
New Onset of Eosinophilic Granulomatosis with Polyangiitis Following mRNA-Based COVID-19 Vaccine

 , ,
, ,  , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
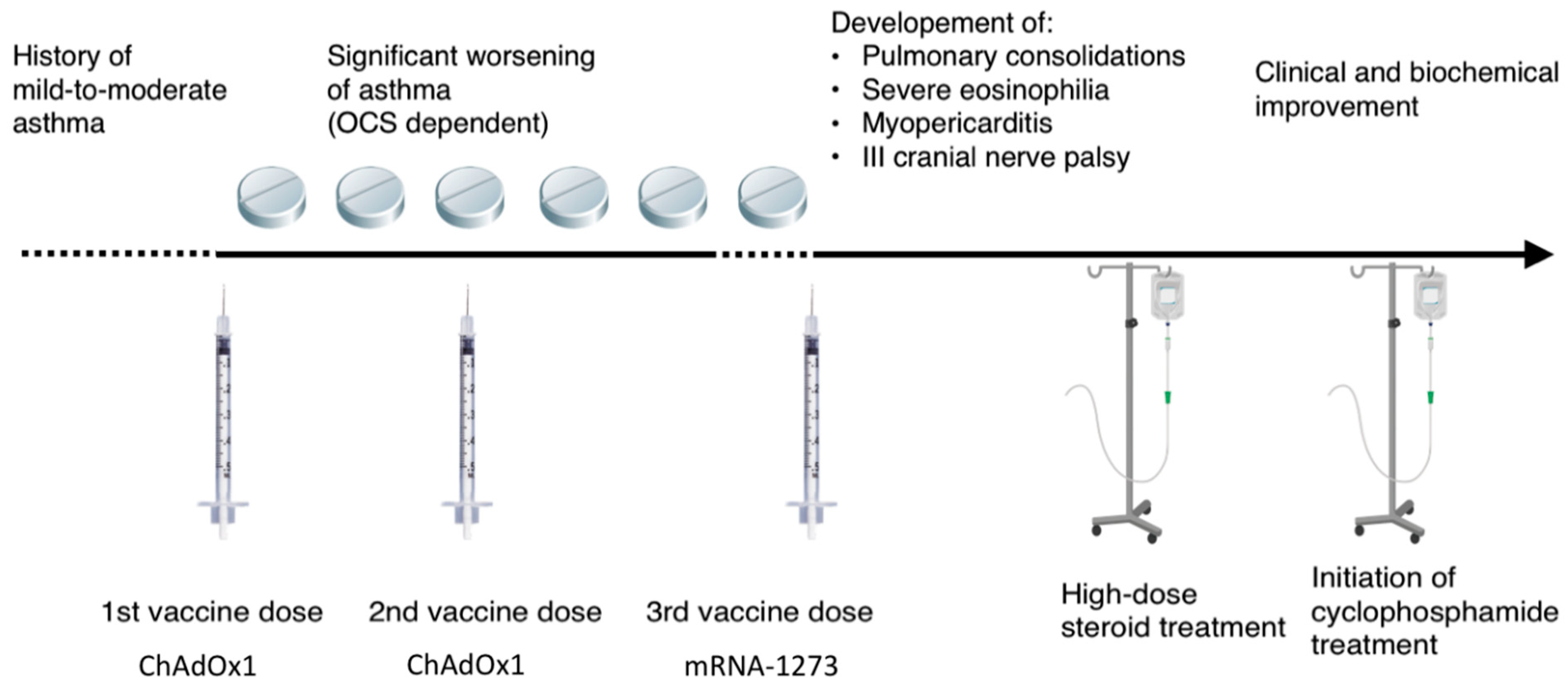
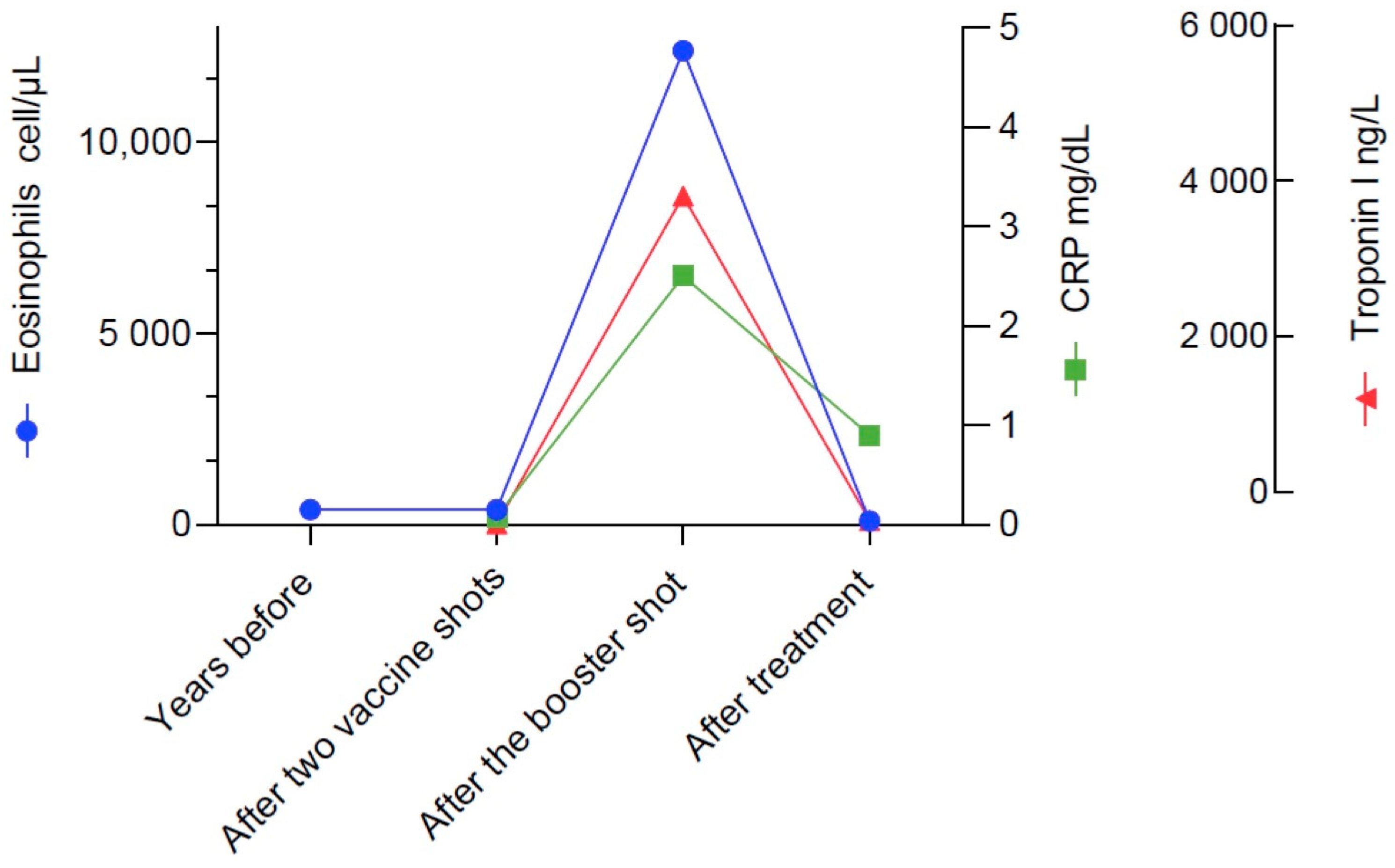
2. Case Presentation
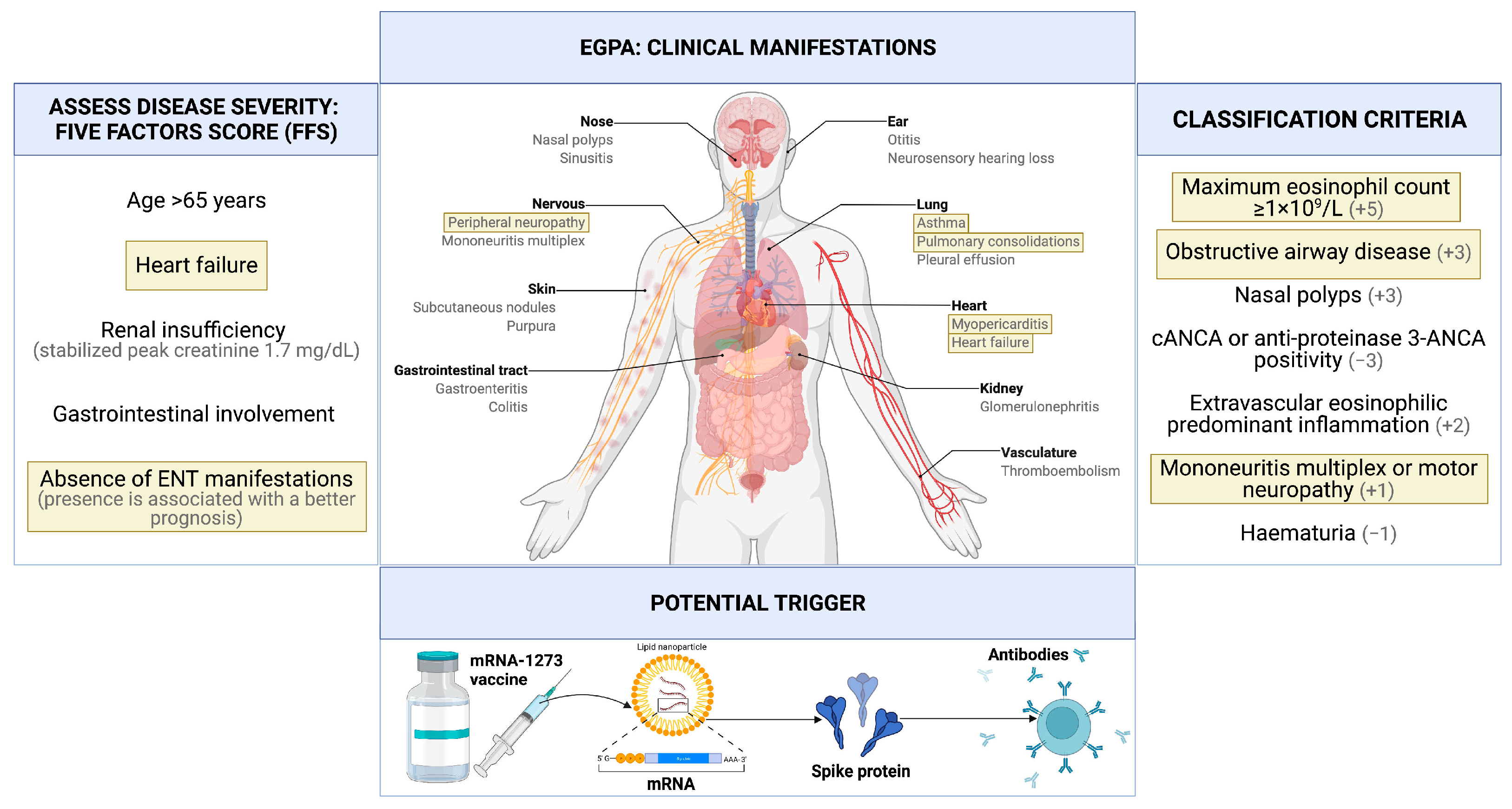
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; el Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the MRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; de Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following MRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef]
- Wu, H.H.L.; Kalra, P.A.; Chinnadurai, R. New-Onset and Relapsed Kidney Histopathology Following COVID-19 Vaccination: A Systematic Review. Vaccines 2021, 9, 1252. [Google Scholar] [CrossRef]
- Feghali, E.J.; Zafar, M.; Abid, S.; Santoriello, D.; Mehta, S. De-Novo Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Following the MRNA-1273 (Moderna) Vaccine for COVID-19. Cureus 2021, 13, e19616. [Google Scholar] [CrossRef]
- Huynh, A.; Kelton, J.G.; Arnold, D.M.; Daka, M.; Nazy, I. Antibody Epitopes in Vaccine-Induced Immune Thrombotic Thrombocytopaenia. Nature 2021, 596, 565–569. [Google Scholar] [CrossRef]
- Vadalà, M.; Poddighe, D.; Laurino, C.; Palmieri, B. Vaccination and Autoimmune Diseases: Is Prevention of Adverse Health Effects on the Horizon? EPMA J. 2017, 8, 295–311. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T. Vasculitis Following Influenza Vaccination: A Review of the Literature. Curr. Rheumatol. Rev. 2017, 13, 188–196. [Google Scholar] [CrossRef]
