
Disparities and Factors Associated with Coronavirus Disease-2019-Related Public Stigma: A Cross-Sectional Study in Thailand

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
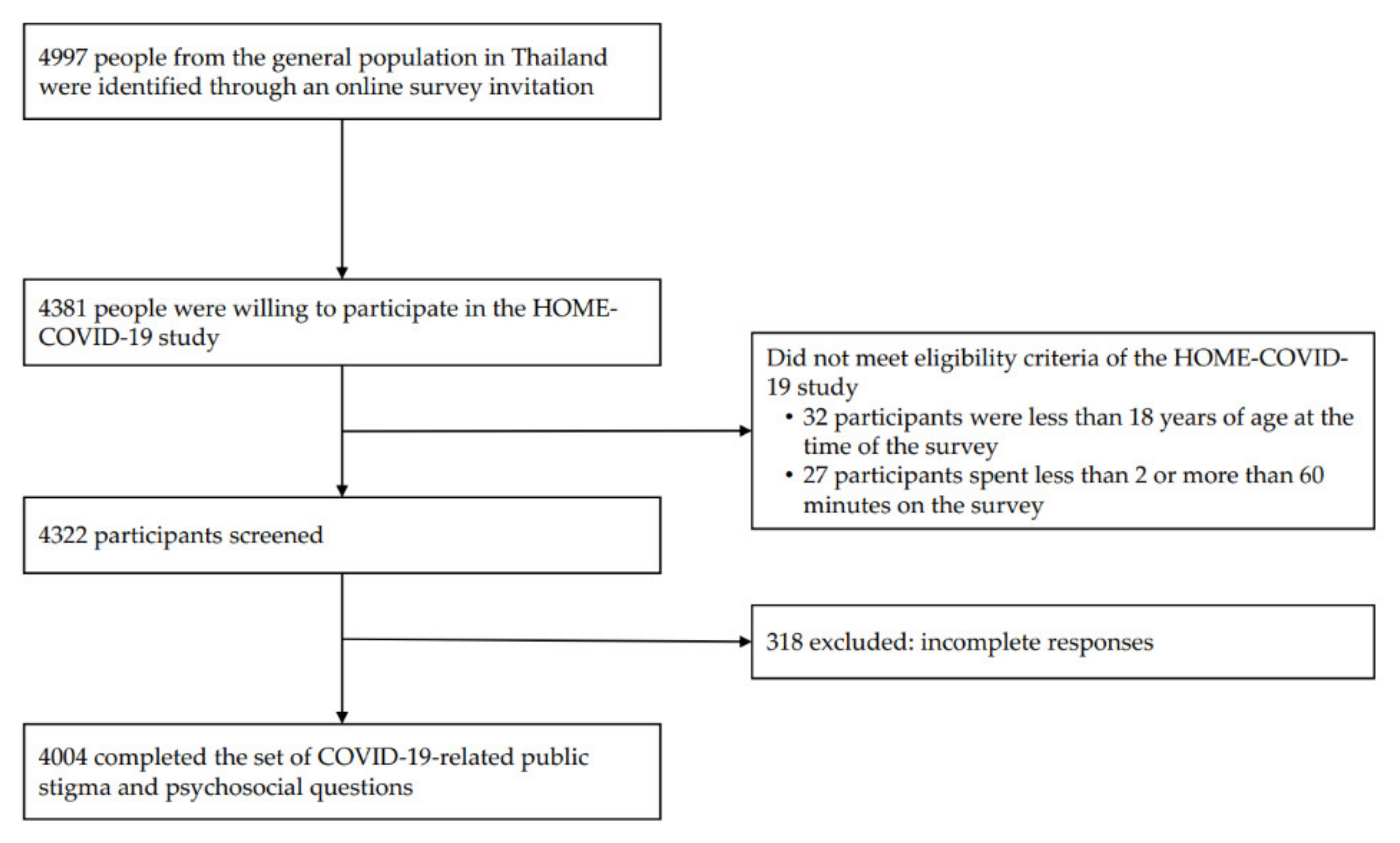
2.1. Study Design and Participants
2.2. Sample Size
2.3. Assessment Tools and Potential Risk Factors
- Public stigma: COVID-PSS comprises ten items with three factors (stereotypes, prejudice, fear), and a possible score range of 10-50 points. The COVID-PSS revealed acceptable psychometric properties in the Thai population, with Cronbach’s α of 0.85. The degree of public stigma was established and classified as no/minimal (≤18 points), moderate (19–25 points), or high (≥26 points) [11].
- Perceived social support: The Multidimensional Scale of Perceived Social Support (MSPSS-12) consists of 12 items that measure individual perceptions of external social support. This scale has excellent internal consistency, with a Cronbach’s α of 0.92 [13]. Perceived social support was categorized as low (12–35 points), moderate (36–60 points), or high (61–84 points).
