
Impact of Full Vaccination with mRNA BNT162b2 on SARS-CoV-2 Infection: Genomic and Subgenomic Viral RNAs Detection in Nasopharyngeal Swab and Saliva of Health Care Workers

 , , , , , , and
, , , , , , and 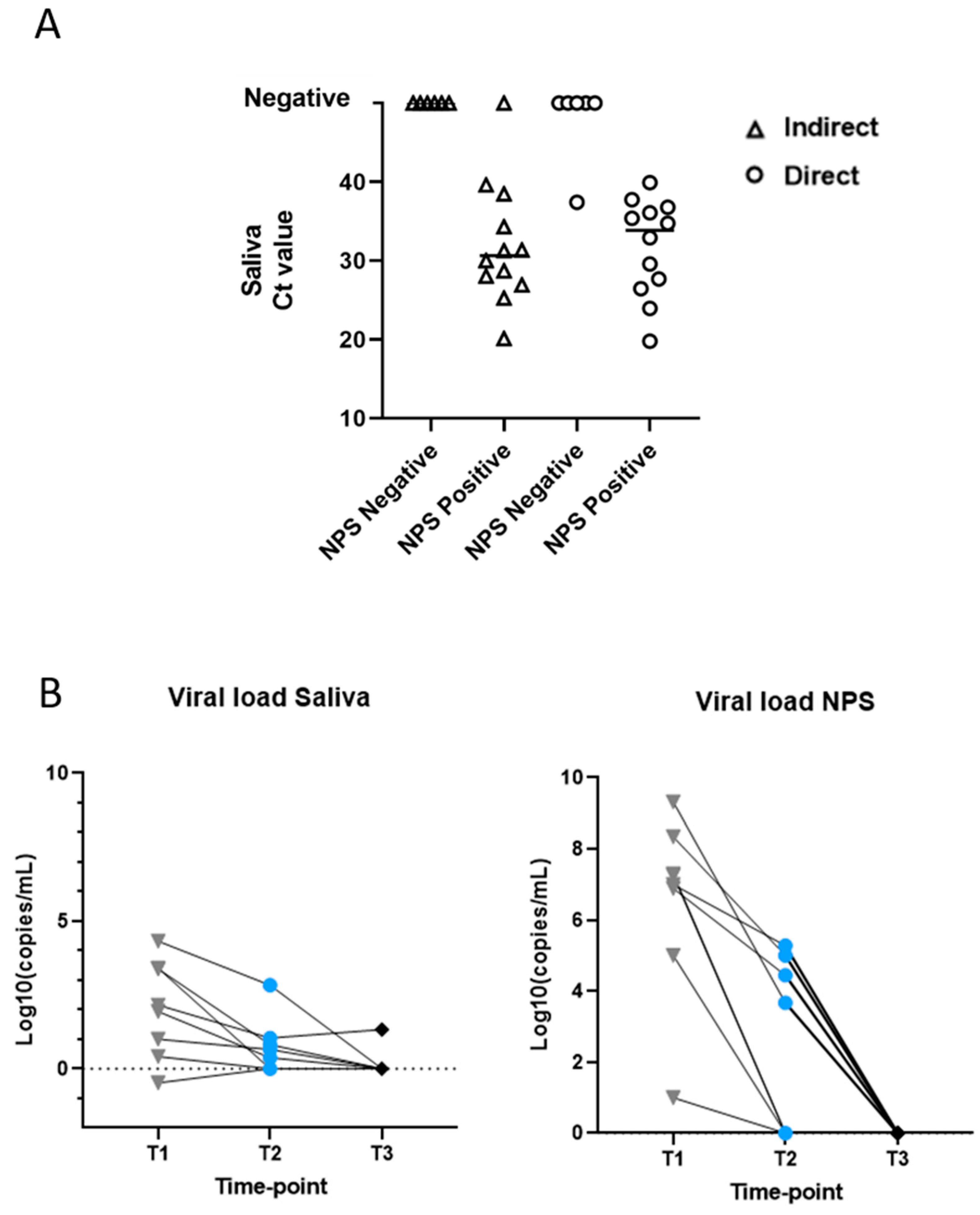{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting of Study
2.2. RNA Extraction
2.3. Reverse Transcriptase Real-Time PCR (RT-PCR)
2.4. Direct Real-Time PCR
2.5. DdPCR-One Step Reverse Transcriptase
2.6. Graphical Representations
3. Results
