
The Effect of Coronavirus 2019 Disease Control Measures on the Incidence of Respiratory Infectious Disease and Air Pollutant Concentrations in the Yangtze River Delta Region, China

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Data Collection (Eight RIDs)
2.3. Data Collection (Air Pollutants)
2.4. Case Definitions
2.5. Statistical Analysis
3. Results
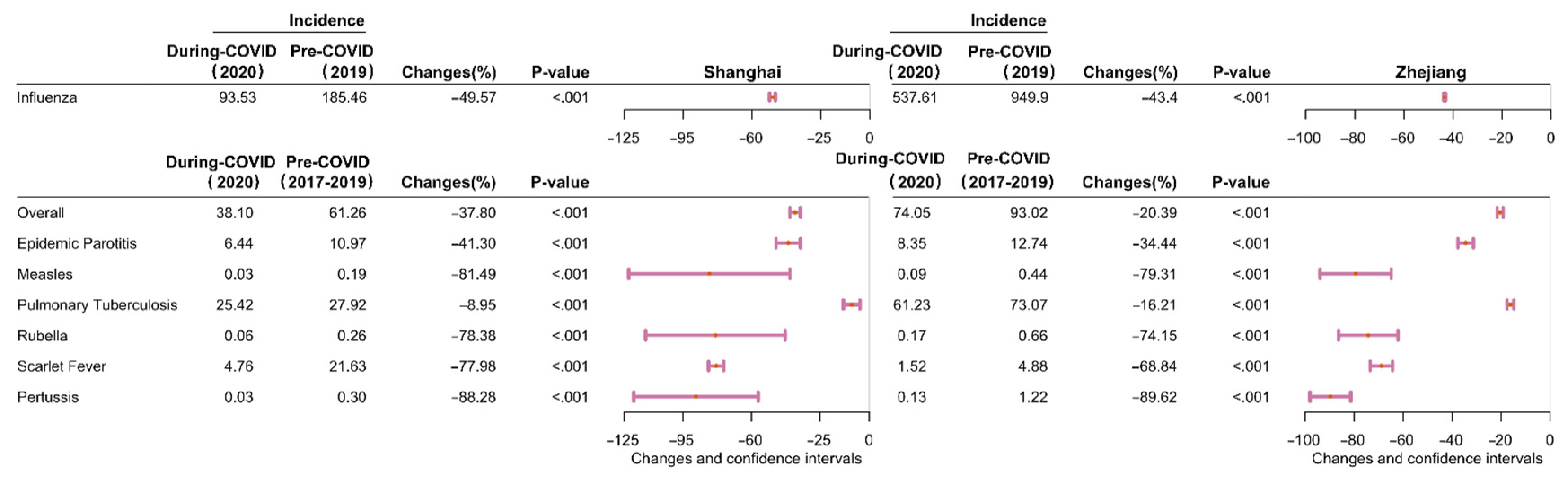
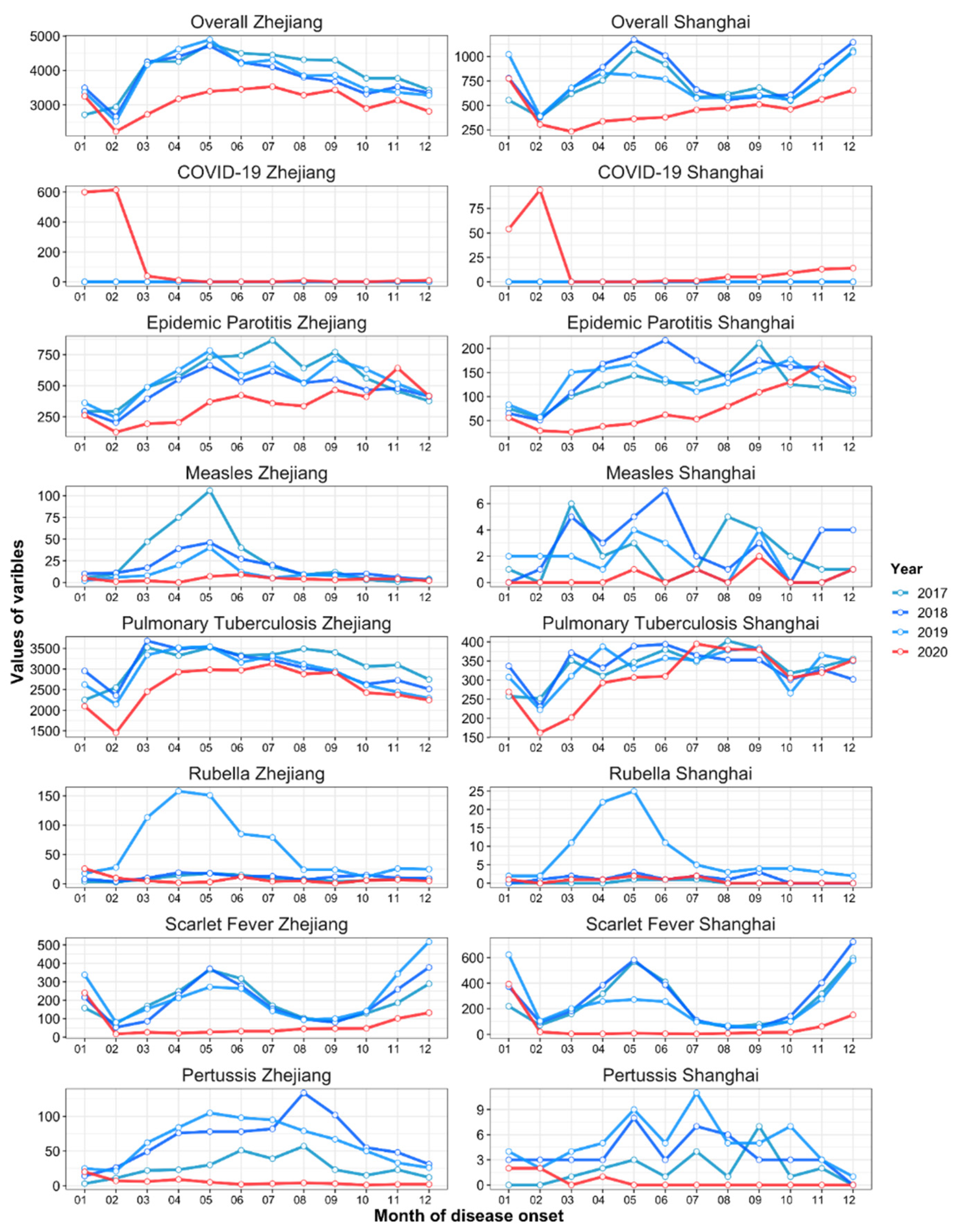
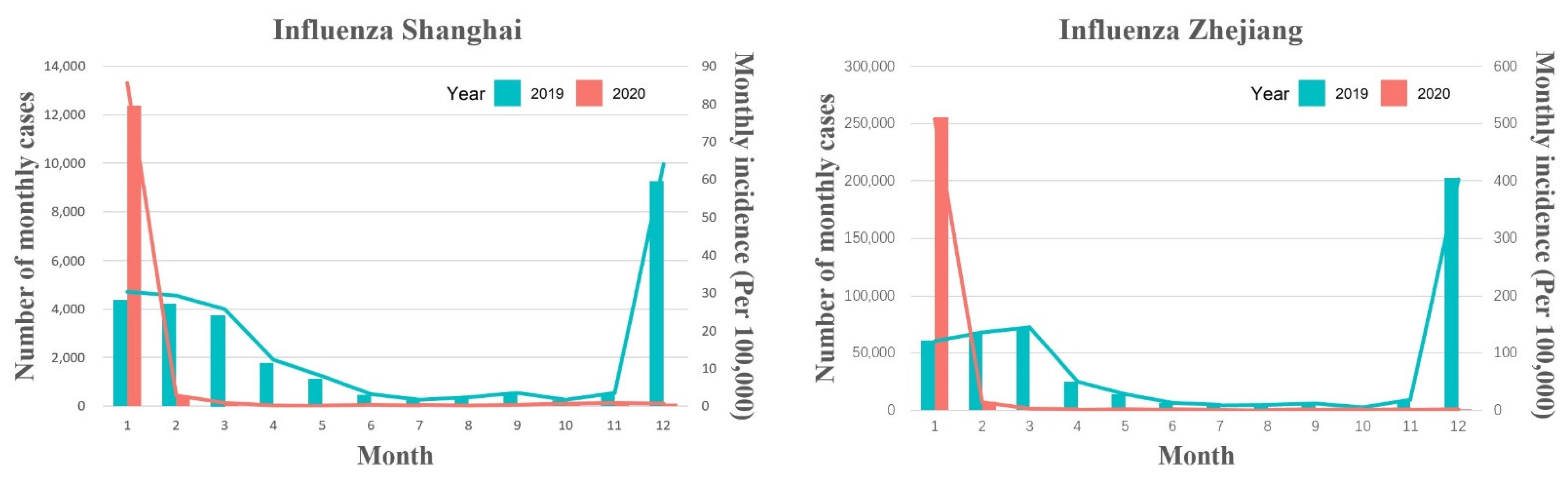
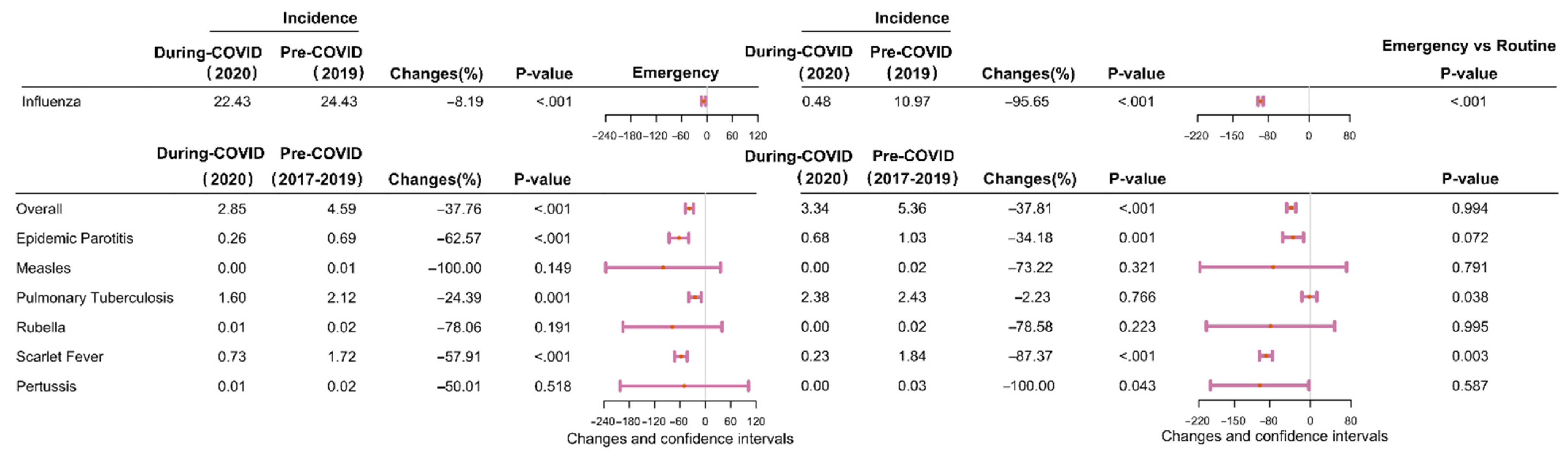
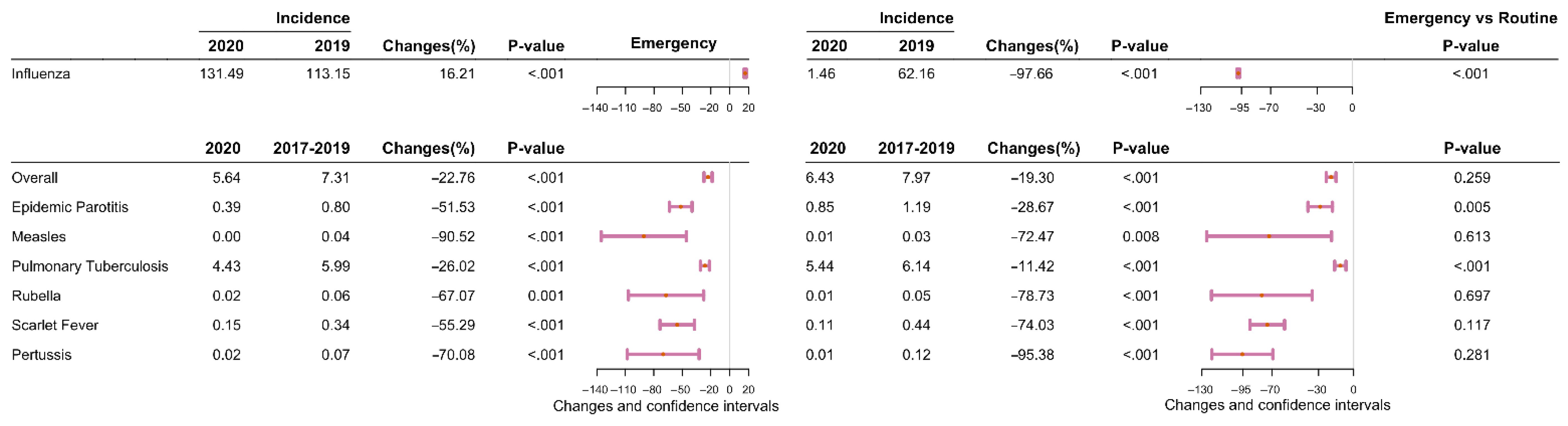
3.1. Descriptive Analysis of the Difference in the Incidence of RIDs between Pre-COVID-19 Period and during COVID-19 Period
3.2. Descriptive Analysis of the Difference in the Overall Incidence of RIDs during the Emergency and Routine Responses to COVID-19 during the COVID-19 Period
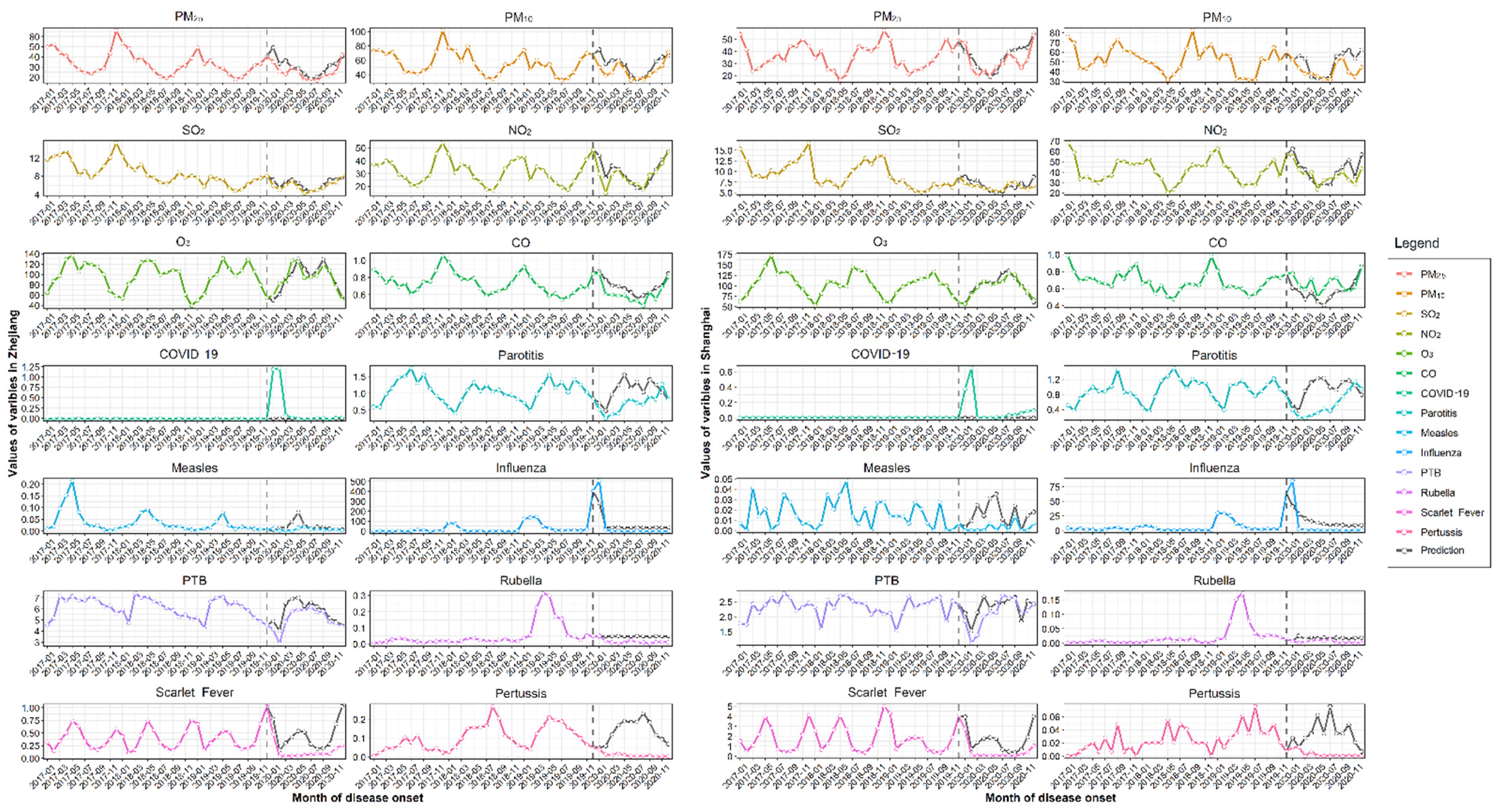
