
The Impact of COVID-19 Era on Pulmonary Embolism Patients: Increased Incidence of Hospitalizations and Higher Mortality—What Can Be Done?

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
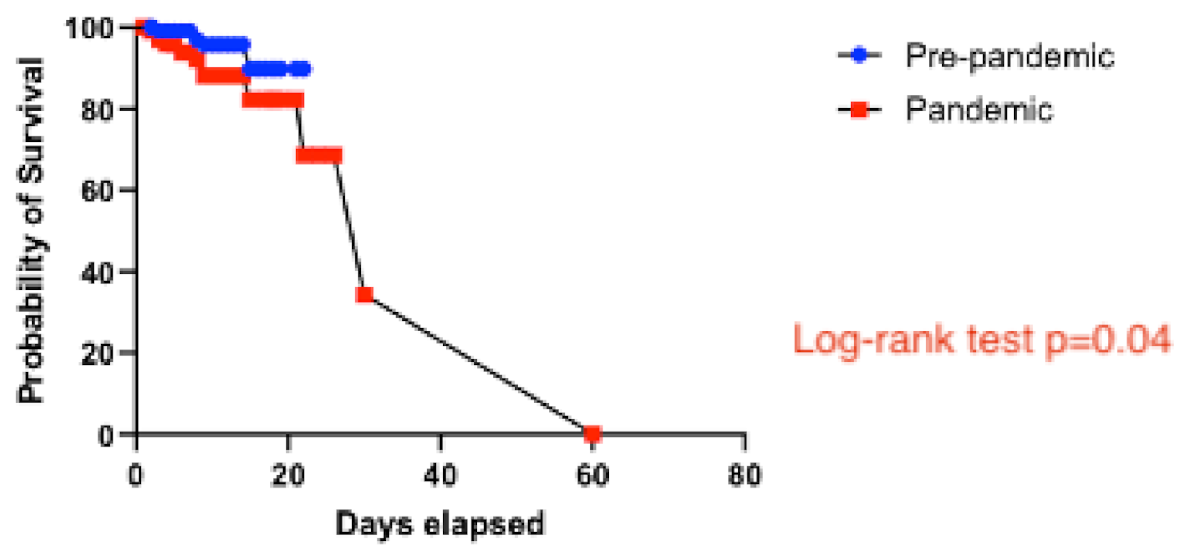
- Patients with PE had worse survival during the pandemic.
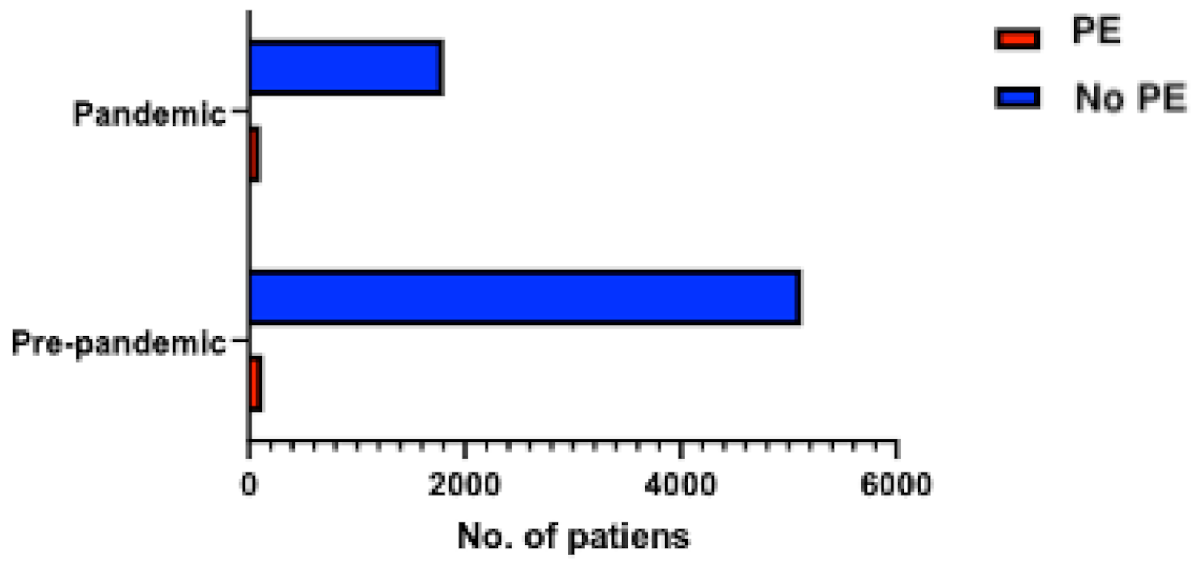
- There was an increased incidence of PE among hospitalizations in our cardiology unit during the COVID-19 pandemic;
- Patients hospitalized with PE during the pandemic were more likely to be obese;
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Respir. J. 2019, 54, 1901647. [Google Scholar] [CrossRef] [Green Version]
- Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Korompoki, E.; Fotiou, D.; Migkou, M.; Tzanninis, I.-G.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Emerging treatment strategies for COVID-19 infection. Clin. Exp. Med. 2020, 21, 167–179. [Google Scholar] [CrossRef]
- Hosseini, E.S.; Kashani, N.R.; Nikzad, H.; Azadbakht, J.; Bafrani, H.H.; Kashani, H.H. The novel coronavirus Disease-2019 (COVID-19): Mechanism of action, detection and recent therapeutic strategies. Virology 2020, 551, 1–9. [Google Scholar] [CrossRef]
- Scudiero, F.; Silverio, A.; Di Maio, M.; Russo, V.; Citro, R.; Personeni, D.; Cafro, A.; D’Andrea, A.; Attena, E.; Pezzullo, S.; et al. Pulmonary embolism in COVID-19 patients: Prevalence, predictors and clinical outcome. Thromb. Res. 2020, 198, 34–39. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Dengju, L.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopahty. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of Thrombotic Complications in Critically Ill ICU Patients with COVID-19. Thromb. Res. 2020, 19, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and thrombotic and thromboembolic disease: Implications for prevention, athithrombotic therapy, and follow-up: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- Canonico, M.E.; Siciliano, R.; Scudiero, F.; Sanna, G.D.; Parodi, G. The tug-of-war between coagulopathy and anticoagulant agents in patients with COVID-19. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.-Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the cardiovascular system: Acute and long-term implications. Eur. Heart J. 2020, 41, 1798–1800. [Google Scholar] [CrossRef] [Green Version]
