
Mental Health and Coping Strategies among University Staff during the COVID-19 Pandemic: A Cross–Sectional Analysis from Saudi Arabia

 ,
, 
 ,
,  ,
,  ,
,  ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
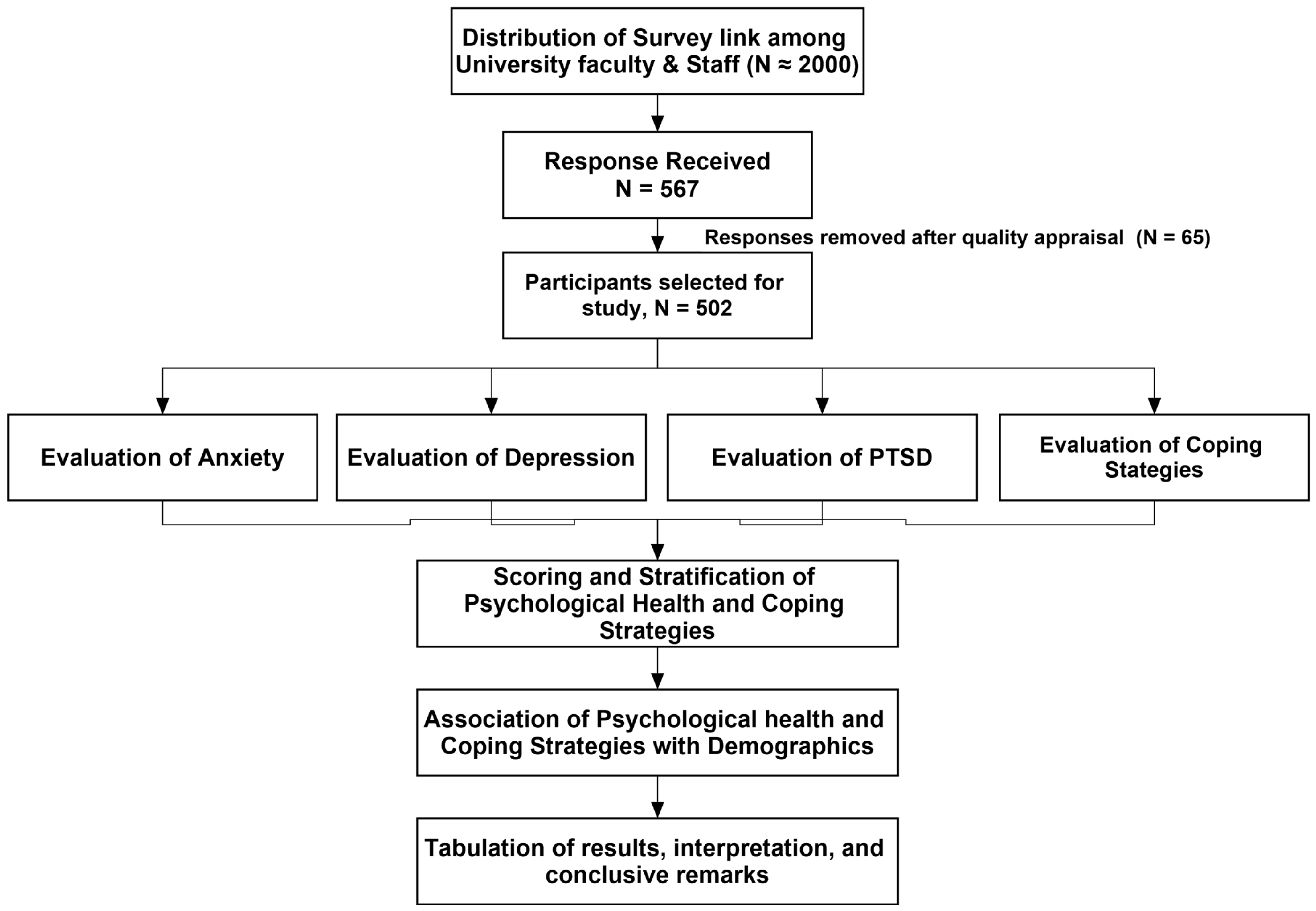
2.1. Study Design, Settings, and Subjects
2.2. Ethics Statement and Approval
2.3. Survey Instrument, Outcome Measures and Validation
2.3.1. Outcome Measures
2.3.2. Translation and Validation
2.4. Sampling and Data Collection
2.5. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Psychological Outcomes
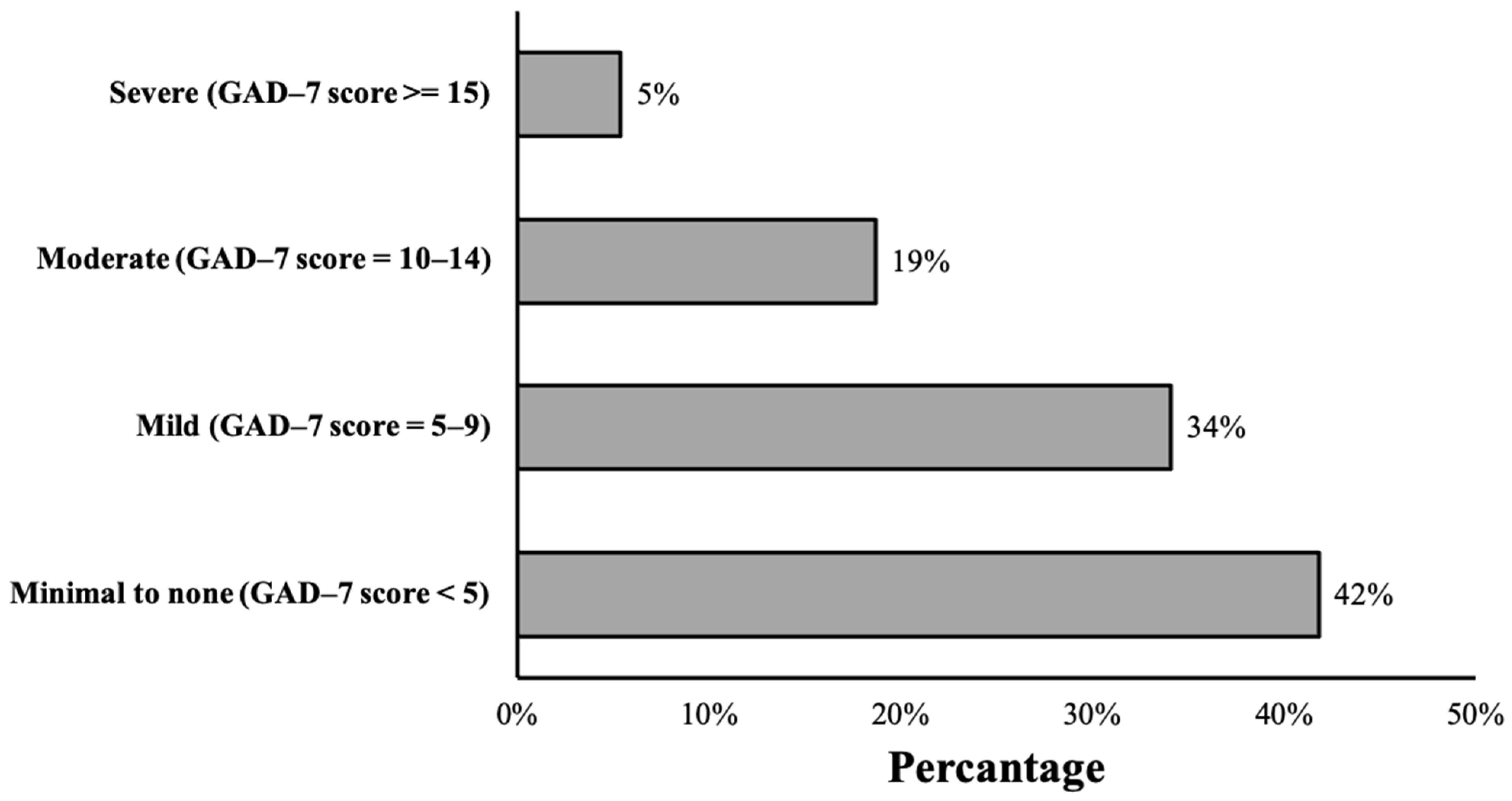
3.2.1. Anxiety and Depression
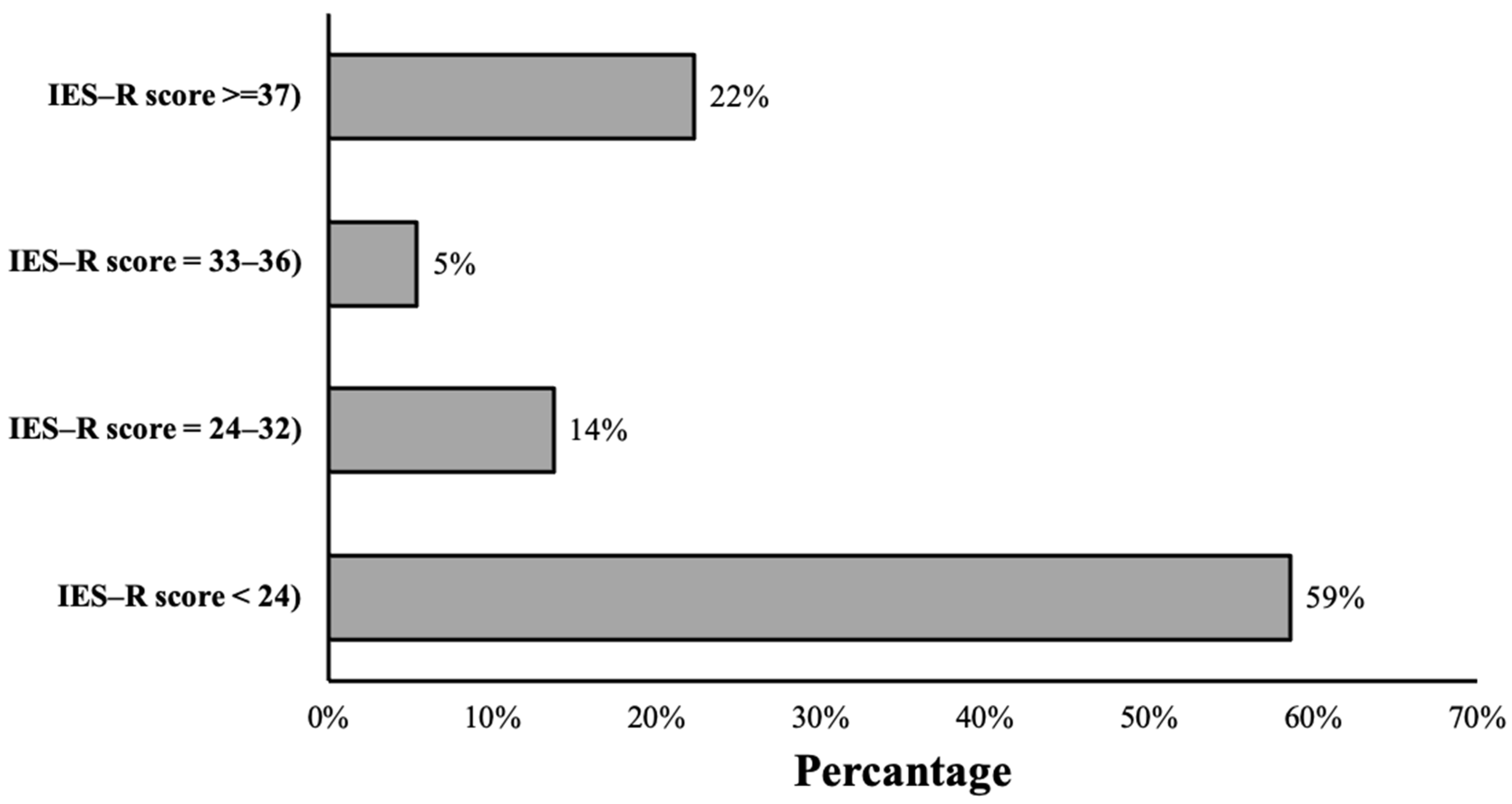
3.2.2. Post-Traumatic Stress Disorder
3.3. Coping Strategies
3.4. Association between Anxiety, Depression, PTSD and Coping Methods
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ILO; FAO; IFAD; WHO. Impact of COVID-19 on People’s Livelihoods, Their Health and Our Food Systems; World Health Organization (WHO): Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief, 2 March 2022; World Health Organization (WHO): Geneva, Switzerland, 2022. [Google Scholar]
- Davtyan, M.; Brown, B.; Folayan, M.O. Addressing Ebola-related stigma: Lessons learned from HIV/AIDS. Glob. Health Action 2014, 7, 26058. