1. Introduction
COVID-19 was declared a “pandemic” by the World Health Organization (WHO) in March 2020, and has posed massive challenges related to health, economy, and the social fabric of the entire human population [
1]. To curb the spread of the virus, the Government of Pakistan, similar to other countries, issued several public health guidelines, preventative measures, and made widely available a solution in the form of vaccination. In Pakistan, with more than 1.15 million confirmed cases of COVID-19, around twenty-five thousand deaths as of 30 August 2021 [
2], and the presence of the concern of variants in the ongoing wave of COVID-19, it is necessary to enhance vaccine coverage in the country in order to acquire herd immunity.
Following the initiation of the push for vaccination campaign in most developed and developing nations, Pakistan launched its vaccination campaign for frontline workers in February 2021 with the Chinese vaccine, Sinopharm. Currently, there are seven different vaccines including Sinopharm, Sinovac, AstraZeneca, Cansino, Sputnik, Pfizer-BioNTech and Moderna, which are registered for use in Pakistan [
3]. Due to the limited production as well as limited availability of vaccine doses in the initial stages of the vaccination campaign, elderly people, healthcare workers, and other frontline individuals were prioritized for vaccination, as they were deemed most susceptible to get infected. The roll out of the vaccine then followed a decreasing age order [
4] or decreasing susceptibility of catching the virus. Following this mechanism of vaccination, experts expected to vaccinate a large number of the population in a short period of time.
In Pakistan, 1% of the population was fully vaccinated and 2.6% was partially vaccinated on 3 June 2021. However, these percentages rose over a period of 3 months, and on the 25th of August, 6.3% of Pakistan’s population was fully vaccinated and 10.8% was partially vaccinated. At the time of the study, only 6.3% of 67 million of the target population of Punjab was vaccinated against COVID-19 [
5]. According to epidemiologists, achieving herd immunity is impossible without 70% of the total world’s population fully immunized with the COVID-19 vaccine [
6].
1.1. Vaccine Hesitancy and Acceptability
One of the biggest challenges in vaccine uptake is vaccine hesitancy [
7]. Poliomyelitis, a vaccine-preventable disease, is eradicated globally but Pakistan is one of the only two countries in the world where it is still endemic [
8]. This highlights the reluctance of people towards not only COVID-19 vaccines, but vaccines in general. A range of religious, cultural, social, and ethnic beliefs may influence the public’s decision to get vaccinated [
9,
10,
11]. In addition to this, mistrust in government institutions [
12], safety concerns and potential risks are considered an important factor in determining the vaccines’ acceptability [
13]. One of the major reasons of vaccine hesitancy among people is the perceived side effects attached with receiving a dose [
14]. Those who are hesitant in getting immunized believe that the rapidly developed vaccines may have alleged harms and unforeseeable adverse reactions [
15], ranging from minor pain at the site of the injection to severe health conditions such as blood clotting [
16,
17].
1.2. Barriers to Vaccine Acceptance
The effectiveness of inoculation campaigns for curbing the spread of the pandemic is not only dependent on the vaccine’s safety and efficacy, but also on its availability and people’s attitude towards them [
18].
According to Fisk [
19], there are two types of barriers that hinder the uptake of vaccines: structural and attitudinal. Structural barriers are the systematic issues which impact an individual’s ability to access a service. They include availability- and affordability-related factors, such as cost, outlet location, or transportation. Attitudinal barriers are the perceptions or beliefs that influence the willingness of individuals that are at-risk to seek out and accept a service. They include perceptions about communicable diseases, perceptions about vaccines, and fear and trust issues with healthcare and Government agencies and satisfaction with the provided services. Of all attitudinal barriers, public trust is particularly important [
19].
Currently, in Punjab, the population of age 17 and above is being registered for vaccination. A large number of vaccination centers have also been established in public schools and colleges for better outreach and access (several were operating 24 h a day and seven days a week in the initial months of the vaccination campaign). Currently, there are 677 COVID-19 Vaccination Centers (CVCs) being operated in Punjab, however, only 17.16% of the population of the country is vaccinated with at least one dose. The 24/7 availability of free vaccines and vaccination centers shows that structural barriers are not restricting Pakistan in achieving full vaccination coverage against COVID-19.