- Gressenberger, P.; Gary, T.; Raggam, R.B.; Borenich, A.; Brodmann, M. Significant increase in the incidence of high-risk pulmonary embolism during the COVID-19 shutdown: The pandemic response causes serious collateral consequences. Eur. J. Intern. Med. 2020, 82, 120–122. [Google Scholar] [CrossRef]
- Watchmaker, J.M.; Goldman, D.T.; Lee, J.Y.; Choi, S.; Mills, A.C.; Toussie, D.; Finkelstein, M.; Sher, A.R.; Jacobi, A.H.; Bernheim, A.M.; et al. Increased Incidence of Acute Pulmonary Embolism in Emergency Department Patients During the COVID-19 Pandemic. Acad. Emerg. Med. 2020, 27, 1340–1343. [Google Scholar] [CrossRef]
- Boeken, T.; Le Berre, A.; Mebazaa, A.; Boulay-Coletta, I.; Hodel, J.; Zins, M. Non-COVID-19 emergencies: Where have all the patients gone? Eur. Radiol. 2020, 30, 5220–5221. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, C.; Maglietta, G.; Meschi, T.; Ticinesi, A.; Silva, M.; Sverzellati, N. Effects of the COVID-19 Epidemic on Hospital Admissions for Non-Communicable Diseases in a Large Italian University-Hospital: A Descriptive Case-Series Study. J. Clin. Med. 2021, 10, 880. [Google Scholar] [CrossRef] [PubMed]
- Santi, L.; Golinelli, D.; Tampieri, A.; Farina, G.; Greco, M.; Rosa, S.; Beleffi, M.; Biavati, B.; Campinoti, F.; Guerrini, S.; et al. Non-COVID-19 patients in times of pandemic: Emergency department visits, hospitalizations and cause-specific mortality in Northern Italy. PLoS ONE 2021, 16, e0248995. [Google Scholar] [CrossRef] [PubMed]
- Nopp, S.; Janata-Schwatczek, K.; Prosch, H.; Sjulym, I.; Konigsbrugge, O.; Pabinger, I.; Ay, C. Pulmonary embolsim during the COVID-19 pandemic: Decline in diagnostic procedures and incidence at a university hospital. Res. Pract. Thromb. Haemost. 2020, 4, 835–841. [Google Scholar] [CrossRef]
- Sindet-Pedersen, C.; Olesen, J.B.; Blanche, P.; Gerds, T.A.; Strange, J.E.; Butt, J.H.; El-Chouli, M.; Phelps, M.; Hansen, M.L.; Schou, M.; et al. Effect of government interventions to contain the COVID-19 pandemic on incidence of pulmonary embolism—A Danish nationwide register-based cohort study. Thromb. Res. 2021, 199, 97–100. [Google Scholar] [CrossRef]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A. Reduced rate of hospital admissions for ACS during Covid-19 outbreak in Northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B. Global pandemics interconnected—Obesity, impaired metabolic health and COVID-19. Nat. Rev. Endocrinol. 2021, 17, 135–149. [Google Scholar] [CrossRef]