3.1. Setting of the Study
3.2. Genomic Viral RNA Detection
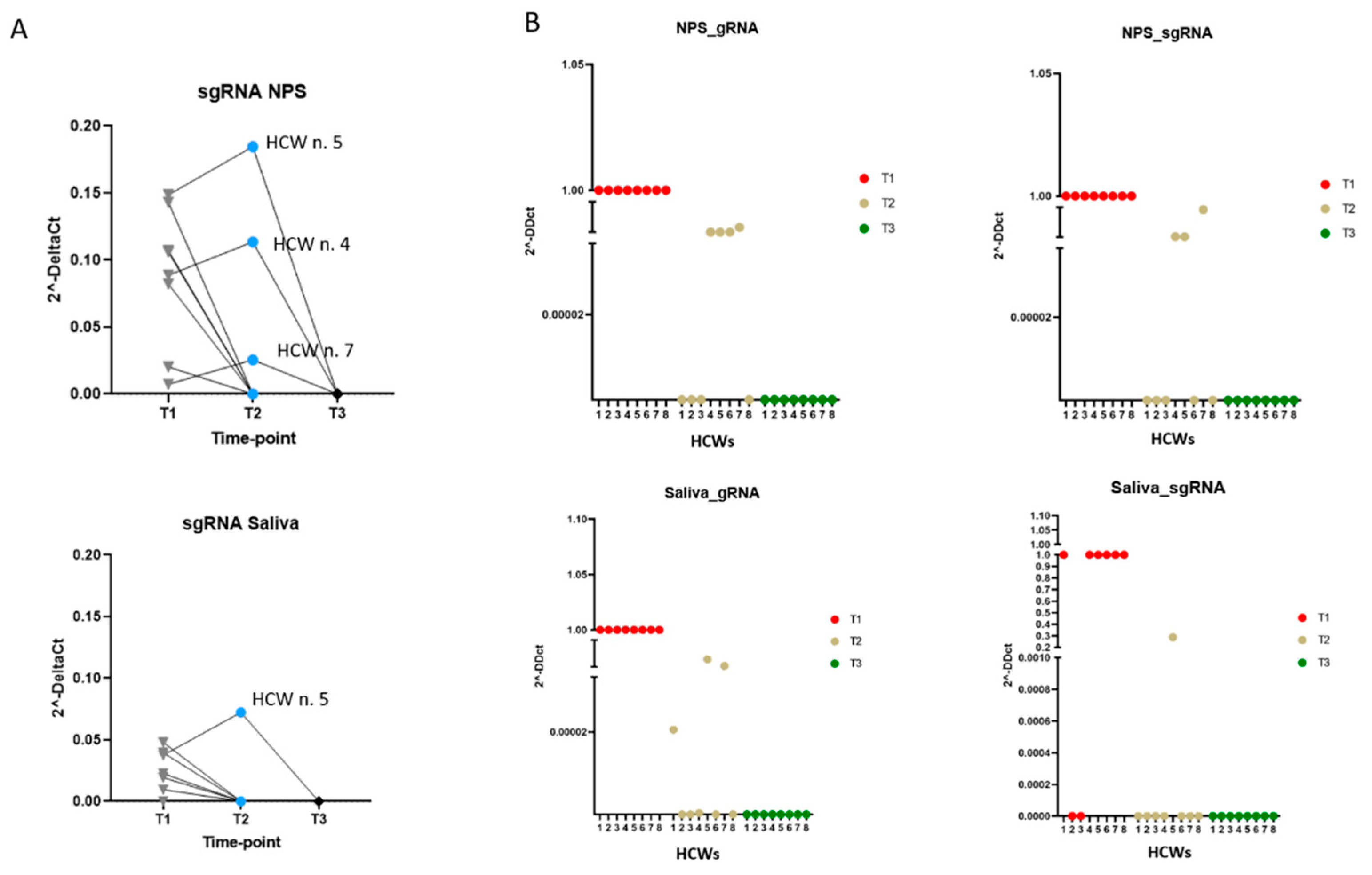
3.3. Subgenomic Viral RNA Detection
3.4. Viral Mutations Snalysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef]
- Communication from the Commission to the European Parliament and the Council. Preparedness for COVID-19 Vaccination Strategies and Vaccine Deployment. Brussels, 15.10. 2020. Available online: https://ec.europa.eu/commission/presscorner/detail/en/ip_20_1903 (accessed on 2 August 2021).