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.; Asif, N.; Mustafa, Z.U.; Khan, T.M.; Shehzadi, N.; Tahir, H.; Raza, M.H.; Khan, M.T.; Hussain, K.; Khan, Y.H. Psychological impairment and coping strategies during the COVID-19 pandemic among students in Pakistan: A cross-sectional analysis. Disaster Med. Public Health Prep. 2022, 16, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.; Mallhi, T.H.; Tanveer, N.; Shehzadi, N.; Khan, H.M.; Mustafa, Z.U.; Khan, T.M.; Hussain, K.; Mohamed, M.S.; Maqbool, F. Evaluation of Conspiracy Beliefs, Vaccine Hesitancy, and Willingness to Pay towards COVID-19 Vaccines in Six Countries from Asian and African Regions: A Large Multinational Analysis. Vaccines 2022, 10, 1866. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, J.F.; Grace, D. The consequences of human actions on risks for infectious diseases: A review. Infect. Ecol. Epidemiol. 2015, 5, 30048. [Google Scholar] [CrossRef]
- Mallhi, T.H.; Ahmad, N.; Salman, M.; Tanveer, N.; Shah, S.; Butt, M.H.; Alatawi, A.D.; Alotaibi, N.H.; Rahman, H.U.; Alzarea, A.I. Estimation of Psychological Impairment and Coping Strategies during COVID-19 Pandemic among University Students in Saudi Arabia: A Large Regional Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14282. [Google Scholar] [CrossRef]
- Zhu, X.; Liu, J. Education in and after COVID-19: Immediate responses and long-term visions. Postdigital Sci. Educ. 2020, 2, 695–699. [Google Scholar] [CrossRef]
- Business, G. Saudi Arabia to Close Schools Indefinitely from Monday. 2020. Available online: https://gulfbusiness.com/saudi-arabia-close-schools-monday/ (accessed on 5 January 2023).