- Senthilingam, M. Covid-19 has made the obesity epidemic worse, but failed to ignite enough action. BMJ 2021, 372, n411. [Google Scholar] [CrossRef]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: The pandemic response causes cardiac collateral damage. Eur. Heart J. 2020, 41, 1852–1853. [Google Scholar] [CrossRef] [Green Version]
- Balahura, A.M.; Guta, A.; Mihalcea, V.; Weiss, E.; Dorobanțu, M.; Bartoș, D.; Bădilă, E.; Dan, G.A. Pulmonary thromboembolism in an emergency hospital: Are our patients different? Rom. J. Internal Med. 2017, 55, 237–244. [Google Scholar] [CrossRef]
- Tilliridou, V.; Kirkbride, R.; Dickinson, R.; Tiernan, J.; Yong, G.L.; van Beek, E.J.; Murchison, J.T.; Williams, M.C. Pulmonary embolism severity before and during the COVID-19 pandemic. Br. J. Radiol. 2021, 94, 20210264. [Google Scholar] [CrossRef] [PubMed]
- Asamoah, K.T. Acute Pulmonary Embolism in the COVID-19 Era: The Experience of a Ghanaian Patient. J. Patient Exp. 2021, 8, 2374373521997230. [Google Scholar] [CrossRef]
- Aktaa, S.; Wu, J.; Nadarajah, R.; Rashid, M.; de Belder, M.; Deanfield, J.; Mamas, M.A.; Gale, C.P. Incidence and mortality due to thromboembolic events during the COVID-19 pandemic: Multi-sourced population-based health records cohort study. Thromb. Res. 2021, 202, 17–23. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pre-Pandemic Group (n = 107) | Pandemic Group (n = 127) | p-Value |
|---|---|---|---|
| Age (years) | 61 ± 16 | 61 ± 17 | 0.77 |
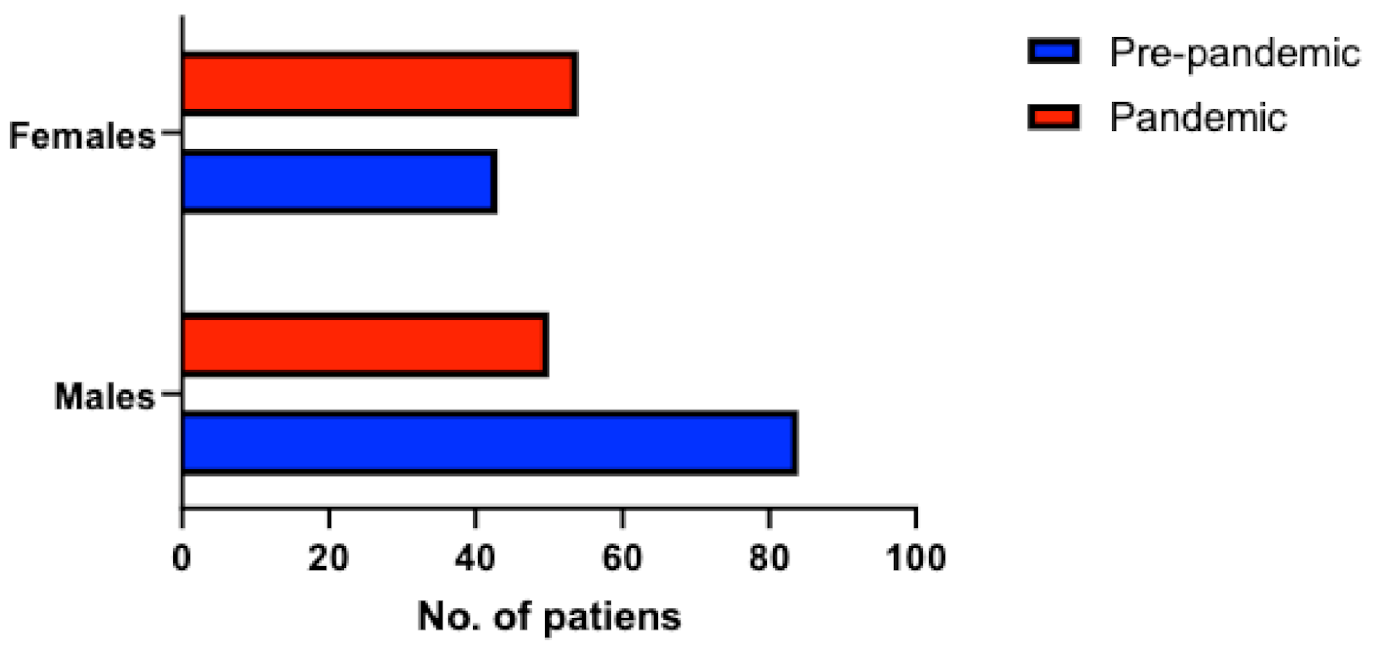
| Men, n (%) | 71 (66%) | 61 (48%) | 0.007 |
| Symptoms on Admission | |||
| Syncope, n (%) | 8 (7%) | 17 (13%) | 0.14 |
| Dyspnea, n (%) | 75 (70%) | 86 (68%) | 0.70 |
| Chest pain, n (%) | 33 (31%) | 31 (24%) | 0.27 |
| Hemodynamic instability, n (%) | 1 (1%) | 2 (2%) | 0.66 |
| PESI score | 88.8 ± 30.5 | 97.0 ± 43.2 | 0.09 |
| Predisposing Factors | |||
| Obesity, n (%) | 16 (15%) | 54 (43%) | <0.001 |
| Prolonged immobility, n (%) | 16 (15%) | 15 (12%) | 0.48 |
| Atrial fibrillation, n (%) | 12 (11%) | 13 (10%) | 0.81 |
| Cancer, n (%) | 26 (24%) | 24 (19%) | 0.32 |
| Thrombophilia, n (%) | 9 (8%) | 9 (7%) | 0.70 |
| History of previous PE, n (%) | 7 (7%) | 8 (6%) | 0.85 |
