
Follow-Up of Side Effects throughout the Entire Course of Coronavirus Vaccination
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Results
3.1.1. Descriptive Results for Individuals
3.1.2. Description of Comorbidities and Other Variables (Allergies and Medications)
3.2. Descriptive for Side Effects Types, Onset, Duration, and Impact
3.2.1. Type of Side Effects and Number of Doses
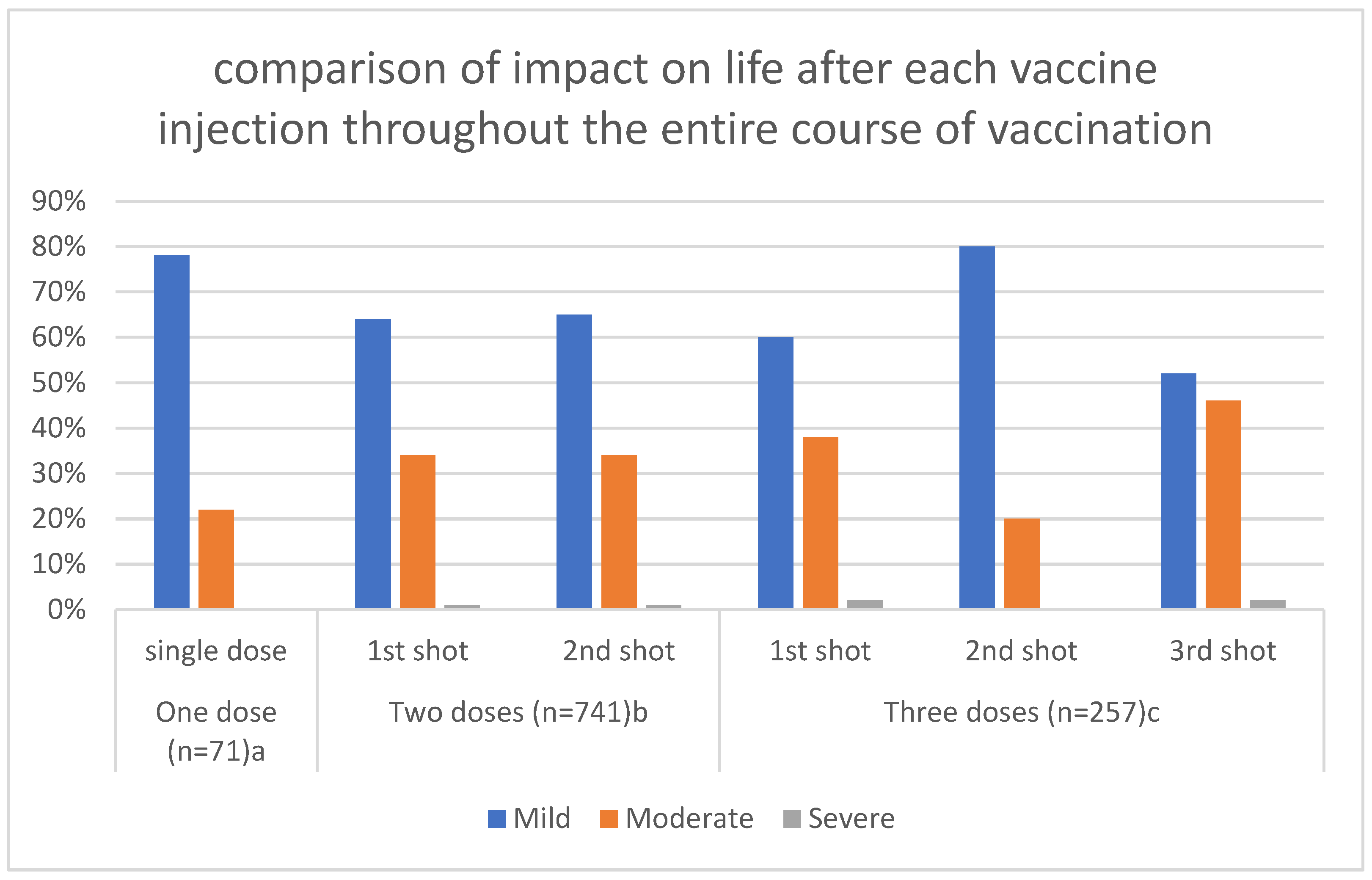
3.2.2. Severity of Reported Side Effects
3.2.3. Side Effects and 1-Week Follow-Up
3.3. Analysis of the Relationship, Associations within and between Variables
3.3.1. Individuals Who Received a Single Dose
3.3.2. Individuals Who Received Two Doses
3.3.3. Individuals Who Received Three Doses of Vaccine
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Y.-D.; Chi, W.-Y.; Su, J.-H.; Ferrall, L.; Hung, C.-F.; Wu, T.-C. Coronavirus vaccine development: From SARS and MERS to COVID-19. J. Biomed. Sci. 2020, 27, 104. [Google Scholar] [CrossRef] [PubMed]
- Habas, K.; Nganwuchu, C.; Shahzad, F.; Gopalan, R.; Haque, M.; Rahman, S.; Majumder, A.A.; Nasim, T. Resolution of coronavirus disease 2019 (COVID-19). Expert Rev. Anti-Infect. Ther. 2020, 18, 1201–1211. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. How the Oxford-AstraZeneca covid-19 vaccine was made. BMJ 2021, 372, n86. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, Y.; Huang, B.; Deng, W.; Quan, Y.; Wang, W.; Xu, W.; Zhao, Y.; Li, N.; Zhang, J.; et al. Development of an Inactivated Vaccine Candidate, BBIBP-CorV, with Potent Protection against SARS-CoV-2. Cell 2020, 182, 713–721.e9. [Google Scholar] [CrossRef]
- Ministry of Health Jordan. Jordanian Government Website. Corona Updat. 2022. Available online: https://corona.moh.gov.jo/en (accessed on 25 July 2022).
- Mushtaq, H.A.; Khedr, A.; Koritala, T.; Bartlett, B.N.; Jain, N.K.; Khan, S.A. A review of adverse effects of COVID-19 vaccines. Le Infez. Med. 2022, 30, 1. [Google Scholar] [CrossRef]
- Babaee, E.; Amirkafi, A.; Tehrani-Banihashemi, A.; SoleimanvandiAzar, N.; Eshrati, B.; Rampisheh, Z.; Asadi-Aliabadi, M.; Nojomi, M. Adverse effects following COVID-19 vaccination in Iran. BMC Infect. Dis. 2022, 22, 476. [Google Scholar] [CrossRef]