- Alrasheedy, A.A.; Abdulsalim, S.; Farooqui, M.; Alsahali, S.; Godman, B. Knowledge, attitude and practice about coronavirus disease (COVID-19) pandemic and its psychological impact on students and their studies: A cross-sectional study among pharmacy students in Saudi Arabia. Risk Manag. Healthc. Policy 2021, 14, 729. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Santxo, N.B.; Mondragon, N.I.; Santamaría, M.D. The psychological state of teachers during the COVID-19 crisis: The challenge of returning to face-to-face teaching. Front. Psychol. 2021, 11, 620718. [Google Scholar] [CrossRef]
- Kita, Y.; Yasuda, S.; Gherghel, C. Online education and the mental health of faculty during the COVID-19 pandemic in Japan. Sci. Rep. 2022, 12, 8990. [Google Scholar] [CrossRef]
- Alhazmi, R.A.; Alghadeer, S.; Al-Arifi, M.N.; Alamer, A.A.; Mubarak, A.M.; Alwhaibi, A.; Alfayez, R.; Alsubaie, S. Prevalence and Factors of Anxiety during the Coronavirus-2019 Pandemic Among Teachers in Saudi Arabia. Front. Public Health 2022, 10, 827238. [Google Scholar] [CrossRef]
- AlHadi, A.N.; AlAteeq, D.A.; Al-Sharif, E.; Bawazeer, H.M.; Alanazi, H.; AlShomrani, A.T.; Shuqdar, R.M.; AlOwaybil, R. An arabic translation, reliability, and validation of Patient Health Questionnaire in a Saudi sample. Ann. Gen. Psychiatry 2017, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- AlHadi, A.N.; Alarabi, M.A.; AlMansoor, K.M. Mental health and its association with coping strategies and intolerance of uncertainty during the COVID-19 pandemic among the general population in Saudi Arabia: Cross-sectional study. BMC Psychiatry 2021, 21, 382. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wilson, J.P.; Keane, T.M. Assessing Psychological Trauma and PTSD; Guilford Press: New York, NY, USA, 2004. [Google Scholar]
- Carver, C.S. You want to measure coping but your protocol’too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Eisenberg, S.A.; Shen, B.-J.; Schwarz, E.R.; Mallon, S. Avoidant coping moderates the association between anxiety and patient-rated physical functioning in heart failure patients. J. Behav. Med. 2012, 35, 253–261. [Google Scholar] [CrossRef]
- Dias, C.; Cruz, J.F.; Fonseca, A.M. The relationship between multidimensional competitive anxiety, cognitive threat appraisal, and coping strategies: A multi-sport study. Int. J. Sport Exerc. Psychol. 2012, 10, 52–65. [Google Scholar] [CrossRef]
- Meyer, B. Coping with severe mental illness: Relations of the Brief COPE with symptoms, functioning, and well-being. J. Psychopathol. Behav. Assess. 2001, 23, 265–277. [Google Scholar] [CrossRef]
- Alghamdi, M. Cross-cultural validation and psychometric properties of the Arabic Brief COPE in Saudi population. Med. J. Malays. 2020, 75, 502–509. [Google Scholar]
- Alharbi, H.Y.; Alharthi, S.S.; Alzahrani, A.S. Reliability and validity of Arabic translation of the impact of event scale-revised for COVID-19 pandemic. Med. Sci. 2020, 24, 3051–3060. [Google Scholar]
- Tomczak, M.; Tomczak, E. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. Trends Sport Sci. 2014, 21, 19–25. [Google Scholar]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Allen, S.F.; Stevenson, J.; Lazuras, L.; Akram, U. The role of the COVID-19 pandemic in altered psychological well-being, mental health and sleep: An online cross-sectional study. Psychol. Health Med. 2022, 27, 343–351. [Google Scholar] [CrossRef]
- Kinman, G.; Jones, F. A life beyond work? Job demands, work-life balance, and wellbeing in UK academics. J. Hum. Behav. Soc. Environ. 2008, 17, 41–60. [Google Scholar] [CrossRef]
- Watts, J.; Robertson, N. Burnout in university teaching staff: A systematic literature review. Educ. Res. 2011, 53, 33–50. [Google Scholar] [CrossRef]
- Kinman, G. Pressure points: A review of research on stressors and strains in UK academics. Educ. Psychol. 2001, 21, 473–492. [Google Scholar] [CrossRef]
- Alfakeh, S.A. Impact of COVID-19 on the Mental Health of University Students. Ann. Med. Health Sci. Res. 2021, 11, 1348. [Google Scholar]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Dragioti, E.; Li, H.; Tsitsas, G.; Lee, K.H.; Choi, J.; Kim, J.; Choi, Y.J.; Tsamakis, K.; Estradé, A.; Agorastos, A. A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J. Med. Virol. 2022, 94, 1935–1949. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, A.A.; Alqassim, A.Y.; Muaddi, M.A.; Makeen, A.M.; Hagawi, A.M.; Shaabi, L.A.; Alhweity, S.M.; Alharbi, M.A.; Sultan, M.A.; Alshamakhi, A.H. Generalized anxiety disorder symptoms during COVID-19 pandemic in Jazan, Saudi Arabia. Heliyon 2022, 8, e09424. [Google Scholar] [CrossRef] [PubMed]