The low uptake can, thus, be linked to attitudinal barriers at the community level. In Pakistan, behavioral and communication strategies such as broadcasting vaccination messages through mobile phone ringtones, at a broader level, and through the engagement of celebrities and Government leaders who share their own vaccination experiences and general information on the vaccine [
20], as well as announcements in residential areas and mosques have been used to motivate masses for immunization against COVID-19 [
21].
As discussed earlier, various religious factors and misinformation circulating on social media platforms continue to influence the uptake of the COVID-19 vaccine in Punjab. Being the largest province in Pakistan, Punjab is at a high risk of COVID-19, with 388,297 confirmed cases up to 27 August 2021. Despite the Provincial Government’s campaign and efforts to promote access to the vaccine, not enough people are getting themselves vaccinated.
This paper is a part of a broader post-vaccination survey on COVID-19. The objectives of this research were to find out the attitude of people towards COVID-19 vaccination and to assess the factors associated with COVID-19 vaccine acceptance or hesitancy in the Punjab province, which houses half of Pakistan’s population. The results of this survey may be helpful in providing a data-driven solution to achieve vaccine targets for the broader population (including the most vulnerable groups), vaccine roll out, and monitoring of vaccine accessibility for all.
2. Materials and Methods
Due to limitations in conducting face-to-face research during the fourth wave of the COVID-19 outbreak in Pakistan from July to September 2021, telephonic interviews were conducted by enumerators using a cross-sectional survey design. Telephone was selected as the medium for data collection because it is one of the most widely used, easily accessible and low-cost platforms for communication in Pakistan [
22]. The study was carried out at the provincial level and samples were collected from almost all cities of Punjab where vaccination centers were established preceding the survey. The data were collected from both vaccinated and non-vaccinated individuals above the age of 40 years.
2.1. Inclusion Criteria
For vaccinated group, the inclusion criteria were individuals 40 years and above who were completely vaccinated with any of the COVID-19 vaccine and/or partially vaccinated with COVID-19 vaccine AstraZeneca (the gap between the two doses of AstraZeneca is 84 days and it was first inoculated in April 2021 in Pakistan. Thus, we assumed that a majority of the recipients of this vaccine would be partially vaccinated at the time of data collection for this study).
For non-vaccinated group, the inclusion criteria were individuals aged 40 and above who either registered for the vaccine and received a vaccination date but still did not receive the dose or did not register and/or did not receive a single dose of any COVID-19 vaccine. Individuals of age 40 and above were targeted because the vaccine roll out in Punjab began with those aged 60 and above, followed by age 50 and then 40-year-olds. At the time of the survey, it was safe to assume that several candidates who had completed two doses of COVID-19 vaccination could be found in this target population. On the other hand, for non-vaccinated individuals above 40 years of age, it was assumed that they might have perceived any barrier in getting vaccination. Respondents who were approached but refused to participate, or had a serious mental or physical disease, were excluded from the survey.
2.2. Data Collection Tool
For data collection, a structured questionnaire was developed on the basis of extensive review of relevant literature, stakeholders’ consultations, and appraisal of misinformation about COVID-19 circulating on social media. The questionnaire was developed in English, but to minimize the communication barrier, it was translated into national language (i.e., Urdu). The questionnaire was pre-tested to identify redundant questions, determine the time required to complete the survey questionnaire and gave an idea about the response rate. The questionnaire was revised and improved in the light of pre-testing experiences as well as according to the suggestions of the experts. The final questionnaire had six sections, each with various close-ended questions (here only three sections are mentioned which are relevant to the present paper).
The first section of the questionnaire records the socio-demographic profile including age, sex, religion, highest level of education, monthly family income, type of occupation, sector of employment, occupation, region, marital status, number of children, and exposure to different forms of media i.e., television, mobile phone, newspapers and internet to seek information. Usage of one media source for seeking information was recoded as ‘low access’, two or three as ‘moderate access’, and four or more as ‘high access’.