- Resilient coping: The Brief Resilient Coping Scale (BRCS) consists of four items to capture tendencies to cope with stress in a highly adaptive manner. The BRCS revealed satisfactory reliability (Cronbach’s α = 0.80) [8]. For scale interpretation, BRCS scores was classified as low- (≤13 points), medium- (14–16 points), or high (≥17 points) resilience copers [14].
- Fear of COVID-19 and perceived risk of COVID-19 infection: A numerical rating scale (NRS) of 0–10 points was used to measure the degree of fear or perceived risk of COVID-19 infection. The degree of fear or perceived risk was classified as no/minimal fear or low perceived risk (0–3 points), moderate fear or medium perceived risk (4–6 points), and severe fear or high perceived risk (7–10 points).
- A set of potential risk factors for public stigma, including sociodemographic characteristics (age, sexual identity, marital status, educational level, occupation, religion, region of residence, living status, personal income, reimbursement scheme, history of mental illness, chronic non-communicable diseases (NCDs)), and issues-related to the COVID-19 pandemic (economic burden (income loss, financial problems), duration of exposure to COVID-19-related information, confirmed cases in the community, quarantine status, and working from home status).
2.4. Statistical Analyses
3. Results
3.1. Overview of Participant Characteristics
3.2. Prevalence and Disparities of COVID-19-Related Public Stigma
3.3. Risk Factors Associated with COVID-19-Related Public Stigma
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Public and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Ransing, R.; Ramalho, R.; Orsolini, L.; Adiukwu, F.; Gonzalez-Diaz, J.M.; Larnaout, A.; Pinto da Costa, M.; Grandinetti, P.; Bytyçi, D.G.; Shalbafan, M.; et al. Can COVID-19 related mental health issues be measured? Brain Behav. Immun. 2020, 88, 32–34. [Google Scholar] [CrossRef] [PubMed]
- International Federation of Red Cross and Red Crescent Societies; UNICEF. A Guide to Preventing and Addressing Social Stigma; International Federation of Red Cross and Red Crescent Societies: Geneva, Switzerland, 2020. [Google Scholar]
- Kaufman, K.R.; Petkova, E.; Bhui, K.S.; Schulze, T.G. A global needs assessment in times of a global crisis: World psychiatry response to the COVID-19 pandemic. BJPsych Open. 2020, 6, e48. [Google Scholar] [CrossRef]
- Baldassarre, A.; Giorgi, G.; Alessio, F.; Lulli, L.G.; Arcangeli, G.; Mucci, N. Stigma and Discrimination (SAD) at the Time of the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6341. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.D.; Mamun, M.A. COVID-19 suicidal behavior among couples and suicide pacts: Case study evidence from press reports. Psychiatry Res. 2020, 289, 113105. [Google Scholar] [CrossRef]
- Guo, Q.; Zheng, Y.; Shi, J.; Wang, J.; Li, G.; Li, C.; Fromson, J.A.; Xu, Y.; Liu, X.; Xu, H.; et al. Immediate psychological distress in quarantined patients with COVID-19 and its association with peripheral inflammation: A mixed-method study. Brain Behav. Immun. 2020, 88, 17–27. [Google Scholar] [CrossRef]