- Gunes, A.T.; Fetil, E.; Akarsu, S.; Ozbagcivan, O.; Babayeva, L. Possible Triggering Effect of Influenza Vaccination on Psoriasis. J. Immunol. Res. 2015, 2015, 258430. [Google Scholar] [CrossRef] [Green Version]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Grayson, P.C.; Ponte, C.; Suppiah, R.; Robson, J.C.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Luqmani, R.A.; Watts, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis With Polyangiitis. Arthritis Rheumatol. 2022, 74, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Pagnoux, C.; Seror, R.; Mahr, A.; Mouthon, L.; Toumelin, P.; Le MD for the French Vasculitis Study Group. The Five-Factor Score Revisited. Medicine 2011, 90, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Vaglio, A.; Casazza, I.; Grasselli, C.; Corradi, D.; Sinico, R.A.; Buzio, C. Churg–Strauss Syndrome. Kidney Int. 2009, 76, 1006–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boita, M.; Rolla, G.; Mallone, R.; Martinuzzi, E.; Heffler, E.; Circosta, P.; Elia, A.R.; Cignetti, A.; Caillat-Zucman, S.; de Menthon, M.; et al. Expression of NKG2D and CD107 in CD8(+) Effector Memory Lymphocytes in Churg-Strauss Syndrome. Clin. Exp. Rheumatol. 2012, 30, S57–S61. [Google Scholar] [PubMed]
- Guida, G.; Vallario, A.; Stella, S.; Boita, M.; Circosta, P.; Mariani, S.; Prato, G.; Heffler, E.; Bergia, R.; Sottile, A.; et al. Clonal CD8+ TCR-Vβ Expanded Populations with Effector Memory Phenotype in Churg Strauss Syndrome. Clin. Immunol. 2008, 128, 94–102. [Google Scholar] [CrossRef]