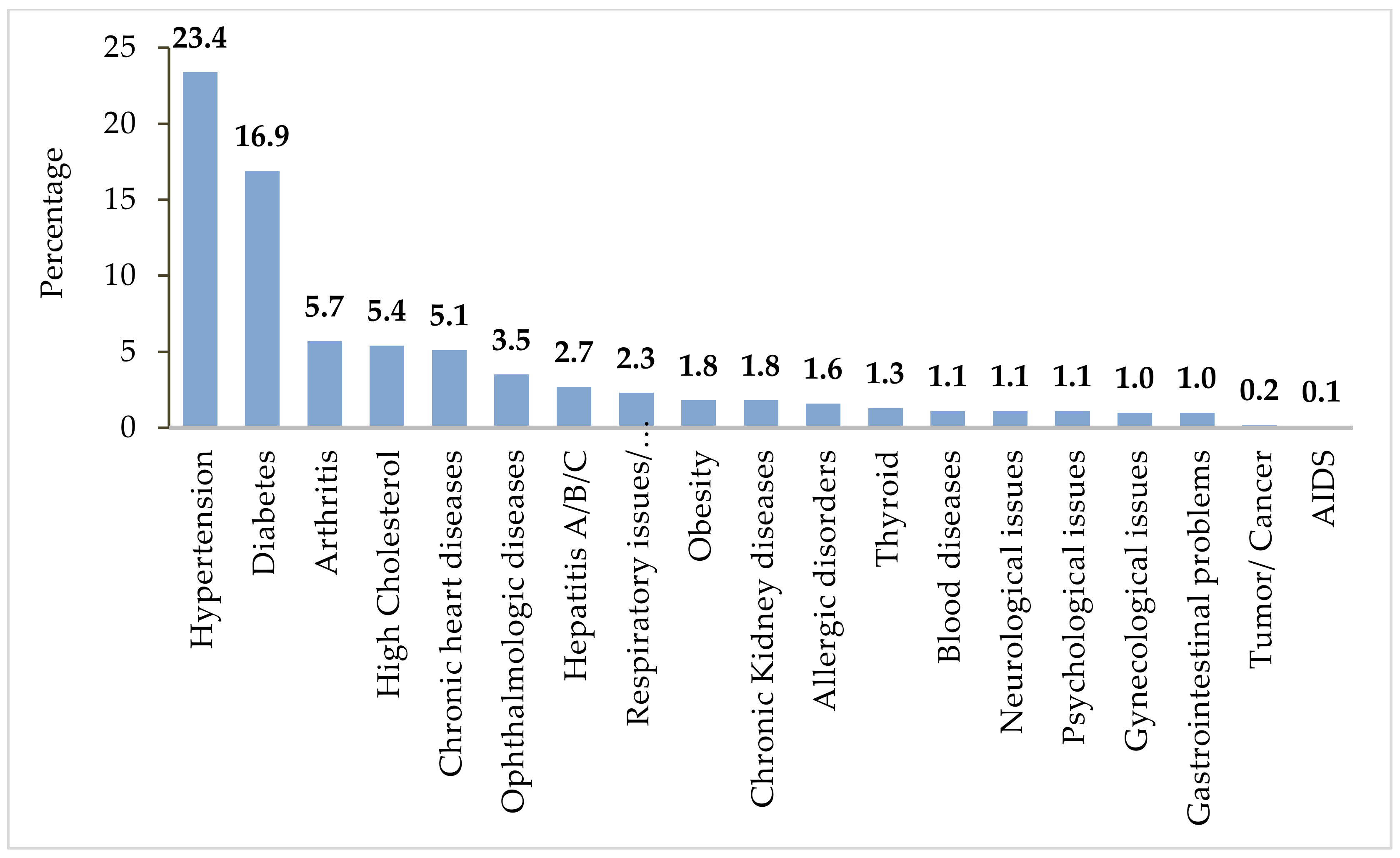
The second section focused on co-morbidities and health status of individuals. The first question, a checklist, asked the respondent about history of various health conditions while other questions inquired about allergies, adverse events due to food, medicine, and any vaccination, including the practice of behaviors such as use of tobacco and exercise pattern [
23]. The questions regarding past history of rejecting any other vaccine and if they received vaccination against influenza were also asked [
24]. The next three questions in this section measured previous infection of COVID-19, testing and intensity of the illness [
25]. The section concluded by assessing current health status through a rating scale ranging from ‘very poor’ to ‘very good’ [
24].