3.3. Descriptive Analysis of the Difference in the Actual and Predicted Overall Incidence of Respiratory Infectious Disease during the COVID-19 Period
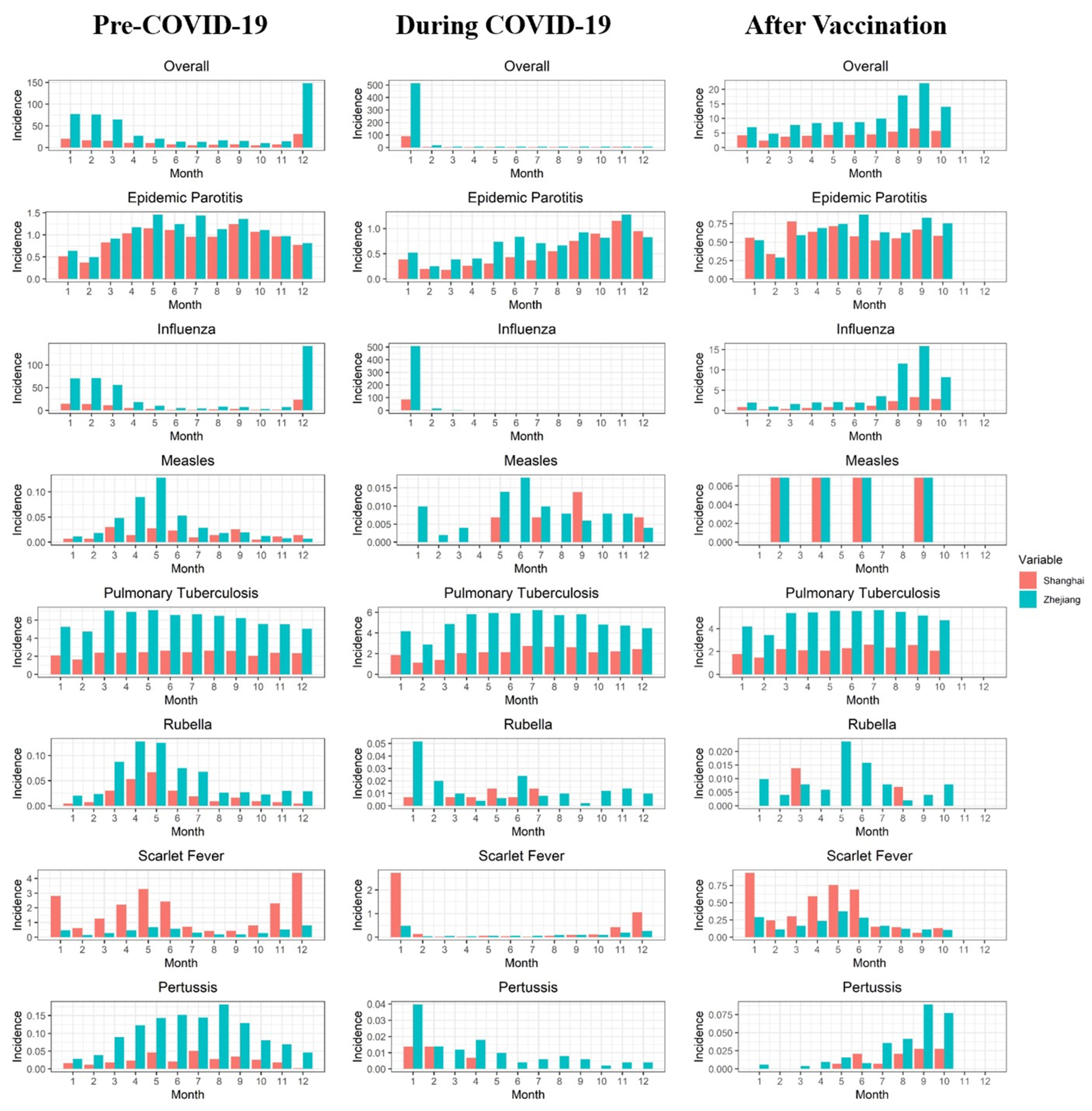
3.4. Descriptive Analysis of the Difference in the Average Monthly Overall Incidence of RIDs Comparing Three Periods: Pre-COVID-19, during COVID-19, and Post-Vaccination
3.5. Descriptive Analysis of the Difference in Air Pollutant Concentrations Comparing Three Periods: Pre-COVID-19, during COVID-19 and Post-Vaccination
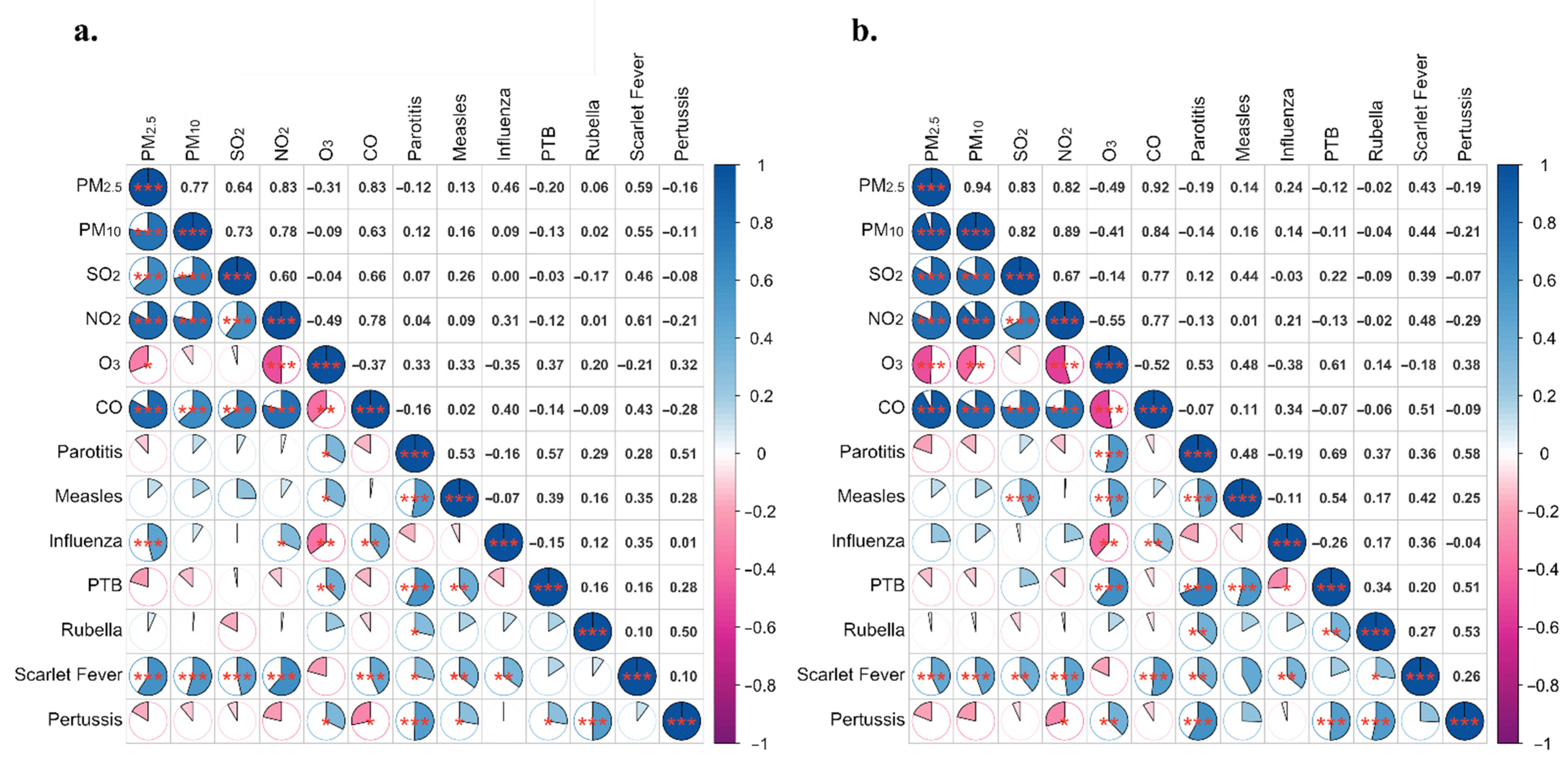
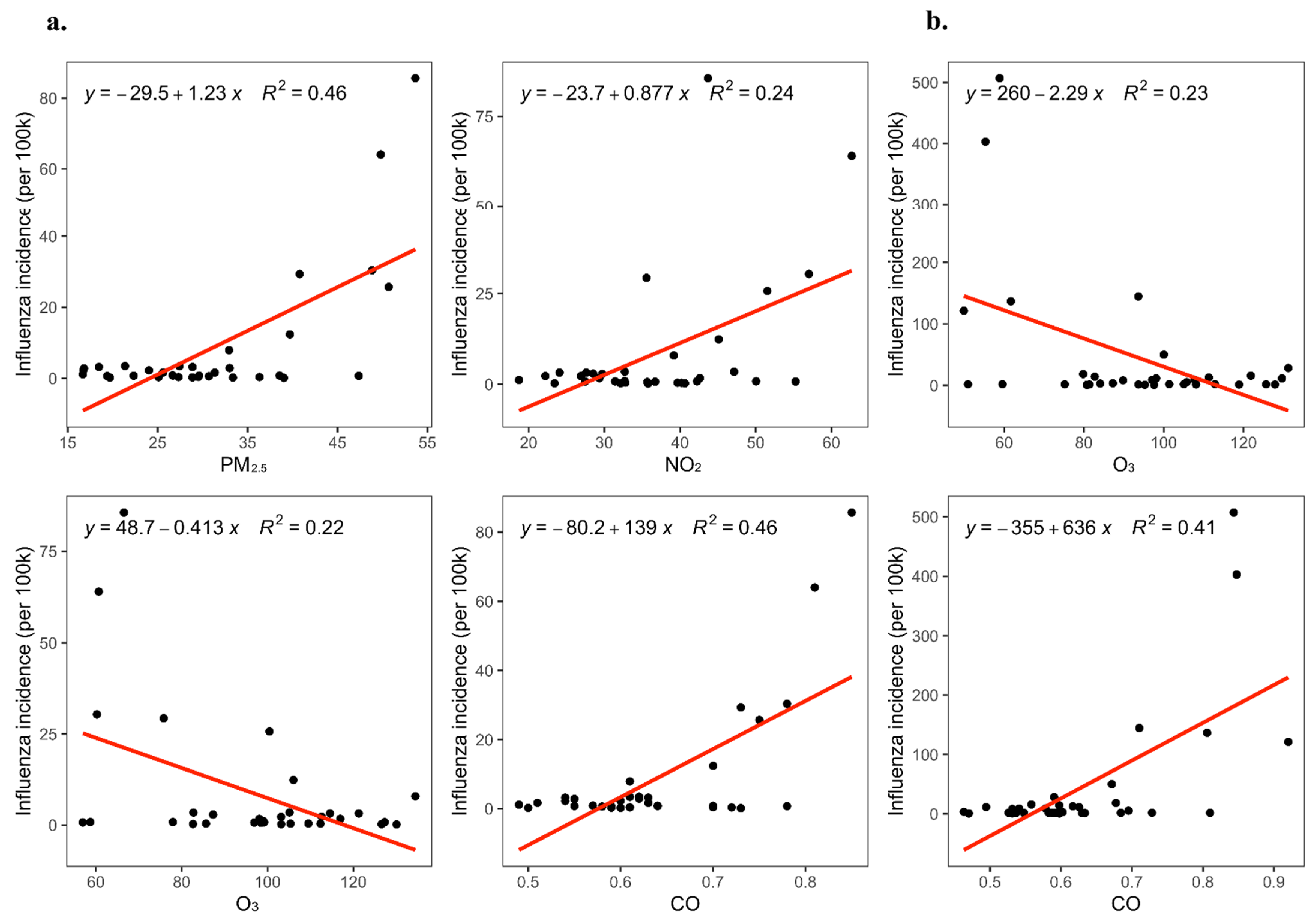
3.6. Descriptive Analysis of the Relationship between the Incidence of RIDs and Air Pollutant Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. WHO 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- WHO. WHO Coronavirus (COVID-19) Dashboard. WHO 2022. Available online: https://covid19.who.int/ (accessed on 6 January 2022).