- Italian Government. Available online: https://www.governo.it/it/cscovid19/report-vaccini (accessed on 2 August 2021).
- ECDC. Risk-of-Transmission-and-Reinfection-of-SARS-CoV-2-Following-Vaccination; 2021. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Risk-of-transmission-and-reinfection-of-SARS-CoV-2-following-vaccination.pdf (accessed on 2 August 2021).
- Keehner, J.; Horton, L.E.; Pfeffer, M.A.; Longhurst, C.A.; Schooley, R.T.; Currier, J.S.; Abeles, S.R.; Torriani, F.J. SARS-CoV-2 Infection after Vaccination in Health Care Workers in California. N. Engl. J. Med. 2021, 384, 1774–1775. [Google Scholar] [CrossRef]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, M.D.; Lindsey, B.B.; Leary, S.; Gaudieri, S.; Chopra, A.; Wyles, M.; Angyal, A.; Green, L.R.; Parsons, P.; Tucker, R.M.; et al. Subgenomic RNA identification in SARS-CoV-2 genomic sequencing data. Genome Res. 2021, 31, 645–658. [Google Scholar] [CrossRef]
- Perera, R.A.P.M.; Tso, E.; Tsang, O.T.Y.; Tsang, D.N.C.; Fung, K.; Leung, Y.W.Y.; Chin, A.W.H.; Chu, D.K.W.; Cheng, S.M.S.; Poon, L.L.M.; et al. SARS-CoV-2 Virus Culture and Subgenomic RNA for Respiratory Specimens from Patients with Mild Coronavirus Disease. Emerg. Infect. Dis. 2020, 26, 2701–2704. [Google Scholar] [CrossRef]
- Wu, H.-Y.; Brian, D.A. Subgenomic messenger RNA amplification in coronaviruses. Proc. Natl. Acad. Sci. USA 2010, 107, 12257–12262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casagrande, M.; Fitzek, A.; Spitzer, M.; Püschel, K.; Glatzel, M.; Krasemann, S.; Aepfelbacher, M.; Nörz, D.; Lütgehetmann, M.; Pfefferle, S.; et al. Detection of SARS-CoV-2 genomic and subgenomic RNA in retina and optic nerve of patients with COVID-19. Br. J. Ophthalmol. 2021, 2020, 318618. [Google Scholar]
- Wong, C.H.; Ngan, C.Y.; Goldfeder, R.L.; Idol, J.; Kuhlberg, C.; Maurya, R.; Kelly, K.; Omerza, G.; Renzette, N.; De Abreu, F.; et al. Subgenomic RNAs as Molecular Indicators of Asymptomatic SARS-CoV-2 infection. bioRxiv. 2021. Available online: https://www.biorxiv.org/ (accessed on 2 August 2021).