- Ibrahim, H.; Alkhatib, A.; Meysami, A. Eosinophilic Granulomatosis With Polyangiitis Diagnosed in an Elderly Female After the Second Dose of MRNA Vaccine Against COVID-19. Cureus 2022, 14, e21176. [Google Scholar] [CrossRef]
- Chan-Chung, C.; Ong, C.S.; Chan, L.L.; Tan, E.K. Eosinophilic Granulomatosis with Polyangiitis after COVID-19 Vaccination. QJM Int. J. Med. 2022, 114, 807–809. [Google Scholar] [CrossRef]
- Costanzo, G.; Ledda, A.G.; Ghisu, A.; Vacca, M.; Firinu, D.; del Giacco, S. Eosinophilic Granulomatosis with Polyangiitis Relapse after COVID-19 Vaccination: A Case Report. Vaccines 2021, 10, 13. [Google Scholar] [CrossRef]
- Prabhahar, A.; Naidu, G.S.R.S.N.K.; Chauhan, P.; Sekar, A.; Sharma, A.; Sharma, A.; Kumar, A.; Nada, R.; Rathi, M.; Kohli, H.S.; et al. ANCA-Associated Vasculitis Following ChAdOx1 NCoV19 Vaccination: Case-Based Review. Rheumatol. Int. 2022, 42, 749–758. [Google Scholar] [CrossRef]
- Jeffs, L.S.; Nitschke, J.; Tervaert, J.W.C.; Peh, C.A.; Hurtado, P.R. Viral RNA in the Influenza Vaccine May Have Contributed to the Development of ANCA-Associated Vasculitis in a Patient Following Immunisation. Clin. Rheumatol. 2016, 35, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Novelli, L.; Motta, F.; de Santis, M.; Ansari, A.A.; Gershwin, M.E.; Selmi, C. The JANUS of Chronic Inflammatory and Autoimmune Diseases Onset during COVID-19—A Systematic Review of the Literature. J. Autoimmun. 2021, 117, 102592. [Google Scholar] [CrossRef] [PubMed]
