [CrossRef]
- Wu, Y.T.; Liu, J.; Xu, J.J.; Chen, Y.F.; Yang, W.; Chen, Y.; Li, C.; Wang, Y.; Liu, H.; Zhang, C.; et al. Neonatal outcome in 29 pregnant women with COVID-19: A retrospective study in Wuhan, China. PLoS Med. 2020, 17, e1003195. [Google Scholar] [CrossRef]
- Servante, J.; Swallow, G.; Thornton, J.G.; Myers, B.; Munireddy, S.; Malinowski, A.K.; Othman, M.; Li, W.; O’Donoghue, K.; Walker, K.F. Haemostatic and thrombo-embolic complications in pregnant women with COVID-19: A systematic review and critical analysis. BMC Pregnancy Childbirth 2021, 21, 108. [Google Scholar] [CrossRef]
- Gulersen, M.; Prasannan, L.; Tam Tam, H.; Metz, C.N.; Rochelson, B.; Meirowitz, N.; Shan, W.; Edelman, M.; Millington, K.A. Histopathologic evaluation of placentas after diagnosis of maternal severe acute respiratory syndrome coronavirus 2 infection. Am. J. Obs. Gynecol. MFM 2020, 2, 100211. [Google Scholar] [CrossRef]
- Pereira, A.; Cruz-Melguizo, S.; Adrien, M.; Fuentes, L.; Marin, E.; Perez-Medina, T. Clinical course of coronavirus disease-2019 in pregnancy. Acta Obs. Gynecol. Scand 2020, 99, 839–847. [Google Scholar] [CrossRef]
- Jani, S.; Jacques, S.M.; Qureshi, F.; Natarajan, G.; Bajaj, S.; Velumula, P.; Agu, C.; Bajaj, M. Clinical Characteristics of Mother–Infant Dyad and Placental Pathology in COVID-19 Cases in Predominantly African American Population. Am. J. Perinatol. Rep. 2021, 11, e15–e20. [Google Scholar] [CrossRef]
- Smithgall, M.C.; Liu-Jarin, X.; Hamele-Bena, D.; Cimic, A.; Mourad, M.; Debelenko, L.; Chen, X. Third-trimester placentas of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-positive women: Histomorphology, including viral immunohistochemistry and in-situ hybridization. Histopathology 2020, 77, 994–999. [Google Scholar] [CrossRef]
- Metz, T.D.; Clifton, R.G.; Hughes, B.L.; Sandoval, G.; Saade, G.R.; Grobman, W.A.; Manuck, T.A.; Miodovnik, M.; Sowles, A.; Clark, K.; et al. Disease Severity and Perinatal Outcomes of Pregnant Patients With Coronavirus Disease 2019 (COVID-19). Obs. Gynecol. 2021, 137, 571–580. [Google Scholar] [CrossRef]
- Litman, E.A.; Yin, Y.; Nelson, S.J.; Capbarat, E.; Kerchner, D.; Ahmadzia, H.K. Adverse perinatal outcomes in a large United States birth cohort during the COVID-19 pandemic. Am. J. Obstet. Gynecol. MFM 2022, 4, 100577. [Google Scholar] [CrossRef]
- Koumoutsea, E.V.; Vivanti, A.J.; Shehata, N.; Benachi, A.; Le Gouez, A.; Desconclois, C.; Whittle, W.; Snelgrove, J.; Malinowski, A.K. COVID-19 and acute coagulopathy in pregnancy. J. Thromb Haemost 2020, 18, 1648–1652. [Google Scholar] [CrossRef]
- Skalska-Świstek, M.; Huras, H.; Jaworowski, A.P.; Świstek, R.; Kołak, M. COVID-19 Infection Complicated by Disseminated Intravascular Coagulation during Pregnancy-Two Cases Report. Diagnostics 2022, 12, 655. [Google Scholar] [CrossRef]
- Mulvey, J.J.; Magro, C.M.; Ma, L.X.; Nuovo, G.J.; Baergen, R.N. Analysis of complement deposition and viral RNA in placentas of COVID-19 patients. Ann. Diagn. Pathol. 2020, 46, 151530. [Google Scholar] [CrossRef]
- Menter, T.; Mertz, K.D.; Jiang, S.; Chen, H.; Monod, C.; Tzankov, A.; Waldvogel, S.; Schulzke, S.M.; Hösli, I.; Bruder, E. Placental Pathology Findings during and after SARS-CoV-2 Infection: Features of Villitis and Malperfusion. Pathobiology 2021, 88, 69–77. [Google Scholar] [CrossRef]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am. J. Clin. Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef]
