


Abstract
Background: The exposure risks to front-line health care workers caring for patients with SARS-CoV-2 infection undergoing surgery or obstetric delivery are unclear, and an understanding of sample types that may harbour virus is important for evaluating risk. We sought to determine whether SARS-CoV-2 viral RNA from patients with SARS-CoV-2 infection undergoing surgery or obstetric delivery was present in the peritoneal cavity of male and female patients, in the female reproductive tract, in the environment of the surgery or delivery suite (surgical instruments or equipment used, air or floors), and inside the masks of the attending health care workers.
Methods: We conducted a cross-sectional study from November 2020 to May 2021 at 2 tertiary academic Toronto hospitals, during urgent surgeries or obstetric deliveries for patients with SARS-CoV-2 infection. The presence of SARS-CoV-2 viral RNA in patient, environmental and air samples was identified by real-time reverse transcription polymerase chain reaction (RT-PCR). Air samples were collected using both active and passive sampling techniques. The primary outcome was the proportion of health care workers’ masks positive for SARS-CoV-2 RNA. We included adult patients with positive RT-PCR nasal swab undergoing obstetric delivery or urgent surgery (from across all surgical specialties).
Results: A total of 32 patients (age 20–88 yr) were included. Nine patients had obstetric deliveries (6 cesarean deliveries), and 23 patients (14 male) required urgent surgery from the orthopedic or trauma, general surgery, burn, plastic surgery, cardiac surgery, neurosurgery, vascular surgery, gastroenterology and gynecologic oncology divisions. SARS-CoV-2 RNA was detected in 20 of 332 (6%) patient and environmental samples collected: 4 of 24 (17%) patient samples, 5 of 60 (8%) floor samples, 1 of 54 (2%) air samples, 10 of 23 (43%) surgical instrument or equipment samples, 0 of 24 cautery filter samples and 0 of 143 (95% confidence interval 0–0.026) inner surface of mask samples.
Interpretation: During the study period of November 2020 to May 2021, we found evidence of SARS-CoV-2 RNA in a small but important number of samples obtained in the surgical and obstetric operative environment. The finding of no detectable virus inside the masks worn by the health care teams would suggest a low risk of infection for health care workers using appropriate personal protective equipment.
While front-line health care workers are at risk of contracting infections when caring for patients with COVID-19,1–3 the risks to health care workers involved in surgery and obstetrics (work involving close, direct and often prolonged patient contact) remain unclear. Health care workers involved in surgery or obstetrics may be at risk of SARS-CoV-2 infections through the known vectors of respiratory droplets, aerosols and fomites,4–6 but infections may potentially be transmitted through exposure to the virus originating from the surgical field or the delivery itself.
SARS-CoV-2 is found in the respiratory tract of infected people.7–10 Additionally, the virus has been documented to be present in the gastrointestinal tract, and consequently, any bowel-related surgery that involves opening the gastrointestinal tract is thought to pose a risk to medical teams.11,12 There are also reports of SARS-CoV-2 detected in peritoneal fluid from patients with COVID-19 undergoing surgery.13,14 In the female reproductive tract, SARS-CoV-2 RNA has been identified in amniotic fluid and vaginal swabbing.15–18 Potentially, if the virus is present on peritoneal surfaces of males or females, in the female reproductive tract or other surgical sites, this virus could be aerosolized via cautery smoke or from the release of CO2 gas from laparoscopic procedures. Although there is no current published research on the presence of SARS-CoV-2 in surgical smoke, other viruses, including human papillomavirus, HIV-1 and hepatitis B virus, have been isolated from surgical smoke.19–28
The risk of aerosolization from the respiratory tract is recognized,29 but the risk of SARS-CoV-2 residing in the surgical site and the subsequent risk of aerosolizing this virus are not well studied. We studied the risk of contamination in the operating room and birthing suite by evaluating the risk of aerosolization from the respiratory tract or from the surgical or obstetric field during surgery, or labour and delivery. This information is key to assessing the risks to health care workers who care for such patients and may help guide best practices regarding the use of personal protective equipment and safety in the operating room and birthing room.
Our objectives were to determine whether SARS-CoV-2 RNA from patients with SARS-CoV-2 infection undergoing surgery or obstetric delivery was present in the peritoneal cavity of males and females, in the female reproductive tract, on surgical instruments or equipment, on procedure room floors, in bioaerosols produced during surgery or obstetric delivery, and inside surgical masks of the attending health care workers.