- Jolly, U.S.; Shih, A.; Moist, L.; Clark, W.; Gabril, M. Influenza A H1N1, Microscopic Polyangiitis and Pulmonary Haemorrhage. Nephrology 2010, 15, 781. [Google Scholar] [CrossRef]
- Frantzeskaki, F.G.; Dimopoulos, S.; Konstantonis, D.; Katsibri, P.; Kostopanagiotou, K.; Theodorakopoulou, M.; Diakaki, C.; Dougenis, D.; Boumpas, D.; Karabinis, A.; et al. Life-Threatening Antineutrophil Cytoplasmic Antibody-Associated Vasculitis after Influenza A H1N1 Infection Requiring Veno-Venous Extracorporeal Membrane Oxygenation. Perfusion 2020, 35, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, G.; Kaliamurthi, S.; Peslherbe, G.H.; Wei, D.Q. Are the Allergic Reactions of COVID-19 Vaccines Caused by mRNA Constructs or Nanocarriers? Immunological Insights. Interdiscip. Sci. 2021, 13, 344–347. [Google Scholar] [CrossRef]
- Kronbichler, A.; Geetha, D.; Smith, R.M.; Egan, A.C.; Bajema, I.M.; Schönermarck, U.; Mahr, A.; Anders, H.-J.; Bruchfeld, A.; Cid, M.C.; et al. The COVID-19 Pandemic and ANCA-Associated Vasculitis—Reports from the EUVAS Meeting and EUVAS Education Forum. Autoimmun. Rev. 2021, 20, 102986. [Google Scholar] [CrossRef]
- Heffler, E.; Detoraki, A.; Contoli, M.; Papi, A.; Paoletti, G.; Malipiero, G.; Brussino, L.; Crimi, C.; Morrone, D.; Padovani, M.; et al. COVID-19 in Severe Asthma Network in Italy (SANI) Patients: Clinical Features, Impact of Comorbidities and Treatments. Allergy 2021, 76, 887–892. [Google Scholar] [CrossRef]
