
Evolution of SARS-CoV-2 IgG Seroprevalence in Children and Factors Associated with Seroconversion: Results from a Multiple Time-Points Study in Friuli-Venezia Giulia Region, Italy

 , , ,
, , ,
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design
2.2. Population and Settings
2.3. Data Collection Procedures
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Patient Enrollment
3.2. Characteristics of Children
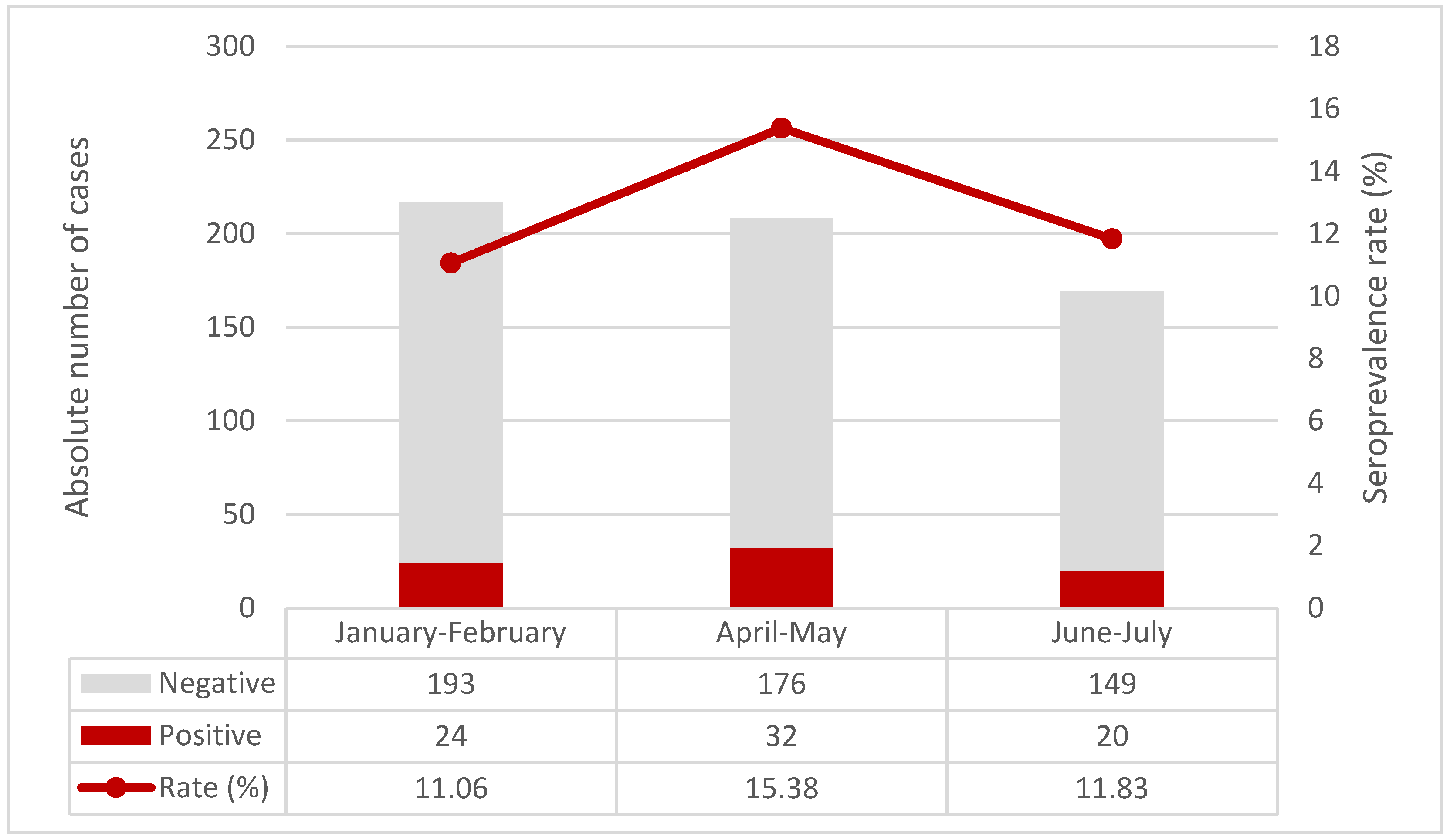
3.3. Findings on Anti-SARS-CoV-2 IgG Antibodies
3.4. Subgroup Analysis
3.5. Multivariate Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Recommendations. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-2-global-serologic-study-for-covid-19 (accessed on 25 January 2022).