Methods
Study design
We conducted a cross-sectional study from November 2020 to May 2021. Patients with a nasopharyngeal or midturbinate swab positive for SARS-CoV-2 by real-time reverse transcription polymerase chain reaction (RT-PCR), in need of urgent surgery or obstetric delivery at 1 of 2 large academic Toronto hospitals (Sunnybrook Health Sciences Centre [Sunnybrook] or Sinai Health System), were prospectively identified by the surgical or obstetric clinical teams.
Urgent surgery, as per Sunnybrook’s operating room policies, was defined as 1A, 1B, 1C and 1D: surgery required within 2 hours, 2–8 hours, 8–48 hours and 2–7 days, respectively, to avoid harm to patients.30 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist was used to report this study.31
Setting
Both Sinai Health System and Sunnybrook are level 3 obstetric units, and obstetric patients were recruited from both sites. The nonobstetric urgent surgical patients were recruited from Sunnybrook, a large regional trauma and burn centre.
Standard hospital procedures and personal protective equipment worn by health care workers attending patients with SARS-CoV-2 infection included the following: disposable protective head covering, mask (either N95 mask or American Society for Testing and Materials [ASTM] level 3 surgical mask), face shield or eye protection, impermeable gown, gloves, and shoe or boot covers. When possible, contaminated personal protective equipment was removed in the adjacent anteroom of the operating room. During intubation and extubation, only the anesthesia team (with N95 masks) remained in the room. N95 mask fit testing was a requirement of hospital health care workers in the surgical and obstetric clinical areas. If able, patients wore ASTM level 3 ear loop masks. All the operating rooms (including those in the birthing area) were equipped with 20 air exchanges per hour.
Participants
Patients were included if they were at least 18 years of age; were within 30 days of a positive nasopharyngeal swab for SARS-CoV-2 (either asymptomatic or symptomatic for COVID-197) or were beyond 30 days from an initial positive nasopharyngeal swab for SARS-CoV-2 and still had symptoms of COVID-19; and required obstetric delivery or urgent surgery.
Health care workers included any consenting health care workers present in the operating or delivery room, caring for the patient.
Data sources
Authors P.E.L., D.P., N.A. and G.Y.L reviewed the patients’ electronic health records and used a data extraction sheet (Appendix 1, available at www.cmajopen.ca/content/10/2/E450/suppl/DC1) to record the extracted information. Some patients were interviewed to clarify clinical information. Data were not extracted in duplicate, nor was a formal questionnaire used for in-person interviews.
Study procedures
Study procedures are described in detail in Appendix 2, available at www.cmajopen.ca/content/10/2/E450/suppl/DC1. Patient sampling for laparotomy cases included peritoneal cavity fluid (male or female). Patient samples for obstetric cases included vaginal fluid, swabs of the myometrium (at time of cesarean delivery) and membranous placenta.
Equipment and environmental samples included swabs of the room floor (within 1 m from the surgical site, and 2 m away from the surgical site6), collection of the cautery filter, swab of equipment (e.g., endotracheal tube, saw blade and surgical instruments), and swab of the inside of the surgical mask worn by health care workers.32–34
Bioaerosol sampling was obtained via 2 previously described methods. Active air sampling via the GilAir Plus sampler was used at 2 locations: as close to the surgical site as possible (within 0.5–1.0 m) and 2–3 m away (Sensidyne, https://www.sensidyne.com/air-sampling-equipment/gilian-air-sampling-pumps/gilair-plus/).35 Passive air sampling was performed using an open Petri dish to collect any viral particles settling by gravity in the dish (within 1–2 m of the patient, 1 m off the floor).33,36–39 Passive air sampling was added for the last third of the cases because of newly published information.33,36–39
Laboratory processes
All samples were processed at Sunnybrook. Aside from the cautery and active air sample filters, the laboratory staff were blinded to the source of the sample.
Virus detection was performed by real-time RT-PCR using a multitarget assay currently used in the laboratory.40 The viral RNA loads from samples were extracted using the EasyMag Platform (bioMérieux, France) according to the manufacturer’s instructions. Detection of the SARS-CoV-2 viral RNA was performed using the Luna Universal Probe One-Step RT-qPCR Kit (New England Biolabs, Canada) with the primers and probe for the E-gene, and the thermocycling conditions that have been described by Corman and colleagues41 on the Rotor-Gene Q platform (Qiagen, Germany).