- Nochaiwong, S.; Ruengorn, C.; Awiphan, R.; Ruanta, Y.; Boonchieng, W.; Nanta, S.; Kowatcharakul, W.; Pumpaisalchai, W.; Kanjanarat, P.; Mongkhon, P.; et al. Mental health circumstances among health care workers and general public under the pandemic situation of COVID-19 (HOME-COVID-19). Medicine 2020, 99, e20751. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Nochaiwong, S.; Ruengorn, C.; Awiphan, R.; Kanjanarat, P.; Ruanta, Y.; Phosuya, C.; Boonchieng, W.; Nanta, S.; Chongruksut, W.; Thavorn, K.; et al. COVID-19 Public Stigma Scale (COVID-PSS): Development, validation, psychometric analysis and interpretation. BMJ Open 2021, 11, e048241. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T. A revised Thai Multi-Dimensional Scale of Perceived Social Support. Span. J. Psychol. 2012, 15, 1503–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Chory, A.; Nyandiko, W.; Ashimosi, C.; Aluoch, J.; Martin, R.; Biegon, W.; Munyoro, D.; Apondi, E.; Vreeman, R. Social Stigma Related to COVID-19 Disease Described by Primary and Secondary School Teachers and Adolescents Living with HIV in Western Kenya. Front. Public Health 2021, 9, 757267. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Long, J.; Wang, X.; Liao, Y.; Liu, Y.; Hao, Y.; Wu, Q.; Zhou, Y.; Wang, Y.; Wang, Y.; et al. A Comparison of COVID-19 Stigma and AIDS Stigma During the COVID-19 Pandemic: A Cross-Sectional Study in China. Front. Psychiatry 2021, 12, 782501. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Zhou, X.; Lin, L.; Pan, Y.; Zhong, Y.; Wang, X.; Zhu, H. COVID-19-related stigma and its influencing factors: A nationwide cross-sectional study during the early stage of the pandemic in China. BMJ Open 2021, 11, e048983. [Google Scholar] [CrossRef]
- Smith, L.E.; Potts, H.W.W.; Amlȏt, R.; Fear, N.T.; Michie, S.; Rubin, G.J. Holding a stigmatizing attitude at the start of the COVID-19 outbreak: A cross-sectional survey. Br. J. Health Psychol. 2021, 27, 588–604. [Google Scholar] [CrossRef]
- Zhang, T.M.; Fang, Q.; Yao, H.; Ran, M.S. Public Stigma of COVID-19 and Its Correlates in the General Population of China. Int. J. Env. Res. Public Health 2021, 18, 11718. [Google Scholar] [CrossRef]
- Cassiani-Miranda, C.A.; Campo-Arias, A.; Tirado-Otálvaro, A.F.; Botero-Tobón, L.A.; Upegui-Arango, L.D.; Rodríguez-Verdugo, M.S.; Botero-Tobón, M.E.; Arismendy-López, Y.A.; Robles-Fonnegra, W.A.; Niño, L.; et al. Stigmatisation associated with COVID-19 in the general Colombian population. Int. J. Soc. Psychiatry 2020, 67, 728–736. [Google Scholar] [CrossRef]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Chatmon, B.N. Males and Mental Health Stigma. Am. J. Mens Health 2020, 14, 1557988320949322. [Google Scholar] [CrossRef]
- Yuan, Y.; Zhao, Y.J.; Zhang, Q.E.; Zhang, L.; Cheung, T.; Jackson, T.; Jiang, G.Q.; Xiang, Y.T. COVID-19-related stigma and its sociodemographic correlates: A comparative study. Glob. Health 2021, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, A.; Sabry, W.; Mostafa, N.S. COVID-19-related stigmatization among a sample of Egyptian healthcare workers. PLoS ONE 2020, 15, e0244172. [Google Scholar] [CrossRef] [PubMed]
- Do Duy, C.; Nong, V.M.; Ngo Van, A.; Doan Thu, T.; Do Thu, N.; Nguyen Quang, T. COVID-19-related stigma and its association with mental health of health-care workers after quarantine in Vietnam. Psychiatry Clin. Neurosci. 2020, 74, 566–568. [Google Scholar] [CrossRef] [PubMed]
- National Statistical Office; Ministry of Digital Economy and Society. The 2018 Survey on Conditions Of Society, Culture and Mental Health; Statistical Forecasting Division, National Statistical Office: Bangkok, Thailand, 2020. [Google Scholar]
