
COVID-19 Vaccine Hesitancy and Emerging Variants: Evidence from Six Countries

 , , ,
, , ,  ,
,  , and
, and
Abstract
:1. Background
2. Methodology
2.1. Questionnaire
2.2. Statistical Analysis
3. Results
3.1. Respondent Characteristics
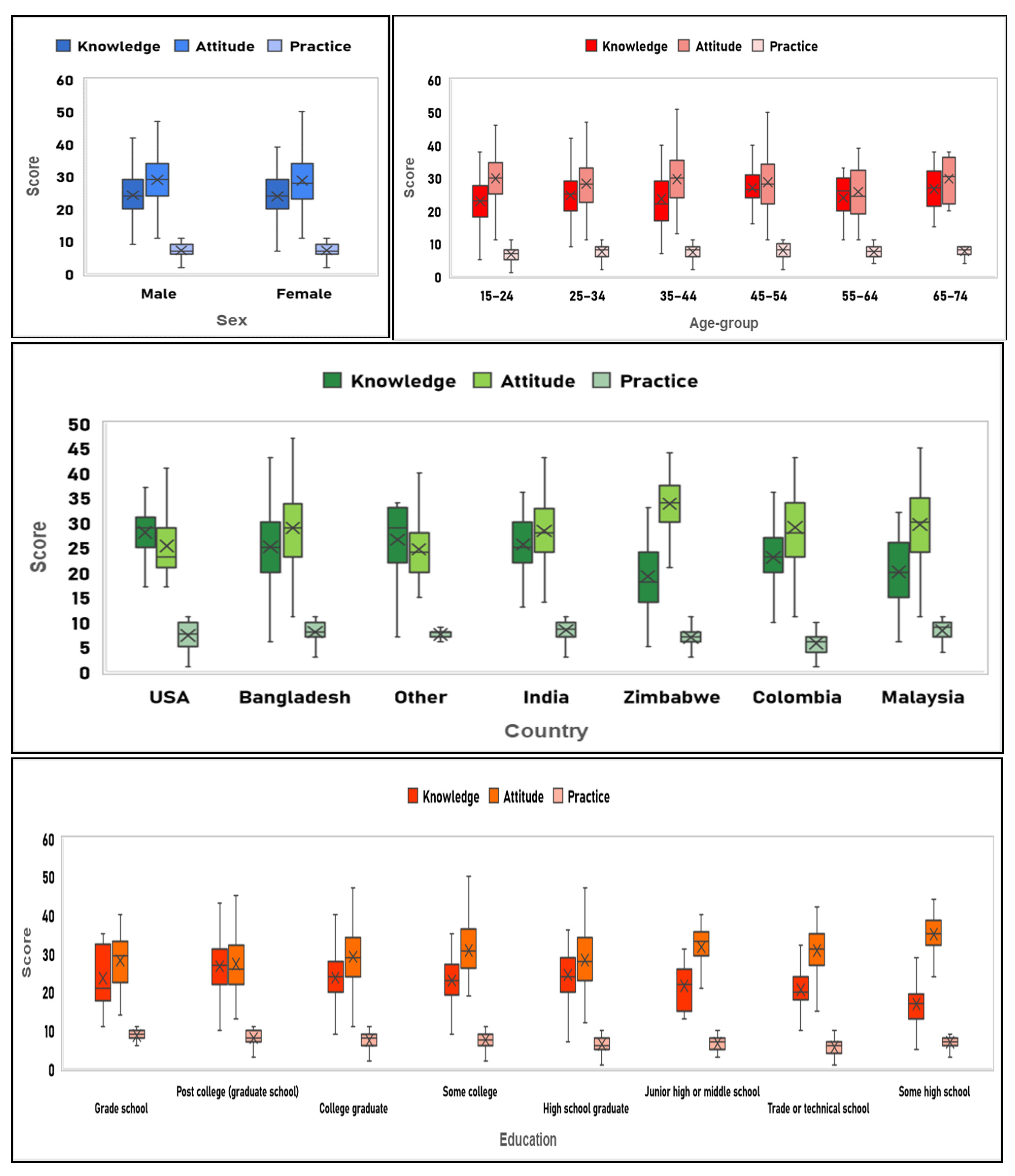
3.2. Scores
3.3. Relationship between Knowledge, Attitude, and Practice
3.4. Knowledge
3.5. Attitude
3.6. Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- WHO. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 1 September 2021).
