
Is SARS-CoV-2 Vaccination of Subjects with a Prior History of Allergies Dangerous? Experiences in the Veneto Region of Italy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Immunization and Adverse Reactions
2.4. Ethical Consideration
2.5. Data and Statistical Analysis
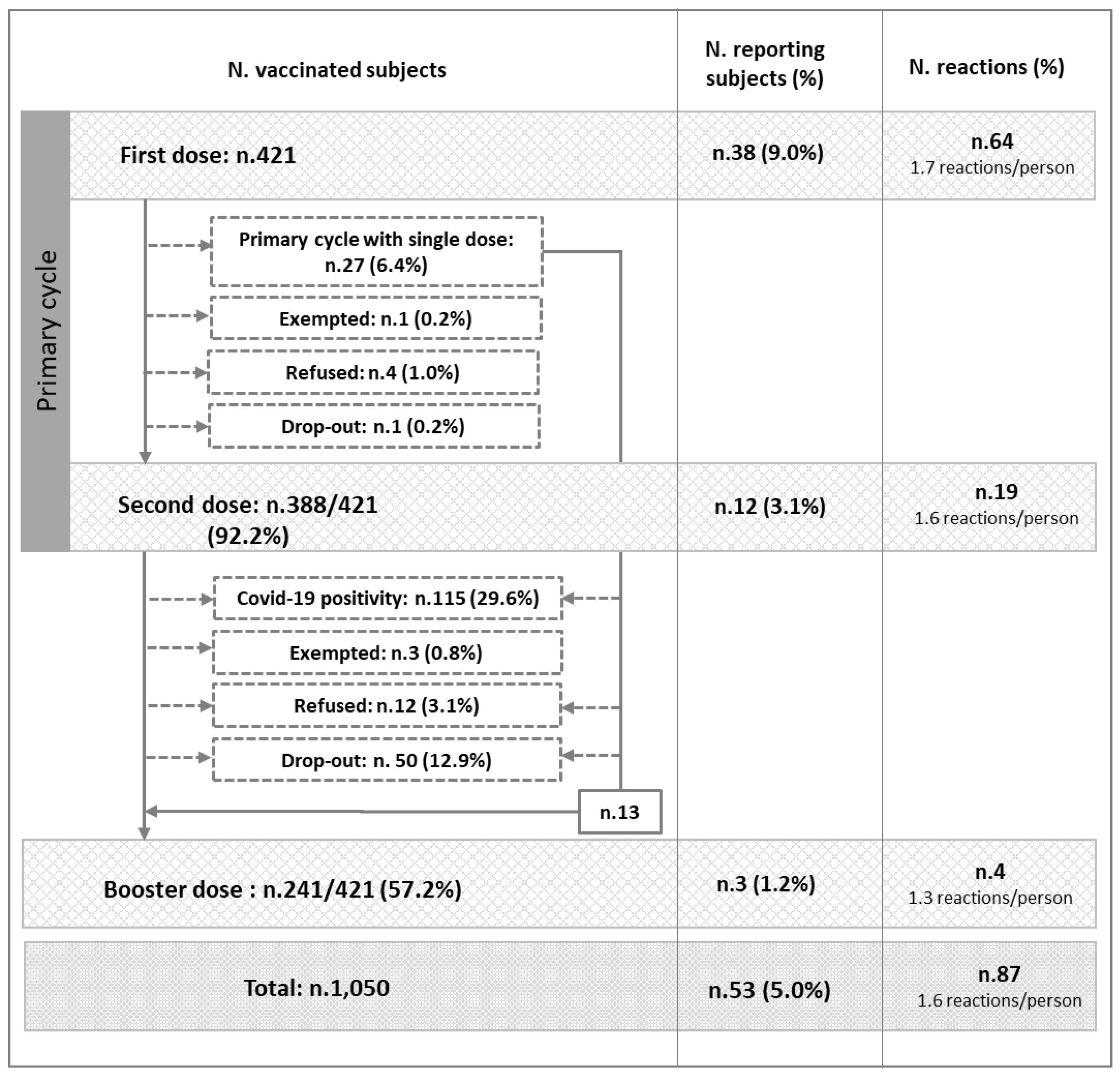
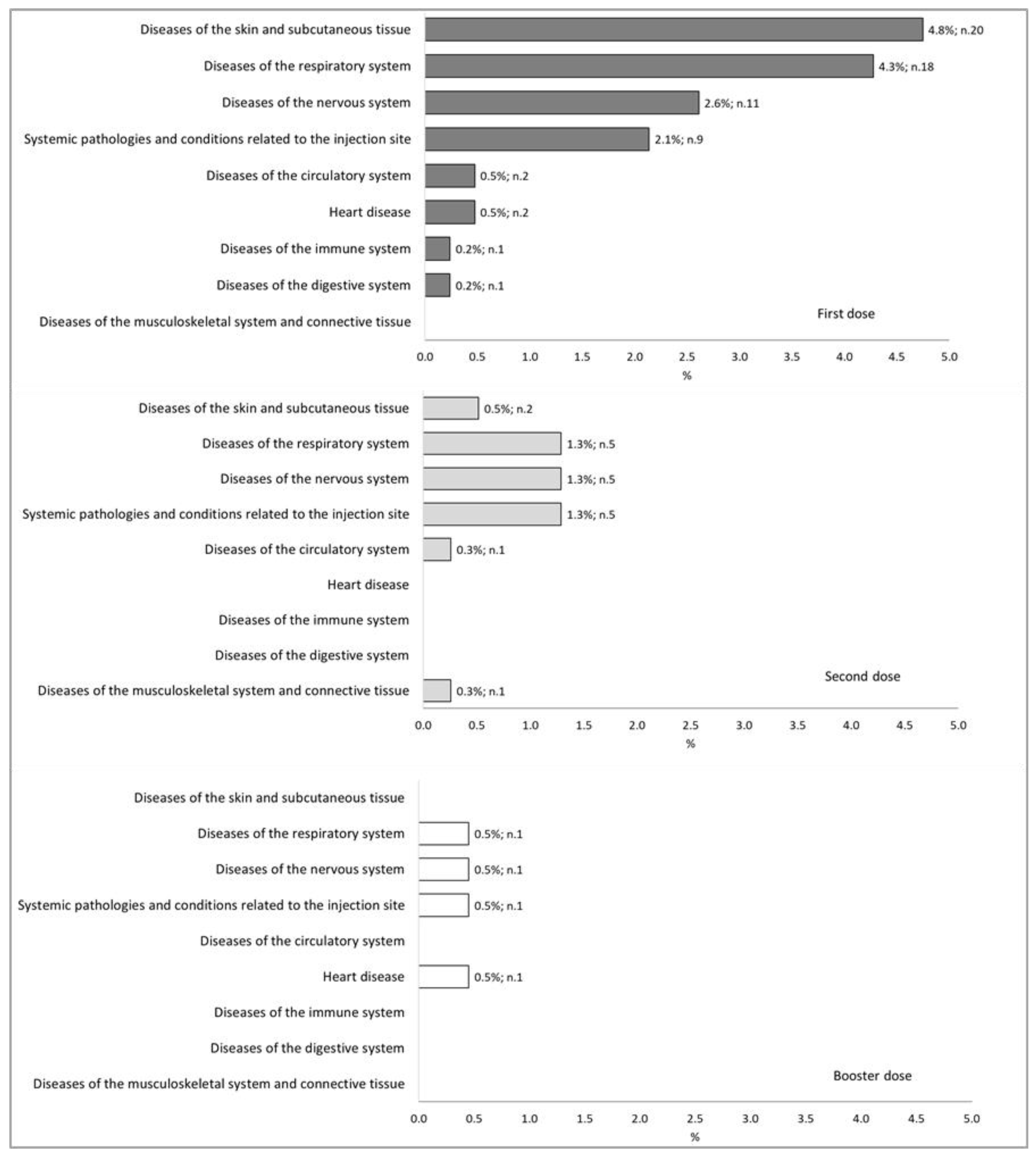
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing COVID-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Baldo, V.; Reno, C.; Cocchio, S.; Fantini, M.P. SARS-CoV-2/COVID-19 Vaccines: The Promises and the Challenges Ahead. Vaccines 2021, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, N.O.; Berasategui, M.A.; Caballer, B.D.L.H.; Santiago, A.V. The Century of mRNA Vaccines: COVID-19 Vaccines and Allergy. J. Investig. Allergol. Clin. Immunol. 2021, 31, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Temiz, S.A.; Abdelmaksoud, A.; Wollina, U.; Kutlu, O.; Dursun, R.; Patil, A.; Lotti, T.; Goldust, M.; Vestita, M. Cutaneous and Allergic reactions due to COVID-19 vaccinations: A review. J. Cosmet. Dermatol. 2022, 21, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, T.T.; Cole, M.; Su, J.R. Reports of Anaphylaxis after Receipt of mRNA COVID-19 Vaccines in the US—14 December 2020–18 January 2021. JAMA 2021, 325, 1101. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Annexes to the Recommendations for Use of the Moderna mRNA-1273 Vaccine against COVID-19; Oms: Geneva, Swiss, 2022; pp. 1–16. [Google Scholar]