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, L.; Yan, Y.; Zhou, Y.; Yin, P.; Qi, J.; Wang, L.; Pan, J.; You, J.; Yang, J.; et al. Excess mortality in Wuhan city and other parts of China during the three months of the COVID-19 outbreak: Findings from nationwide mortality registries. BMJ 2021, 372, n415. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, Q.; Feng, L.; Rodewald, L.; Xia, Y.; Yu, H.; Zhang, R.; An, Z.; Yin, W.; Chen, W.; et al. Active case finding with case management: The key to tackling the COVID-19 pandemic. Lancet 2020, 396, 63–70. [Google Scholar] [CrossRef]
- Ren, R.; Zhang, Y.; Li, Q.; McGoogan, J.M.; Feng, Z.; Gao, G.F.; Wu, Z. Asymptomatic SARS-CoV-2 infections among persons entering China from April 16 to October 12, 2020. JAMA 2021, 325, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Attanayake, A.; Perera, S.S.N.; Jayasinghe, S. Phenomenological modelling of COVID-19 epidemics in Sri Lanka, Italy, the United States, and Hebei Province of China. Comput. Math. Methods Med. 2020, 2020, 6397063. [Google Scholar] [CrossRef]
- Wang, X.Y.; Zhang, Y.Q.; Cai, L.W. Spatiotemporal characteristics of the COVID-19 resurgence in the metropolitan wholesale market of Beijing, China. J. Travel Med. 2021, 28, taab008. [Google Scholar] [CrossRef]
- Gao, G.F. COVID-19: A year long and beyond? China CDC Wkly. 2021, 3, 2. [Google Scholar] [CrossRef]
- Lee, H.H.; Lin, S.H. Effects of COVID-19 prevention measures on other common infections, Taiwan. Emerg. Infect. Dis. 2020, 26, 2509–2511. [Google Scholar] [CrossRef]
- Soo, R.J.J.; Chiew, C.J.; Ma, S.; Pung, R.; Lee, V. Decreased influenza incidence under COVID-19 control measures, Singapore. Emerg. Infect. Dis. 2020, 26, 1933–1935. [Google Scholar] [CrossRef]