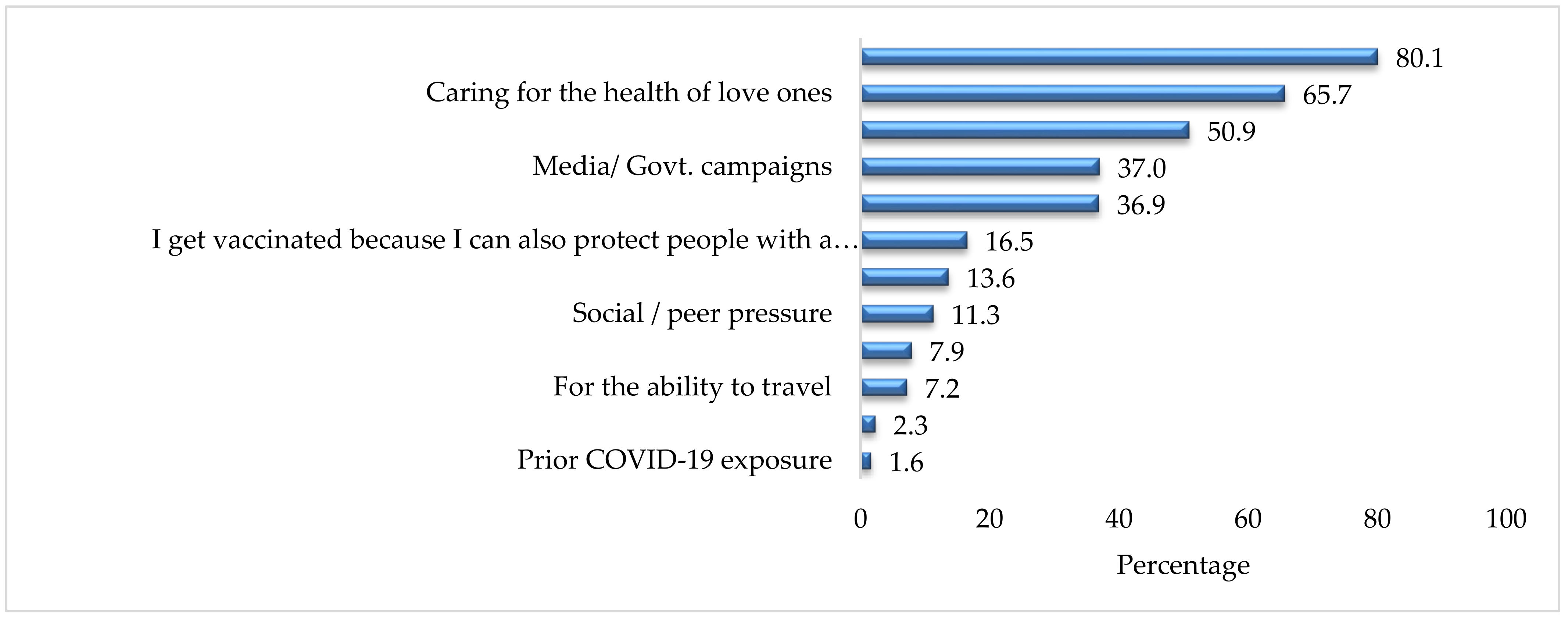
The third section made use of seven questions to determine the acceptability rate of COVID-19 vaccination. The respondent was asked whether he/she is vaccinated or not and about the factors involved in the decision to get or not to get vaccinated [
10,
11,
12,
26,
27]. In case the respondent is not vaccinated, he/she is inquired about willingness to get vaccinated.
2.3. Sample Size, Sampling Technique and Recruitment of Respondents
Sample size of the survey was calculated as 1067 on the basis of a previous study on the acceptance of COVID-19 vaccination in Southeast Asia [
28]. The sample size was calculated using the formula
n = (z
2 ×
pq)/e
2 with a 3% margin of error, 95% confidence interval and a 50% vaccine acceptability. Where:
e is the desired level of precision (i.e., the margin of error),
p is the (estimated) proportion of the population that has vaccination acceptability,
q is 1 − p
Assuming non-response rate of 20% (based on previous research carried out by Azoulay [
29], the sample size was increased to 1284 before starting the data collection. Since one of the key objectives of this study was to determine the perceived effectiveness of COVID-19 vaccination in the province, a relatively larger sample of vaccine recipients (60%) was included, as compared to vaccine non-recipients (40%).