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics against Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Freitas, L.D.; Basdeo, D.; Wang, H.I. Public Trust, Information Sources and Vaccine Willingness Related to the COVID-19 Pandemic in Trinidad and Tobago: An Online Cross-Sectional Survey. Lancet Reg. Health 2021. [Google Scholar] [CrossRef]
- Pennington, M. Vaccine Hesitancy: A Story as Old as Vaccines Themselves. 2021. Available online: https://www.criver.com/eureka/vaccine-hesitancy-story-old-vaccines-themselves (accessed on 14 October 2021).
- MacDonald, N.E.; Hesitancy, S.W.G.O.V. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Seale, H.; Heywood, A.E.; McLaws, M.L.; Ward, K.F.; Lowbridge, C.P.; Van, D.; MacIntyre, C.R. Why do I need it? I am not at risk! Public perceptions towards the pandemic (H1N1) 2009 vaccine. BMC Infect. Dis. 2010, 10, 99. [Google Scholar] [CrossRef] [Green Version]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Mesch, G.S.; Schwirian, K.P. Social and political determinants of vaccine hesitancy: Lessons learned from the H1N1 pandemic of 2009–2010. Am. J. Infect. Control. 2015, 43, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Fraser, N.; Brierley, L.; Dey, G.; Polka, J.K.; Palfy, M.; Nanni, F.; Coates, J.A. The evolving role of preprints in the dissemination of COVID-19 research and their impact on the science communication landscape. PLoS Biol. 2021, 19, e3000959. [Google Scholar] [CrossRef]
- Bricout, H.; Torcel-Pagnon, L.; Lecomte, C.; Almas, M.F.; Matthews, I.; Lu, X.; Wheelock, A.; Sevdalis, N. Determinants of shingles vaccine acceptance in the United Kingdom. PLoS ONE 2019, 14, e0220230. [Google Scholar] [CrossRef] [Green Version]
- Daniels, N.A.; Gouveia, S.; Null, D.; Gildengorin, G.L.; Winston, C.A. Acceptance of pneumococcal vaccine under standing orders by race and ethnicity. J. Natl. Med. Assoc. 2006, 98, 1089–1094. [Google Scholar]
- Fiebach, N.H.; Viscoli, C.M. Patient acceptance of influenza vaccination. Am. J. Med. 1991, 91, 393–400. [Google Scholar] [CrossRef]
- Reese, T.; Segall, N.; Nesbitt, P.; Del Fiol, G.; Waller, R.; Macpherson, B.C.; Tonna, J.E.; Wright, M.C. Patient information organization in the intensive care setting: Expert knowledge elicitation with card sorting methods. J. Am. Med. Inform. Assoc. 2018, 25, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Kok, G. The theory of planned behavior: A review of its applications to health-related behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Vaccination Coverage Worldwide by Vaccine|Statista. Available online: [https://www.statista.com/statistics/785838/worldwide-vaccine-coverage-by-vaccine-type/ (accessed on 6 August 2021).
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Burgos, R.M.; Badowski, M.E.; Drwiega, E.; Ghassemi, S.; Griffith, N.; Herald, F.; Johnson, M.; Smith, R.O.; Michienzi, S.M. The race to a COVID-19 vaccine: Opportunities and challenges in development and distribution. Drugs Context 2021, 10. [Google Scholar] [CrossRef]
- Deb, B.; Shah, H.; Goel, S. Current global vaccine and drug efforts against COVID-19: Pros and cons of bypassing animal trials. J. Biosci. 2020, 45, 82. [Google Scholar] [CrossRef]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gomez Roman, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef]
- Baumgaertner, B.; Carlisle, J.E.; Justwan, F. The influence of political ideology and trust on willingness to vaccinate. PLoS ONE 2018, 13, e0191728. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Ellyatt, H. After Being Ravaged by the Delta Covid Variant, How Is India Doing Now? 2021. Available online: https://www.cnbc.com/2021/07/23/coronavirus-how-india-is-doing-now-after-delta-variant-spread.html (accessed on 1 September 2021).