Additionally, the cycle threshold (Ct) value of the assay as an estimate of the viral load was obtained for all samples where possible, including values from the patient’s initial diagnostic swab. Limit of detection was determined to be a Ct value of 40 (as an estimate, this is about 20 viral copies/mL).
Outcomes
The outcome of interest was SARS-CoV-2 RNA PCR-positive samples. Whole genome sequencing was not performed with our surgical or obstetric samples but was performed on diagnostic nasopharyngeal swabs when possible, to identify variants of concern (VOCs). The primary outcome was the proportion of health care workers’ mask samples with positive SARS-CoV-2 RNA PCR results. Other outcomes included the rate of SARS-CoV-2 RNA PCR-positive samples from the surgical site (relevant patient samples), surgical equipment, cautery filter, floor, and ambient air of the operating or birthing room. Additionally, as described in the “Laboratory processes” section, the Ct value was obtained for all positive samples where possible.
Statistical analysis
The expected outcome for the primary outcome (proportion of SARS-CoV-2 RNA PCR-positive samples from the health care workers’ masks) was 0% positivity. We planned to study a total of at least 100 health care workers’ masks, which, with an expected positive rate of 0%, would provide a 95% confidence interval (CI) of 0%–5%. Not all patients had similar data as there were different clinical scenarios. Analysis was performed on all available data.
Descriptive statistics, the Shapiro–Wilk normality test, the Mann–Whitney U test and the 2-sample test for equality of proportions with continuity correction tests were used where appropriate. The Ct values from the RT-PCR on nasopharyngeal swabs in patients with VOCs versus patients without VOCs, and in patients who had at least 1 positive study sample versus patients with no positive study samples were compared using the Mann–Whitney U test. All statistical analyses were conducted with R Statistical Software (R version 3.5.3, 2019).