- Lombardi, C.; Gani, F.; Berti, A.; Comberiati, P.; Peroni, D.; Cottini, M. Asthma and COVID-19: A Dangerous Liaison? Asthma Res. Pract. 2021, 7, 9. [Google Scholar] [CrossRef]
- Dolby, T.; Nafilyan, V.; Morgan, A.; Kallis, C.; Sheikh, A.; Quint, J.K. Relationship between Asthma and Severe COVID-19: A National Cohort Study. Thorax 2022, thoraxjnl-2021-218629. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappi, E.; De Santis, M.; Paoletti, G.; Pelaia, C.; Terenghi, F.; Pini, D.; Ciccarelli, M.; Selmi, C.F.; Puggioni, F.; Canonica, G.W.; et al. New Onset of Eosinophilic Granulomatosis with Polyangiitis Following mRNA-Based COVID-19 Vaccine. Vaccines 2022, 10, 716. https://doi.org/10.3390/vaccines10050716
Nappi E, De Santis M, Paoletti G, Pelaia C, Terenghi F, Pini D, Ciccarelli M, Selmi CF, Puggioni F, Canonica GW, et al. New Onset of Eosinophilic Granulomatosis with Polyangiitis Following mRNA-Based COVID-19 Vaccine. Vaccines. 2022; 10(5):716. https://doi.org/10.3390/vaccines10050716
Chicago/Turabian StyleNappi, Emanuele, Maria De Santis, Giovanni Paoletti, Corrado Pelaia, Fabrizia Terenghi, Daniela Pini, Michele Ciccarelli, Carlo Francesco Selmi, Francesca Puggioni, Giorgio Walter Canonica, and et al. 2022. "New Onset of Eosinophilic Granulomatosis with Polyangiitis Following mRNA-Based COVID-19 Vaccine" Vaccines 10, no. 5: 716. https://doi.org/10.3390/vaccines10050716