- Trenholme, A.; Webb, R.; Lawrence, S.; Arrol, S.; Taylor, S.; Ameratunga, S.; Byrnes, C.A. COVID-19 and infant hospitalizations for seasonal respiratory virus infections, New Zealand, 2020. Emerg. Infect. Dis. 2021, 27, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Wong, N.S.; Leung, C.C.; Lee, S.S. Abrupt subsidence of seasonal influenza after COVID-19 outbreak, Hong Kong, China. Emerg. Infect. Dis. 2020, 26, 2753–2755. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P. COVID-19 versus seasonal influenza 2019-2020: USA. Wien. Klin. Wochenschr. 2020, 132, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ding, H.; Chang, S.T.; Lu, R.; Zhong, H.; Zhao, N.; Lin, T.H.; Bao, Y.; Yap, L.; Xu, W. Exposure to air pollution and scarlet fever resurgence in China: A six-year surveillance study. Nat. Commun. 2020, 11, 4229. [Google Scholar] [CrossRef]
- GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, A.; Yin, J. Short-term effects of ambient ozone, PM2.5, and meteorological factors on COVID-19 confirmed cases and deaths in Queens, New York. Int. J. Environ. Res. Public Health 2020, 17, 4047. [Google Scholar] [CrossRef]
- Box, G.E.P.; Jenkins, G.M. Time Series Analysis: Forecasting and Control; Holden-Day: San Francisco, CA, USA, 1976; ISBN 816211043. [Google Scholar]
- Cai, J.H.; Wang, X.S.; Ge, Y.L.; Xia, A.M.; Chang, H.L.; Tian, H.; Zhu, Y.X.; Wang, Q.R.; Zeng, J.S. First case of 2019 novel coronavirus infection in children in Shanghai. Chin. J. Pediatr. 2020, 58, 86–87. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ueda, P. Seasonal influenza activity during the SARS-CoV-2 outbreak in Japan. JAMA 2020, 323, 1969–1971. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Q.; Qi, B.; Hu, D.; Wang, J.; Zhang, J.; Yang, H.; Zhang, S.; Liu, L.; Xu, L.; Li, W. Spatiotemporal variations and reduction of air pollutants during the COVID-19 pandemic in a megacity of Yangtze River Delta in China. Sci. Total Environ. 2021, 751, 141820. [Google Scholar] [CrossRef]