- Saeed, B.Q.; Al-Shahrabi, R.; Alhaj, S.S.; Alkokhardi, Z.M.; Adrees, A.O. Side effects and perceptions following Sinopharm COVID-19 vaccination. Int. J. Infect. Dis. 2021, 111, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, R.; Barary, M.; Mehdinezhad, H.; Sio, T.T.; Langer, F.; Khosravi, S. Thrombotic thrombocytopenia after Sinopharm BBIBP-CorV COVID-19 vaccination. Res. Pract. Thromb. Haemost. 2022, 6, e12750. [Google Scholar] [CrossRef]
- Dighriri, I.M.; Alhusayni, K.M.; Mobarki, A.Y.; Aljerary, I.S.; Alqurashi, K.A.; Aljuaid, F.A.; Alamri, K.A.; Mutwalli, A.A.; Maashi, N.A.; Aljohani, A.M.; et al. Pfizer-BioNTech COVID-19 Vaccine (BNT162b2) Side Effects: A Systematic Review. Cureus 2022, 14, e23526. [Google Scholar] [CrossRef]
- Tsabouri, S.; Makis, A.; Kosmeri, C.; Siomou, E. Risk Factors for Severity in Children with Coronavirus Disease 2019. Pediatr. Clin. North Am. 2020, 68, 321–338. [Google Scholar] [CrossRef]
- Rumain, B.; Schneiderman, M.; Geliebter, A. Prevalence of COVID-19 in adolescents and youth compared with older adults in states experiencing surges. PLoS ONE 2021, 16, e0242587. [Google Scholar] [CrossRef] [PubMed]
- Szablewski, C.M.; Chang, K.T.; Brown, M.M.; Chu, V.T.; Yousaf, A.R.; Anyalechi, N.; Aryee, P.A.; Kirking, H.L.; Lumsden, M.; Mayweather, E.; et al. SARS-CoV-2 Transmission and Infection Among Attendees of an Overnight Camp—Georgia, June 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1023–1025. [Google Scholar] [CrossRef]
- Buonsenso, D.; Roland, D.; De Rose, C.; Vásquez-Hoyos, P.; Ramly, B.; Chakakala-Chaziya, J.N.; Munro, A.; González-Dambrauskas, S. Schools Closures During the COVID-19 Pandemic. Pediatr. Infect. Dis. J. 2021, 40, e146–e150. [Google Scholar] [CrossRef] [PubMed]
- Masonbrink, A.R.; Hurley, E. Advocating for Children During the COVID-19 School Closures. Pediatrics 2020, 146, e20201440. [Google Scholar] [CrossRef]
- Food and Drug Administration (FDA). Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight Against Pandemic. Food Drug Adm. 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use (accessed on 10 May 2021).