- Mendez, R. Delta Variant Now Accounts for 83% of All Sequenced Covid Cases in the U.S., CDC Director Walensky Says. 2021. Available online: https://www.cnbc.com/2021/07/20/delta-variant-now-accounts-for-83percent-of-all-sequenced-covid-cases-in-the-us-cdc-director-walensky-says.html (accessed on 2 September 2021).
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Kestenbaum, L.A.; Feemster, K.A. Identifying and addressing vaccine hesitancy. Pediatr. Ann. 2015, 44, e71–e75. [Google Scholar] [CrossRef] [Green Version]
- Jony, S.S.R.; Haque, U.; Webb, N.J.; Spence, E.; Rahman, M.S.; Aghamohammadi, N.; Lie, Y.; Angulo-Molina, A.; Ananth, S.; Ren, X.; et al. Analyzing Predictors of Control Measures and Psychosocial Problems Associated with COVID-19 Pandemic: Evidence from Eight Countries. Behav. Sci. 2021, 11, 106. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N.; Cornaglia, G.; Group, E.V.S. Barriers to the vaccination of children and adolescents and possible solutions. Clin. Microbiol. Infect. 2014, 20 (Suppl. S5), 25–31. [Google Scholar] [CrossRef] [Green Version]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and Vaccine Hesitancy: A Challenge the United States Must Overcome. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef]
- Preskorn, S.H. The 5% of the Population at High Risk for Severe COVID-19 Infection Is Identifiable and Needs to Be Taken into Account When Reopening the Economy. J. Psychiatr. Pract. 2020, 26, 219–227. [Google Scholar] [CrossRef]
- d’Onofrio, A.; Manfredi, P. Vaccine demand driven by vaccine side effects: Dynamic implications for SIR diseases. J. Theor. Biol. 2010, 264, 237–252. [Google Scholar] [CrossRef] [Green Version]
- Khan, Y.H.; Mallhi, T.H.; Alotaibi, N.H.; Alzarea, A.I.; Alanazi, A.S.; Tanveer, N.; Hashmi, F.K. Threat of COVID-19 Vaccine Hesitancy in Pakistan: The Need for Measures to Neutralize Misleading Narratives. Am. J. Trop. Med. Hyg. 2020, 103, 603–604. [Google Scholar] [CrossRef]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Anazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Franco, O.H. Public trust, misinformation and COVID-19 vaccination willingness in Latin America and the Caribbean: Today’s key challenges. Lancet Reg. Health Am. 2021, 3, 100073. [Google Scholar] [CrossRef]
- Shrestha, N.; Shad, M.Y.; Ulvi, O.; Khan, M.H.; Karamehic-Muratovic, A.; Nguyen, U.D.T.; Baghbanzadeh, M.; Wardrup, R.; Aghamohammadi, N.; Cervantes, D.; et al. The impact of COVID-19 on globalization. One Health 2020, 11, 100180. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, M.T.H.; Khan, I.M.; Jony, S.S.R.; Robinson, R.; Keellings, D.; Rahman, M.S.; Haque, U. The Disproportionate Impact of COVID-19 among Undocumented Immigrants and Ethnic Minorities in the US. Available online: https://ssrn.com/abstract=3909781 (accessed on 20 October 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Independent Variable | Respondents with Score > 23.5 | Univariate Logistic Regression | Multiple Logistic Regression | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | OR | p-Value | 95% CI | AOR | p-Value | 95% CI | ||||