- Sola, I.; Almazán, F.; Zúñiga, S.; Enjuanes, L. Continuous and Discontinuous RNA Synthesis in Coronaviruses. Annu. Rev. Virol. 2015, 2, 265–288. [Google Scholar] [CrossRef] [Green Version]
- Strafella, C.; Caputo, V.; Guerrera, G.; Termine, A.; Fabrizio, C.; Cascella, R.; Picozza, M.; Caltagirone, C.; Rossini, A.; Balice, M.P.; et al. Case Report: Sars-CoV-2 Infection in a Vaccinated Individual: Evaluation of the Immunological Profile and Virus Transmission Risk. Front. Immunol. 2021, 12, 708820. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Warren, J.L.; Geng, B.; Muenker, M.C.; Moore, A.J.; et al. Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 1283–1286. [Google Scholar] [CrossRef]
- Nasiri, K.; Dimitrova, A. Comparing saliva and nasopharyngeal swab specimens in the detection of COVID-19: A systematic review and meta-analysis. J. Dent. Sci. 2021, 16, 799–805. [Google Scholar] [CrossRef]
- Cañete, M.G.; Valenzuela, I.M.; Garcés, P.C.; Massó, I.C.; González, M.J.; Providell, S.G. Saliva sample for the massive screening of SARS-CoV-2 infection: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 540–548. [Google Scholar] [CrossRef]
- Ott, I.M.; Strine, M.S.; Watkins, A.E.; Boot, M.; Kalinich, C.C.; Harden, C.A.; Vogels, C.B.F.; Casanovas-Massana, A.; Moore, A.J.; Muenker, M.C.; et al. Simply Saliva: Stability of SARS-CoV-2 Detection Negates the Need for Expensive Collection Devices. medRxiv 2020. Available online: https://www.medrxiv.org/ (accessed on 2 August 2021).
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Martinelli, F.; Perrone, A.; Della Noce, I.; Colombo, L.; Lo Priore, S.; Romano, S. Application of a portable instrument for rapid and reliable detection of SARS-CoV-2 infection in any environment. Immunol. Rev. 2020, 295, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Smyrlaki, I.; Ekman, M.; Lentini, A.; Rufino de Sousa, N.; Papanicolaou, N.; Vondracek, M.; Aarum, J.; Safari, H.; Muradrasoli, S.; Rothfuchs, A.G.; et al. Massive and rapid COVID-19 testing is feasible by extraction-free SARS-CoV-2 RT-PCR. Nat. Commun. 2020, 11, 4812. [Google Scholar] [CrossRef] [PubMed]
- Deiana, M.; Mori, A.; Piubelli, C.; Scarso, S.; Favarato, M.; Pomari, E. Assessment of the direct quantitation of SARS-CoV-2 by droplet digital PCR. Sci. Rep. 2020, 10, 18764. [Google Scholar] [CrossRef] [PubMed]
- Dimcheff, D.E.; Valesano, A.L.; Rumfelt, K.E.; Fitzsimmons, W.J.; Blair, C.; Mirabelli, C.; Petrie, J.G.; Martin, E.T.; Bhambhani, C.; Tewari, M.; et al. SARS-CoV-2 Total and Subgenomic RNA Viral Load in Hospitalized Patients. J. Infect. Dis. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/33870434/ (accessed on 2 August 2021).