- Shavit, R.; Maoz-Segal, R.; Iancovici-Kidon, M.; Offengenden, I.; Yahia, S.H.; Maayan, D.M.; Lifshitz-Tunitsky, Y.; Niznik, S.; Frizinsky, S.; Deutch, M.; et al. Prevalence of Allergic Reactions after Pfizer-BioNTech COVID-19 Vaccination among Adults with High Allergy Risk. JAMA Netw. Open 2021, 4, e2122255. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.P.; Desai, A.P.; Loomis, G.J. Relationship between pre-existing allergies and anaphylactic reactions post mRNA COVID-19 vaccine administration. Vaccine 2021, 39, 4407–4409. [Google Scholar] [CrossRef] [PubMed]
- Italian Drug Agency (AIFA). Rapporto Sulla Sorveglianza dei Vaccini COVID-19 (11; 27/12/2020-26/03/2022); AIFA: Rome, Italy, 2021; pp. 1–16. Available online: https://www.aifa.gov.it/rapporti-su-sorveglianza-dei-vaccini-COVID-19 (accessed on 12 December 2022).
- European Medicines Agency. Spikevax (Previously COVID-19 Vaccine Moderna). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/spikevax (accessed on 23 November 2022).
- World Health Organization. Statement for Healthcare Professionals: How COVID-19 Vaccines Are Regulated for Safety and Effectiveness (Revised March 2022). 2022. Available online: https://www.who.int/news/item/17-05-2022-statement-for-healthcare-professionals-how-COVID-19-vaccines-are-regulated-for-safety-and-effectiveness (accessed on 23 November 2022).
- Kaplan, B.; Farzan, S.; Coscia, G.; Rosenthal, D.W.; McInerney, A.; Jongco, A.M.; Ponda, P.; Bonagura, V.R. Allergic reactions to coronavirus disease 2019 vaccines and addressing vaccine hesitancy. Ann. Allergy Asthma Immunol. 2021, 128, 161–168.e1. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Igarashi, A.; Morikane, K.; Hachiya, O.; Watanabe, M.; Kakehata, S.; Sato, S.; Ueno, Y. Adverse reactions to BNT162b2 mRNA COVID-19 vaccine in medical staff with a history of allergy. Respir. Investig. 2022, 60, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2022. Available online: www.ginasthma.org (accessed on 20 December 2022).