| Sex | |||||||||||
| Male ® | 206 | 51.76 | |||||||||
| Female | 208 | 54.31 | 1.11 | 0.48 | 0.84 | 1.47 | 1.28 | 0.14 | 0.92 | 1.77 | |
| Age groups | |||||||||||
| 15–24 ® | 104 | 44.07 | |||||||||
| 25–34 | 177 | 56.55 | 1.65 * | 0.00 | 1.18 | 2.32 | 1.10 | 0.72 | 0.66 | 1.84 | |
| 35–44 | 64 | 46.38 | 1.10 | 0.67 | 0.72 | 1.67 | 0.92 | 0.80 | 0.49 | 1.75 | |
| 45–54 | 45 | 83.33 | 6.35 * | 0.00 | 2.97 | 13.58 | 5.81 * | 0.00 | 2.30 | 14.69 | |
| 55–64 | 17 | 56.67 | 1.66 | 0.20 | 0.77 | 3.57 | 2.43 | 0.12 | 0.80 | 7.38 | |
| 65–74 | 7 | 70.00 | 2.96 | 0.12 | 0.75 | 11.73 | 7.47 | 0.07 | 0.86 | 64.82 | |
| Nationality | |||||||||||
| Bangladeshi ® | 173 | 62.45 | |||||||||
| American | 25 | 75.76 | 1.88 | 0.14 | 0.82 | 4.32 | |||||
| Colombian | 101 | 42.62 | 0.45 * | 0.00 | 0.31 | 0.64 | |||||
| Indian | 66 | 65.35 | 1.13 | 0.61 | 0.70 | 1.83 | |||||
| Malaysian | 18 | 30.51 | 0.26 * | 0.00 | 0.14 | 0.48 | |||||
| Zimbabwean | 13 | 26.00 | 0.21 * | 0.00 | 0.11 | 0.42 | |||||
| Other | 18 | 75.00 | 1.80 | 0.23 | 0.69 | 4.69 | |||||
| Country | |||||||||||
| Bangladesh ® | 164 | 61.19 | |||||||||
| Colombia | 102 | 43.40 | 0.49 * | 0.00 | 0.34 | 0.69 | 0.56 * | 0.02 | 0.34 | 0.92 | |
| India | 61 | 63.54 | 1.11 | 0.69 | 0.68 | 1.79 | 1.37 | 0.29 | 0.77 | 2.44 | |
| Malaysia | 18 | 31.03 | 0.29 * | 0.00 | 0.16 | 0.52 | 0.23 * | 0.00 | 0.12 | 0.47 | |
| USA | 42 | 84.00 | 3.33 * | 0.00 | 1.50 | 7.37 | 3.16 * | 0.01 | 1.35 | 7.38 | |
| Zimbabwe | 14 | 26.42 | 0.23 * | 0.00 | 0.12 | 0.44 | 0.60 | 0.27 | 0.25 | 1.47 | |
| Other | 13 | 61.90 | 1.03 | 0.95 | 0.41 | 2.57 | 1.33 | 0.59 | 0.48 | 3.71 | |
| Education | |||||||||||
| College graduate ® | 141 | 52.03 | |||||||||
| Grade school | 6 | 37.50 | 0.55 | 0.26 | 0.20 | 1.56 | 0.39 | 0.12 | 0.12 | 1.29 | |
| Junior high or middle school | 7 | 41.18 | 0.65 | 0.39 | 0.24 | 1.75 | 0.77 | 0.66 | 0.25 | 2.38 | |
| Some high school | 3 | 10.34 | 0.11 * | 0.00 | 0.03 | 0.36 | 0.13* | 0.01 | 0.03 | 0.59 | |
| High school graduate | 52 | 52.00 | 1.00 | 1.00 | 0.63 | 1.58 | 1.25 | 0.47 | 0.68 | 2.28 | |
| Trade or technical school | 19 | 25.33 | 0.31 * | 0.00 | 0.18 | 0.55 | 0.41 * | 0.01 | 0.21 | 0.80 | |
| Some college | 12 | 46.15 | 0.79 | 0.57 | 0.35 | 1.77 | 0.46 | 0.10 | 0.18 | 1.16 | |