| Deep vein thrombosis, n (%) | 51 (48%) | 66 (52%) | 0.51 |
| Days of hospitalization | 10 (7–12.25) | 8 (6–11) | 0.07 |
| ECG Changes | Pre-Pandemic Group (n = 107) | Pandemic Group (n = 127) | p-Value |
|---|---|---|---|
| Newly developed RBBB, n (%) | 17 (16%) | 19 (15%) | 0.84 |
| ST elevation in precordial leads, n (%) | 0 (0%) | 1 (1%) | 0.55 |
| T wave inversion in precordial leads, n (%) | 20 (19%) | 38 (30%) | 0.07 |
| S1Q3T3 pattern, n (%) | 22 (21%) | 19 (15%) | 0.34 |
| Echocardiographic Changes | Pre-Pandemic Group (n = 107) | Pandemic Group (n = 127) | p-Value |
|---|---|---|---|
| Intracardiac thrombus, n (%) | 6 (6%) | 7 (6%) | 0.80 |
| TAPSE (mm) | 20 ± 4 | 20 ± 4 | 0.74 |
| RV diameter (mm) | 37 ± 10 | 38 ± 10 | 0.25 |
| RA diameter (mm) | 37 ± 9 | 37 ± 9 | 0.74 |
| RV-RA gradient (mm Hg) | 30 ± 12 | 30 ± 16 | 0.96 |
| Antithrombotic Treatment at Discharge | Pre-Pandemic Group (n = 103) | Pandemic Group (n = 113) | p-Value |
|---|---|---|---|
| Anti-vitamin K, n (%) | 30 (28%) | 32 (25%) | 0.98 |
| Rivaroxaban, n (%) | 32 (30%) | 29 (23%) | 0.47 |
| Apixaban, n (%) | 29 (27%) | 38 (30%) | 0.47 |
| Dabigatran, n (%) | 5 (5%) | 1 (1%) | 0.17 |
| LMWH, n (%) | 7 (7%) | 13 (10%) | 0.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vîjîiac, A.; Stănciulescu, D.I.; Băetu, A.E.; Grigore, I.-A.; Vintilă, D.; Cojocaru, C.; Bădilă, E.; Moldovan, H.; Scafa-Udriște, A. The Impact of COVID-19 Era on Pulmonary Embolism Patients: Increased Incidence of Hospitalizations and Higher Mortality—What Can Be Done? COVID 2021, 1, 357-365. https://doi.org/10.3390/covid1010030
Vîjîiac A, Stănciulescu DI, Băetu AE, Grigore I-A, Vintilă D, Cojocaru C, Bădilă E, Moldovan H, Scafa-Udriște A. The Impact of COVID-19 Era on Pulmonary Embolism Patients: Increased Incidence of Hospitalizations and Higher Mortality—What Can Be Done? COVID. 2021; 1(1):357-365. https://doi.org/10.3390/covid1010030
Chicago/Turabian StyleVîjîiac, Aura, Diana Irena Stănciulescu, Alexandru Emil Băetu, Iulia-Adelina Grigore, Denisa Vintilă, Cosmin Cojocaru, Elisabeta Bădilă, Horatiu Moldovan, and Alexandru Scafa-Udriște. 2021. "The Impact of COVID-19 Era on Pulmonary Embolism Patients: Increased Incidence of Hospitalizations and Higher Mortality—What Can Be Done?" COVID 1, no. 1: 357-365. https://doi.org/10.3390/covid1010030