To receive the COVID-19 vaccine in Punjab, individuals need to register themselves with the National Database and Registration Authority (NADRA). Data related to Government vaccinations is fed into this database in Punjab by the Primary and Secondary Healthcare Department (P&SHD). Hence, the list of vaccine recipients was obtained from the P&SHD.
Regarding non-vaccinated individuals, the Department maintained a limited list of those who registered for the vaccine but had not received it yet. Convenient sampling was used to generate a database of non-vaccinated individuals from all the contacts (vaccinated and non-vaccinated) provided by P&SHD. Additional contacts were collected from public sector employees including lady health workers (LHWs), lady health supervisors (LHSs) and lady health visitors (LHVs) of respective districts, individuals working under Social Security Department, workers of different factories and private organizations to generate a database of non-vaccinated individuals above 40 years of age.
From the generated databases of both vaccinated and non-vaccinated individuals, survey respondents were recruited through random sampling using computer-generated random numbers. The lists were first divided based on districts of the potential respondents to ensure that each district in the Province was represented in the sample, and then it was further divided based on the type of vaccine, so that each vaccination type was included. After this, numbers were selected using the Random Number Function (RAND) in Microsoft Excel (Microsoft Corporation, Albuquerque, NM, USA). Enumerators contacted the respondents through their given phone/mobile numbers, introduced the study to them and asked them for their consent to participate in the study.
The questionnaire was pre-tested with 156 participants. The minimum sample for pre-testing was calculated by taking 10 percent of the total sample. Same method, inclusion criteria and sampling technique was followed for pre-testing and the sample of pre-testing was not included in the final sample size.
For data collection, telephonic calls were made using official P&SHD landline connections over a period of two weeks from 12 July to 26 July 2021. This was done to increase respondents’ willingness to accept calls and therefore increase the response rate of the study, because a call from an official government organization is considered safe and secure, as opposed to a number from a private network. If a person has given the wrong number or the number of a relative, efforts were made to trace the individual using the available contact number. Numbers not responding on a specific day and time were re-attempted on other days at different times. If the telephone calls were not answered after three attempts on varying days and times, it was marked as non-response.
2.4. Training of Research Team
A one-day training was imparted to the research team. The interviewers were trained to communicate effectively with respondents to maximize responses. They were trained to answer potential questions of respondents (especially reluctant respondents) in a quick and confident manner to improve the response rate of the study. The research team was made aware of the contents of the survey tool, telephonic interview protocols, steps for implementing the survey tool, data submission guidelines, and roles and responsibilities of enumerators. They were also trained in following ethical considerations including respecting consent, anonymity, and confidentiality of the respondents. If the respondents were not willing to partake in the interview, they would not be forced to participate.
2.5. Ethical Considerations
The study protocols were reviewed and approved by the Institutional Ethics Review Board, University of the Punjab (D/No: 182/DFEMS/PU). The study strictly followed international guidelines for ethical review of epidemiological studies [
30]. As described earlier, informed consent was obtained from all respondents over the telephone before formally starting the interview. The study was introduced to the respondents, and they were ensured of confidentiality of information and protection of privacy. They were guaranteed that their names and data, including health information, would only be used for research purposes.
Data collected by enumerators was submitted to field supervisors on a daily basis. All questionnaires received from the enumerators were checked by supervisors and data analysts before data entry. Data entry was done by data entry clerks, and to minimize the inconsistencies and human error, data was thoroughly cleaned by data analysts, data entry clerks, and field supervisors. Close coordination with the team lead and the deputy team lead of the project team for review and feedback was maintained throughout the project.