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Gee, J.; Baggs, J.; Abara, W.E.; Marquez, P.; Thompson, D.; Su, J.R.; Licata, C.; Rosenblum, H.G.; Myers, T.R.; et al. COVID-19 Vaccine Safety in Adolescents Aged 12–17 Years. Morb. Mortal. Wkly. Rep. 2021, 70, 1053–1058. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Hernández-Vanegas, L.E.; Núñez, I.; Hernández-Valdivia, N.; Carrillo-García, D.A.; Michel-Chávez, A.; Galnares-Olalde, J.A.; Carbajal-Sandoval, G.; Saniger-Alba, M.D.M.; et al. Neurologic adverse events among 704,003 first-dose recipients of the BNT162b2 mRNA COVID-19 vaccine in Mexico: A nationwide descriptive study. Clin. Immunol. 2021, 229, 108786. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Matta, A.; Kunadharaju, R.; Osman, M.; Jesme, C.; McMiller, Z.; Johnson, E.M.; Matta, D.; Kallamadi, R.; Bande, D. Clinical Presentation and Outcomes of Myocarditis Post mRNA Vaccination: A Meta-Analysis and Systematic Review. Cureus 2021, 13, e19240. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Phadke, N.A.; Bates, D.W. Safety Surveillance of COVID-19 mRNA Vaccines through the Vaccine Safety Datalink. JAMA 2021, 326, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.R.; Pan, W.; Schumsky, D.A. Recalculation of the Critical Values for Lawshe’s Content Validity Ratio. Meas. Evaluation Couns. Dev. 2012, 45, 197–210. [Google Scholar] [CrossRef] [Green Version]
- Our Warld in Data. Coronavirus (COVID-19) Vaccinations. Vaccin. Dataset. 2021. Available online: https://ourworldindata.org/covid-vaccinations?country=JOR (accessed on 1 November 2021).
- Taherdoost, H. Determining Sample Size; How to Calculate Survey Sample Size. Int. J. Econ. Manag. Syst. 2017, 2, 236–239. [Google Scholar]
- Qualtrics. Sample Size Calculater. 2020. Available online: https://www.qualtrics.com/blog/calculating-sample-size/?fbclid=IwAR0urxilwycKuIxHio2ttEZ_yFvncrYA9BgXCJd5jQJeho2zmzfR4l3z2TU (accessed on 2 November 2021).
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Chi-Square Tests for Goodness of Fit and Contingency Tables. Stat Power Anal Behav. Sci. 1977, 2, 215–271. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Chi-squared test and Fisher’s exact test. Restor. Dent. Endod. 2017, 42, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Dudley, M.Z.; Chen, X.; Bai, X.; Dong, K.; Zhuang, T.; Salmon, D.; Yu, H. Evaluation of the safety profile of COVID-19 vaccines: A rapid review. BMC Med. 2021, 19, 173. [Google Scholar] [CrossRef] [PubMed]
- Omeish, H.; Najadat, A.; Al-Azzam, S.; Tarabin, N.; Abu Hameed, A.; Al-Gallab, N.; Abbas, H.; Rababah, L.; Rabadi, M.; Karasneh, R.; et al. Reported COVID-19 vaccines side effects among Jordanian population: A cross sectional study. Hum. Vaccines Immunother. 2021, 18, 1981086. Available online: https://www.tandfonline.com/doi/suppl/10.1080/21645515.2021.1981086?scroll=top&role=tab (accessed on 1 November 2021). [CrossRef]
- Hatmal, M.; Al-Hatamleh, M.; Olaimat, A.; Hatmal, M.; Alhaj-Qasem, D.; Olaimat, T.; Mohamud, R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef]