Ethics approval
The Sunnybrook Research Ethics Board (1676) and the Mount Sinai Hospital Research Ethics Board (20-0224-A) granted ethics approval.
Patient samples (peritoneal fluid, vaginal, myometrial or placental swabs) were collected in patients providing informed consent. Mask sampling of attending health care workers was performed with health care workers’ consent. Patient or health care worker consent was not required for sampling from the air, floor, surgical instrument or cautery filters. Consenting health care workers agreed to follow up with hospital occupational health departments if SARS-CoV-2 RNA was detected on their mask.
Results
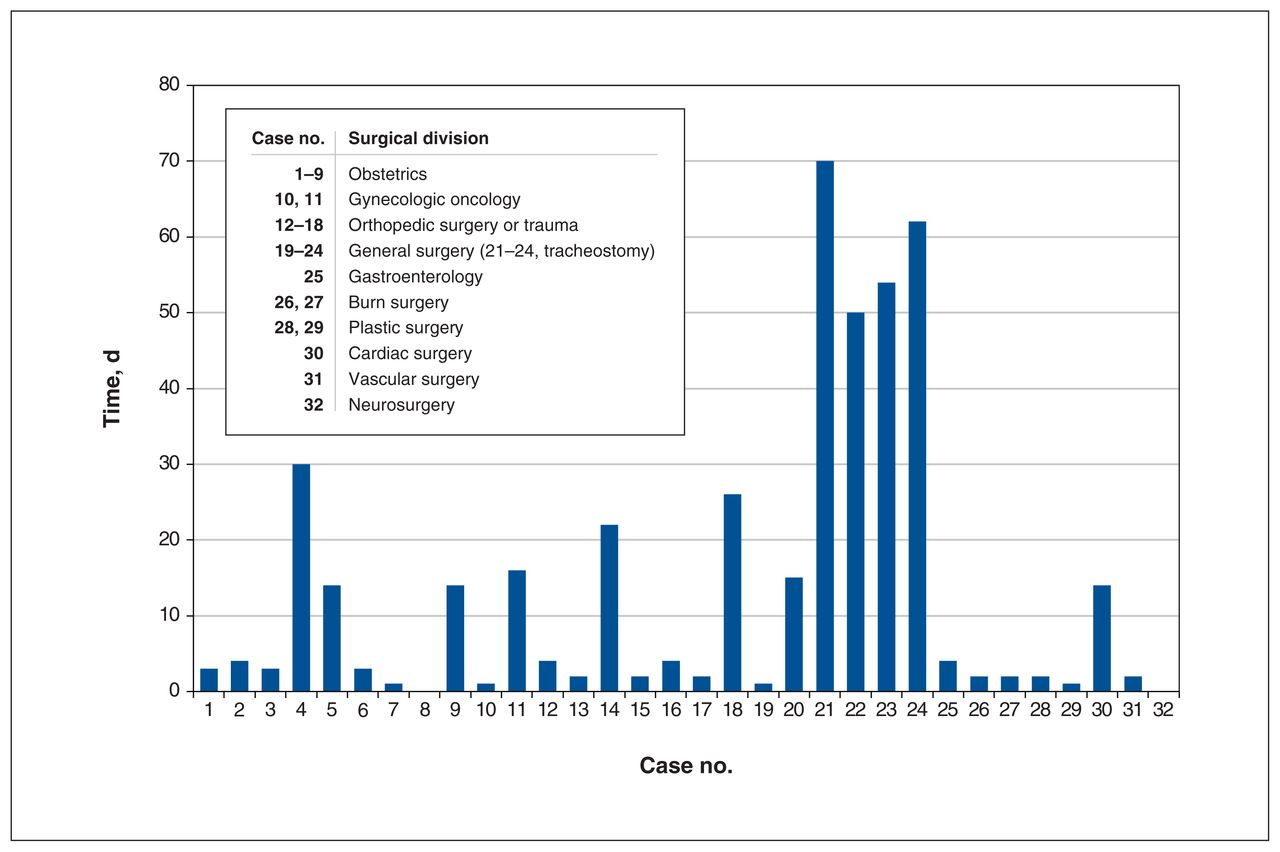
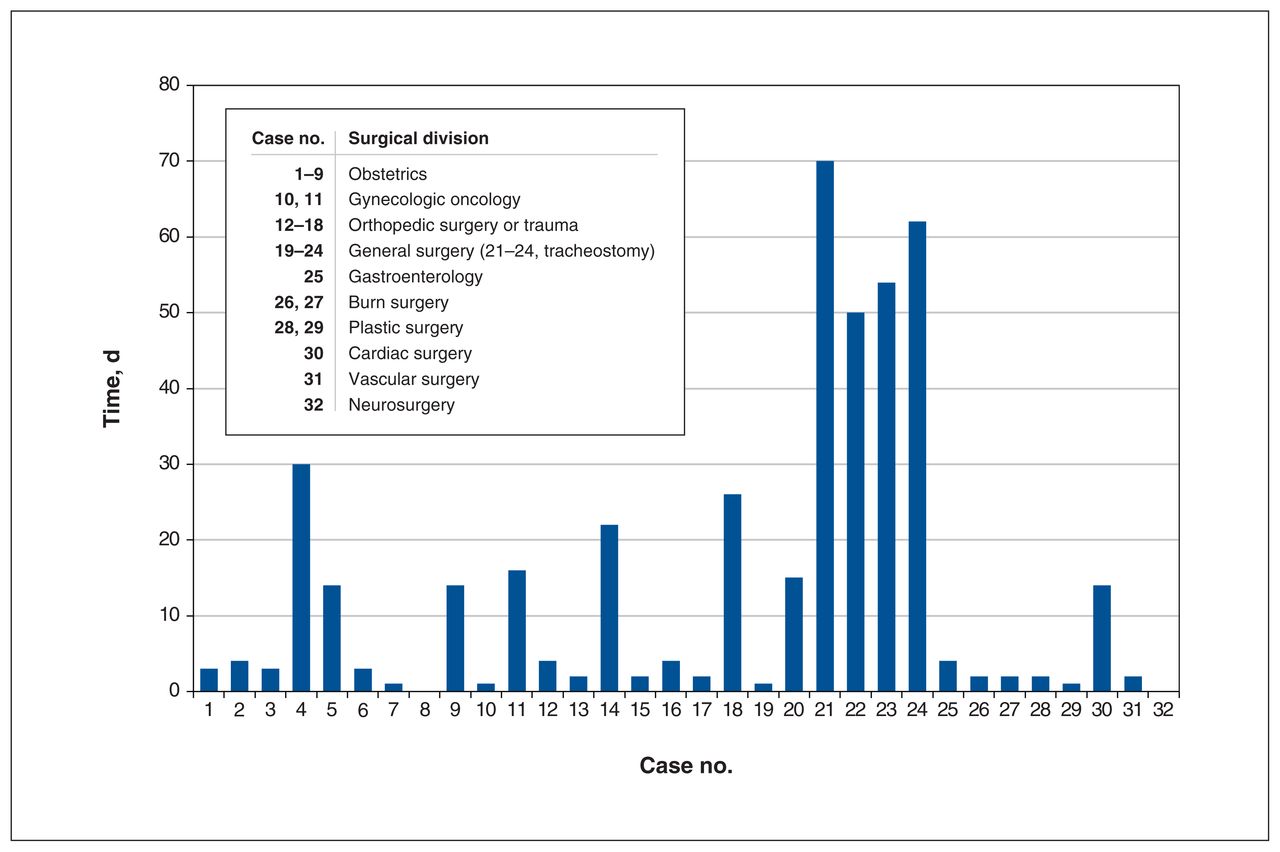
A total of 32 patients with SARS-CoV-2 infection (Table 1 [detailed table provided in Appendix 3, available at www.cmajopen.ca/content/10/2/E450/suppl/DC1], Figure 1), 18 female and 14 male, were enrolled (mean age 53.6, standard deviation 18.1, yr; range 20–88 yr). Nine patients had obstetric deliveries at either Sunnybrook or Sinai Health System, and 23 had urgent surgery at Sunnybrook.
Patient and case characteristics with results of samples taken*
Time from a positive SARS-CoV-2 test to the patient’s surgical or delivery date.
All patients and surgical team leads who were approached to enter this study agreed and provided consent. However, not all patients were able to provide consent (e.g., urgency of the procedure, decreased level of consciousness) for surgical site samples (e.g., peritoneal, vaginal fluid). In one case of laparotomy, the peritoneal fluid sample was not taken. Although all team leads of included patients agreed to participate, several surgical and obstetric team members in the room declined mask sampling for reasons that included concern about quarantine and loss of pay if they tested positive for SARS-CoV-2.