- Davidson, R.J.; Anne, H. Visions of Compassion: Western Scientists and Tibetan Buddhists Examine Human Nature; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Meaney, R.; Hasking, P.; Reupert, A. Prevalence of Borderline Personality Disorder in University Samples: Systematic Review, Meta-Analysis and Meta-Regression. PLoS ONE 2016, 11, e0155439. [Google Scholar] [CrossRef]
- Yuan, Q.; Seow, E.; Abdin, E.; Chua, B.Y.; Ong, H.L.; Samari, E.; Chong, S.A.; Subramaniam, M. Direct and moderating effects of personality on stigma towards mental illness. BMC Psychiatry 2018, 18, 358. [Google Scholar] [CrossRef] [Green Version]
- Duan, W.; Bu, H.; Chen, Z. COVID-19-related stigma profiles and risk factors among people who are at high risk of contagion. Soc. Sci. Med. 2020, 266, 113425. [Google Scholar] [CrossRef]
- Valeri, L.; Amsalem, D.; Jankowski, S.; Susser, E.; Dixon, L. Effectiveness of a Video-Based Intervention on Reducing Perceptions of Fear, Loneliness, and Public Stigma Related to COVID-19: A Randomized Controlled Trial. Int. J. Public Health 2021, 66, 1604164. [Google Scholar] [CrossRef]


{kind=link}
| Participant Characteristics | Degree of COVID-19-Related Public Stigma | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| No/Minimal: COVID-PSS ≤ 18 Points (n = 983) | Moderate: COVID-PSS 19–25 Points (n = 1364) | High: COVID-PSS ≥ 26 Points (n = 1657) | |||||||
| No. of Cases/No. of Total | Prevalence Estimated (% [95% CI]) † | p-Value | No. of Cases/No. of Total | Prevalence Estimated (% [95% CI]) † | p-Value | No. of Cases/No. of Total | Prevalence Estimated (% [95% CI]) † | p-Value | |
| Age, year | |||||||||
| ≤30 | 704/2659 | 25.9 (23.7–28.4) | <0.001 | 953/2659 | 37.1 (34.5–39.8) | <0.001 | 1002/2659 | 37.0 (34.4–39.6) | <0.001 |
| 31–50 | 253/1088 | 23.8 (20.3–27.7) | 355/1088 | 33.6 (29.9–37.5) | 480/1088 | 42.6 (38.7–46.7) | |||
| ≥51 | 26/257 | 8.0 (4.6–13.6) | 56/257 | 25.2 (18.2–33.8) | 175/257 | 66.8 (58.0–74.5) | |||
| Sexual identity | |||||||||
| Female | 673/2619 | 25.5 (23.3–28.0) | <0.001 | 896/2619 | 35.4 (32.8–38.0) | 0.845 | 1050/2619 | 39.1 (36.5–41.8) | 0.227 |
| Male | 260/1231 | 19.3 (16.4–22.6) | 415/1231 | 36.0 (32.3–39.9) | 556/1231 | 44.7 (40.8–48.6) | |||
| Others | 50/154 | 34.5 (24.3–46.4) | 53/154 | 34.1 (24.2–45.7) | 51/154 | 31.4 (21.7–43.0) | |||
| Marital status | |||||||||
| Single | 854/3208 | 26.2 (24.1–28.4) | <0.001 | 1162/3208 | 37.7 (35.4–40.2) | <0.001 | 1192/3208 | 36.1 (33.8–38.5) | <0.001 |
| Married/domestic partnership | 115/693 | 17.6 (13.8–22.2) | 170/693 | 23.6 (19.6–28.1) | 408/693 | 58.8 (53.6–63.8) | |||
| Divorced/widowed/separated | 14/103 | 5.6 (2.9–10.7) | 32/103 | 42.6 (29.4–57.0) | 57/103 | 51.7 (38.0–65.2) | |||
| Education level | |||||||||
| Illiterate/primary school/junior high school | 28/127 | 21.0 (12.1–33.9) | 0.474 | 41/127 | 35.6 (24.9–47.9) | 0.784 | 58/127 | 43.4 (32.0–55.6) | 0.373 |
| Senior high school/diploma/high vocational | 482/1893 | 25.4 (22.7–28.2) | 654/1893 | 36.4 (33.4–39.5) | 757/1893 | 38.2 (35.2–41.4) | |||
| Bachelor’s degree/ higher education | 473/1984 | 23.1 (20.6–25.8) | 669/1984 | 34.4 (31.5–37.4) | 842/1984 | 42.5 (39.4–45.6) | |||
| Occupation | |||||||||
| Unemployed/retried | 95/391 | 23.4 (18.3–29.5) | 0.276 | 129/391 | 38.1 (31.3–45.5) | 0.112 | 167/391 | 38.4 (31.9–45.3) | 0.074 |
| Employed | 480/2024 | 24.2 (21.6–27.0) | 663/2024 | 32.4 (29.7–35.3) | 881/2024 | 43.3 (40.3–46.4) | |||
| College student | 408/1589 | 24.4 (21.6–27.5) | 572/1589 | 38.0 (34.7–41.5) | 609/1589 | 37.5 (34.2–41.0) | |||
| Religion | |||||||||