| Post college (graduate school) | 174 | 70.45 | 2.20 * | 0.00 | 1.53 | 3.16 | 1.83 * | 0.00 | 1.23 | 2.74 | |
| Employment | |||||||||||
| Employed full time ® | 221 | 60.22 | |||||||||
| Employed part time | 19 | 55.88 | 0.84 | 0.62 | 0.41 | 1.70 | 0.91 | 0.81 | 0.41 | 2.01 | |
| Retired | 7 | 43.75 | 0.47 * | 0.03 | 0.24 | 0.95 | 0.45 * | 0.04 | 0.21 | 0.96 | |
| Self-employed | 22 | 44.90 | 0.58 * | 0.00 | 0.42 | 0.79 | 1.11 | 0.71 | 0.65 | 1.89 | |
| Student | 126 | 46.67 | 0.51 | 0.20 | 0.19 | 1.41 | 0.30 | 0.17 | 0.05 | 1.64 | |
| Unemployed | 15 | 41.67 | 0.54 * | 0.04 | 0.30 | 0.98 | 0.53 | 0.07 | 0.26 | 1.05 | |
| Other | 4 | 44.44 | 0.53 | 0.35 | 0.14 | 2.00 | 0.22 * | 0.04 | 0.05 | 0.96 | |
| Independent Variable | Respondents with a Score >27.5 | Univariate Logistic Regression | Multiple Logistic Regression | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | OR | p-Value | 95% CI | AOR | p-Value | 95% CI | ||||
| Sex | |||||||||||
| Male ® | 229 | 57.54 | |||||||||
| Female | 203 | 53.00 | 0.83 | 0.20 | 0.63 | 1.10 | 0.81 | 0.20 | 0.60 | 1.11 | |
| Age groups | |||||||||||
| 15–24 ® | 147 | 62.29 | |||||||||
| 25–34 | 159 | 50.80 | 0.63 * | 0.01 | 0.44 | 0.88 | 0.78 | 0.32 | 0.47 | 1.28 | |
| 35–44 | 79 | 57.25 | 0.81 | 0.34 | 0.53 | 1.24 | 0.98 | 0.94 | 0.53 | 1.81 | |
| 45–54 | 28 | 51.85 | 0.65 | 0.16 | 0.36 | 1.18 | 0.90 | 0.78 | 0.42 | 1.92 | |
| 55–64 | 12 | 40.00 | 0.40 * | 0.02 | 0.19 | 0.88 | 0.47 | 0.15 | 0.16 | 1.33 | |
| 65–74 | 7 | 70.00 | 1.41 | 0.62 | 0.36 | 5.60 | 1.89 | 0.49 | 0.31 | 11.40 | |
| Nationality | |||||||||||
| Bangladeshi ® | 154 | 55.60 | |||||||||
| American | 9 | 27.27 | 0.30 * | 0.00 | 0.13 | 0.67 | |||||
| Colombian | 129 | 54.43 | 0.95 | 0.79 | 0.67 | 1.35 | |||||
| Indian | 53 | 52.48 | 0.88 | 0.59 | 0.56 | 1.39 | |||||
| Malaysian | 35 | 59.32 | 1.16 | 0.60 | 0.66 | 2.06 | |||||
| Zimbabwean | 43 | 86.00 | 4.91 * | 0.00 | 2.13 | 11.29 | |||||
| Other | 9 | 37.50 | 0.48 | 0.09 | 0.20 | 1.13 | |||||
| Country | |||||||||||
| Bangladesh ® | 149 | 55.60 | |||||||||
| Colombia | 129 | 54.89 | 0.97 | 0.87 | 0.68 | 1.38 | 0.72 | 0.18 | 0.44 | 1.17 | |
| India | 52 | 54.17 | 0.94 | 0.81 | 0.59 | 1.51 | 0.81 | 0.46 | 0.47 | 1.41 | |
| Malaysia | 34 | 58.62 | 1.13 | 0.67 | 0.64 | 2.01 | 0.98 | 0.95 | 0.52 | 1.84 | |
| USA | 16 | 32.00 | 0.38 * | 0.00 | 0.20 | 0.71 | 0.36* | 0.00 | 0.18 | 0.72 | |
| Zimbabwe | 45 | 84.91 | 4.49 * | 0.00 | 2.04 | 9.90 | 1.80 | 0.25 | 0.67 | 4.88 | |
| Other | 7 | 33.33 | 0.40 | 0.06 | 0.16 | 1.02 | 0.37 | 0.06 | 0.14 | 1.02 | |
| Education | |||||||||||
| College graduate ® | 155 | 57.20 | |||||||||
| Grade school | 9 | 56.25 | 0.96 | 0.94 | 0.35 | 2.66 | 0.85 | 0.77 | 0.29 | 2.49 | |
| Junior high or middle school | 14 | 82.35 | 3.49 * | 0.05 | 0.98 | 12.44 | 3.52 | 0.07 | 0.91 | 13.56 | |