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M.; Nourollahpour Shiadeh, M.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Einarsdóttir, J. Research with children: Methodological and ethical challenges. Eur. Early Child. Educ. Res. J. 2007, 15, 197–211. [Google Scholar] [CrossRef]
- SeroTracker. Available online: https://serotracker.com/en/Explore (accessed on 17 October 2021).
- Istat. Indagine Sierologica su Covid-19 Condotta da Ministero Della Salute e Istat. 12 June 2020. Available online: https://www.istat.it/it/archivio/242676 (accessed on 17 October 2021).
- Pagani, G.; Conti, F.; Giacomelli, A.; Bernacchia, D.; Rondanin, R.; Prina, A.; Scolari, V.; Gandolfi, C.E.; Castaldi, S.; Marano, G.; et al. Seroprevalence of SARS-CoV-2 significantly varies with age: Preliminary results from a mass population screening. J. Infect. 2020, 81, e10–e12. [Google Scholar] [CrossRef] [PubMed]
- Cerino, P.; Coppola, A.; Volzone, P.; Pizzolante, A.; Pierri, B.; Atripaldi, L.; Zollo, M.; Capasso, M.; Ascierto, P.A.; Triassi, M.; et al. Seroprevalence of SARS-CoV-2-specific antibodies in the town of Ariano Irpino (Avellino, Campania, Italy): A population-based study. Future Sci. OA 2021, 12, FSO673. [Google Scholar] [CrossRef]
- Capai, L.; Ayhan, N.; Masse, S.; Canarelli, J.; Priet, S.; Simeoni, M.H.; Charrel, R.; Lamballerie, X.; Falchi, A. Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020. J. Clin. Med. 2020, 5, 3569. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Dolci, C.; Boccalari, E.; Izadi, S.; Salvatierra Rios, L.H.; Festa, M.; Panetta, V.; De Vito, D.; Tartaglia, G.M. Serological Profile of Children and Young Adults with at Least One SARS-CoV-2 Positive Cohabitant: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 1488. [Google Scholar] [CrossRef]
- Hozé, N.; Paireau, J.; Lapidus, N.; Tran Kiem, C.; Salje, H.; Severi, G.; Touvier, M.; Zins, M.; de Lamballerie, X.; Lévy-Bruhl, D.; et al. Monitoring the proportion of the population infected by SARS-CoV-2 using age-stratified hospitalisation and serological data: A modelling study. Lancet Public Health 2021, 8, S2468–S2667. [Google Scholar] [CrossRef]
- Stringhini, S.; Zaballa, M.E.; Perez-Saez, J.; Pullen, N.; de Mestral, C.; Picazio, A.; Pennacchio, F.; Wisniak, A.; Richard, A.; Baysson, H.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies after the second pandemic peak. Lancet Infect Dis. 2021, 21, 600–601. [Google Scholar] [CrossRef]
- Ulyte, A.; Radtke, T.; Abela, I.A.; Haile, S.R.; Berger, C.; Huber, M.; Schanz, M.; Schwarzmueller, M.; Trkola, A.; Fehr, J.; et al. Clustering and longitudinal change in SARS-CoV-2 seroprevalence in school children in the canton of Zurich, Switzerland: Prospective cohort study of 55 schools. BMJ 2021, 372, n616. [Google Scholar] [CrossRef]
- Waterfield, T.; Watson, C.; Moore, R.; Ferris, K.; Tonry, C.; Watt, A.; McGinn, C.; Foster, S.; Evans, J.; Lyttle, M.D.; et al. Seroprevalence of SARS-CoV-2 antibodies in children: A prospective multicentre cohort study. Arch. Dis. Child. 2021, 106, 680–686. [Google Scholar] [CrossRef]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; CMMID COVID-19 Working Group; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Comar, M.; Benvenuto, S.; Lazzerini, M.; Fedele, G.; Barbi, E.; Amaddeo, A.; Risso, F.M.; Strajn, T.; Di Rocco, P.; Stefanelli, P.; et al. Prevalence of SARS-CoV-2 infection in Italian pediatric population: A regional seroepidemiological study. Ital. J. Pediatr. 2021, 5, 131. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Friuli Venezia-Giulia Region. Available online: https://www.regione.fvg.it/rafvg/export/sites/default/RAFVG/cultura-sport/immigrazione/FOGLIA2/allegati/7_POPOLAZIONE_STRANIERA_2020_Report_07-20.pdf (accessed on 11 December 2021).