| Irreligion | 143/375 | 32.9 (26.8–39.6) | 0.167 | 126/375 | 39.1 (32.2–46.6) | 0.795 | 106/375 | 28.0 (22.0–34.9) | <0.001 |
| Buddhist | 787/3454 | 35.3 (33.1–37.6) | 1183/3454 | 35.3 (33.1–37.6) | 1484/3454 | 41.8 (39.4–44.1) | |||
| Christian/Muslim/Others | 53/175 | 28.8 (21.1–38.1) | 55/175 | 29.6 (21.4–39.4) | 67/175 | 41.6 (32.6–51.2) | |||
| Region of residence | |||||||||
| Capital city and its environs | 412/1425 | 28.9 (26.6–31.3) | <0.001 | 498/1425 | 34.9 (32.5–37.5) | 0.382 | 515/1425 | 36.1 (33.7–38.7) | <0.001 |
| Non-capital city and its environs | 571/2579 | 22.9 (20.6–25.3) | 866/2579 | 35.6 (33.0–38.3) | 1142/2579 | 41.5 (38.8–44.2) | |||
| Living status | |||||||||
| Alone | 161/576 | 27.0 (22.0–32.7) | 0.547 | 203/576 | 36.7 (31.2–42.5) | 0.473 | 212/576 | 36.3 (30.7–42.3) | 0.224 |
| With family | 745/3164 | 23.4 (21.4–25.6) | 1074/3164 | 35.4 (33.0–37.8) | 1345/3164 | 41.2 (38.8–43.6) | |||
| With others | 77/264 | 29.8 (22.3–38.6) | 87/264 | 34.5 (26.4–43.6) | 100/264 | 35.6 (27.4–44.8) | |||
| Person income, baht/month § | |||||||||
| ≤10,000 (≤308 USD) | 465/1905 | 24.8 (22.1–27.7) | 0.124 | 654/1905 | 36.2 (33.1–39.4) | 0.747 | 786/1905 | 39.0 (35.9–42.2) | 0.100 |
| 10,001–20,000 (309–616 USD) | 299/1054 | 28.0 (24.3–32.0) | 357/1054 | 35.7 (31.8–39.8) | 398/1054 | 36.3 (32.3–40.5) | |||
| >20,000 (>616 USD) | 219/1045 | 19.0 (16.1–22.3) | 353/1045 | 33.7 (30.0–37.6) | 473/1045 | 47.3 (43.2–51.4) | |||
| Reimbursement scheme | |||||||||
| Government/state enterprises | 112/539 | 20.3 (15.9–25.5) | 0.404 | 157/539 | 30.7 (25.4–36.5) | 0.116 | 270/539 | 49.0 (43.1–55.0) | 0.025 |
| Universal coverage scheme | 346/1329 | 26.1 (22.8–29.7) | 466/1329 | 36.6 (32.9–40.5) | 517/1329 | 37.3 (33.6–41.1) | |||
| Social security scheme | 284/1161 | 23.8 (20.6–27.4) | 402/1161 | 36.3 (32.6–40.1) | 475/1161 | 39.9 (36.1–43.8) | |||
| Self-payment/others | 241/975 | 24.7 (21.2–28.6) | 339/975 | 36.3 (32.3–40.6) | 395/975 | 39.0 (34.9–43.2) | |||
| History of mental illness | |||||||||
| No | 875/3645 | 23.7 (21.8–25.7) | 0.527 | 1249/3645 | 35.5 (33.3–37.7) | 0.394 | 1521/3645 | 40.8 (38.6–43.1) | 0.158 |
| Yes | 108/359 | 30.3 (24.2–37.2) | 115/359 | 35.4 (28.6–42.7) | 136/359 | 34.4 (28.0–41.3) | |||
| History of chronic NCDs ‡ | |||||||||
| No | 861/3405 | 25.2 (23.2–27.3) | 0.010 | 1187/3405 | 36.2 (34.0–38.6) | 0.114 | 1357/3405 | 38.6 (36.3–40.9) | <0.001 |
| Yes | 122/599 | 18.4 (14.6–23.1) | 177/599 | 30.9 (25.9–36.4) | 300/599 | 50.6 (44.9–56.3) | |||
| Income loss during the COVID-19 pandemic | |||||||||
| No | 585/2340 | 23.9 (21.5–26.4) | 0.433 | 825/2340 | 36.2 (33.5–39.0) | 0.060 | 930/2340 | 39.9 (37.1–42.7) | 0.125 |
| Yes | 398/1664 | 24.8 (21.9–27.9) | 539/1664 | 34.4 (31.2–37.7) | 727/1664 | 40.8 (37.6–44.2) | |||
| Financial problems during the COVID-19 pandemic | |||||||||
| No | 498/1992 | 24.4 (21.8–27.1) | 0.511 | 713/1992 | 37.3 (34.3–40.3) | 0.218 | 781/1992 | 38.3 (35.4–41.4) | 0.540 |
| Yes | 485/2012 | 23.1 (21.5–26.9) | 651/2012 | 33.8 (30.9–36.8) | 876/2012 | 42.1 (39.1–45.2) | |||
| Information exposure during the COVID-19 pandemic | |||||||||
| <1 h/day | 408/1481 | 27.0 (23.9–30.4) | <0.001 | 503/1481 | 35.5 (32.1–39.1) | 0.726 | 570/1481 | 37.4 (34.0–40.9) | 0.128 |
| 1–2 h/day | 391/1644 | 22.9 (20.2–25.9) | 571/1644 | 35.9 (32.7–39.3) | 682/1644 | 41.1 (37.8–44.5) | |||
| ≥3 h/day | 184/879 | 43.5 (38.9–48.3) | 290/879 | 34.6 (30.2–39.2) | 405/879 | 43.5 (38.9–48.3) | |||