- Alsaif, B.; Algahtani, F.D.; Alzain, M.A.; Zrieq, R.; Aldhmadi, B.K.; Alnasser, B.; Hassan, S.-u.-N. Risk of depression, anxiety, and stress among the Saudi general population during the COVID-19 pandemic. BMC Psychol. 2022, 10, 304. [Google Scholar] [CrossRef]
- Lee, K.W.; Yap, S.F.; Ong, H.T.; Pheh, K.S.; Lye, M.S. Anxiety and coping strategies during the COVID-19 pandemic: A cross-sectional study of staff and students from a tertiary education center in Malaysia. Front. Public Health 2022, 10, 936486. [Google Scholar] [CrossRef]
- Ali, M.S.; Naoreen, B.; Iqbal, A.; Jalal, H. Online Teaching, Psychological State, and Job Satisfaction: Teachers’ Perspective during COVID-19 Pandemic. Ilkogr. Online 2021, 20, 358–364. [Google Scholar]
- Miguel, C.; Castro, L.; Marques dos Santos, J.P.; Serrão, C.; Duarte, I. Impact of COVID-19 on medicine lecturers’ mental health and emergency remote teaching challenges. Int. J. Environ. Res. Public Health 2021, 18, 6792. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the students of Saudi Arabia. Open Public Health J. 2021, 14, 12–23. [Google Scholar] [CrossRef]
- Idoiaga, N.; Legorburu, I.; Ozamiz-Etxebarria, N.; Lipnicki, D.M.; Villagrasa, B.; Santabárbara, J. Prevalence of Post-Traumatic Stress Disorder (PTSD) in University Students during the COVID-19 Pandemic: A Meta-Analysis Attending SDG 3 and 4 of the 2030 Agenda. Sustainability 2022, 14, 7914. [Google Scholar] [CrossRef]
- Fan, C.; Fu, P.; Li, X.; Li, M.; Zhu, M. Trauma exposure and the PTSD symptoms of college teachers during the peak of the COVID-19 outbreak. Stress Health 2021, 37, 914–927. [Google Scholar] [CrossRef]
- Akour, A.; Ala’a, B.; Barakat, M.; Kanj, R.; Fakhouri, H.N.; Malkawi, A.; Musleh, G. The impact of the COVID-19 pandemic and emergency distance teaching on the psychological status of university teachers: A cross-sectional study in Jordan. Am. J. Trop. Med. Hyg. 2020, 103, 2391. [Google Scholar] [CrossRef]
- Al Miskry, A.S.A.; Hamid, A.A.M.; Darweesh, A.H.M. The Impact of COVID-19 Pandemic on University Faculty, Staff, and Students and Coping Strategies Used During the Lockdown in the United Arab Emirates. Front. Psychol. 2021, 12, 682757. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yu, W.; Wu, X.; Wan, H.; Wang, Y.; Lu, G. Psychological resilience and positive coping styles among Chinese undergraduate students: A cross-sectional study. BMC Psychol. 2020, 8, 79. [Google Scholar] [CrossRef]
- García, F.E.; Barraza-Peña, C.G.; Wlodarczyk, A.; Alvear-Carrasco, M.; Reyes-Reyes, A. Psychometric properties of the Brief-COPE for the evaluation of coping strategies in the Chilean population. Psicol. Reflexão E Crítica 2018, 31. [Google Scholar] [CrossRef] [PubMed]
- Alyami, H.; Alyami, M.; Krageloh, C.; Nemengani, D.; Henning, M. Coping strategies during the COVID-19 pandemic and compliance with precautionary health behaviors: An online study among the Saudi general population. Saudi J. Health Sci. 2021, 10, 21–26. [Google Scholar] [CrossRef]
- Hidalgo-Andrade, P.; Hermosa-Bosano, C.; Paz, C. Teachers’ mental health and self-reported coping strategies during the COVID-19 pandemic in Ecuador: A mixed-methods study. Psychol. Res. Behav. Manag. 2021, 14, 933. [Google Scholar] [CrossRef] [PubMed]
- Frimpong, J.B.; Agormedah, E.K.; Srem-Sai, M.; Quansah, F.; Hagan, J.E., Jr. Examining risk perception and coping strategies of senior high school teachers in Ghana: Does COVID-19-related knowledge matter? COVID 2022, 2, 660–673. [Google Scholar] [CrossRef]
- Allen, M.T. Explorations of avoidance and approach coping and perceived stress with a computer-based avatar task: Detrimental effects of resignation and withdrawal. PeerJ 2021, 9, e11265. [Google Scholar] [CrossRef]
- dos Santos Ribeiro, M.; da Silva Borges, M.; de Araújo, T.C.C.F.; dos Santos Souza, M.C. Coping strategies used by the elderly regarding aging and death: An integrative review. Rev. Bras. De Geriatr. E Gerontol. 2017, 20, 869–877. [Google Scholar] [CrossRef]
- Matud, M.P. Gender differences in stress and coping styles. Personal. Individ. Differ. 2004, 37, 1401–1415. [Google Scholar] [CrossRef]
- Graves, B.S.; Hall, M.E.; Dias-Karch, C.; Haischer, M.H.; Apter, C. Gender differences in perceived stress and coping among college students. PLoS ONE 2021, 16, e0255634. [Google Scholar] [CrossRef]