- Presidency of The Council of Ministers, Civil Protection Department. Available online: https://mappe.protezionecivile.gov.it/it/mappe-emergenze/mappe-coronavirus/situazione-desktop (accessed on 4 December 2021).
- Wang, R.; Jin, F.; Cao, S.; Yuan, H.; Qu, J.; Zhang, J.; Li, Y.; Chen, X.; Song, W.; Xie, Z. Seroprevalence of SARS-CoV-2 infections among children visiting a hospital. Pediatr. Investig. 2020, 4, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Oeser, C.; Whitaker, H.; Linley, E.; Borrow, R.; Tonge, S.; Brown, C.S. Large increases in SARS-CoV-2 seropositivity in children in England: Effects of the delta wave and vaccination. J. Infect. 2021, 30. [Google Scholar] [CrossRef]
- Wauthier, L.; Delefortrie, Q.; Eppe, N.; Vankerkhoven, P.; Wolff, E.; Dekeyser, M.; Cirriez, J.M.; Grimmelprez, A. SARS-CoV-2 seroprevalence in high-risk health care workers in a Belgian general hospital: Evolution from the first wave to the second. Acta Clin. Belg. 2021, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sughayer, M.A.; Mansour, A.; Al Nuirat, A.; Souan, L.; Ghanem, M.; Siag, M. Dramatic rise in seroprevalence rates of SARS-CoV-2 antibodies among healthy blood donors: The evolution of a pandemic. Int. J. Infect. Dis. 2021, 107, 116–120. [Google Scholar] [CrossRef]
- Italian National Institute of Health. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bolletino-sorveglianza-integrata-COVID-19_3-novembre-2021_appendix.pdf (accessed on 11 December 2021).
- GIMBE Foundation. Available online: https://coronavirus.gimbe.org/regioni.it-IT.html#Friuli%20Venezia%20Giulia (accessed on 11 December 2021).
- Szépfalusi, Z.; Schmidthaler, K.; Sieber, J.; Kopanja, S.; Götzinger, F.; Schoof, A.; Hoz, J.; Willinger, B.; Makristathis, A.; Weseslindtner, L.; et al. Lessons from low seroprevalence of SARS-CoV-2 antibodies in schoolchildren: A cross-sectional study. Pediatr. Allergy Immunol. 2021, 32, 762–770. [Google Scholar] [CrossRef]
- Sananez, I.; Raiden, S.C.; Algieri, S.C.; Uranga, M.; Grisolía, N.A.; Filippo, D.; De Carli, N.; Lalla, S.D.; Cairoli, H.; Chiolo, M.J.; et al. A poor and delayed anti-SARS-CoV2 IgG response is associated to severe COVID-19 in children. EBioMedicine 2021, 72, 103615. [Google Scholar] [CrossRef]
- Weisberg, S.P.; Connors, T.J.; Zhu, Y.; Baldwin, M.R.; Lin, W.H.; Wontakal, S.; Szabo, P.A.; Wells, S.B.; Dogra, P.; Gray, J.; et al. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat. Immunol. 2021, 22, 25–31. [Google Scholar] [CrossRef]
- Posfay-Barbe, K.M.; Andrey, D.O.; Virzi, J.; Cohen, P.; Pigny, F.; Goncalves, A.R.; Pinosch, S.; Lacroix, L.; Stringhini, S.; Kaiser, L.; et al. Prevalence of Immunoglobulin G (IgG) Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Evaluation of a Rapid MEDsan IgG Test in Children Seeking Medical Care. Clin. Infect. Dis. 2021, 72, e192–e195. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.S.; Costa, V.; Racine-Brzostek, S.E.; Acker, K.P.; Yee, J.; Chen, Z.; Karbaschi, M.; Zuk, R.; Rand, S.; Sukhu, A.; et al. Association of Age With SARS-CoV-2 Antibody Response. JAMA Netw. Open. 2021, 4, e214302. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Valentini, P.; De Rose, C.; Pata, D.; Sinatti, D.; Speziale, D.; Ricci, R.; Carfì, A.; Landi, F.; Ferrari, V.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in children with household exposure to adults with COVID-19: Preliminary findings. Pediatr. Pulmonol. 2021, 56, 1374–1377. [Google Scholar] [CrossRef] [PubMed]
- Reggio Emilia COVID-19 Working Group. Prevalence of SARS-CoV-2 (Covid-19) in Italians and in immigrants in an area of Northern Italy (Reggio Emilia). Epidemiol. Prev. 2020, 44, 304–307. [Google Scholar] [CrossRef]
- Balachandran, H.; Phetsouphanh, C.; Agapiou, D.; Adhikari, A.; Rodrigo, C.; Hammoud, M. Maintenance of broad neutralizing antibodies and memory B cells 1 year post-infection is predicted by SARS-CoV-2-specific CD4+ T cell responses. Cell Rep. 2022, 19, 110345. [Google Scholar] [CrossRef]
- Pfizer. Press Release Archive. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-receive-first-us-fda-emergency-use (accessed on 11 December 2021).