2.6. Statistical Analysis
Data entry was done in SPSS (version 26) (IBM, Armonk, NY, USA) by data entry clerks in parallel with data collection. After complete data entry, data was cleaned thoroughly by data entry clerks, data analysts, and field supervisors. After proper cleaning of data, it was analyzed using descriptive and inferential statistics in SPSS by data analysts. For the descriptive analysis, univariate analysis including frequencies, percentages, and graphs were used while for inferential statistics, Chi-square and binary logistic regression analysis with 95% confidence interval and 0.05 significance was used. The variables significant at binary logistic regression analysis were placed in multivariate logistic regression analysis. Odds ratio (OR), adjusted odds ratio (AOR) and 95 percent confidence intervals are presented. p-value less than 0.05 was considered statistically significant. In multivariable logistic regression, all independent variables that were significant at 0.05 level were entered in the model. The multi-collinearity between the variables was also assessed and highly correlated variables were eliminated from the logistical model. For example, multicollinearity was assessed between employment status and sector of employment. Since it was significant, sector of employment was eliminated from the model.
4. Discussion
The best strategy to deal with any pandemic and to reduce the impact of infection is to ensure the availability of an effective and accessible vaccination. Likewise, to control the effects of the COVID-19 pandemic on people’s lives, the entire world is in the process of mass inoculations, with efforts to vaccinate a large proportion of the population in the shortest possible time, making it the fastest vaccine delivery in history [
31]. However, as of now, only one-fourth of the total world’s population has been vaccinated [
32]. The share of the vaccinated population varies from country to country with UAE having the highest vaccination rate of almost 90% being fully vaccinated while only 23.5% of the population of Pakistan is fully vaccinated, as of 3 December 2021 [
32]. The varying vaccination rates in different countries can be attributed to hesitancy [
7] and concerns of people regarding the effectiveness and safety of the vaccines [
13].
This is the first province-wide study conducted in the province of Punjab examining the reasons for vaccine acceptance and hesitancy. Our study found that a majority of respondents were male, in the 40–49 age group, lived in urban areas, followed Islam as a religion, and belonged to the middle-income class. A relative low participation of women in the vaccination campaign can be seen within the context of socio-cultural aspects of Pakistani society. Women are socially and economically disadvantaged, which subjects them to various cultural restrictions including mobility constraint [
33], vaccine registration of female respondents from the telephone number of any male member of family, hesitancy of females to talk to strangers or to give them any kind of information and relatively less possession of personal mobile devices by females compared to males [
34], which makes women non-uniform passive recipients of benefits [
35].
In addition to this, women in Pakistan are not majorly part of a formal workforce of the country and they do not have any obligation of getting vaccinated, as a majority of the females resides at home as housewives [
33]. It is important to mention here that workplaces in Pakistan, especially in the public sectors, have made it compulsory for their employees to get COVID-19 vaccination [
36].
The findings of the present study are consistent with previous research. For example, socio-demographic variables such as age group being 60–69 years [
37,
38,
39,
40,
41,
42,
43,
44], middle or higher level of education [
38,
40,
41,
42,
45,
46,
47], being currently married [
48,
49,
50], being employed [
42,
51,
52], having a monthly family income of 20,001–50,000 PKR [
40,
43,
45,
47,
48,
51], residing in urban areas, having high access to mass media, having a history of influenza vaccination [
38,
41,
49,
53,
54,
55], performing physical activity, and perceiving fair and good status of health [
47], were significantly associated with COVID-19 vaccination uptake. Findings revealed that the pandemic had largely affected the income, work, and daily lives of more than 40% of the respondents. Despite this, people feel reluctant to get vaccinated. Low vaccination coverage, despite the Government’s best efforts, may point towards the hesitancy and reluctance of people in accepting the vaccines [
7]. In order to expand vaccination coverage and to achieve maximum vaccination rates, understanding people’s perception and behavior towards vaccines is necessary.