| Confirmed cases in the community | |||||||||
| No | 637/2562 | 25.1 (22.7–27.7) | 0.808 | 871/2562 | 35.2 (32.5–38.0) | 0.775 | 1054/2562 | 39.7 (37.0–42.5) | 0.025 |
| Yes | 136/641 | 20.2 (16.5–24.6) | 215/641 | 33.1 (28.6–37.9) | 290/641 | 46.6 (41.7–51.6) | |||
| Not known | 210/801 | 25.1 (21.4–29.2) | 278/801 | 38.7 (34.1–43.4) | 313/801 | 36.3 (31.9–40.9) | |||
| Quarantine status | |||||||||
| Never | 486/1781 | 27.6 (24.6–30.7) | <0.001 | 567/1781 | 32.3 (29.3–35.5) | 0.059 | 728/1781 | 40.1 (36.8–43.4) | 0.456 |
| Past | 359/1575 | 22.6 (19.9–25.6) | 563/1575 | 36.5 (33.2–39.8) | 653/1575 | 40.9 (37.6–44.3) | |||
| Current | 138/648 | 20.1 (16.2–24.5) | 234/648 | 40.8 (35.4–46.3) | 276/648 | 39.2 (34.1–44.6) | |||
| Working from home | |||||||||
| No | 209/865 | 23.9 (20.1–28.1) | 0.764 | 293/865 | 34.1 (29.9–38.5) | 0.892 | 363/865 | 42.1 (37.6–46.7) | 0.695 |
| Yes | 774/3139 | 24.3 (22.2–26.5) | 1071/3139 | 35.8 (33.5–38.3) | 1294/3139 | 39.8 (37.4–42.3) | |||
| Perceived social support | |||||||||
| Low perceived support | 59/226 | 32.9 (24.6–42.6) | <0.001 | 69/226 | 33.7 (25.8–42.6) | 0.137 | 98/226 | 33.4 (26.3–41.3) | 0.653 |
| Moderate perceived support | 501/1833 | 27.1 (24.4–30.1) | 574/1833 | 32.7 (29.7–35.8) | 758/1833 | 40.2 (37.1–43.4) | |||
| High perceived support | 423/1945 | 20.5 (18.1–23.2) | 721/1945 | 38.4 (35.3–41.6) | 801/1945 | 41.1 (38.0–44.3) | |||
| Resilient coping | |||||||||
| Low resilient copers | 425/1756 | 23.9 (21.2–26.8) | 0.815 | 605/1756 | 36.8 (33.7–40.1) | 0.864 | 726/1756 | 39.3 (36.2–42.4) | 0.969 |
| Medium resilient copers | 393/1570 | 25.2 (22.1–28.5) | 525/1570 | 34.2 (30.9–37.6) | 652/1570 | 40.6 (37.2–44.2) | |||
| High resilient copers | 165/678 | 23.1 (18.9–27.8) | 234/678 | 34.7 (29.7–40.1) | 279/678 | 42.2 (36.9–47.8) | |||
| Fear of COVID-19 | |||||||||
| No/minimal | 169/200 | 82.9 (74.2–89.0) | <0.001 | 29/200 | 16.4 (10.3–25.1) | <0.001 | 2/200 | 0.7 (0.2–2.9) | <0.001 |
| Moderate | 662/1698 | 38.7 (35.4–42.0) | 754/1698 | 45.8 (42.4–49.2) | 282/1698 | 15.5 (13.3–18.1) | |||
| Severe | 152/2106 | 8.1 (6.5–9.9) | 581/2106 | 28.9 (26.2–31.8) | 1373/2106 | 63.0 (60.0–65.9) | |||
| Perceived risk of COVID-19 infection | |||||||||
| Low perceived risk | 584/767 | 74.5 (69.8–78.7) | <0.001 | 171/767 | 23.8 (19.7–28.5) | <0.001 | 12/767 | 1.7 (0.8–3.7) | <0.001 |
| Medium perceived risk | 385/1997 | 19.9 (17.5–22.5) | 990/1997 | 51.6 (48.5–54.6) | 622/1997 | 28.6 (25.9–31.4) | |||
| High perceived risk | 14/1240 | 1.0 (0.4–2.2) | 203/1240 | 16.7 (13.9–19.9) | 1023/1240 | 82.3 (79.1–85.2) | |||
| Overall | 983/4004 | 24.2 (22.2–26.2) | 1364/4004 | 35.5 (33.4–37.6) | 1657/4004 | 40.3 (38.2–42.4) | |||
| Factors | Moderate vs. No/Minimal | High vs. No/Minimal | ||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted OR (95% CI) † | p-Value | Adjusted OR (95% CI) † | p-Value | Unadjusted OR (95% CI) † | p-Value | Adjusted OR (95% CI) † | p-Value | |
| Age, year | ||||||||
| ≤30 | Reference (1.00) | Reference (1.00) | Reference (1.00) | Reference (1.00) | ||||
| 31–50 | 0.99 (0.76–1.29) | 0.927 | 1.59 (1.08–2.34) | 0.018 | 1.26 (0.97–1.63) | 0.083 | 2.22 (1.36–3.62) | 0.001 |
| ≥51 | 2.19 (1.11–4.35) | 0.024 | 4.34 (1.49–12.64) | 0.007 | 5.84 (3.14–10.83) | <0.001 | 10.31 (3.13–34.01) | <0.001 |
| Sexual identity | ||||||||
| Female | Reference (1.00) | Reference (1.00) | Reference (1.00) | Reference (1.00) | ||||