- Ganesan, S.; Al Ketbi, L.M.B.; Al Kaabi, N.; Al Mansoori, M.; Al Maskari, N.N.; Al Shamsi, M.S.; Alderei, A.S.; El Eissaee, H.N.; Al Ketbi, R.M.; Al Shamsi, N.S.; et al. Vaccine Side Effects Following COVID-19 Vaccination Among the Residents of the UAE—An Observational Study. Front. Public Health 2022, 10, 876336. [Google Scholar] [CrossRef]
- Almughais, E.S.; Alharbi, A.H.; Aldarwish, H.A.; Alshammari, A.F.; Alsuhaymi, R.S.; Almuaili, J.A.; Alanizy, A.M. Side-effects of COVID-19 vaccines among the Saudi population. Saudi Med. J. 2022, 43, 386–393. [Google Scholar] [CrossRef]
- Yesuf, E.A.; Riad, A.; Sofi-Mahmudi, A.; Sudhakar, M.; Mekonnen, A.; Endalkachew, S.; Mama, F.; Muhidin, S.; Ayele, B.; Yahya, M.; et al. Self-reported side effects of the Oxford AstraZeneca COVID-19 vaccine among healthcare workers in Ethiopia, Africa: A cross-sectional study. Front. Public Health 2022, 10, 937794. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity Following Receipt of mRNA-Based COVID-19 Vaccines. JAMA 2021, 325, 2201–2202. [Google Scholar] [CrossRef] [PubMed]
- Omeish, H.; Najadat, A.; Al-Azzam, S.; Tarabin, N.; Abu Hameed, A.; Al-Gallab, N.; Abbas, H.; Rababah, L.; Rabadi, M.; Karasneh, R.; et al. Reported COVID-19 vaccines side effects among Jordanian population: A cross sectional study. Hum. Vaccines Immunother. 2021, 18, 1981086. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.J.; Dutta, S.; Bhardwaj, P.; Charan, J.; Dhingra, S.; Mitra, P.; Singh, K.; Yadav, D.; Sharma, P.; Misra, S. Adverse Events Reported From COVID-19 Vaccine Trials: A Systematic Review. Indian J. Clin. Biochem. 2021, 36, 427–439. [Google Scholar] [CrossRef]
- Al-Qazaz, H.K.; Al-Obaidy, L.M.; Attash, H.M. COVID-19 vaccination, do women suffer from more side effects than men? A retrospective cross-sectional study. Pharm. Pract. 2022, 20, 2678. [Google Scholar] [CrossRef] [PubMed]
- Elnaem, M.H.; Taufek, N.H.M.; Ab Rahman, N.S.; Nazar, N.I.M.; Zin, C.S.; Nuffer, W.; Turner, C.J. COVID-19 Vaccination Attitudes, Perceptions, and Side Effect Experiences in Malaysia: Do Age, Gender, and Vaccine Type Matter? Vaccines 2021, 9, 1156. [Google Scholar] [CrossRef]
- Taneja, V. Sex Hormones Determine Immune Response. Front. Immunol. 2018, 9, 1931. [Google Scholar] [CrossRef]
- Vassallo, A.; Shajahan, S.; Harris, K.; Hallam, L.; Hockham, C.; Womersley, K.; Woodward, M.; Sheel, M. Sex and Gender in COVID-19 Vaccine Research: Substantial Evidence Gaps Remain. Front. Glob. Women’s Health 2021, 2, 761511. [Google Scholar] [CrossRef]
- Alemayehu, A.; Demissie, A.; Yusuf, M.; Abdullahi, Y.; Abdulwehab, R.; Oljira, L.; Feleke, D. COVID-19 vaccine side effect: Age and gender disparity in adverse effects following the first dose of AstraZeneca COVID-19 vaccine among the vaccinated population in Eastern Ethiopia: A community-based study. SAGE Open Med. 2022, 10, 205031212211086. [Google Scholar] [CrossRef] [PubMed]
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Mohamud, R.; Fawaz, M.; Kateeb, E.T.; Alkhairy, O.K.; Tayyem, R.; Lounis, M.; Al-Raee, M.; et al. Reported Adverse Effects and Attitudes among Arab Populations Following COVID-19 Vaccination: A Large-Scale Multinational Study Implementing Machine Learning Tools in Predicting Post-Vaccination Adverse Effects Based on Predisposing Factors. Vaccines 2022, 10, 366. [Google Scholar] [CrossRef]