- Goudarzi, S.; Firouzabadi, F.D.; Mahmoudzadeh, F.; Aminimoghaddam, S. Pulmonary embolism in pregnancy with COVID-19 infection: A case report. Clin. Case Rep. 2021, 9, 1882–1886. [Google Scholar] [CrossRef]
- Kripalani, Y.; Parulekar, L. Pulmonary Embolism in a COVID-19-Positive Primigravida After Caesarean Section Despite Prophylaxis. Eur. J. Case Rep. Intern. Med. 2021, 8, 002684. [Google Scholar] [CrossRef]
- Mongula, J.E.; Frenken, M.W.E.; van Lijnschoten, G.; Arents, N.L.A.; de Wit-Zuurendonk, L.D.; Schimmel-de Kok, A.P.A.; van Runnard Heimel, P.J.; Porath, M.M.; Goossens, S. COVID-19 during pregnancy: Non-reassuring fetal heart rate, placental pathology and coagulopathy. Ultrasound Obs. Gynecol. 2020, 56, 773–776. [Google Scholar] [CrossRef]
- Ahmed, I.; Azhar, A.; Eltaweel, N.; Tan, B.K. First COVID-19 maternal mortality in the UK associated with thrombotic complications. Br. J. Haematol. 2020, 190, e37–e38. [Google Scholar] [CrossRef]
- Marinho, P.S.; da Cunha, A.J.L.A.; Chimelli, L.; Avvad-Portari, E.; Andreiuolo, F.d.M.; de Oliveira-Szejnfeld, P.S.; Mendes, M.A.; Gomes, I.C.; Souza, L.R.Q.; Guimarães, M.Z.; et al. Case Report: SARS-CoV-2 Mother-to-Child Transmission and Fetal Death Associated With Severe Placental Thromboembolism. Front. Med. 2021, 8, 1315. [Google Scholar] [CrossRef]
- Martinelli, I.; Ferrazzi, E.; Ciavarella, A.; Erra, R.; Iurlaro, E.; Ossola, M.; Lombardi, A.; Blasi, F.; Mosca, F.; Peyvandi, F. Pulmonary embolism in a young pregnant woman with COVID-19. Thromb Res. 2020, 191, 36–37. [Google Scholar] [CrossRef]
- Wastnedge, E.A.N.; Reynolds, R.M.; van Boeckel, S.R.; Stock, S.J.; Denison, F.C.; Maybin, J.A.; Critchley, H.O.D. Pregnancy and COVID-19. Physiol. Rev. 2021, 101, 303–318. [Google Scholar] [CrossRef]
- Kadir, R.A.; Kobayashi, T.; Iba, T.; Erez, O.; Thachil, J.; Kazi, S.; Malinowski, A.K.; Othman, M. COVID-19 coagulopathy in pregnancy: Critical review, preliminary recommendations, and ISTH registry-Communication from the ISTH SSC for Women’s Health. J. Thromb Haemost 2020, 18, 3086–3098. [Google Scholar] [CrossRef]
- Gąsecka, A.; Borovac, J.A.; Guerreiro, R.A.; Giustozzi, M.; Parker, W.; Caldeira, D.; Chiva-Blanch, G. Thrombotic Complications in Patients with COVID-19: Pathophysiological Mechanisms, Diagnosis, and Treatment. Cardiovasc. Drugs 2021, 35, 215–229. [Google Scholar] [CrossRef]
- Arnett, S. What We Know about COVID-19 and the Inflammatory Response. 2021. Available online: https://www.drugtargetreview.com/article/85765/what-we-know-about-covid-19-and-the-inflammatory-response/ (accessed on 1 October 2022).
- Lee, C.; Choi, W.J. Overview of COVID-19 inflammatory pathogenesis from the therapeutic perspective. Arch. Pharmacal Res. 2021, 44, 99–116. [Google Scholar] [CrossRef]
- Branchford, B.R.; Carpenter, S.L. The Role of Inflammation in Venous Thromboembolism. Front. Pediatr. 2018, 6, 142. [Google Scholar] [CrossRef]
- Page, E.M.; Ariëns, R.A.S. Mechanisms of thrombosis and cardiovascular complications in COVID-19. Thromb Res. 2021, 200, 1–8. [Google Scholar] [CrossRef]
- What Is Sepsis? Available online: https://www.cdc.gov/sepsis/what-is-sepsis.html#:~:text=Sepsis%20is%20the%20body’s%20extreme,%2C%20skin%2C%20or%20gastrointestinal%20tract (accessed on 1 October 2022).