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2021, 386, 35–46. [Google Scholar] [CrossRef]
- Moghadas, S.M.; Fitzpatrick, M.C.; Shoukat, A. Simulated Identification of Silent COVID-19 Infections Among Children and Estimated Future Infection Rates With Vaccination. JAMA Netw. Open 2021, 4, e217097. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| January–February N = 217 n (%) | April–May N = 208 n (%) | June–July N = 169 n (%) | p-Value | |
|---|---|---|---|---|
| Sociodemographic characteristics | ||||
| Sex | ||||
| Female | 101 (46.5) | 99 (47.6) | 77 (45.6) | 0.92 |
| Male | 116 (53.5) | 109 (52.4) | 92 (54.4) | 0.92 |
| Age, median [IQR; min–max] | 11 [7–13; 0–17] | 11 [7–14; 0–18] | 11 [6–13; 0–18] | 0.26 |
| Age as category | ||||
| <5 years | 44 (20.3) | 40 (19.2) | 39 (23.1) | 0.64 |
| 5–11 years | 69 (31.8) | 70 (33.7) | 64 (37.9) | 0.45 |
| 12–18 years | 104 (47.9) | 98 (47.1) | 66 (39.1) | 0.17 |
| Citizenship | ||||
| Italian | 197 (90.8) | 196 (94.2) | 152 (89.9) | 0.26 |
| Foreign | 20 (9.2) | 12 (5.8) | 17 (10.1) | 0.26 |
| Children cohabitant with a healthcare worker | 27 (12.4) | 28 (13.5) | 19 (11.2) | 0.81 |
| Comorbidity, any | 108 (49.8) 1 | 79 (38.0) | 66 (39.1) | 0.03 |
| Syndromes or genetic disorders | 23 (10.6) | 28 (13.5) | 25 (14.8) | 0.44 |
| Autoimmune diseases | 21 (9.7) 1 | 8 (3.8) | 6 (3.6) | 0.01 |
| Obesity/overweight | 13 (6.0) | 13 (6.2) | 6 (3.6) | 0.45 |
| Preterm | 8 (3.7) | 8 (3.8) | 4 (2.4) | 0.71 |
| Asthma or allergic disease | 8 (3.7) | 3 (1.4) | 4 (2.4) | 0.33 |
| Type 1 Diabetes Mellitus | 4 (1.8) | 3 (1.4) | 6 (3.6) | 0.38 |
| Cerebral palsy/disability/other neurological disease | 4 (1.8) | 4 (1.9) | 5 (3.0) | 0.73 |
| Other | 13 (6.0) | 7 (3.4) | 6 (3.6) | 0.34 |
| More than one comorbidity | 14 (6.5) | 5 (2.4) | 4 (2.4) | 0.06 |
| No comorbidities | 109 (50.2) 1 | 129 (62.0) | 103 (60.9) | 0.03 |
| Nasopharyngeal swab | ||||
| Children ever tested with a nasopharyngeal swab * | 148 (68.2) | 148 (71.2) | 125 (74.0) | 0.46 |
| Children ever tested and positive | 6/142 (4.1) | 7/148 (4.7) | 3/122 (2.4) | 0.59 |
| Timing (for children ever tested and positive) | ||||
| <3 months before | 5/6 (83.3) | 2/7 (28.6) | 1/3 (33.3) | 0.13 |
| 3–6 months before | 1/6 (16.7) | 4/7 (57.1) | 2/3 (66.7) | 0.29 |
| >6 months before | 0/6 (0.0) | 1/7 (14.3) | 0/3 (0.0) | >0.99 |
| Children cohabitant with a person with a history of a previous positive nasopharyngeal swab ** | 28 (12.9) | 36 (17.3) | 24 (14.2) | 0.43 |
| Children tested by nasopharyngeal swab | 28/28 (100) 1 | 28/36 (77.8) | 22/24 (91.7) | 0.02 |
| Resulting positive | 4/28 (14.3) | 6/28 (21.4) | 2/22 (9.1) | 0.54 |
| Results of anti-SARS-CoV-2 Spike protein IgG antibodies | ||||