| Male | 1.34 (1.03–1.75) | 0.028 | 1.68 (1.21–2.33) | 0.002 | 1.51 (1.17–1.95) | 0.001 | 2.35 (1.58–3.49) | <0.001 |
| Others | 0.72 (0.40–1.28) | 0.256 | 1.00 (0.50–2.03) | 0.992 | 0.59 (0.33–1.08) | 0.088 | 1.00 (0.42–2.37) | 0.993 |
| Marital status | ||||||||
| Single | Reference (1.00) | Reference (1.00) | Reference (1.00) | Reference (1.00) | ||||
| Married/domestic partnership | 0.93 (0.65–1.33) | 0.690 | 0.88 (0.52–1.49) | 0.627 | 2.42 (1.75–3.36) | <0.001 | 1.97 (1.07–3.64) | 0.030 |
| Divorced/widowed/separated | 5.24 (2.36–11.64) | <0.001 | 3.88 (1.42–10.55) | 0.008 | 6.64 (3.16–13.99) | <0.001 | 3.69 (1.00–13.60) | 0.050 |
| Education level | ||||||||
| Illiterate/primary school/junior high school | Reference (1.00) | Reference (1.00) | ||||||
| Senior high school/diploma/high vocational | 0.85 (0.40–1.79) | 0.655 | 0.73 (0.36–1.49) | 0.387 | ||||
| Bachelor’s degree/higher education | 0.88 (0.42–1.85) | 0.736 | 0.89 (0.44–1.82) | 0.748 | ||||
| Occupation | ||||||||
| Unemployed/retried | Reference (1.00) | Reference (1.00) | ||||||
| Employed | 0.82 (0.55–1.23) | 0.340 | 1.09 (0.75–1.60) | 0.645 | ||||
| College student | 0.96 (0.64–1.44) | 0.833 | 0.94 (0.64–1.38) | 0.747 | ||||
| Religion | ||||||||
| Irreligion | Reference (1.00) | Reference (1.00) | Reference (1.00) | |||||
| Buddhist | 1.29 (0.90–1.85) | 0.159 | 2.14 (1.47–3.11) | <0.001 | 2.11 (1.22–3.63) | 0.007 | ||
| Christian/Muslim/Others | 0.86 (0.47–1.59) | 0.632 | 1.69 (0.95–3.01) | 0.073 | 1.41 (0.59–3.35) | 0.439 | ||
| Region of residence | ||||||||
| Capital city and its environs | Reference (1.00) | Reference (1.00) | ||||||
| Non-capital city and its environs | 1.29 (1.06–1.57) | 0.012 | 1.45 (1.20–1.76) | <0.001 | 1.45 (1.08–1.95) | 0.013 | ||
| Living status | ||||||||
| Alone | Reference (1.00) | Reference (1.00) | ||||||
| With family | 1.11 (0.80–1.54) | 0.523 | 1.31 (0.94–1.83) | 0.114 | ||||
| With others | 0.85 (0.50–1.46) | 0.564 | 0.89 (0.52–1.54) | 0.676 | ||||
| Person income, baht/month § | ||||||||
| ≤10,000 (≤308 USD) | Reference (1.00) | Reference (1.00) | ||||||
| 10,001–20000 (309–616 USD) | 0.88 (0.66–1.15) | 0.342 | 0.83 (0.63–1.08) | 0.169 | ||||
| >20,000 (>616 USD) | 1.22 (0.92–1.62) | 0.174 | 1.59 (1.21–2.09) | 0.001 | ||||
| Reimbursement scheme | ||||||||
| Government/state enterprises | Reference (1.00) | Reference (1.00) | ||||||
| Universal coverage scheme | 0.93 (0.62–1.38) | 0.709 | 0.59 (0.41–0.86) | 0.006 | ||||
| Social security scheme | 1.01 (0.67–1.51) | 0.974 | 0.69 (0.47–1.01) | 0.056 | ||||
| Self-payment/others | 0.97 (0.64–1.47) | 0.892 | 0.65 (0.44–0.96) | 0.030 | ||||
| History of mental illness | ||||||||
| No | Reference (1.00) | Reference (1.00) | ||||||
| Yes | 0.78 (0.53–1.14) | 0.205 | 0.66 (0.46–0.95) | 0.026 | ||||
| History of chronic NCDs ‡ | ||||||||
| No | Reference (1.00) | Reference (1.00) | ||||||
| Yes | 1.17 (0.82–1.65) | 0.383 | 1.79 (1.30–2.48) | <0.001 | ||||
| Income loss during the COVID-19 pandemic | ||||||||
| No | Reference (1.00) | Reference (1.00) | ||||||
| Yes | 0.91 (0.72–1.16) | 0.457 | 0.99 (0.78–1.24) | 0.908 | ||||
| Financial problems during the COVID-19 pandemic | ||||||||
| No | Reference (1.00) | Reference (1.00) | ||||||
| Yes | 0.92 (0.72–1.16) | 0.463 | 1.53 (1.30–1.80) | 0.362 | ||||
| Information exposure during the COVID-19 pandemic | ||||||||
| <1 h/day | Reference (1.00) | Reference (1.00) | Reference (1.00) | |||||
| 1–2 h/day | 1.19 (0.92–1.55) | 0.184 | 1.30 (1.01–1.67) | 0.045 | 1.52 (1.05–2.21) | 0.027 | ||