| Some high school | 27 | 93.10 | 10.10 * | 0.00 | 2.35 | 43.34 | 5.37 | 0.06 | 0.93 | 31.15 | |
| High school graduate | 51 | 51.00 | 0.78 | 0.29 | 0.49 | 1.23 | 0.84 | 0.56 | 0.47 | 1.51 | |
| Trade or technical school | 50 | 66.67 | 1.50 | 0.14 | 0.87 | 2.56 | 1.85 | 0.06 | 0.99 | 3.46 | |
| Some college | 18 | 69.23 | 1.68 | 0.24 | 0.71 | 4.01 | 1.89 | 0.18 | 0.75 | 4.75 | |
| Post college (graduate school) | 108 | 43.72 | 0.58 * | 0.00 | 0.41 | 0.82 | 0.56 * | 0.00 | 0.39 | 0.82 | |
| Employment | |||||||||||
| Employed full time ® | 192 | 52.32 | |||||||||
| Employed part time | 20 | 58.82 | 1.30 | 0.47 | 0.64 | 2.66 | 1.24 | 0.58 | 0.58 | 2.66 | |
| Retired | 10 | 62.50 | 1.14 | 0.71 | 0.57 | 2.27 | 1.05 | 0.90 | 0.50 | 2.20 | |
| Self-employed | 31 | 63.27 | 1.23 | 0.20 | 0.90 | 1.69 | 0.78 | 0.34 | 0.47 | 1.30 | |
| Student | 155 | 57.41 | 1.52 | 0.43 | 0.54 | 4.27 | 1.39 | 0.65 | 0.33 | 5.92 | |
| Unemployed | 20 | 55.56 | 1.57 | 0.15 | 0.85 | 2.91 | 1.62 | 0.15 | 0.84 | 3.15 | |
| Other | 4 | 44.44 | 0.73 | 0.64 | 0.19 | 2.76 | 0.79 | 0.75 | 0.18 | 3.39 | |
| Independent Variable | Respondents with a Score > 5.5 | Univariate Logistic Regression | Multiple Logistic Regression | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | OR | p-Value | 95% CI | AOR | p-Value | 95% CI | ||||
| Sex | |||||||||||
| Male ® | 320 | 80.40 | |||||||||
| Female | 300 | 78.33 | 0.88 | 0.47 | 0.62 | 1.25 | 1.24 | 0.29 | 0.83 | 1.85 | |
| Age groups | |||||||||||
| 15–24 ® | 171 | 72.46 | |||||||||
| 25–34 | 256 | 81.79 | 1.71 * | 0.01 | 1.14 | 2.56 | 1.23 | 0.50 | 0.67 | 2.25 | |
| 35–44 | 114 | 82.61 | 1.81 * | 0.03 | 1.07 | 3.05 | 1.86 | 0.11 | 0.87 | 3.97 | |
| 45–54 | 45 | 83.33 | 1.90 | 0.10 | 0.88 | 4.11 | 1.84 | 0.22 | 0.70 | 4.89 | |
| 55–64 | 25 | 83.33 | 1.90 | 0.21 | 0.70 | 5.18 | 3.79 | 0.07 | 0.90 | 15.92 | |
| 65–74 | 9 | 90.00 | 3.42 | 0.25 | 0.42 | 27.54 | 34.12 * | 0.02 | 1.80 | 647.89 | |
| Nationality | |||||||||||
| Bangladeshi ® | 250 | 90.25 | |||||||||
| American | 18 | 54.55 | 0.13 * | 0.00 | 0.06 | 0.29 | |||||
| Colombian | 139 | 58.65 | 0.15 * | 0.00 | 0.10 | 0.25 | |||||
| Indian | 97 | 96.04 | 2.62 | 0.08 | 0.89 | 7.68 | |||||
| Malaysian | 53 | 89.83 | 0.95 | 0.92 | 0.38 | 2.43 | |||||
| Zimbabwean | 42 | 84.00 | 0.57 | 0.19 | 0.24 | 1.33 | |||||
| Other | 21 | 87.50 | 0.76 | 0.67 | 0.21 | 2.70 | |||||
| Country | |||||||||||
| Bangladesh ® | 242 | 90.30 | |||||||||
| Colombia | 137 | 58.30 | 0.15 * | 0.00 | 0.09 | 0.24 | 0.15 * | 0.00 | 0.08 | 0.28 | |
| India | 92 | 95.83 | 2.47 | 0.10 | 0.84 | 7.27 | 3.68 * | 0.03 | 1.15 | 11.74 | |
| Malaysia | 52 | 89.66 | 0.93 | 0.88 | 0.36 | 2.38 | 0.92 | 0.87 | 0.33 | 2.52 | |