Of the 32 patients enrolled, the patient’s first SARS-CoV-2 positive nasopharyngeal swab occurred a median of 4 days before their procedure (mean 13.8, range 0–70 d). Eleven of 32 patients had a repeat nasopharyngeal swab closer to the date of their procedure (median 3, mean 5.1, range 0–24 d).
SARS-CoV-2 positivity of samples
A total of 343 samples were taken for SARS-CoV-2 RNA detection. Of these, 11 were duplicates (1 person submitted 2 masks; 10/12 endotracheal tubes were sampled twice with a different methodology: flocked swab [4/12 samples positive for viral RNA] and dental pledget [7/10 samples positive]).
Twenty of the 332 (6%) samples tested positive for SARS-CoV-2 RNA (Table 2 [detailed table provided in Appendix 4, available at www.cmajopen.ca/content/10/2/E450/suppl/DC1]): 8 of 12 endotracheal tubes, 1 of 6 peritoneal fluid samples (1/5 cesarean delivery cases, 0/1 trauma laparotomy case), 1 of 7 placentas, 1 of 4 myometrial swabs, 1 of 7 vaginal fluid samples, 2 of 11 samples from surgical equipment of 11 different surgical cases, 1 of 7 passive air samples, and 5 of 60 floor samples. There were no positive samples for SARS-CoV-2 RNA from among cautery filters (0/24 cases), active air sampling (0/47, 25 cases) or the inside of health care workers’ masks (0/143, 95% CI 0–0.026; 32 cases sampled).
Positive tests for SARS-CoV-2 RNA*
In 5 surgical cases, the initial positive diagnostic test had been done 30 days or more before the surgical procedure: 1 cesarean delivery (30 d) and 4 tracheostomies (50, 54, 62 and 70 d). Four of 5 of these cases (30, 54, 62 and 70 d) had positive endotracheal tube samples, and 2 of the 4 cases of positive endotracheal tube samples had positive floor samples (54 and 62 d since diagnosis of SARS-CoV-2 infection).