- Barbara Stepko. Protect Yourself from Sepsis. Available online: https://www.aarp.org/health/conditions-treatments/info-2018/sepsis-prevention-tips.html#:~:text=Sepsis%20is%20a%20complication%20that,bloodstream%20to%20fight%20the%20infection (accessed on 1 October 2022).
- Fabregues, F.; Peñarrubia, J. Assisted reproduction and thromboembolic risk in the COVID-19 pandemic. Reprod. Biomed. Online 2020, 41, 361–364. [Google Scholar] [CrossRef]
- Jevtic, S.D.; Malinowski, A.K.; Othman, M.; Abdul Kadir, R.A. Physician experiences in management of COVID-19-associated coagulopathy in pregnancy: Communication from the ISTH SSC Subcommittee on Women’s Health Issues in Thrombosis and Haemostasis. J. Thromb Haemost 2021, 19, 2539–2545. [Google Scholar] [CrossRef]
- Lorini, F.L.; Di Matteo, M.; Gritti, P.; Grazioli, L.; Benigni, A.; Zacchetti, L.; Bianchi, I.; Fabretti, F.; Longhi, L. Coagulopathy and COVID-19. Eur. Heart J. Suppl. 2021, 23, E95–E98. [Google Scholar] [CrossRef]
- Mackman, N. New insights into the mechanisms of venous thrombosis. J. Clin. Investig. 2012, 122, 2331–2336. [Google Scholar] [CrossRef]
- Resta, L.; Vimercati, A.; Cazzato, G.; Mazzia, G.; Cicinelli, E.; Colagrande, A.; Fanelli, M.; Scarcella, S.V.; Ceci, O.; Rossi, R. SARS-CoV-2 and Placenta: New Insights and Perspectives. Viruses 2021, 13, 723. [Google Scholar] [CrossRef]
- Ko, J.Y.; DeSisto, C.L.; Simeone, R.M.; Ellington, S.; Galang, R.R.; Oduyebo, T.; Gilboa, S.M.; Lavery, A.M.; Gundlapalli, A.V.; Shapiro-Mendoza, C.K. Adverse Pregnancy Outcomes, Maternal Complications, and Severe Illness Among US Delivery Hospitalizations With and Without a Coronavirus Disease 2019 (COVID-19) Diagnosis. Clin. Infect. Dis. 2021, 73, S24–S31. [Google Scholar] [CrossRef]
- Levitan, D.; London, V.; McLaren, R.A.; Mann, J.D.; Cheng, K.; Silver, M.; Balhotra, K.S.; McCalla, S.; Loukeris, K. Histologic and Immunohistochemical Evaluation of 65 Placentas From Women With Polymerase Chain Reaction-Proven Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Arch. Pathol. Lab. Med. 2021, 145, 648–656. [Google Scholar] [CrossRef]
- Zhang, P.; Salafia, C.; Heyman, T.; Salafia, C.; Lederman, S.; Dygulska, B. Detection of severe acute respiratory syndrome coronavirus 2 in placentas with pathology and vertical transmission. Am. J. Obstet. Gynecol. MFM 2020, 2, 100197. [Google Scholar] [CrossRef]
- What Is Venous Thromboembolism? Available online: https://www.cdc.gov/ncbddd/dvt/facts.html (accessed on 1 October 2022).
- Wang, Y.; Liang, X.; Wang, H.; Li, L.; Xiong, G.; Mi, L. A considerable asymptomatic proportion and thromboembolism risk of pregnant women with COVID-19 infection in Wuhan, China. J. Perinat. Med. 2021, 49, 237–240. [Google Scholar] [CrossRef]
- Klovaite, J.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Benn, M. Elevated fibrinogen levels are associated with risk of pulmonary embolism, but not with deep venous thrombosis. Am. J. Respir. Crit. Care Med. 2013, 187, 286–293. [Google Scholar] [CrossRef]
- VTE Clinical Practice Guideline: Prevention and Treatment of Venous Thromboembolism. 2013. Available online: https://www.moh.gov.my/moh/attachments/9005.pdf (accessed on 1 October 2022).