| Positive | 24 (11.1) | 32 (15.4) | 20 (11.8) | 0.37 |
| January–February n/N (%) | April–May n/N (%) | June–July n/N (%) | p-Value | |
|---|---|---|---|---|
| Children with a previous positive nasopharyngeal swab * | ||||
| Positive anti-SARS-CoV-2 Spike protein IgG antibodies | 6/6 (100) | 4/7 (57.1) | 3/3 (100) | 0.17 |
| Children with a previous negative nasopharyngeal swab * | ||||
| Positive anti-SARS-CoV-2 Spike protein IgG antibodies | 16/142 (11.3) | 17/141 (12.1) | 15/122 (12.3) | 0.96 |
| Anti-SARS-CoV-2 Spike Protein IgG Antibodies | |||
|---|---|---|---|
| Positive N = 76 n (%) | Negative N = 518 n (%) | p-Value | |
| Sociodemographic characteristics | |||
| Sex | |||
| Female | 38 (50.0) | 239 (46.1) | 0.61 |
| Male | 38 (50.0) | 279 (53.9) | 0.61 |
| Age, median (IQR; min–max) | 11.0 (6.0, 15.0; 0–18) | 11.0 (7.0, 14.0; 0–17) | 0.49 |
| Age as category | |||
| <5 years | 18 (23.7) | 105 (20.3) | 0.49 |
| 5–11 years | 22 (28.9) | 181 (34.9) | 0.30 |
| 12–18 years | 36 (47.4) | 232 (44.8) | 0.67 |
| Citizenship | |||
| Italian | 63 (82.9) | 482 (93.1) | 0.005 |
| Foreign | 13 (17.1) | 36 (6.9) | 0.005 |
| Children cohabitant with a healthcare worker | 10 (13.2) | 64 (12.4) | 0.99 |
| Comorbidity, any | 38 (50.0) | 215 (41.5) | 0.16 |
| Syndromes or genetic disorders | 12 (15.8) | 64 (12.4) | |
| Autoimmune diseases | 4 (5.3) | 31 (6.0) | >0.99 |
| Obesity/overweight | 5 (6.6) | 27 (5.2) | 0.62 |
| Preterm | 5 (6.6) | 15 (2.9) | 0.096 |
| Asthma or allergic disease | 1 (1.3) | 14 (2.7) | 0.71 |
| Type 1 Diabetes Mellitus | 2 (2.6) | 11 (2.1) | 0.68 |
| Cerebral palsy/disability/other neurological disease | 2 (2.6) | 11 (2.1) | 0.68 |
| Other | 2 (2.6) | 24 (4.6) | 0.56 |
| More than one comorbidity | 5 (6.6) | 18 (3.5) | 0.19 |
| No comorbidities | 38 (50.0) | 303 (58.5) | 0.46 |
| Nasopharyngeal swab | |||
| Children ever tested with a nasopharyngeal swab * | 61 (80.3) | 360 (69.5) | 0.05 |
| Children ever tested * and positive | 13/61 (21.3) | 3/360 (0.8) | <0.001 |
| Timing (for children ever tested and positive) | |||
| <3 months before | 6/13 (46.2) | 2/3 (66.7) | >0.99 |
| 3–6 months before | 7/13 (53.8) | 0/3 (0.0) | 0.21 |
| >6 months before | 0/13 (0.0) | 1/3 (33.3) | 0.19 |
| Children cohabitant with a person with a history of a previous positive nasopharyngeal swab ** | 41 (54.0) | 47 (9.1) | <0.001 |
| Children tested by nasopharyngeal swab | 35/41 (85.4) | 43/47 (91.5) | 0.50 |
| Resulting positive | 9/35 (25.7) | 3/43 (7.0) | 0.03 |
| Anti-SARS-CoV-2 Spike protein IgG antibodies titre (BAU/mL) (IQR; min–max) | 201 (74.1–382.2; 33.9–3900) | - | - |
| AdjOR (95%CI) | p-Value | |
|---|---|---|
| Sex | ||