There are different reasons that contribute towards increasing people’s reluctance to accepting vaccines in general, including concerns about vaccine effectiveness, and its safety and side effects [
14]. However, in a country such as Pakistan, vaccine acceptance rates are low as the health decisions of a majority of the population is also influenced by various religious, cultural, social, and ethnic values [
9,
10,
11]. Similar to our study, various studies from Pakistan show that people in Pakistan perceive vaccination campaigns to be a Western/American/Illuminati agenda [
9], as an attempt of genocide against Muslims [
11] and/or a means to reduce the fertility rates of Muslims [
10]. Greater vaccine hesitancy rates in Pakistan also points towards the lack of health literacy and lack of trust of government policies [
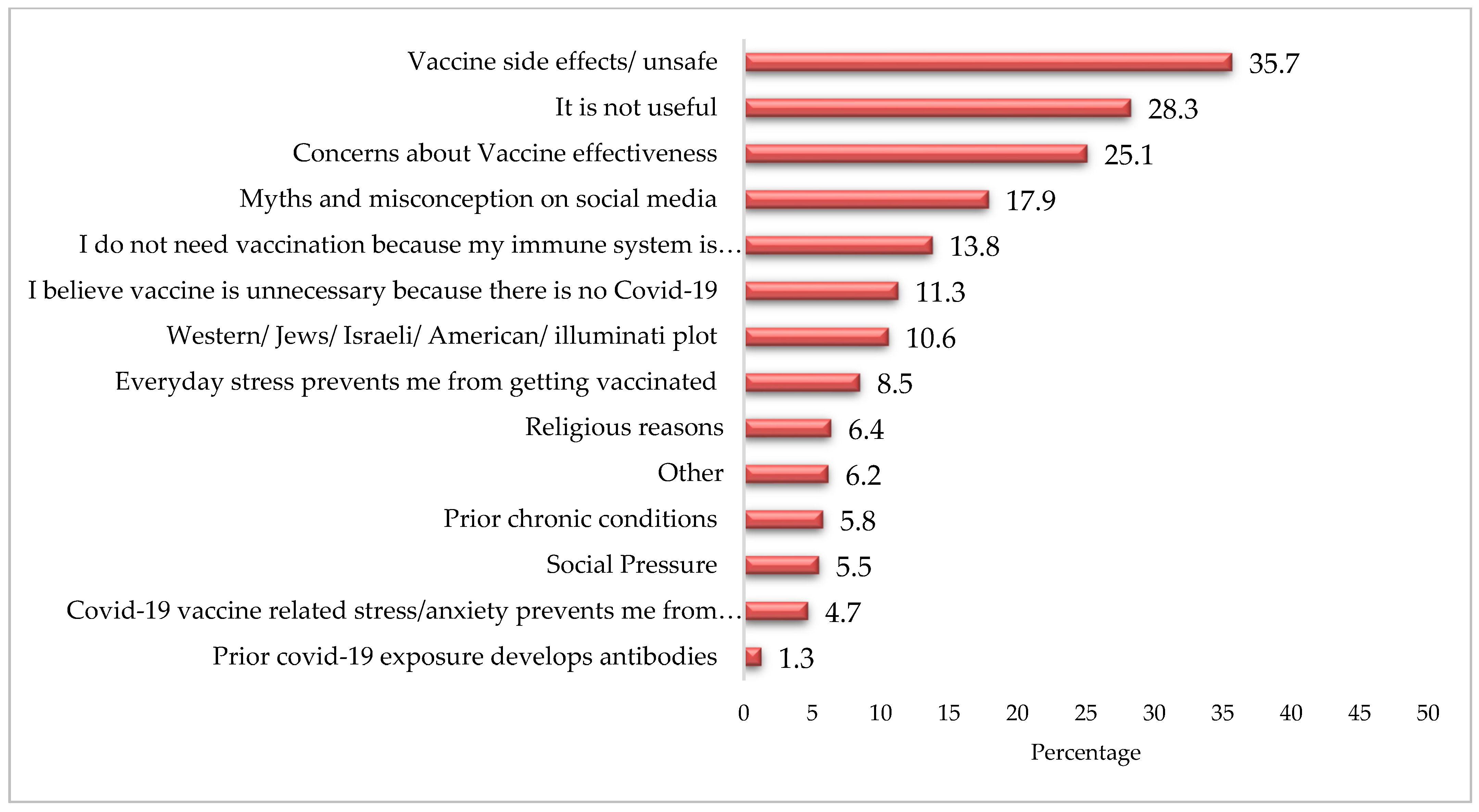
12]. In addition to this, there are various myths and misinformation attached with the COVID-19 vaccine. For example, a large proportion of the non-vaccinated respondents believed that the vaccines were unsafe (35.7%); moreover, 28.3% considered it useless, while one-fourth (25.1%) of the respondents reported to be concerned about vaccine effectiveness.