| USA | 34 | 68.00 | 0.23 * | 0.00 | 0.11 | 0.47 | 0.19 * | 0.00 | 0.09 | 0.40 | |
| Zimbabwe | 44 | 83.02 | 0.53 | 0.13 | 0.23 | 1.20 | 0.55 | 0.32 | 0.17 | 1.80 | |
| Other | 19 | 90.48 | 1.02 | 0.98 | 0.22 | 4.63 | 1.01 | 0.99 | 0.21 | 4.84 | |
| Education | |||||||||||
| College graduate ® | 214 | 78.97 | |||||||||
| Grade school | 15 | 93.75 | 4.00 | 0.18 | 0.52 | 30.89 | 3.39 | 0.26 | 0.40 | 28.39 | |
| Junior high or middle school | 12 | 70.59 | 0.64 | 0.42 | 0.22 | 1.89 | 1.48 | 0.54 | 0.42 | 5.27 | |
| Some high school | 24 | 82.76 | 1.28 | 0.63 | 0.47 | 3.50 | 1.78 | 0.47 | 0.38 | 8.38 | |
| High school graduate | 70 | 70.00 | 0.62 | 0.07 | 0.37 | 1.04 | 2.16 * | 0.03 | 1.07 | 4.38 | |
| Trade or technical school | 42 | 56.00 | 0.34 * | 0.00 | 0.20 | 0.58 | 1.15 | 0.68 | 0.59 | 2.25 | |
| Some college | 22 | 84.62 | 1.46 | 0.50 | 0.49 | 4.42 | 0.91 | 0.89 | 0.26 | 3.24 | |
| Post college (graduate school) | 221 | 89.47 | 2.26 * | 0.00 | 1.37 | 3.73 | 1.97 * | 0.02 | 1.11 | 3.47 | |
| Employment | |||||||||||
| Employed full time ® | 313 | 85.29 | |||||||||
| Employed part time | 26 | 76.47 | 0.56 | 0.18 | 0.24 | 1.30 | 0.89 | 0.81 | 0.34 | 2.31 | |
| Retired | 12 | 75.00 | 0.71 | 0.45 | 0.30 | 1.71 | 0.79 | 0.65 | 0.29 | 2.16 | |
| Self-employed | 40 | 81.63 | 0.43 * | 0.00 | 0.29 | 0.64 | 0.88 | 0.69 | 0.47 | 1.63 | |
| Student | 193 | 71.48 | 0.52 | 0.27 | 0.16 | 1.66 | 0.13 * | 0.04 | 0.02 | 0.94 | |
| Unemployed | 29 | 80.56 | 0.77 | 0.50 | 0.35 | 1.67 | 1.13 | 0.78 | 0.48 | 2.68 | |
| Other | 7 | 77.78 | 0.60 | 0.54 | 0.12 | 2.98 | 0.32 | 0.20 | 0.06 | 1.82 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangla, S.; Zohra Makkia, F.T.; Pathak, A.K.; Robinson, R.; Sultana, N.; Koonisetty, K.S.; Karamehic-Muratovic, A.; Nguyen, U.-S.D.T.; Rodriguez-Morales, A.J.; Sanchez-Duque, J.A.; et al. COVID-19 Vaccine Hesitancy and Emerging Variants: Evidence from Six Countries. Behav. Sci. 2021, 11, 148. https://doi.org/10.3390/bs11110148
Mangla S, Zohra Makkia FT, Pathak AK, Robinson R, Sultana N, Koonisetty KS, Karamehic-Muratovic A, Nguyen U-SDT, Rodriguez-Morales AJ, Sanchez-Duque JA, et al. COVID-19 Vaccine Hesitancy and Emerging Variants: Evidence from Six Countries. Behavioral Sciences. 2021; 11(11):148. https://doi.org/10.3390/bs11110148
Chicago/Turabian StyleMangla, Sherry, Fatima Tuz Zohra Makkia, Ashok Kumar Pathak, Renee Robinson, Nargis Sultana, Kranthi Swaroop Koonisetty, Ajlina Karamehic-Muratovic, Uyen-Sa D.T. Nguyen, Alfonso J. Rodriguez-Morales, Jorge A. Sanchez-Duque, and et al. 2021. "COVID-19 Vaccine Hesitancy and Emerging Variants: Evidence from Six Countries" Behavioral Sciences 11, no. 11: 148. https://doi.org/10.3390/bs11110148