| Female | 1.12 (0.63–2.00) | 0.69 |
| Male | Ref | Ref |
| Age | ||
| <5 years | 1.44 (0.69–2.98) | 0.33 |
| 5–11 years | 1.02 (0.52–1.98) | 0.96 |
| 12–18 years | Ref | Ref |
| Citizenship | ||
| Italian | Ref | Ref |
| Foreign | 2.45 (1.05–5.70) | 0.002 |
| Children cohabitant with a healthcare worker | ||
| Yes | 0.69 (0.28–1.75) | 0.44 |
| No | Ref | Ref |
| Comorbidity | ||
| Syndromes or genetic disorders | 1.13 (0.49–2.63) | 0.78 |
| Autoimmune diseases | 0.79 (0.21–2.96) | 0.72 |
| Obesity/overweight | 1.47 (0.49–4.40) | 0.13 |
| Preterm | 1.73 (0.43–7.00) | 0.44 |
| Asthma or allergic disease | 0.45 (0.05–3.94) | 0.47 |
| Type 1 Diabetes Mellitus | 1.55 (0.27–8.94) | 0.62 |
| Cerebral palsy/disability/other neurological disease | 1.39 (0.24–8.01) | 0.71 |
| Other | 0.62 (0.08–4.45) | 0.63 |
| More than one comorbidity | 3.07 (0.87–10.82) | 0.08 |
| No comorbidities | Ref | Ref |
| Children ever tested with a nasopharyngeal swab * | ||
| Yes | 0.99 (0.50–1.97) | 0.28 |
| No | Ref | Ref |
| Children ever resulted positive to a nasopharyngeal swab * | ||
| Yes | 15.41 (3.44–69.04) | <0.001 |
| No | Ref | Ref |
| Children cohabitant with a person with a history of a previous positive nasopharyngeal swab ** | ||
| Yes | 9.95 (5.35–18.52) | <0.001 |
| No | Ref | Ref |
| Anti-SARS-CoV-2 Spike protein IgG antibodies test | ||
| January–February | Ref | Ref |
| April–May | 1.45 (0.73–2.86) | 0.29 |
| June–July | 1.18 (0.57–2.47) | 0.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazzerini, M.; Benvenuto, S.; Mariani, I.; Fedele, G.; Leone, P.; Stefanelli, P.; Vittori, G.; Schreiber, S.; Tommasini, A.; Rezza, G.; et al. Evolution of SARS-CoV-2 IgG Seroprevalence in Children and Factors Associated with Seroconversion: Results from a Multiple Time-Points Study in Friuli-Venezia Giulia Region, Italy. Children 2022, 9, 246. https://doi.org/10.3390/children9020246
Lazzerini M, Benvenuto S, Mariani I, Fedele G, Leone P, Stefanelli P, Vittori G, Schreiber S, Tommasini A, Rezza G, et al. Evolution of SARS-CoV-2 IgG Seroprevalence in Children and Factors Associated with Seroconversion: Results from a Multiple Time-Points Study in Friuli-Venezia Giulia Region, Italy. Children. 2022; 9(2):246. https://doi.org/10.3390/children9020246
Chicago/Turabian StyleLazzerini, Marzia, Simone Benvenuto, Ilaria Mariani, Giorgio Fedele, Pasqualina Leone, Paola Stefanelli, Giada Vittori, Silvana Schreiber, Alberto Tommasini, Giovanni Rezza, and et al. 2022. "Evolution of SARS-CoV-2 IgG Seroprevalence in Children and Factors Associated with Seroconversion: Results from a Multiple Time-Points Study in Friuli-Venezia Giulia Region, Italy" Children 9, no. 2: 246. https://doi.org/10.3390/children9020246