- Cappella, E.; Jackson, D.R.; Bilal, C.; Hamre, B.K.; Soulé, C. Bridging mental health and education in urban elementary schools: Participatory research to inform intervention development. Sch. Psychol. Rev. 2011, 40, 486–508. [Google Scholar] [CrossRef]
- Nastasi, B.K.; Sarkar, S.; Varjas, K.; Jayasena, A. Participatory model of mental health programming: Lessons learned from work in a developing country. Sch. Psychol. Rev. 1998, 27, 260–276. [Google Scholar] [CrossRef]
- Carr, E.; Davis, K.; Bergin-Cartwright, G.; Lavelle, G.; Leightley, D.; Oetzmann, C.; Polling, C.; Stevelink, S.A.M.; Wickersham, A.; Razavi, R. Mental health among UK university staff and postgraduate students in the early stages of the COVID-19 pandemic. Occup. Environ. Med. 2022, 79, 259–267. [Google Scholar] [CrossRef]
- Desouky, D.; Allam, H. Occupational stress, anxiety and depression among Egyptian teachers. J. Epidemiol. Glob. Health 2017, 7, 191–198. [Google Scholar] [CrossRef]
- Agyapong, B.; Obuobi-Donkor, G.; Burback, L.; Wei, Y. Stress, burnout, anxiety and depression among teachers: A scoping review. Int. J. Environ. Res. Public Health 2022, 19, 10706. [Google Scholar] [CrossRef] [PubMed]
- Al-Gelban, K.S. Psychiatric morbidity among Saudi secondary schoolteachers. Neurosci. J. 2008, 13, 288–290. [Google Scholar]
- Kidger, J.; Brockman, R.; Tilling, K.; Campbell, R.; Ford, T.; Araya, R.; King, M.; Gunnell, D. Teachers’ wellbeing and depressive symptoms, and associated risk factors: A large cross sectional study in English secondary schools. J. Affect. Disord. 2016, 192, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Is burnout a depressive disorder? A reexamination with special focus on atypical depression. Int. J. Stress Manag. 2014, 21, 307. [Google Scholar] [CrossRef]
- Hamatani, S.; Hiraoka, D.; Makita, K.; Tomoda, A.; Mizuno, Y. Longitudinal impact of COVID-19 pandemic on mental health of children in the ABCD study cohort. Sci. Rep. 2022, 12, 19601. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2022, 52, 2549–2558. [Google Scholar] [CrossRef]
- Foster, S.; Estévez-Lamorte, N.; Walitza, S.; Mohler-Kuo, M. The Impact of the COVID-19 Pandemic on Young Adults’ Mental Health in Switzerland: A Longitudinal Cohort Study from 2018 to 2021. Int. J. Environ. Res. Public Health 2023, 20, 2598. [Google Scholar] [CrossRef] [PubMed]
- Votruba, N.; Thornicroft, G.; FundaMental, S.D.G.S.G. Sustainable development goals and mental health: Learnings from the contribution of the FundaMentalSDG global initiative. Glob. Ment. Health 2016, 3, e26. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Mondragon, N.I.; Santamaría, M.D.; Gorrotxategi, M.P. Psychological symptoms during the two stages of lockdown in response to the COVID-19 outbreak: An investigation in a sample of citizens in Northern Spain. Front. Psychol. 2020, 11, 1491. [Google Scholar] [CrossRef] [PubMed]
- Vadivel, R.; Shoib, S.; El Halabi, S.; El Hayek, S.; Essam, L.; Bytyçi, D.G.; Karaliuniene, R.; Teixeira, A.L.S.; Nagendrappa, S.; Ramalho, R. Mental health in the post-COVID-19 era: Challenges and the way forward. Gen. Psychiatry 2021, 34, e100424. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall | Mean Rank | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Anxiety Symptoms Score | Sig. | Effect Size (r/є2) | Depressive Symptoms Score | Sig. | Effect Size (r/є2) | PTSD Symptoms Score | Sig. | Effect Size (r/є2) | ||
| Age (Median 36, IQR 15) | 0.045 * | 0.012 | 0.032 * | 0.014 | 0.206 | 0.006 | ||||
| ≤30 years | 159 (31.7) | 266.46 | 269.15 | 249.20 | ||||||
| 31–50 years | 301 (60.0) | 239.06 | 238.03 | 247.46 | ||||||
| >50 years | 42 (8.4) | 284.04 | 281.24 | 289.15 | ||||||
| Gender | <0.001 * | −0.236 | <0.001 * | −0.247 | <0.001 * | −0.187 | ||||
| Male | 333 (66.3) | 227.38 | 226.02 | 232.32 | ||||||
| Female | 169 (33.7) | 299.02 | 301.16 | 289.29 | ||||||
| Education | 0.121 | 0.012 | 0.381 | 0.006 | 0.015 * | 0.021 | ||||
| Bachelor | 178 (35.5) | 243.10 | 241.65 | 235.44 | ||||||
| Master | 72 (14.3) | 288.89 | 276.53 | 265.51 | ||||||
| PhD | 199 (39.6) | 246.16 | 252.08 | 271.08 | ||||||
| Other | 53 (10.6) | 248.99 | 248.38 | 212.88 | ||||||
| Experience (median 5, IQR 7) years) | <0.001 * | 0.031 | <0.001 * | 0.044 | <0.001 * | 0.036 | ||||
| ≤5 years | 271 (54.0) | 273.79 | 277.12 | 276.13 | ||||||
| 6–10 years | 140 (27.9) | 233.03 | 235.28 | 229.85 | ||||||
| >10 years | 91 (18.1) | 213.54 | 200.16 | 211.46 | ||||||