- European Medicines Agency. EMA: Amsterdam, The Netherlands. 2022. Available online: https://www.ema.europa.eu/en/documents/other/meddra-important-medical-event-terms-list-version-250_en.xlsx (accessed on 13 February 2023).
- Italian Drug Agency (AIFA). FAQ per la Gestione delle Segnalazioni nell’ambito della Rete Nazionale di Farmacovigilanza, AIFA: Rome, Italy. 2021. Available online: https://www.aifa.gov.it/documents/20142/1447627/FAQ_gestione_segnalazioni_Marzo2021.pdf/ (accessed on 20 December 2022).
- Italian Drug Agency (AIFA). Rapporto Annuale Sulla Sicurezza dei Vaccini Anti-COVID-19. AIFA: Rome, Italy. 2021. Available online: https://www.aifa.gov.it/documents/20142/1315190/Rapporto_annuale_su_sicurezza_vaccini%20anti-COVID-19.pdf (accessed on 20 December 2022).
- Lee, Y.W.; Lim, S.Y.; Lee, J.-H.; Lim, J.S.; Kim, M.; Kwon, S.; Joo, J.; Kwak, S.H.; Kim, E.O.; Jung, J.; et al. Adverse Reactions of the Second Dose of the BNT162b2 mRNA COVID-19 Vaccine in Healthcare Workers in South Korea. J. Korean Med. Sci. 2021, 36, e153. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.-A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]
- Vanijcharoenkarn, K.; Lee, F.E.-H.; Martin, L.; Shih, J.; Sexton, M.E.; Kuruvilla, M.E. Immediate Reactions after the First Dose of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Messenger RNA Vaccines Do Not Preclude Second-Dose Administration. Clin. Infect. Dis. 2021, 73, 2108–2111. [Google Scholar] [CrossRef] [PubMed]
- Unina. Vaccino ed Allergie: Domande e Risposte per Saperne di più. Available online: https://www.policlinico.unina.it/flex/cm/pages/ServeBLOB.php/L/IT/IDPagina/3479#:~:text=Circa%20la%20met%C3%A0%20delle%20reazioni,%20di%204%20ore%20dalla%20vaccinazione (accessed on 23 November 2022).