- Becker, S.; Soukup, J.M. Exposure to urban air particulates alters the macrophage-mediated inflammatory response to respiratory viral infection. J. Toxicol. Environ. Health A 1999, 57, 445–457. [Google Scholar] [CrossRef]
- Ng, Y.C.; Chung, W.C.; Kang, H.R.; Cho, H.J.; Park, E.B.; Kang, S.J.; Song, M.J. A DNA-sensing-independent role of a nuclear RNA helicase, DHX9, in stimulation of NF-κB-mediated innate immunity against DNA virus infection. Nucleic Acids Res. 2018, 46, 9011–9026. [Google Scholar] [CrossRef] [PubMed]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Wang, K.; Zhong, H.; Zhao, N.; Xu, W.; Yang, Y.; He, Y.; Liu, S. The Effect of Coronavirus 2019 Disease Control Measures on the Incidence of Respiratory Infectious Disease and Air Pollutant Concentrations in the Yangtze River Delta Region, China. Int. J. Environ. Res. Public Health 2022, 19, 1286. https://doi.org/10.3390/ijerph19031286
Wang L, Wang K, Zhong H, Zhao N, Xu W, Yang Y, He Y, Liu S. The Effect of Coronavirus 2019 Disease Control Measures on the Incidence of Respiratory Infectious Disease and Air Pollutant Concentrations in the Yangtze River Delta Region, China. International Journal of Environmental Research and Public Health. 2022; 19(3):1286. https://doi.org/10.3390/ijerph19031286
Chicago/Turabian StyleWang, Lan, Kehan Wang, Hui Zhong, Na Zhao, Wangli Xu, Yunmei Yang, Yiran He, and Shelan Liu. 2022. "The Effect of Coronavirus 2019 Disease Control Measures on the Incidence of Respiratory Infectious Disease and Air Pollutant Concentrations in the Yangtze River Delta Region, China" International Journal of Environmental Research and Public Health 19, no. 3: 1286. https://doi.org/10.3390/ijerph19031286