| Location | 0.732 | 0.001 | 0.661 | 0.002 | 0.831 | 0.001 | ||||
| Sakaka | 361 (71.9) | 250.02 | 248.59 | 250.59 | ||||||
| Qurryat | 86 (17.1) | 248.58 | 253.69 | 248.37 | ||||||
| Tabarjal | 55 (11.0) | 265.80 | 267.18 | 262.38 | ||||||
| Family member or relative got COVID-19 | 0.759 | −0.013 | 0.480 | −0.032 | 0.231 | −0.054 | ||||
| Yes | 465 (92.6) | 252.05 | 252.77 | 253.67 | ||||||
| No | 37 (7.4) | 244.54 | 244.54 | 224.22 | ||||||
| Infected with COVID-19? | 0.036 * | −0.094 | 0.147 | −0.065 | 0.192 | −0.058 | ||||
| Yes | 265 (52.8) | 264.19 | 260.27 | 259.43 | ||||||
| No | 237 (47.2) | 237.31 | 241.69 | 242.63 | ||||||
| Sample 1—Sample 2 | Anxiety | Depression | PTSD | |||
|---|---|---|---|---|---|---|
| Sig. | Adjusted Sig. # | Sig. | Adjusted Sig. # | Sig. | Adjusted Sig. # | |
| Age (years) | ||||||
| ≤30–31–50 | 0.051 | 0.153 | 0.027 | 0.080 | -- | -- |
| ≤30–>50 | 0.479 | 1.000 | 0.627 | 1.000 | -- | -- |
| 31–50–>50 | 0.056 | 0.169 | 0.067 | 0.201 | -- | -- |
| Education | ||||||
| Bachelor—master | -- | -- | -- | -- | 0.135 | 0.807 |
| Bachelor—PhD | -- | -- | -- | -- | 0.016 | 0.098 |
| Bachelor—other | -- | -- | -- | -- | 0.316 | 1.000 |
| Master—PhD | -- | -- | -- | -- | 0.779 | 1.000 |
| Master—other | -- | -- | -- | -- | 0.043 | 0.259 |
| PhD—other | -- | -- | -- | -- | 0.009 | 0.053 |
| Experience (years) | ||||||
| ≤5–6–10 | 0.006 | 0.019 * | 0.005 | 0.015 * | 0.002 | 0.006 * |
| ≤5–>10 | 0.001 | 0.002 * | <0.001 | <0.001 * | <0.001 | <0.001 * |
| 6–10–>10 | 0.312 | 0.936 | 0.069 | 0.206 | 0.342 | 1.000 |
| Variables | Academic Staff (N = 299) | Non-Academic Staff (N = 203) | Sig. | Effect Size (r) | ||
|---|---|---|---|---|---|---|
| Median (IQR) | Mean Rank | Median (IQR) | Mean Rank | |||
| Psychological impairment | ||||||
| Anxiety symptoms score | 7 (0, 10) | 260.78 | 5 (0, 9) | 237.83 | 0.078 | −0.079 |
| Depression symptoms score | 9 (0, 13) | 260.21 | 7 (0, 12) | 238.67 | 0.098 | −0.074 |
| PTSD symptoms score | 22 (4, 37) | 265.92 | 17 (0, 30) | 230.27 | 0.006 * | −0.122 |
| Major Brief-COPE domains | ||||||
| Avoidant coping | 24 (16, 29) | 266.40 | 21 (15, 26) | 229.56 | 0.005 * | −0.125 |
| Approach coping | 25 (18, 30) | 262.40 | 24 (15, 29) | 235.44 | 0.041 * | −0.091 |
| Coping methods | ||||||
| Self-distraction | 4 (3, 5) | 254.54 | 4 (3, 5) | 247.02 | 0.561 | −0.026 |
| Active coping | 4 (3, 5) | 259.96 | 4 (3, 5) | 239.03 | 0.105 | −0.072 |
| Denial | 4 (2, 5) | 263.09 | 3 (2, 5) | 234.43 | 0.025 * | −0.100 |
| Substance use | 4 (2, 5) | 267.37 | 2 (2, 4) | 228.12 | 0.002 * | −0.139 |
| Emotional support | 4 (2, 5) | 259.65 | 4 (2, 5) | 239.49 | 0.116 | −0.070 |
| Instrumental support | 4 (2, 5) | 259.78 | 4 (2, 5) | 239.31 | 0.112 | −0.071 |
| Behavioural disengagement | 4 (2, 5) | 265.65 | 3 (2, 5) | 231.59 | 0.009 * | −0.117 |
| Venting | 4 (2, 5) | 262.54 | 4 (2, 5) | 235.25 | 0.033 * | −0.094 |
| Positive reframing | 4 (2, 5) | 259.19 | 4 (2, 5) | 240.18 | 0.139 | −0.066 |
| Planning | 4 (2, 5) | 258.59 | 4 (2, 5) | 241.06 | 0.174 | −0.061 |
| Humour | 4 (2, 5) | 261.19 | 4 (2, 5) | 237.23 | 0.062 | −0.083 |
| Acceptance | 4 (3, 5) | 260.05 | 4 (2, 5) | 238.90 | 0.101 | −0.073 |
| Religion | 4 (3, 5) | 254.12 | 4 (2, 6) | 247.64 | 0.616 | −0.022 |
| Self-blame | 4 (2, 5) | 260.71 | 4 (2, 5) | 237.93 | 0.076 | −0.079 |
| Coping Strategies | Overall | Mean Rank | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (IQR) | Anxiety | Without Anxiety | Sig. # | Effect Size | Depression | Without Depression | Sig. # | Effect Size | PTSD | Without PTSD | Sig. # | Effect Size | |
| Self-distraction | 4.00 ± 1.48 | 4 (3, 5) | 298.74 | 236.50 | <0.001 * | −0.188 | 272.44 | 237.63 | 0.007 * | −0.120 | 295.22 | 234.76 | <0.001 * | −0.191 |
| Active coping | 4.34 ± 1.54 | 4 (3, 5) | 287.30 | 240.13 | 0.001 * | −0.142 | 284.21 | 229.84 | <0.001 * | −0.187 | 320.47 | 225.09 | <0.001 * | −0.300 |
| Denial | 3.76 ± 1.65 | 4 (2, 5) | 334.13 | 225.26 | <0.001 * | −0.330 | 321.96 | 204.84 | <0.001 * | −0.407 | 351.14 | 213.35 | <0.001 * | −0.437 |
| Substance use | 3.53 ± 1.64 | 3 (2, 5) | 334.81 | 225.04 | <0.001 * | 0.340 | 314.00 | 210.11 | <0.001 * | −0.368 | 331.43 | 220.89 | <0.001 * | −0.358 |
| Emotional support | 3.77 ± 1.62 | 4 (2, 5) | 331.47 | 226.10 | <0.001 * | −0.319 | 321.87 | 204.90 | <0.001 * | −0.405 | 338.60 | 218.15 | <0.001 * | −0.382 |