Variants of concern
Variants of concern were identified in 10 cases. Of the 10 VOC cases, 9 were the Alpha variant (United Kingdom/ B.1.1.7), and 1 was either the Beta or Gamma variant (South African/B.1.351 or Brazilian/P.1). Of the 10 VOC cases, the following sites tested positive for SARS-CoV-2 RNA: 3 of 4 endotracheal tubes, 2 of 18 floor samples (including 1 sample 2 m away), 1 of 5 passive air samples, and 2 of 6 cases in which the surgical instruments were tested. There was no significant difference between the proportion of positive samples when comparing the VOC group (n = 10) and the unknown or not VOC group (n = 22).
Viral load
The Ct value of the initial nasopharyngeal swab positive for SARS-CoV-2 RNA was recorded for 20 of 32 patients (median 30.3, mean 26.65, range 11.86–37.25). For the VOC group, 9 of 10 had Ct values recorded (median 24.41; mean 24.52, 95% CI 18.72–30.99; range 11.86–37.25). For the unknown or not VOC group, 11 of 22 had Ct values recorded (median 31.10; mean 28.41, 95% CI 25.35–30.33; range 13.45–35.29). There was no significant difference in Ct values between these 2 groups (Mann–Whitney U test, p = 0.5). The Ct values of the initial nasopharyngeal swabs were significantly lower in those tested who were subsequently found to have any study sample with SARS-CoV-2 RNA (13/32: Ct recorded in 8/13) versus those without any positive study samples (19/32: Ct recorded in 12/19) with a mean Ct of 21.72 (95% CI 16.90–27.29) versus mean 29.96 (95% CI 27.07–33.43), respectively (Mann–Whitney U test, p = 0.007).
Interpretation
From November 2020 to May 2021, we found evidence of SARS-CoV-2 RNA in samples taken in the surgical and obstetric operative environment. We found no detectable virus on the inner surface of masks worn by our health care teams.
Several studies have documented potential risks of SARS-CoV-2 infection to health care workers in clinic and hospital ward settings and in caring for patients with tracheostomies (an aerosol-generating procedure).1,6,29,42 We evaluated potential exposure risks to health care workers in the operating room with a variety of surgical procedures not known to be aerosol generating. Health care workers are in prolonged and very close contact with patients in the operating room. In our study, we detected SARS-CoV-2 RNA in nonrespiratory patient samples (peritoneal fluid, vaginal fluid, myometrium, placenta), surgical equipment and instruments, and the surgical room environment; however, no contamination of the surgical masks worn by health care workers was detected.
Our study corroborates earlier studies that have shown evidence of virus in the respiratory tract and in surgical or obstetric fields.12,13,15–18,43–45 We have documented evidence of SARS-CoV-2 RNA in the gastrointestinal tract, peritoneal cavity and female genital tract, all of which could potentially be sources of aerosolized virus or viral particles. We did not find evidence of viral RNA in the orthopedic, cardiac and burn surgical equipment sampled. This may indicate that SARS-CoV-2 does not reside in this type of tissue or at least was not present with a viral load high enough for detection.
With our study and others reporting the finding of virus in the peritoneal cavity, use of laparoscopy (which theoretically may be considered an aerosol-generating procedure), could result in aerosolization of SARS-CoV-2.11,13,14,46–50
We used standard techniques for air and floor sampling and found evidence of aerosolization of SARS-CoV-2.6,33,36,38,51 Although the frequency of positive tests was low, this does indicate that aerosolization of the virus does occur in the surgical or obstetric environments; however, the source of the virus (respiratory, or surgical or obstetric fields) is unknown. It is possible that the true positive rates were higher since some contamination was likely below the detection limits of the tests.6,33,36,38,51
We looked for characteristics of patients’ infections that would increase the risks of detection of viral RNA in the surgical or obstetric fields, or local environment. Higher viral load detected on the initial nasopharyngeal swab (as indicated by lower Ct value) was associated with higher risk of detectable virus in our samples, whereas the subtype of SARS-CoV-2 was not.
We were unable to determine whether the surgical smoke was the origin of aerosolized or droplet virus. Others have not detected SARS-CoV-2 in electrocautery smoke, despite using high viral loads in an in vitro setting.28 Although the lack of any positive viral RNA found on the smoke evacuator filters tested would indicate that the viral contamination from the surgical field is absent or below detection limits, these results cannot be used to definitely conclude that surgical smoke does not harbour SARS-CoV-2.