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb Haemost 2020, 18, 1023–1026. [Google Scholar] [CrossRef] [Green Version]
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Thachil, J.; Giannis, D.; et al. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb Haemost 2020, 18, 1859–1865. [Google Scholar] [CrossRef]
- Simcox, L.E.; Ormesher, L.; Tower, C.; Greer, I.A. Pulmonary thrombo-embolism in pregnancy: Diagnosis and management. Breathe 2015, 11, 282–289. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19), Treatment Guidelines, National Institutes of Health. 2022. Available online: https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf (accessed on 1 October 2022).


{kind=link}
| Study Design |
| Term of Pregnancy during Admission (Prepartum/Postpartum/Gestational Age) | Term of Pregnancy during Thrombotic Event (Prepartum/Postpartum) | Comorbidities/ Medical History | Clinical Presentations |
|---|---|---|---|---|---|---|
| Case series |
| Prepartum | Prepartum | - | - |
| Case series |
| 34–35 weeks | Prepartum | Hypothyroidism diagnosed in first trimester | - |
| Case series |
| Prepartum | Postpartum | - | - |
| Case series |
| Prepartum | Postpartum | - | - |
| Case series |
| Postpartum | Postpartum | - | - |
| Case report |
| 30 weeks 5 days | Prepartum | - | Loss of consciousness, double mydriasis, tonic-clonic seizure |
| Case report |
| 38 weeks 1 day | Postpartum | - | - |
| Case report |
| 31–32 weeks | Prepartum | Type 1 diabetes with low dose insulin, pre-eclampsia in previous pregnancy | - |
| Case report |
| 29 weeks | Postpartum | Type 2 diabetes mellitus, renal tubular acidosis, asthma, vitamin D deficiency | - |
| Case report |
| 34 weeks 4 days | Postpartum | A history of previous bariatric surgery (Roux-en-Y gastric bypass) | - |
| Case report |
| 29 weeks | Prepartum | - | - |
|
|
| Term of Pregnancy during Admission (Prepartum/Postpartum/ Gestational Age) | Term of Pregnancy during Thrombotic Events (Prepartum/Postpartum) | Comorbidities/Medical History of the Mothers |
|---|---|---|---|---|---|
|
|
| Third trimester | Postpartum | - |
|
|
| 35–41 weeks | Postpartum | - |
|
|
| Prepartum | Postpartum | - |
|
|
| Prepartum | Postpartum | - |
|
|
| Postpartum | Postpartum | Obesity, Hypertension, Pre-eclampsia, Diabetes, Hypothyroidism, Asthma |
|
|
| Prepartum | Prepartum | - |
|
|
| Prepartum | Prepartum | Asthma, Autoimmune disease, Chronic kidney disease, Diabetes Mellitus, Gestational diabetes mellitus, Gestational hypertension, Hypertension, Major mental illness, Pulmonary disease |
| Laboratory Findings | Prevalence of TE Complications (n) | Outcomes (Death/Alive) (n) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| D-Dimer (mg/L) NR: 0.1–1.7 | CRP (mg/L) NR: 0.1–10 | Fibrinogen (g/L) NR: 1.5–4.2 | Radiological Imaging Confirmation | DIC | PE | IVT | CAC | Placental Thrombosis | ||
| >20 | >37 | Elevated | - | - | - | - | 2 | - | All recovered |
| >34.47 | - | 3.1 | - | 2 | - | - | - | - | All discharged |
| - | - | - | Routine histopathology & complement staining: Frank thrombosis of fetal chorionic plate vessels | - | - | - | - | 5 | Mothers were discharged, unknown outcome for fetals |
| - | - | - | - | - | - | 1 | - | - | - |
| - | - | - | - | - | - | 6 | - | - | No maternal and neonatal death |
| High | - | 810 | - | - | 1 | - | - | - | Maternal death and fetal death in mother’s uterus |
| Elevated (1.8) | - | - | CTPA: signs of a hypodense filling defect, suggestive of pulmonary thromboembolism in theanterior basal and lateral basal segmental and subsegmental branches of the right lower lobar pulmonary artery | - | 1 | - | - | - | Discharged |