| Instrumental support | 3.89 ± 1.68 | 4 (2, 5) | 330.86 | 226.30 | <0.001 * | −0.316 | 315.84 | 208.89 | <0.001 * | −0.370 | 339.52 | 217.80 | <0.001 * | −0.385 |
| Behavioural disengagement | 3.76 ± 1.63 | 4 (2, 5) | 334.60 | 225.11 | <0.001 * | −0.330 | 330.23 | 199.36 | <0.001 * | −0.456 | 350.79 | 213.48 | <0.001 * | −0.437 |
| Venting | 3.84 ± 1.65 | 4 (2, 5) | 336.61 | 224.47 | <0.001 * | −0.340 | 327.64 | 201.08 | <0.001 * | −0.439 | 354.76 | 211.96 | <0.001 * | −0.453 |
| Positive reframing | 3.96 ± 1.72 | 4 (2, 5) | 336.71 | 224.76 | <0.001 * | −0.336 | 320.38 | 205.88 | <0.001 * | −0.397 | 345.56 | 215.48 | <0.001 * | −0.412 |
| Planning | 3.97 ± 1.61 | 4 (2, 5) | 340.96 | 223.09 | <0.001 * | −0.356 | 317.98 | 207.47 | <0.001 * | −0.382 | 352.33 | 212.89 | <0.001 * | −0.440 |
| Humour | 3.83 ± 1.57 | 4 (2, 5) | 332.23 | 225.86 | <0.001 * | −0.322 | 323.78 | 203.63 | <0.001 * | −0.416 | 341.45 | 217.06 | <0.001 * | −0.394 |
| Acceptance | 4.15 ± 1.79 | 4 (2, 5) | 307.60 | 233.69 | <0.001 * | −0.223 | 299.85 | 219.48 | <0.001 * | −0.277 | 327.06 | 222.57 | <0.001 * | −0.330 |
| Religion | 4.20 ± 1.79 | 4 (2, 5) | 324.22 | 228.41 | <0.001 * | −0.288 | 311.04 | 212.07 | <0.001 * | −0.341 | 342.12 | 216.80 | <0.001 * | −0.394 |
| Self-blame | 3.80 ± 1.62 | 4 (2, 5) | 334.01 | 225.30 | <0.001 * | −0.330 | 328.03 | 200.82 | <0.001 * | −0.441 | 358.19 | 210.65 | <0.001 * | −0.468 |
| Variables | Avoidant Coping | Approach Coping | ||||
|---|---|---|---|---|---|---|
| Mean Rank | Sig. | Effect Size (r/є2) | Mean Rank | Sig. | Effect Size (r/є2) | |
| Age | 0.016 * | 0.017 | 0.155 | 0.007 | ||
| ≤30 years | 236.73 | 240.35 | ||||
| 31–50 years | 251.27 | 252.19 | ||||
| >50 years | 309.08 | 288.75 | ||||
| Gender | <0.001 * | −0.175 | <0.001 * | −0.164 | ||
| Male | 233.41 | 234.63 | ||||
| Female | 287.15 | 284.15 | ||||
| Education | 0.244 | 0.008 | 0.177 | 0.010 | ||
| Bachelor | 234.33 | 232.83 | ||||
| Master | 262.37 | 263.31 | ||||
| PhD | 262.98 | 264.04 | ||||
| Other | 251.26 | 251.11 | ||||
| Experience | 0.039 * | 0.013 | 0.003 * | 0.023 | ||
| ≤5 years | 263.77 | 271.24 | ||||
| 6–10 years | 248.59 | 233.33 | ||||
| >10 years | 219.45 | 220.65 | ||||
| Location | 0.986 | 0.000 | 0.606 | 0.002 | ||
| Sakaka | 251.94 | 254.66 | ||||
| Qurryat | 249.15 | 249.49 | ||||
| Tabarjal | 252.30 | 233.88 | ||||
| Family member got COVID-19 | 0.001 * | −0.149 | 0.012 * | −0.112 | ||
| Yes | 257.60 | 256.10 | ||||
| No | 174.81 | 193.74 | ||||
| Infected with COVID-19? | 0.004 * | −0.128 | 0.159 | −0.063 | ||
| Yes | 269.06 | 260.10 | ||||
| No | 231.86 | 241.88 | ||||
| Sample 1—Sample 2 | Avoidant Coping | Approach Coping | ||
|---|---|---|---|---|
| Sig. | Adjusted Sig. # | Sig. | Adjusted Sig. # | |
| Age (years) | ||||
| ≤30–31–50 | 0.306 | 0.917 | -- | -- |
| ≤30–>50 | 0.004 * | 0.012 * | -- | -- |
| 31–50–>50 | 0.015 * | 0.046 * | -- | -- |
| Experience (years) | ||||
| ≤5–6–10 | 0.314 | 0.941 | 0.012 * | 0.036 * |
| ≤5–>10 | 0.011 * | 0.034 * | 0.004 * | 0.012 * |
| 6–10–>10 | 0.135 | 0.404 | 0.516 | 1.000 |
| Spearman’s Rho | Anxiety | Depression | PTSD | SD | AC | D | SU | ES | IS | BD | V | PR | P | H | A | R | SB |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anxiety | 1.000 | ||||||||||||||||
| Depression | 0.844 | 1.000 | |||||||||||||||
| PTSD | 0.650 | 0.676 | 1.000 | ||||||||||||||
| SD | 0.158 | 0.165 | 0.235 | 1.000 | |||||||||||||
| AC | 0.215 | 0.227 | 0.373 | 0.608 | 1.000 | ||||||||||||
| D | 0.521 | 0.534 | 0.630 | 0.345 | 0.405 | 1.000 | |||||||||||
| SU | 0.485 | 0.495 | 0.564 | 0.241 | 0.347 | 0.703 | 1.000 | ||||||||||
| ES | 0.495 | 0.511 | 0.567 | 0.437 | 0.513 | 0.665 | 0.611 | 1.000 | |||||||||
| IS | 0.489 | 0.484 | 0.570 | 0.407 | 0.508 | 0.636 | 0.595 | 0.692 | 1.000 | ||||||||
| BD | 0.519 | 0.561 | 0.628 | 0.350 | 0.440 | 0.749 | 0.680 | 0.722 | 0.679 | 1.000 | |||||||
| V | 0.533 | 0.562 | 0.647 | 0.392 | 0.476 | 0.723 | 0.692 | 0.718 | 0.708 | 0.716 | 1.000 | ||||||
| PR | 0.505 | 0.527 | 0.621 | 0.413 | 0.477 | 0.667 | 0.605 | 0.710 | 0.703 | 0.721 | 0.738 | 1.000 | |||||
| P | 0.518 | 0.495 | 0.634 | 0.416 | 0.527 | 0.628 | 0.533 | 0.681 | 0.703 | 0.663 | 0.684 | 0.759 | 1.000 | ||||
| H | 0.476 | 0.515 | 0.582 | 0.364 | 0.421 | 0.609 | 0.624 | 0.603 | 0.650 | 0.680 | 0.695 | 0.674 | 0.639 | 1.000 | |||
| A | 0.361 | 0.377 | 0.489 | 0.448 | 0.506 | 0.462 | 0.395 | 0.539 | 0.595 | 0.509 | 0.567 | 0.639 | 0.681 | 0.595 | 1.000 | ||
| R | 0.451 | 0.459 | 0.564 | 0.433 | 0.495 | 0.519 | 0.413 | 0.579 | 0.678 | 0.582 | 0.617 | 0.705 | 0.763 | 0.605 | 0.741 | 1.000 | |