- Abukhalil, A.D.; Shatat, S.S.; Abushehadeh, R.R.; Al-Shami, N.; Naseef, H.A.; Rabba, A. Side effects of Pfizer/BioNTech (BNT162b2) COVID-19 vaccine reported by the Birzeit University community. BMC Infect. Dis. 2023, 23, 5. [Google Scholar] [CrossRef] [PubMed]
- Al-Hanawi, M.K.; Keetile, M.; Kadasah, N.A.; Alshareef, N.; Qattan, A.M.N.; Alsharqi, O. Side Effects and Perceptions of COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Study. Front. Med. 2022, 9, 1462. [Google Scholar] [CrossRef]
- Capponi, M.; Pulvirenti, F.; Cinicola, B.L.; Brindisi, G.; Conti, M.G.; Colaiocco, G.; de Castro, G.; Guido, C.A.; Duse, M.; Midulla, F.; et al. Short-Term Side Effects and SARS-CoV-2 Infection after COVID-19 Pfizer–BioNTech Vaccine in Children Aged 5–11 Years: An Italian Real-World Study. Vaccines 2022, 10, 1056. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Sim, J.; Sherman, S.M.; Amlôt, R.; Cutts, M.; Dasch, H.; Sevdalis, N.; Rubin, G.J. Psychological factors associated with reporting side effects following COVID-19 vaccination: A prospective cohort study (CoVAccS—Wave 3). J. Psychosom. Res. 2023, 164, 111104. [Google Scholar] [CrossRef]
- Barsky, A.J.; Saintfort, R.; Rogers, M.P.; Borus, J.F. Nonspecific Medication Side Effects and the Nocebo Phenomenon. JAMA 2002, 287, 622–627. [Google Scholar] [CrossRef]
- Faasse, K.; Petrie, K.J. The nocebo effect: Patient expectations and medication side effects. Postgrad. Med. J. 2013, 89, 540–546. [Google Scholar] [CrossRef] [Green Version]
- Sever, P. Nocebo affects after COVID-19 vaccination. Lancet Reg. Health Eur. 2021, 12, 100273. [Google Scholar] [CrossRef]
- Amanzio, M.; Mitsikostas, D.D.; Giovannelli, F.; Bartoli, M.; Cipriani, G.E.; Brown, W.A. Adverse events of active and placebo groups in SARS-CoV-2 vaccine randomized trials: A systematic review. Lancet Reg. Health Eur. 2021, 12, 100253. [Google Scholar] [CrossRef]
- Lee, Y.H.; Song, G.G. Nocebo responses in randomized controlled trials of COVID-19 vaccines. Int. J. Clin. Pharmacol. Ther. 2022, 60, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Webster, R.K.; Weinman, J.; Rubin, G.J. A systematic review of factors that contribute to nocebo effects. Health Psychol. 2016, 35, 1334–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vambheim, S.M.; Flaten, M.A. A systematic review of sex differences in the placebo and the nocebo effect. J. Pain Res. 2017, 10, 1831–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enck, P.; Klosterhalfen, S. Does Sex/Gender Play a Role in Placebo and Nocebo Effects? Conflicting Evidence From Clinical Trials and Experimental Studies. Front. Neurosci. 2019, 13, 160. [Google Scholar] [CrossRef]
- Hoffman, Y.S.G.; Levin, Y.; Palgi, Y.; Goodwin, R.; Ben-Ezra, M.; Greenblatt-Kimron, L. Vaccine hesitancy prospectively predicts nocebo side-effects following COVID-19 vaccination. Sci. Rep. 2022, 12, 20018. [Google Scholar] [CrossRef]
- Davies, H.T.; Crombie, I.K. Bias in cohort studies. Hosp. Med. 2000, 61, 133–135. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10748794 (accessed on 9 March 2023).