- Nomburg, J.; Meyerson, M.; DeCaprio, J.A. Pervasive generation of non-canonical subgenomic RNAs by SARS-CoV-2. Genome Med. 2020, 12, 108. [Google Scholar] [CrossRef]
- Zollo, M.; Ferrucci, V.; Izzo, B.; Quarantelli, F.; Di Domenico, C.; Comegna, M.; Paolillo, C.; Amato, F.; Siciliano, R.; Castaldo, G.; et al. SARS-CoV-2 Subgenomic N (sgN) Transcripts in Oro-Nasopharyngeal Swabs Correlate with the Highest Viral Load, as Evaluated by Five Different Molecular Methods. Diagnostics 2021, 11, 288. [Google Scholar] [CrossRef]
- Medeiros da Silva, R.C.; Nogueira Marinho, L.C.; de Araújo Silva, D.N.; Costa de Lima, K.; Pirih, F.Q.; Luz de Aquino Martins, A.R. Saliva as a possible tool for the SARS-CoV-2 detection: A review. Travel Med. Infect. Dis. 2020, 38, 101920. [Google Scholar] [CrossRef]
- Huang, N.; Pérez, P.; Kato, T.; Mikami, Y.; Okuda, K.; Gilmore, R.C.; Conde, C.D.; Gasmi, B.; Stein, S.; Beach, M.; et al. SARS-CoV-2 infection of the oral cavity and saliva. Nat. Med. 2021, 27, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination With BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef] [PubMed]
- Jalkanen, P.; Kolehmainen, P.; Häkkinen, H.K.; Huttunen, M.; Tähtinen, P.A.; Lundberg, R.; Maljanen, S.; Reinholm, A.; Tauriainen, S.; Pakkanen, S.H.; et al. COVID-19 mRNA vaccine induced antibody responses against three SARS-CoV-2 variants. Nat. Commun. 2021, 12, 3991. [Google Scholar] [CrossRef]
- Marot, S.; Malet, I.; Leducq, V.; Zafilaza, K.; Sterlin, D.; Planas, D.; Gothland, A.; Jary, A.; Dorgham, K.; Bruel, T.; et al. Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers. Nat. Commun. 2021, 12, 844. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.S.; O’Halloran, J.A.; Kalaidina, E.; Kim, W.; Schmitz, A.J.; Zhou, J.Q.; Lei, T.; Thapa, M.; Chen, R.E.; Case, J.B.; et al. SARS-CoV-2 mRNA vaccines induce persistent human germinal centre responses. Nature 2021, 596, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Torres, I.; Albert, E.; Giménez, E.; Alcaraz, M.J.; Botija, P.; Amat, P.; Remigia, M.J.; Beltrán, M.J.; Rodado, C.; Huntley, D.; et al. B- and T-cell Immune Responses Elicited by the Comirnaty® COVID-19 Vaccine in Nursing-Home Residents. Clin. Microbiol. Infect. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34174397/ (accessed on 2 August 2021).
- Harris, R.J.; Hall, J.A.; Zaidi, A.; Andrews, N.J.; Dunbar, J.K.; Dabrera, G. Effect of Vaccination on Household Transmission of SARS-CoV-2 in England. N. Engl. J. Med. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34161702/ (accessed on 2 August 2021).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deiana, M.; Mori, A.; Piubelli, C.; Perandin, F.; Treggiari, D.; Martini, D.; Chesini, F.; Angheben, A.; Bonfante, F.; Terregino, C.; et al. Impact of Full Vaccination with mRNA BNT162b2 on SARS-CoV-2 Infection: Genomic and Subgenomic Viral RNAs Detection in Nasopharyngeal Swab and Saliva of Health Care Workers. Microorganisms 2021, 9, 1738. https://doi.org/10.3390/microorganisms9081738
Deiana M, Mori A, Piubelli C, Perandin F, Treggiari D, Martini D, Chesini F, Angheben A, Bonfante F, Terregino C, et al. Impact of Full Vaccination with mRNA BNT162b2 on SARS-CoV-2 Infection: Genomic and Subgenomic Viral RNAs Detection in Nasopharyngeal Swab and Saliva of Health Care Workers. Microorganisms. 2021; 9(8):1738. https://doi.org/10.3390/microorganisms9081738
Chicago/Turabian StyleDeiana, Michela, Antonio Mori, Chiara Piubelli, Francesca Perandin, Davide Treggiari, Davide Martini, Fabio Chesini, Andrea Angheben, Francesco Bonfante, Calogero Terregino, and et al. 2021. "Impact of Full Vaccination with mRNA BNT162b2 on SARS-CoV-2 Infection: Genomic and Subgenomic Viral RNAs Detection in Nasopharyngeal Swab and Saliva of Health Care Workers" Microorganisms 9, no. 8: 1738. https://doi.org/10.3390/microorganisms9081738