Since infection with SARS-CoV-2 is primarily via the respiratory tract, we chose to sample the inside of health care workers’ masks to identify viral contamination in close proximity to their respiratory tract. Face mask sampling has been shown to be effective in detecting contamination with Mycobacterium tuberculosis and viruses52–54 and has been used to detect SARS-CoV-2 contamination of masks worn by health care workers exposed to infected patients (0/25 positive, inside surface) and directly from patient masks (6/10 positive).32 Others have studied SARS-CoV-2 viral contamination on the outer surface of face shields worn by health care workers attending patients with COVID-19 in labour (1 vaginal delivery with all face shields tested being positive).36 We sampled the inside of masks and found 0 of 143 health care workers’ masks and 0 of 4 health care workers’ face shields to be positive for SARS-CoV-2 RNA.
In the future, there are 3 important studies to complete: to determine whether the detected environmental viral RNA is infectious, to determine the risk of clinical and subclinical infections of health care workers when exposed to patients with COVID-19 undergoing surgery or labour and delivery, and to validate our findings externally.
Limitations
The study has some limitations. We do not have information on postexposure SARS-CoV-2 infections among health care workers, and we did not obtain information on health care workers’ vaccination status or previous infections. In each of the 32 cases, the patient’s positive SARS-CoV-2 status was known, and hence it is possible that extra care was taken by the surgical and obstetric teams, although the intubation and extubation protocol was universal.
We recognize that, because of detection limits of the test and sampling issues, it is possible that not all viral contamination was detected in this study. Detection of SARS-CoV-2 RNA in bioaerosols is recognized to be challenging, being highly dependent on air flow, exchange rates and source of emissions (reviewed by Borges and colleagues55), and it is suggested that parallel sampling with more than 1 technique may increase sensitivity.55 We did take measures such as using 2 different air sampling techniques, increasing the size of floor samples taken for the testing and using multiple testing to mitigate these issues. Finally, even though viral RNA was detected, this study did not determine whether infectious virus was present.
Conclusion
During our study period of November 2020 to May 2021, we found evidence of SARS-CoV-2 RNA in the operative environment (surgical surfaces and aerosolized) for surgical and obstetric patients, and this reinforces the need for appropriate cleaning of the environment (floors and hand hygiene, as examples) after these procedures. However, the finding of no detectable virus on the inner surface of masks worn by the health care teams in our study reassuringly suggests a low risk of infection when appropriate personal protective equipment is worn.
Acknowledgements
The authors are grateful to the operating room nurses and obstetric nurses who participated in this study, as well as the patients, their anesthetists and their surgeons.
Footnotes
Competing interests: Robert Kozak reports a grant from the Ontario Together Fund. Grace Liu reports a speaker payment from Hologic and reports an unpaid position as a board member for the American Association of Gynecologic Laparoscopists, 2019–2021. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Patricia Lee, Grace Liu, Robert Kozak, Nasrin Alavi, Hamza Mbareche, Noor Ladhani and Albert Yee contributed to the concept and design. All authors contributed to the acquisition, analysis or interpretation of data. Patricia Lee, Grace Liu, Robert Kozak and Noor Ladhani drafted the manuscript. Stephanie Jarvi and Rose Kung performed the statistical analysis. Patricia Lee obtained funding. Nasrin Alavi, Hamza Mbareche, Rose Kung, Darian Perruzza, Stephanie Jarvi, Elsa Salvant, Robert Kozak, Louise-Helene Gagnon, Richard Jenkinson, Patricia Lee and Grace Liu contributed administrative, technical or material support. Patricia Lee, Grace Liu, Robert Kozak, Rose Kung and Kellie Murphy supervised the study. All authors critically revised the manuscript for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported by the Sunnybrook AFP Association through the Innovation Fund of the Alternative Funding Plan for the Academic Health Sciences Centres of Ontario (Patricia Lee) and a Chair’s Summer Research Student Award from the Department of Obstetrics and Gynaecology, University of Toronto (Darian Perruzza). The funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Data sharing: Primary deidentified data are available on reasonable request to the corresponding author.
Editor’s note: This article appears as a preprint (medRxiv): https://doi.org/10.1101/2021.09.03.21262874.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/2/E450/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools