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Outcome | Frequency (n = 1069) | Percentage (%) | |
|---|---|---|---|---|
| Gender | Male | 542 | 50.7% | |
| Female | 527 | 49.3% | ||
| Ag | <18 | 145 | 13.6% | |
| 18–40 | 681 | 63.7% | ||
| 40–60 | 179 | 16.7% | ||
| More 60 | 64 | 6% | ||
| Education | Primary School | 52 | 4.9% | |
| Secondary School | 179 | 16.7% | ||
| Diploma | 104 | 9.7% | ||
| Bachelor’s | 685 | 64.1% | ||
| Higher Education (Master/PhD) | 49 | 4.6% | ||
| Occupation | HCWs | 406 | 38% | |
| Non HCWs | 662 | 62% | ||
| Smoking | ||||
| Smoker | Yes | 195 | 18.2% | |
| No | 874 | 81.8% | ||
| Duration of Smoking (Years) | <5 | 85 | 43.6% | |
| 5–10 | 48 | 24.6% | ||
| >10 | 62 | 31.7% | ||
| Packets (Per day) | 1 | 153 | 78.4% | |
| 2 | 38 | 19.5% | ||
| 3 or more | 4 | 2% | ||
| Place of Residence | Amman | 701 | 65.6% | |
| Zarqa | 187 | 17.5% | ||
| Irbid | 35 | 3.3% | ||
| Mafraq | 34 | 3.2% | ||
| Balqa’ | 28 | 2.6% | ||
| Jerash | 25 | 2.3% | ||
| Madaba | 15 | 1.4% | ||
| Karak | 13 | 1.2% | ||
| Tafila | 12 | 1.1% | ||
| Ajloun | 9 | 0.8% | ||
| Ma’an | 5 | 0.5% | ||
| Aqaba | 5 | 0.5% | ||
| Vaccine type | Pfizer-Biontic | 637 | 59.6% | |
| Sinopharm | 387 | 36.2% | ||
| AstraZeneca | 45 | 4.2% | ||
| Number of doses | Single dose | 71 | 6.6% | |
| Two doses | 741 | 69.4% | ||
| Three doses | 257 | 24.0% | ||
| Vaccine type and doses | Pfizer-Biontic, n = 637 | Single dose | 46 | 7.2% |
| Two doses | 410 | 64.4% | ||
| Three doses | 181 | 28.4% | ||
| Sinopharm, n = 387 | Single dose | 21 | 5.4% | |
| Two doses | 303 | 78.3% | ||
| Three doses | 63 | 16.3% | ||
| AstraZeneca, n = 45 | Single dose | 4 | 8.9% | |
| Two doses | 28 | 62.2% | ||
| Three doses | 13 | 28.9% | ||
| Allergy | Yes | No | Not Sure | Total |
|---|---|---|---|---|
| Bee allergy | 34 | 881 | 154 | 1069 |
| Egg allergy | 19 | 1029 | 21 | 1069 |
| Fruit allergy | 6 | 1003 | 60 | 1069 |
| Milk allergy | 32 | 1005 | 32 | 1069 |
| Walnut allergy | 8 | 1037 | 24 | 1069 |
| Drug allergy | 59 | 897 | 113 | 1069 |
| Pet allergy | 72 | 932 | 65 | 1069 |
| Spring allergy | 270 | 728 | 71 | 1069 |
| Allergy to other things | 68 | 841 | 159 | 1068 |
| chronic disease | Yes | No | Not sure | Total |
| diabetes | 85 | 976 | 8 | 1069 |
| hypertension | 100 | 960 | 9 | 1069 |
| coronary artery disease | 64 | 995 | 10 | 1069 |
| liver disease | 8 | 1053 | 8 | 1069 |
| kidney disease | 9 | 1055 | 5 | 1069 |
| immunodeficiency | 10 | 1052 | 7 | 1069 |
| hematological disease | 15 | 1047 | 7 | 1069 |
| endocrine disease | 42 | 1016 | 11 | 1069 |
| respiratory disease | 41 | 1019 | 9 | 1069 |
| neurological disease | 8 | 1055 | 6 | 1069 |
| other diseases | 41 | 991 | 36 | 1068 |
| Medications | Yes | No | Not sure | Total |
| Hypertension medications | 103 | 963 | 3 | 1069 |
| Diabetes medications | 89 | 977 | 3 | 1069 |
| Anticoagulants | 95 | 971 | 3 | 1069 |
| Asthma medications | 37 | 1028 | 4 | 1069 |
| Thyroid hormone | 47 | 1016 | 6 | 1069 |
| Analgesics (NSAIDs, Paracetam) | 197 | 855 | 17 | 1069 |
| Opioids | 9 | 1056 | 4 | 1069 |
| Immunosuppressants | 22 | 1044 | 3 | 1069 |
| Antidepressants | 16 | 1048 | 5 | 1069 |
| Antibiotics | 65 | 997 | 7 | 1069 |
| Contraceptives | 20 | 1047 | 2 | 1069 |
| Seizure medications | 0 | 1067 | 2 | 1069 |
| Others | 74 | 983 | 11 | 1068 |
| One Dose (n = 71) a | Two Doses (n = 741) b | Three Doses, (n = 257) c | ||||
|---|---|---|---|---|---|---|
| Single Dose | 1st Shot | 2nd Shot | 1st Shot | 2nd Shot | 3rd Shot | |
| Ageusia | 0 (0%) | 22 (3%) | 37 (5%) | 3 (1%) | 3 (1%) | 13 (5%) |
| Anosmia | 2 (3%) | 30 (4%) | 44 (6%) | 5 (2%) | 23 (9%) | 13 (5%) |
| Arthralgia | 20 (28%) | 348 (47%) | 319 (43%) | 54 (21%) | 62 (24%) | 105 (41%) |
| Chest pain | 9 (13%) | 89 (12%) | 126 (17%) | 26 (10%) | 18 (7%) | 28 (11%) |
| Chills | 24 (34%) | 348 (47%) | 348 (47%) | 82 (32%) | 75 (29%) | 90 (35%) |
| Cough | 4 (6%) | 74 (10%) | 96 (13%) | 31 (12%) | 18 (7%) | 26 (10%) |
| Diarrhea | 6% (4) | 44 (6%) | 59 (8%) | 10 (4%) | 5 (2%) | 8 (3%) |
| dizziness | 11 (15%) | 177 (24%) | 185 (25%) | 41 (16%) | 15 (6%) | 59 (23%) |
| Face/lips swelling | 2 (3%) | 22 (3%) | 22 (3%) | 3 (1%) | 3 (1%) | 3 (1%) |
| Fatigue | 49 (69%) | 585 (79%) | 578 (78%) | 157 (61%) | 162 (63%) | 167 (65%) |
| Fever | 29 (41%) | 358 (52%) | 400 (54%) | 93 (36%) | 105 (41%) | 116 (45%) |
| Headache | 35 (49%) | 489 (66%) | 459 (62%) | 100 (39%) | 105 (41%) | 131 (51%) |
| localized pain | 53 (75%) | 615 (83%) | 585 (79%) | 200 (78%) | 167 (65%) | 195 (76%) |
| localized Redness | 24 (34%) | 259 (35%) | 274 (37%) | 113 (44%) | 89 (35%) | 105 (41%) |
| Myalgia | 27 (38%) | 437 (59%) | 393 (53%) | 64 (25%) | 67 (26%) | 115 (45%) |
| Nasal congestion | 13 (18%) | 89 (12%) | 104 (14%) | 31 (12%) | 21 (8%) | 33 (13%) |
| Nausea | 9 (13%) | 126 (17%) | 148 (20%) | 15 (6%) | 8 (3%) | 21 (8%) |
| Neurological symptoms | 0 (0%) | 22 (3%) | 30 (4%) | 3 (1%) | 5 (2%) | 23 (9%) |
| rhinorrhea | 13 (18%) | 82 (11%) | 104 (14%) | 31 (12%) | 23 (9%) | 39 (15%) |
| Shortness of breath | 16 (23%) | 126 (17%) | 163 (22%) | 28 (11%) | 15 (6%) | 26 (10%) |
| Sneezing | 6 (8%) | 67 (9%) | 93 (13%) | 21 (8%) | 13 (5%) | 28 (11%) |
| Sore throat | 11 (15%) | 96 (13%) | 89 (12%) | 26 (10%) | 21 (8%) | 51 (20%) |
| Vomiting | 6 (8%) | 30 (4%) | 37 (5%) | 5 (2%) | 3 (1%) | 15 (6%) |
| Variables | One Dose (n = 71) a | Two Doses (n = 741) b | X2 (p-Value) d | Three Doses (n = 257) c | X2 (p-Value) e | |||
|---|---|---|---|---|---|---|---|---|
| Single Dose | 1st Shot | 2nd Shot | 1st Shot | 2nd Shot | 3rd Shot | |||
| The Onset of Side Effects after Vaccination | ||||||||
| within 24 h | 58 (82%) | 615 (83%) | 608 (82%) | 0.09 (0.76) | 231 (90%) | 221 (86%) | 244 (95%) | 8.1 (0.045) |
| 1–3 days | 13 (18%) | 111 (15%) | 111 (15%) | 0.17 (0.68) | 26 (10%) | 28 (11%) | 10 (4%) | 13.1 (0.0003) |
| 3–5 days | 0 (0%) | 7 (1%) | 7 (1%) | 0.19 (0.65) | 0 (0%) | 8 (3%) | 3 (1%) | 2.7 (0.12) |
| 1 week | 0 (0%) | 7 (1%) | 15 (2%) | 4.15 (0.042) | 0 (0%) | 0 (0%) | 0 (0%) | Not Applicable |
| Duration of side effects | ||||||||
| less than 24 h | 36 (51%) | 207 28%) | 81 (11%) | 104 (<0.0001) | 157 (61%) | 177 (69%) | 129 (50%) | 1.3 (0.25) |
| 1–3 days | 29 (41%) | 401 (54%) | 363 (49%) | 0.51 (0.48) | 44 (17%) | 59 (23%) | 33 (13%) | 13.9 (0.0002) |
| 3–7 days | 6 (8%) | 89 (12%) | 230 (31%) | 81.2 (<0.0001) | 44 (17%) | 18 (7%) | 59 (23%) | 6.1 (0.015) |
| more than 1 week | 0 (0%) | 44 (6%) | 67 (9%) | 10.5 (0.0012) | 12 (5%) | 3 (1%) | 36 (14%) | 24.1 (<0.0001) |
| One Dose (n = 71) | Two Doses (n = 741) | Three Doses (n = 257) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single Dose | 1st Shot | 2nd Shot | 1st Shot | 2nd Shot | 3rd Shot | ||||||||
| Variable | category | Reported Side Effects n (%) | P a (Phi Value) b | Reported Side Effects n (%) | P a (Phi Value) b | Reported Side Effects n (%) | P a (Phi Value) b | Reported Side Effects n (%) | P a (Phi Value)b | Reported Side Effects n (%) | P a (Phi Value) b | Reported Side Effects n (%) | P a (Phi Value) b |
| Gender | Female | 19 (59.4) | 0.15 | 204 (57.6) | 0.001, (0.53) | 160 (58) | 0.001, (0.38) | 77 (63.6) | 0.045 (0.13) | 59 (60.8) | 0.46 | 105 (60) | 0.29 |
| Male | 13 (40.6) | 150 (42.2) | 116 (42) | 44 (36.4) | 38 (39.2) | 70 (40) | |||||||
| Age | <18 | 14 (43.8) | 0.9 | 55 (15.5) | 0.9 | 56 (20.3) | 0.006 (0.11) | Not Applicable | |||||
| 18 -40 | 18 (56.3) | 299 (84.5) | 220 (79.7) | ||||||||||
| Smoker | No | 31 (96.9) | 0.35 | 311 (87.9) | 0.041, (0.08) | 244 (88.4) | 0.042 (0.08) | 84 (69.4) | 0.8 | 66 (68) | 0.75 | 121 (69.1) | 0.84 |
| Yes | 1 (3.1) | 43 (12.1) | 32 (11.6) | 37 (30.6) | 31 (32) | 54 (30.9) | |||||||
| Vaccine type | Pfizer | 22 (68.8) | 0.22 | 229 (64.7) | <0.001 (0.26) | 195 (70.7) | <0.001 (0.27) | 93 (76.9) | 0.002 (0.25) | 76 (78.4) | <0.001 (0.28) | 6 (3.4) | <0.001 (0.33) |
| Sinopharm | 7 (21.9) | 102 (28.8) | 67 (24.3) | 19 (15.7) | 15 (15.5) | 52 (29.7) | |||||||
| AstraZeneca | 3 (9.4) | 23 (6.5) | 14 (5.1) | 9 (7.4) | 6 (6.2) | 117 (66.9) | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odeh, M.; Al-Jussani, G.N.; Ashour, A.; AlNaqah, H.; Hasan, H.A.; Sbitan, L.; Dawabsheh, A.; Alhawi, M. Follow-Up of Side Effects throughout the Entire Course of Coronavirus Vaccination. Vaccines 2023, 11, 704. https://doi.org/10.3390/vaccines11030704
Odeh M, Al-Jussani GN, Ashour A, AlNaqah H, Hasan HA, Sbitan L, Dawabsheh A, Alhawi M. Follow-Up of Side Effects throughout the Entire Course of Coronavirus Vaccination. Vaccines. 2023; 11(3):704. https://doi.org/10.3390/vaccines11030704
Chicago/Turabian StyleOdeh, Mohanad, Ghada Nazar Al-Jussani, Abdelrahman Ashour, Husam AlNaqah, Hamza A. Hasan, Lana Sbitan, Amro Dawabsheh, and Moayad Alhawi. 2023. "Follow-Up of Side Effects throughout the Entire Course of Coronavirus Vaccination" Vaccines 11, no. 3: 704. https://doi.org/10.3390/vaccines11030704