| ≥3 h/day | 1.20 (0.87–1.66) | 0.261 | 1.44 (1.06–1.96) | 0.021 | 1.32 (0.84–2.07) | 0.232 | ||
| Confirmed cases in the community | ||||||||
| No | Reference (1.00) | Reference (1.00) | ||||||
| Yes | 1.17 (0.85–1.61) | 0.341 | 1.46 (1.07–1.98) | 0.016 | ||||
| Not known | 1.10 (0.83–1.46) | 0.504 | 0.91 (0.69–1.21) | 0.526 | ||||
| Quarantine status | ||||||||
| Never | Reference (1.00) | Reference (1.00) | Reference (1.00) | Reference (1.00) | ||||
| Past | 1.38 (1.07–1.78) | 0.014 | 1.35 (0.99–1.84) | 0.061 | 1.24 (0.97–1.59) | 0.081 | 1.33 (0.92–1.93) | 0.131 |
| Current | 1.73 (1.24–2.43) | 0.001 | 2.08 (1.31–3.33) | 0.002 | 1.34 (0.97–1.87) | 0.076 | 1.75 (1.03–2.97) | 0.039 |
| Working from home | ||||||||
| No | Reference (1.00) | Reference (1.00) | ||||||
| Yes | 0.97 (0.73–1.28) | 0.826 | 1.08 (0.82–1.41) | 0.593 | ||||
| Perceived social support | ||||||||
| Low perceived support | Reference (1.00) | Reference (1.00) | ||||||
| Moderate perceived support | 1.18 (0.71–1.96) | 0.525 | 1.46 (0.92–2.32) | 0.106 | ||||
| High perceived support | 1.83 (1.10–3.04) | 0.020 | 1.98 (1.24–3.16) | 0.004 | ||||
| Resilient coping | ||||||||
| Low resilient copers | Reference (1.00) | Reference (1.00) | ||||||
| Medium resilient copers | 0.90 (0.64–1.27) | 0.546 | 0.88 (0.63–1.23) | 0.450 | ||||
| High resilient copers | 1.02 (0.73–1.43) | 0.890 | 0.90 (0.65–1.24) | 0.511 | ||||
| Fear of COVID-19 | ||||||||
| No/minimal | Reference (1.00) | Reference (1.00) | Reference (1.00) | Reference (1.00) | ||||
| Moderate | 5.98 (3.4–10.42) | <0.001 | 3.70 (1.95–7.03) | <0.001 | 45.91 (11.13–189.40) | <0.001 | 20.71 (4.11–104.19) | <0.001 |
| Severe | 18.10 (10.04–32.61) | <0.001 | 6.24 (3.16–12.36) | <0.001 | 891.66 (215.11–3695.96) | <0.001 | 111.70 (21.90–569.63) | <0.001 |
| Perceived risk of COVID-19 infection | ||||||||
| Low perceived risk | Reference (1.00) | Reference (1.00) | Reference (1.00) | Reference (1.00) | ||||
| Medium perceived risk | 8.12 (6.06–10.90) | <0.001 | 7.78 (5.61–10.79) | <0.001 | 63.85 (27.90–146.14) | <0.001 | 60.15 (23.80–152.00) | <0.001 |
| High perceived risk | 52.43 (22.46–122.42) | <0.001 | 41.94 (17.56–100.15) | <0.001 | 3672.46 (1183.11–11399.61) | <0.001 | 2245.43 (667.25–7556.23) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruengorn, C.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Thavorn, K.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S. Disparities and Factors Associated with Coronavirus Disease-2019-Related Public Stigma: A Cross-Sectional Study in Thailand. Int. J. Environ. Res. Public Health 2022, 19, 6436. https://doi.org/10.3390/ijerph19116436
Ruengorn C, Awiphan R, Phosuya C, Ruanta Y, Thavorn K, Wongpakaran N, Wongpakaran T, Nochaiwong S. Disparities and Factors Associated with Coronavirus Disease-2019-Related Public Stigma: A Cross-Sectional Study in Thailand. International Journal of Environmental Research and Public Health. 2022; 19(11):6436. https://doi.org/10.3390/ijerph19116436
Chicago/Turabian StyleRuengorn, Chidchanok, Ratanaporn Awiphan, Chabaphai Phosuya, Yongyuth Ruanta, Kednapa Thavorn, Nahathai Wongpakaran, Tinakon Wongpakaran, and Surapon Nochaiwong. 2022. "Disparities and Factors Associated with Coronavirus Disease-2019-Related Public Stigma: A Cross-Sectional Study in Thailand" International Journal of Environmental Research and Public Health 19, no. 11: 6436. https://doi.org/10.3390/ijerph19116436