| >9.4 | >14 | 0.7–4.2 | - | - | - | - | 1 | - | Recovered and discharged |
| - | - | - | CTPA: revealed right lower lobar pulmonary embolism. | - | 1 | - | - | - | Death |
| 17.22 | - | 3530 | Fetal-placenta Magnetic Resonance Imaging: The placenta had a posterior uterine wall insertion, large and dilated vessels with massive thrombosis | - | - | 1 | - | - | Death |
| >15.8 | >28.1 | >5.43 | Chest CT scan:segmental pulmonary embolus in the right superior lobe, | - | 1 | - | - | - | Discharged |
| Laboratory Findings | Cases of TE Complications (n) | Outcomes (Death/Alive) (n) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| D-Dimer (mg/L) NR: 0.1–1.7 | CRP (mg/L) NR: 0.1–10 | Radiological Imaging Confirmation | DIC | PE | DVT | TE | IVT | SCT | CAC | ||
| - | - | - | - | - | - | - | 13 | - | - | - |
| - | 22.2 | - | - | - | - | - | - | - | 2 | All discharged |
| >1.9 | >60 | - | - | - | 2 | - | - | - | - | No maternal death |
| - | - | Placenta pathology: Small isolated intervillous thrombi were seen in seven (21%) placentas | - | - | - | - | 7 | - | - | - |
| - | - | - | - | - | - | - | 8 | 9 | - | - |
| - | - | - | - | - | - | 8 | - | - | - | - |
| - | - | - | 35 | - | - | 5 | - | - | - | Discharged home (2610) Post-acute care (37) Death (3) Rehab (8) Hospice (1) |
| Author’s Name | Study Design | Number of Patients Included (n) | Laboratory Findings | Cases of TE Complications (n) | Outcome (Death/Alive) (n) | |||
|---|---|---|---|---|---|---|---|---|
| D-Dimer (mg/L) NR: 0.1–1.7 | Fibrinogen (g/L) NR: 1.5–4.2 | DIC | PE | TE | ||||
| Servante, J., et al. [9] | Systematic review | 1063 mothers | >19.06 | <2.2 | 7 | 2 | 1 (Inferior vena cava) | 2 DIC cases reported dead |
| Author’s Name | Cases of TE Complications (n) | Types & Dose of Thromboprophylaxis | ||||
|---|---|---|---|---|---|---|
| DIC | PE | DVT | TE | CAC | ||
| Servante, J., et al. [9] | 7 | 2 | - | 1 (Inferior vena cava) | - | Enoxaparin 40 mg OD (n = 3) Therapeutic anticoagulation (n = 1) |
| Pereira, A., et al. [11] | - | - | 2 | - | - | LMWH (no information on type and dose) |
| Metz, T. D., et al. [14] | - | - | - | 8 | - | Prophylactic anticoagulant in 5 out of 8 TE patients (no information on type and dose) |
| Koumoutsea, E. V., et al. [16] | - | - | - | - | 2 | LMWH prophylactic dose |
| Skalska-Swistek, M., et al. [17] | 2 | - | - | - | - | LMWH prophylactic dose 2nd patient |
| Goudarzi, S., et al. [21] | - | 1 | - | - | - | No information |
| Kripalani, Y., et al. [22] | - | 1 | - | - | - | Enoxaparin 60 mg OD |
| Ahmed, I., et al. [24] | - | 1 | - | - | - | Enoxaparin (no information on dose) |
| Martinelli, I., et al. [26] | - | 1 | - | - | - | Enoxaparin 40 mg OD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohd Ariff, N.S.; Abdul Halim Zaki, I.; Mohd Noordin, Z.; Md Hussin, N.S.; Goh, K.W.; Ming, L.C.; Zulkifly, H.H. A Review of the Prevalence of Thromboembolic Complications among Pregnant Women Infected with COVID-19. J. Clin. Med. 2022, 11, 5934. https://doi.org/10.3390/jcm11195934
Mohd Ariff NS, Abdul Halim Zaki I, Mohd Noordin Z, Md Hussin NS, Goh KW, Ming LC, Zulkifly HH. A Review of the Prevalence of Thromboembolic Complications among Pregnant Women Infected with COVID-19. Journal of Clinical Medicine. 2022; 11(19):5934. https://doi.org/10.3390/jcm11195934
Chicago/Turabian StyleMohd Ariff, Nurul Syafiqah, Izzati Abdul Halim Zaki, Zakiah Mohd Noordin, Nur Sabiha Md Hussin, Khang Wen Goh, Long Chiau Ming, and Hanis Hanum Zulkifly. 2022. "A Review of the Prevalence of Thromboembolic Complications among Pregnant Women Infected with COVID-19" Journal of Clinical Medicine 11, no. 19: 5934. https://doi.org/10.3390/jcm11195934