- Allergic Reactions Including Anaphylaxis after Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine—United States, 14–23 December 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Number Reactions (SOC Classification) | First Dose | Second Dose | Booster Dose | Total | ||||
|---|---|---|---|---|---|---|---|---|
| (n.421) | (n.388) | (n.241) | (n.1050) | |||||
| n | (%) | n | (%) | n | (%) | n | (%) | |
| 0 | 383 | (91.0) | 376 | (96.9) | 238 | (98.8) | 997 | (95.0) |
| 1 | 20 | (4.8) | 6 | (1.5) | 2 | (0.8) | 28 | (2.7) |
| 2 | 11 | (2.6) | 5 | (1.3) | 1 | (0.4) | 17 | (1.6) |
| 3 | 6 | (1.4) | 1 | (0.3) | 7 | (0.7) | ||
| 4 | 1 | (0.2) | 1 | (0.1) | ||||
| Covariates | Doses Administered (n.1050) | Reactions | p | adjOR (CI95%) | ||
|---|---|---|---|---|---|---|
| n. | (%) | |||||
| Sex | ||||||
| Males | 293 | 11 | (3.8) | ref | ||
| Females | 757 | 42 | (5.5) | 0.553 | 1.20 (0.66–2.16) | |
| Age (media ± DS) | 53.0 ± 18.5 | 43.6 ± 14.9 | <0.001 | 0.95 (0.94–0.97) | ||
| Doses | ||||||
| First | 421 | 38 | (9.0) | ref | ||
| Second | 388 | 12 | (3.1) | <0.001 | 0.25 (0.13–0.49) | |
| Booster | 241 | 3 | (1.2) | <0.001 | 0.12 (0.04–0.39) | |
| Number of previous allergies (media ± SD) | 2.3 ± 1.4 | 2.5 ± 1.2 | 0.987 | 1.00 (0.78–1.29) | ||
| Vaccine allergy | ||||||
| no | 897 | 41 | (4.6) | ref | ||
| yes | 153 | 12 | (7.8) | 0.379 | 1.39 (0.67–2.89) | |
| Food allergy | ||||||
| no | 713 | 36 | (5.0) | ref | ||
| yes | 337 | 17 | (5.0) | 0.217 | 0.66 (0.34–1.28) | |
| Medicine allergy | ||||||
| no | 298 | 14 | (4.7) | ref | ||
| yes | 752 | 39 | (5.2) | 0.866 | 1.06 (0.52–2.19) | |
| Other medicine with PEG allergy | ||||||
| no | 681 | 34 | (5.0) | ref | ||
| yes | 369 | 19 | (5.1) | 0.856 | 1.07 (0.54–2.09) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cocchio, S.; Girolametto, G.; Pierobon, A.; Furlan, P.; Destefani, E.; Bulegato, L.; Stano, A.; Fietta, S.; Poletto, A.; Baldo, V. Is SARS-CoV-2 Vaccination of Subjects with a Prior History of Allergies Dangerous? Experiences in the Veneto Region of Italy. Vaccines 2023, 11, 574. https://doi.org/10.3390/vaccines11030574
Cocchio S, Girolametto G, Pierobon A, Furlan P, Destefani E, Bulegato L, Stano A, Fietta S, Poletto A, Baldo V. Is SARS-CoV-2 Vaccination of Subjects with a Prior History of Allergies Dangerous? Experiences in the Veneto Region of Italy. Vaccines. 2023; 11(3):574. https://doi.org/10.3390/vaccines11030574
Chicago/Turabian StyleCocchio, Silvia, Gloria Girolametto, Alice Pierobon, Patrizia Furlan, Emanuela Destefani, Lorenzo Bulegato, Antonio Stano, Silvia Fietta, Annachiara Poletto, and Vincenzo Baldo. 2023. "Is SARS-CoV-2 Vaccination of Subjects with a Prior History of Allergies Dangerous? Experiences in the Veneto Region of Italy" Vaccines 11, no. 3: 574. https://doi.org/10.3390/vaccines11030574