| SB | 0.509 | 0.541 | 0.616 | 0.420 | 0.466 | 0.661 | 0.599 | 0.662 | 0.656 | 0.676 | 0.724 | 0.682 | 0.694 | 0.714 | 0.605 | 0.625 | 1.000 |
| Model | Unstandardized Coefficients | Standardized Coefficients | 95% CI for B | Sig. | ||
|---|---|---|---|---|---|---|
| B | SE | Beta | Lower Bound | Upper Bound | ||
| Regression model for probable anxiety | ||||||
| Self-distraction | −0.142 | 0.173 | −0.040 | −0.482 | 0.197 | 0.411 |
| Active coping | −0.472 | 0.176 | −0.138 | −0.818 | −0.127 | 0.007 * |
| Denial | 0.447 | 0.190 | 0.140 | 0.074 | 0.820 | 0.019 * |
| Substance use | 0.291 | 0.178 | 0.091 | −0.058 | 0.640 | 0.102 |
| Emotional support | 0.200 | 0.198 | 0.061 | −0.190 | 0.589 | 0.315 |
| Instrumental support | 0.105 | 0.191 | 0.033 | −0.270 | 0.479 | 0.584 |
| Behavioural disengagement | 0.253 | 0.207 | 0.078 | −0.153 | 0.660 | 0.222 |
| Venting | 0.289 | 0.212 | 0.090 | −0.128 | 0.706 | 0.174 |
| Positive reframing | −0.039 | 0.198 | −0.013 | −0.427 | 0.349 | 0.844 |
| Planning | 0.374 | 0.224 | 0.115 | −0.065 | 0.814 | 0.095 |
| Humour | 0.200 | 0.196 | 0.060 | −0.185 | 0.585 | 0.307 |
| Acceptance | −0.276 | 0.170 | −0.093 | −0.609 | 0.058 | 0.105 |
| Religion | 0.476 | 0.188 | 0.162 | 0.107 | 0.845 | 0.012 * |
| Self-blame | 0.364 | 0.197 | 0.112 | −0.024 | 0.752 | 0.066 |
| Regression model for probable depression | ||||||
| Self-distraction | −0.346 | 0.227 | −0.072 | −0.791 | 0.100 | 0.128 |
| Active coping | −0.408 | 0.230 | −0.089 | −0.861 | 0.045 | 0.077 |
| Denial | 0.570 | 0.249 | 0.133 | 0.081 | 1.059 | 0.022 * |
| Substance use | 0.333 | 0.233 | 0.077 | −0.125 | 0.790 | 0.153 |
| Emotional support | 0.220 | 0.260 | 0.050 | −0.291 | 0.730 | 0.398 |
| Instrumental support | −0.091 | 0.250 | −0.021 | −0.582 | 0.401 | 0.717 |
| Behavioural disengagement | 0.547 | 0.271 | 0.126 | 0.014 | 1.080 | 0.044 * |
| Venting | 0.613 | 0.278 | 0.143 | 0.067 | 1.160 | 0.028 * |
| Positive reframing | 0.086 | 0.259 | 0.021 | −0.423 | 0.595 | 0.741 |
| Planning | −0.061 | 0.293 | −0.014 | −0.638 | 0.516 | 0.835 |
| Humour | 0.324 | 0.257 | 0.072 | −0.181 | 0.828 | 0.208 |
| Acceptance | −0.231 | 0.222 | −0.058 | −0.668 | 0.206 | 0.299 |
| Religion | 0.637 | 0.246 | 0.161 | 0.153 | 1.121 | 0.010 * |
| Self-blame | 0.695 | 0.259 | 0.159 | 0.187 | 1.203 | 0.007 * |
| Regression model for probable PTSD | ||||||
| Self-distraction | −1.426 | 0.517 | −0.117 | −2.442 | −0.409 | 0.006 * |
| Active coping | 0.571 | 0.526 | 0.049 | −0.462 | 1.605 | 0.278 |
| Denial | 1.813 | 0.568 | 0.165 | 0.697 | 2.930 | 0.002 * |
| Substance use | 0.544 | 0.532 | 0.049 | −0.500 | 1.589 | 0.306 |
| Emotional support | −0.365 | 0.593 | −0.033 | −1.531 | 0.801 | 0.538 |
| Instrumental support | −0.357 | 0.571 | −0.033 | −1.478 | 0.764 | 0.532 |
| Behavioural disengagement | 1.716 | 0.620 | 0.155 | 0.499 | 2.933 | 0.006 * |
| Venting | 1.640 | 0.635 | 0.149 | 0.392 | 2.888 | 0.010 * |
| Positive reframing | −0.297 | 0.591 | −0.028 | −1.459 | 0.865 | 0.615 |
| Planning | 2.078 | 0.670 | 0.185 | 0.761 | 3.394 | 0.002 * |
| Humour | 0.892 | 0.586 | 0.077 | −0.260 | 2.044 | 0.129 |
| Acceptance | −0.070 | 0.508 | −0.007 | −1.068 | 0.927 | 0.890 |
| Religion | 0.955 | 0.563 | 0.095 | −0.151 | 2.060 | 0.090 |
| Self-blame | 1.298 | 0.590 | 0.116 | 0.138 | 2.458 | 0.028 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mallhi, T.H.; Khan, N.A.; Siddique, A.; Salman, M.; Bukhari, S.N.A.; Butt, M.H.; Khan, F.U.; Khalid, M.; Mustafa, Z.U.; Tanveer, N.; et al. Mental Health and Coping Strategies among University Staff during the COVID-19 Pandemic: A Cross–Sectional Analysis from Saudi Arabia. Sustainability 2023, 15, 8545. https://doi.org/10.3390/su15118545
Mallhi TH, Khan NA, Siddique A, Salman M, Bukhari SNA, Butt MH, Khan FU, Khalid M, Mustafa ZU, Tanveer N, et al. Mental Health and Coping Strategies among University Staff during the COVID-19 Pandemic: A Cross–Sectional Analysis from Saudi Arabia. Sustainability. 2023; 15(11):8545. https://doi.org/10.3390/su15118545
Chicago/Turabian StyleMallhi, Tauqeer Hussain, Nimra Aslam Khan, Amina Siddique, Muhammad Salman, Syed Nasir Abbas Bukhari, Muhammad Hammad Butt, Faiz Ullah Khan, Mohammad Khalid, Zia Ul Mustafa, Nida Tanveer, and et al. 2023. "Mental Health and Coping Strategies among University Staff during the COVID-19 Pandemic: A Cross–Sectional Analysis from Saudi Arabia" Sustainability 15, no. 11: 8545. https://doi.org/10.3390/su15118545