Given the current situation of the healthcare system in Pakistan, and previous experiences of different vaccination campaigns, understanding vaccine acceptance in Pakistan is very necessary to control the pandemic. The attitudes and perceptions of people regarding vaccines are key factors that determine vaccine acceptance [
18]. Pakistan, being a country of rich cultural and religious profiles, has cultural variations that are prevalent in the shape of ethnicity as well as based on region of residence (rural/urban/semi urban) [
56]. This study found that people believed in the emergence of Islamophobia in the West, due to which they perceived the COVID-19 infection as well as the vaccination campaign as a genocidal attempt towards Muslims to control their population by causing infertility and considering it a “Western plot” in general, as is perceived about other vaccination campaigns by some communities in Pakistan [
9,
10,
11]. Additionally, the prevalence of other myths and misconceptions included considering COVID-19 to be a man-made virus [
18,
57], fear of insertion of a secret micro-chip under the guise of vaccination [
18], increased chances of death, and a lack of trust in the government [
40], health workers [
50], and the vaccine [
24,
39,
42,
47,
51,
58,
59,
60]. The present study reported these factors to be responsible for vaccine hesitancy in Pakistan. Other factors highlighted by the present study that contributes to COVID-19 vaccine hesitancy among people include the perceived side effects of the COVID-19 vaccine [
15,
24,
38,
52,
53,
60,
61,
62], concerns of people regarding different types of vaccines developed in a short period of time [
58,
60], and their alleged side effects including increased chances of death. People also reported some structural barriers, such as time constraint and facility accessibility issues [
19,
48]. This highlights the need for developing strategies to not only eliminate attitudinal but structural barriers as well.
In accordance with the findings of previous studies [
24,
39], the present study revealed that females are more hesitant than males in getting COVID-19 vaccination while people working in the private sector, had any chronic illness, were inoculated with influenza vaccination in the past or had contact with COVID-19 cases were more likely to accept the vaccine. Fisher et al. [
38] also revealed the higher likelihood of influenza vaccine recipients to accept the COVID-19 vaccine in the United States while Reno and colleagues [
52] reported the positive association of the prevalence of any chronic illness with the likelihood of getting the COVID-19 vaccination. The present study further reported that people with higher levels of education and income were more likely to accept the COVID-19 vaccine, which also echoes the findings in the literature on COVID-19 vaccine acceptance [
38,
52].
The results of the present study as well as of many previous studies that explored the reasons for vaccine hesitancy highlighted that the majority of unvaccinated people did not want to get vaccinated due to a low perceived susceptibility or risk to contracting the virus, believe in the conspiracies against the vaccine [
43,
57], religious reasons [
10,
11] and concerns about the efficacy, effectiveness, and safety of the vaccine [
14]. There are rigorous COVID-19 vaccination campaigns being implemented globally including Pakistan. These campaigns have met with some success by targeting a large number of the population. However, more comprehensive and concerted efforts such as Reach Every Door and Reach Every Community (RED/REC) are needed to engage the community in the vaccination campaign to understand as well as tackle attitudinal barriers, especially in the context of Pakistan that is a milieu of various socio-cultural, ethnic, and religious forces and lags far behind in achieving the goal of Universal Health Coverage [
63].
6. Conclusions
The study concludes that there are various socio-economic characteristics such as sex, income, education, employment, rural residence, as well as access to sources of information, history of influenza vaccination, and disease-related factors which were associated with COVID-19 vaccine uptake. However, vaccine non-recipients were influenced by many myths and misinformation which hindered them in getting vaccinated. These myths, misinformation, and conspiracy theories need to be addressed individually and systematically through effective and well-targeted information, education, and communication strategies. Because of attitudinal barriers, people have a lack of trust in the government, healthcare workers, and on vaccine efficacy and effectiveness. Multi-faceted, comprehensive approaches are needed which involve the entire population and are tailored for different groups, especially for marginalized sections of the society. Behavioral change interventions involving all relevant stakeholders at individual, community, and institutional levels are needed to deal with the barriers perceived by people. In order to expand vaccination coverage and improve vaccine acceptance in Pakistan, academics, public health experts, policy makers, and healthcare workers need to work together to enhance community participation and community mobilization for the COVID-19 vaccination program.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}